

Identification of a Link between Suspected Metabolic Syndrome and Cognitive Impairment within Pharmaceutical Care in Adults over 75 Years of Age
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Settings, Design and Sample Size
2.2. Study Participants and Selection
2.3. Classification of MetS and Assessment of Cognitive Function
2.4. Statistical Analysis
3. Results
3.1. Prevalence of sMetS and Cognitive Impairment
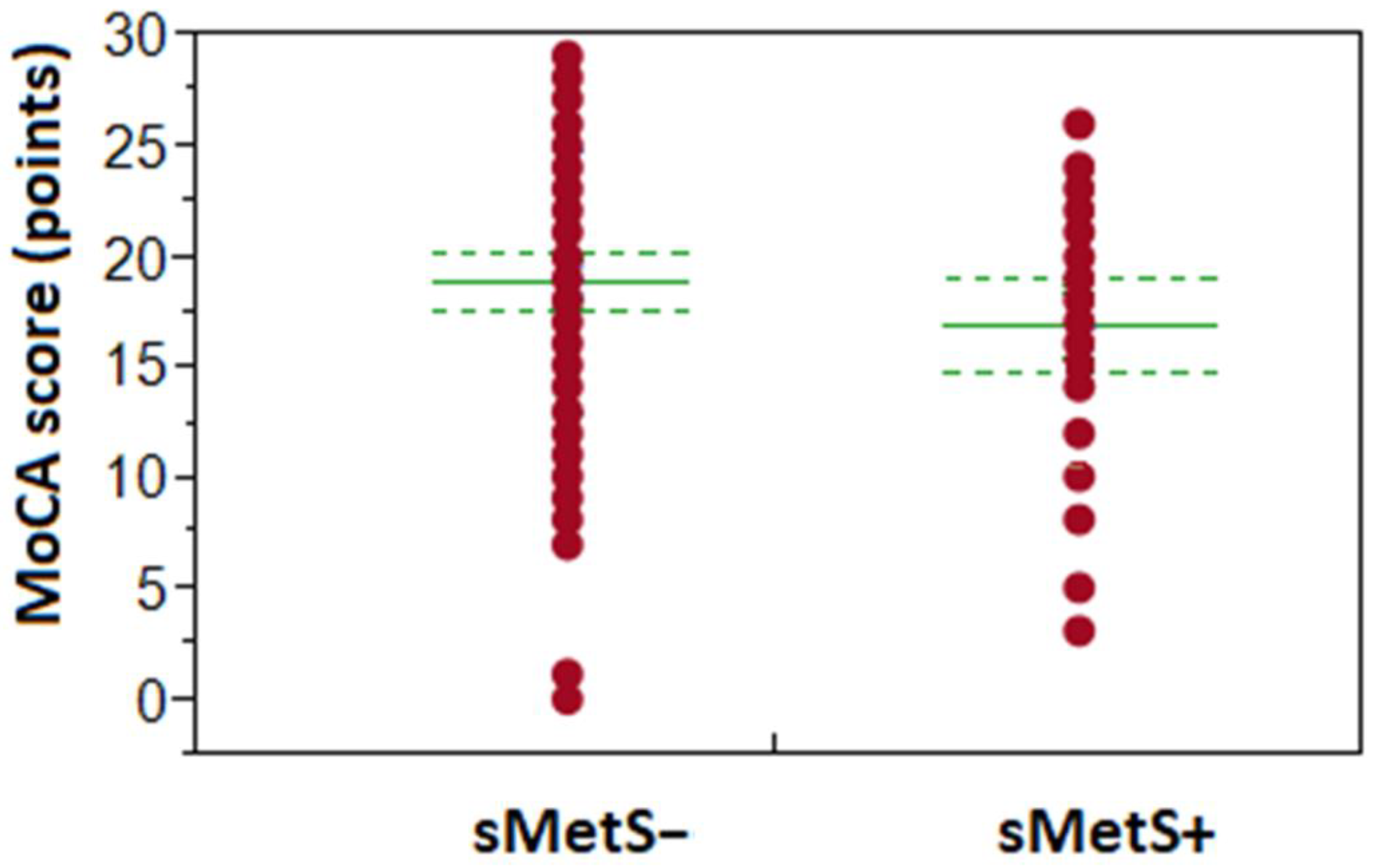
3.2. Occurrence of sMetS and Patients’ Cognitive Performance
3.3. Number of MetS Components and Patients’ Cognitive Performance
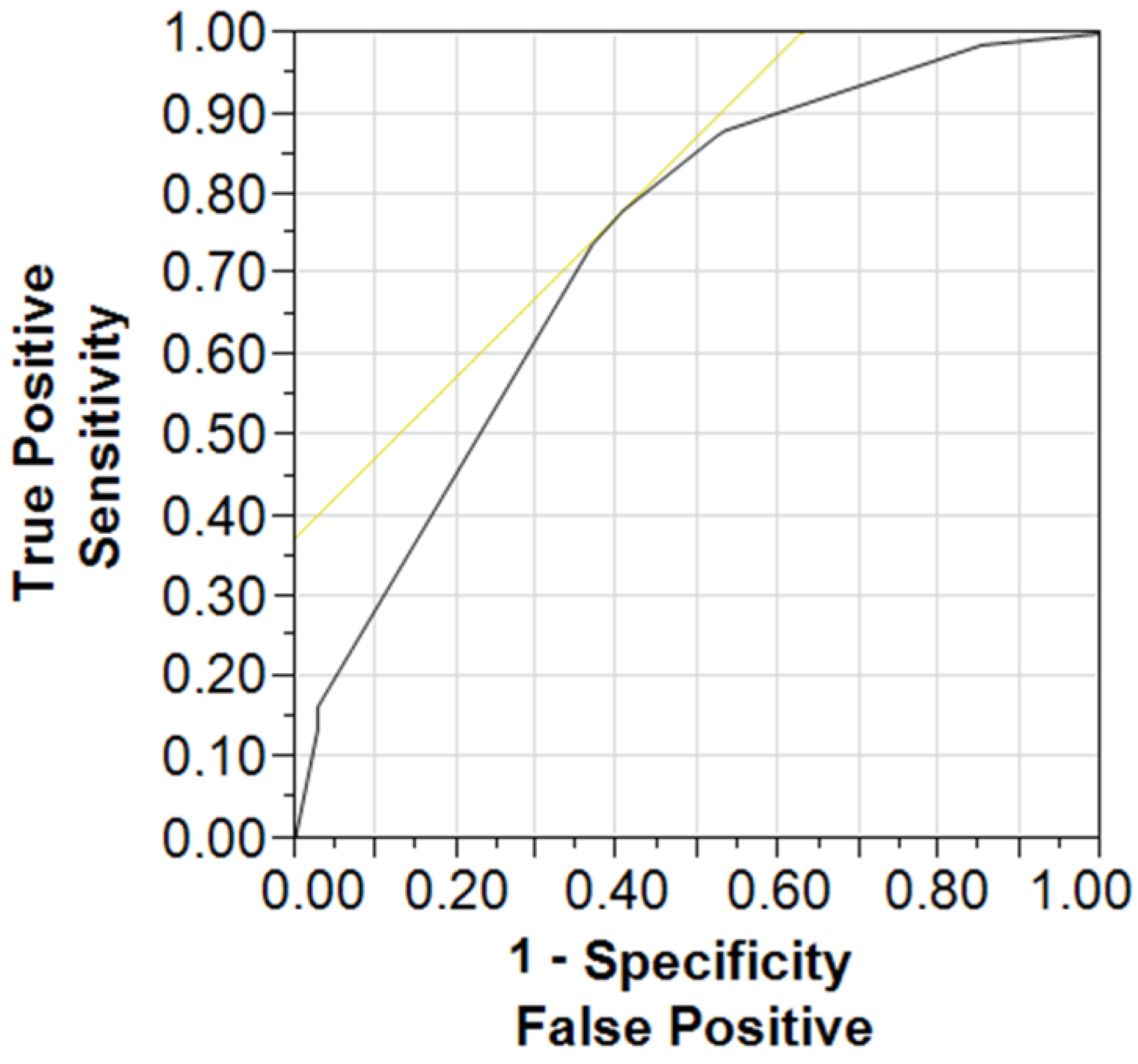
3.4. Association between a MetS Status, Age, Education Level and Cognitive Performance
4. Discussion
4.1. Prevalence of MetS and Cognitive Impairment in Elderly
4.2. Prevalence of MetS and Cognitive Impairment in Younger Elderly Patients
4.3. Prevalence of MetS and Cognitive Impairment in Older Elderly Patients
4.4. Coexistence of the Three Risk Factors: Occurrence of MetS, Age 75+, Lower Education Predicts Lower Cognitive Performance
4.5. Possible Pathological Background Explaining the Link between sMetS and CI
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Assuncao, N.; Sudo, F.K.; Drummond, C.; de Felice, F.G.; Mattos, P. Metabolic Syndrome and cognitive decline in the elderly: A systematic review. PLoS ONE 2018, 13, e0194990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.; He, Y.; Jiang, B.; Wu, L.; Wang, J.; Yang, S.; Wang, Y. Association between metabolic syndrome and mild cognitive impairment and its age difference in a Chinese community elderly population. Clin. Endocrinol. 2015, 82, 844–853. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar]
- Saukkonen, T.; Jokelainen, J.; Timonen, M.; Cederberg, H.; Laakso, M.; Härkönen, P.; Keinänen-Kiukaanniemi, S.; Rajala, U. Prevalence of metabolic syndrome components among the elderly using three different definitions: A cohort study in Finland. Scand. J. Prim. Health Care 2012, 30, 29–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devers, M.C.; Campbell, S.; Simmons, D. Influence of age on the prevalence and components of the metabolic syndrome and the association with cardiovascular disease. BMJ Open Diabetes Res. Care 2016, 4, e000195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hildrum, B.; Mykletun, A.; Hole, T.; Midthjell, K.; Dahl, A.A. Age-specific prevalence of the metabolic syndrome defined by the International Diabetes Federation and the National Cholesterol Education Program: The Norwegian HUNT 2 study. BMC Public Health 2007, 7, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzheimer’s Disease International. Available online: https://www.alzint.org/about/dementia-facts-figures/dementia-statistics/ (accessed on 15 February 2023).
- Lewicki, J.; Religioni, U.; Merks, P. Evaluation of the Community Pharmacy Comorbidities Screening Service on Patients with Chronic Diseases. Patient Prefer. Adherence 2021, 15, 1611–1619. [Google Scholar] [CrossRef]
- Ownby, R.L.; Hertzog, C.; Crocco, E.; Duara, R. Factors related to medication adherence in memory disorder clinic patients. Aging Ment. Health 2006, 10, 378–385. [Google Scholar] [CrossRef]
- Macekova, Z.; Fazekas, T.; Stanko, P.; Vyhnalek, M.; Dragasek, J.; Krivosova, M.; Klimas, J. Cognitive screening within advanced pharmaceutical care in elderly patients with suspected metabolic syndrome. Int. J. Gerontol. 2022, 16, 355–360. [Google Scholar]
- Macekova, Z.; Krivosova, M.; Fazekas, T.; Snopkova, M.; Klimas, J. Short cognitive screening in elderlies as a part of advanced pharmaceutical care in Slovak community pharmacies—The pilot study KOGIMET-SK. Eur. Pharm. J. 2022, 69, 37–42. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Ilardo, M.L.; Speciale, A. The Community Pharmacist: Perceived Barriers and Patient-Centered Care Communication. Int. J. Environ. Res. Public Health 2020, 17, 536. [Google Scholar] [CrossRef] [Green Version]
- Steed, L.; Kassavou, A.; Madurasinghe, V.W.; Edwards, E.A.; Todd, A.; Summerbell, C.D.; Nkansah, N.; Bero, L.; Durieux, P.; Taylor, S.J.; et al. Community pharmacy interventions for health promotion: Effects on professional practice and health outcomes. Cochrane Database Syst. Rev. 2019, 12, CD011207. [Google Scholar] [CrossRef] [Green Version]
- Huber, C.A.; Szucs, T.D.; Rapold, R.; Reich, O. Identifying patients with chronic conditions using pharmacy data in Switzerland: An updated mapping approach to the classification of medications. BMC Public Health 2013, 13, 1030. [Google Scholar] [CrossRef] [Green Version]
- Melton, B.L.; Lai, Z. Review of community pharmacy services: What is being performed, and where are the opportunities for improvement? Integr. Pharm. Res. Pract. 2017, 6, 79–89. [Google Scholar] [CrossRef] [Green Version]
- Meyerson, B.E.; Ryder, P.T.; Richey-Smith, C. Achieving pharmacy-based public health: A call for public health engagement. Public Health Rep. 2013, 128, 140–143. [Google Scholar] [CrossRef] [Green Version]
- Climent, M.T.; Pardo, J.; Muñoz-Almaraz, F.J.; Guerrero, M.D.; Moreno, L. Decision Tree for Early Detection of Cognitive Impairment by Community Pharmacists. Front. Pharmacol. 2018, 9, 1232. [Google Scholar] [CrossRef] [Green Version]
- Rickles, N.M.; Skelton, J.B.; Davis, J.; Hopson, J. Cognitive memory screening and referral program in community pharmacies in the United States. Int. J. Clin. Pharm. 2014, 36, 360–367. [Google Scholar] [CrossRef] [Green Version]
- Algameel, M. Patterns of medication use and adherence to medications among residents in the elderly homes. Pak. J. Med. Sci. 2020, 36, 729–734. [Google Scholar] [CrossRef]
- Lee, S.W.H.; Mak, V.S.L.; Tang, Y.W. Pharmacist services in nursing homes: A systematic review and meta-analysis. Br. J. Clin. Pharmacol 2019, 85, 2668–2688. [Google Scholar] [CrossRef]
- Yaffe, K.; Weston, A.L.; Blackwell, T.; Krueger, K.A. The metabolic syndrome and development of cognitive impairment among older women. Arch. Neurol. 2009, 66, 324–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorodeski, E.Z.; Hashmi, A.Z. Integrating assessment of cognitive status in elderly cardiovascular care. Clin. Cardiol. 2020, 43, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, V.; Jacinto, A.F.; Araújo, L.M.Q.; Cendoroglo, M.S.; Almada Filho, C.M. Cognitive impairment and metabolic syndrome in a population of Brazilian oldest-old. Rev. Assoc. Med. Bras. 2021, 67, 496–499. [Google Scholar] [CrossRef] [PubMed]
- Siervo, M.; Harrison, S.L.; Jagger, C.; Robinson, L.; Stephan, B.C.M. Metabolic Syndrome and Longitudinal Changes in Cognitive Function: A Systematic Review and Meta-Analysis. J. Alzheimer’s Dis. 2014, 41, 151–161. [Google Scholar] [CrossRef]
- Zimmerman, B.; Rypma, B.; Gratton, G.; Fabiani, M. Age-related changes in cerebrovascular health and their effects on neural function and cognition: A comprehensive review. Psychophysiology 2021, 58, e13796. [Google Scholar] [CrossRef] [PubMed]
- Chiang, P.H.; Liu, C.L.; Lin, M.H.; Peng, L.N.; Chen, L.-K.; Chen, J.D.; Hou, S.M. Survival benefits of metabolic syndrome among older men aged 75 years and over in Taiwan. J. Nutr. Health Aging 2012, 16, 520–524. [Google Scholar] [CrossRef]
- Liu, C.L.; Lin, M.H.; Peng, L.N.; Su, C.T.; Liu, L.K.; Chen, L.-K.; Chen, L.Y. Late-life metabolic syndrome prevents cognitive decline among older men aged 75 years and over: One-year prospective cohort study. J. Nutr. Health Aging 2013, 17, 523–526. [Google Scholar] [CrossRef]
- Katsumata, Y.; Todoriki, H.; Higashiuesato, Y.; Yasura, S.; Willcox, D.C.; Ohya, Y.; Willcox, B.J.; Dodge, H.H. Metabolic syndrome and cognitive decline among the oldest old in Okinawa: In search of a mechanism. The KOCOA Project. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 126–134. [Google Scholar] [CrossRef] [Green Version]
- van den Berg, E.; Biessels, G.J.; de Craen, A.J.; Gussekloo, J.; Westendorp, R.G. The metabolic syndrome is associated with decelerated cognitive decline in the oldest old. Neurology 2007, 69, 979–985. [Google Scholar] [CrossRef]
- Vanhanen, M.; Koivisto, K.; Moilanen, L.; Helkala, E.L.; Hänninen, T.; Soininen, H.; Kervinen, K.; Kesäniemi, Y.A.; Laakso, M.; Kuusisto, J. Association of metabolic syndrome with Alzheimer disease: A population-based study. Neurology 2006, 67, 843–847. [Google Scholar] [CrossRef]
- Cerreta, F.; Temple, R.; Asahina, Y.; Connaire, C. Regulatory activities to address the needs of older patients. J. Nutr. Health Aging 2015, 19, 232–233. [Google Scholar] [CrossRef]
- Bartos, A.; Fayette, D. Validation of the Czech Montreal Cognitive Assessment for Mild Cognitive Impairment due to Alzheimer Disease and Czech Norms in 1,552 Elderly Persons. Dement Geriatr. Cogn. Disord. 2018, 46, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.P.; Feng, L.; Nyunt, M.S.; Feng, L.; Gao, Q.; Lim, M.L.; Collinson, S.L.; Chong, M.S.; Lim, W.S.; Lee, T.S.; et al. Metabolic Syndrome and the Risk of Mild Cognitive Impairment and Progression to Dementia: Follow-Up of the Singapore Longitudinal Ageing Study Cohort. JAMA Neurol. 2016, 73, 456–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, S.L.; Stephan, B.C.; Siervo, M.; Granic, A.; Davies, K.; Wesnes, K.A.; Kirkwood, T.B.L.; Robinson, L.; Jagger, C. Is there an association between metabolic syndrome and cognitive function in very old adults? The Newcastle 85+ Study. J. Am. Geriatr. Soc. 2015, 63, 667–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laudisio, A.; Marzetti, E.; Pagano, F.; Cocchi, A.; Franceschi, C.; Bernabei, R.; Zuccalà, G. Association of metabolic syndrome with cognitive function: The role of sex and age. Clin. Nutr. 2008, 27, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Sergi, G.; De Rui, M.; Coin, A.; Inelmen, E.M.; Manzato, E. Weight loss and Alzheimer’s disease: Temporal and aetiologic connections. Proc. Nutr. Soc. 2013, 72, 160–165. [Google Scholar] [CrossRef] [Green Version]
- Na, K.S. Prediction of future cognitive impairment among the community elderly: A machine-learning based approach. Sci. Rep. 2019, 9, 3335. [Google Scholar] [CrossRef] [Green Version]
- Hu, M.; Shu, X.; Yu, G.; Wu, X.; Välimäki, M.; Feng, H. A Risk Prediction Model Based on Machine Learning for Cognitive Impairment Among Chinese Community-Dwelling Elderly People with Normal Cognition: Development and Validation Study. J. Med. Internet Res. 2021, 23, e20298. [Google Scholar] [CrossRef]
- Sato, N.; Morishita, R. Roles of vascular and metabolic components in cognitive dysfunction of Alzheimer disease: Short- and long-term modification by non-genetic risk factors. Front. Aging Neurosci. 2013, 5, 64. [Google Scholar] [CrossRef] [Green Version]
- Biessels, G.J.; Whitmer, R.A. Cognitive dysfunction in diabetes: How to implement emerging guidelines. Diabetologia 2020, 63, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Watts, A.S.; Loskutova, N.; Burns, J.M.; Johnson, D.K. Metabolic syndrome and cognitive decline in early Alzheimer’s disease and healthy older adults. J. Alzheimers Dis. 2013, 35, 253–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, C.K.; Kao, T.W.; Lee, J.T.; Wu, C.J.; Hueng, D.Y.; Liang, C.S.; Wang, G.C.; Yang, F.C.; Chen, W.L. Increased risk of cognitive impairment in patients with components of metabolic syndrome. Medicine 2016, 95, e4791. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.S.; Vidal, J.S.; Masaki, K.; Petrovitch, H.; Ross, G.W.; Tilley, C.; Launer, L.J. Midlife blood pressure, plasma β-amyloid, and the risk for Alzheimer disease: The Honolulu Asia Aging Study. Hypertension 2012, 59, 780–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, M.; Sigurdsson, S.; Kjartansson, O. Joint effect of mid- and late-life blood pressure on the brain: The AGES-Reykjavik study. Neurology 2014, 82, 2187–2195. [Google Scholar] [CrossRef] [Green Version]
- Power, M.C.; Tchetgen, E.J.; Sparrow, D.; Schwartz, J.; Weisskopf, M.G. Blood pressure and cognition: Factors that may account for their inconsistent association. Epidemiology 2013, 24, 886–893. [Google Scholar] [CrossRef] [Green Version]
- Levine, D.A.; Galecki, A.T.; Langa, K.M.; Unverzagt, F.W.; Kabeto, M.U.; Giordani, B.; Cushman, M.; McClure, L.A.; Safford, M.M.; Wadley, V.G. Blood Pressure and Cognitive Decline Over 8 Years in Middle-Aged and Older Black and White Americans. Hypertension 2019, 73, 310–318. [Google Scholar] [CrossRef]
- Hou, Q.; Guan, Y.; Yu, W.H.; Liu, X.T.; Wu, L.H.; Xiao, M.Z.; Lu, Y. Associations between obesity and cognitive impairment in the Chinese elderly: An observational study. Clin. Interv. Aging 2019, 14, 367–373. [Google Scholar] [CrossRef] [Green Version]
- Yaneva-Sirakova, T.; Traykov, L.; Petrova, J.; Gruev, I.; Vassilev, D. Screening for mild cognitive impairment in patients with cardiovascular risk factors. Neuropsychiatr. Dis. Treat. 2017, 13, 2925–2934. [Google Scholar] [CrossRef] [Green Version]
- Shalev, D.; Arbuckle, M.R. Metabolism and Memory: Obesity, Diabetes, and Dementia. Biol. Psychiatry 2017, 82, e81–e83. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Age Groups | 60–74 Years N (%) | 75+ Years N (%) |
|---|---|---|
| Participants, N (%) | ||
| All | 205 (63) | 118 (37) |
| Gender, N (%) | ||
| Female | 128 (63) | 91 (77) |
| Male | 77 (37) | 27 (23) |
| Age, median ± SD | 67.1 ± 4.0 | 82.9 ± 4.1 |
| Education (years), mean ± SD | 12.3 ± 2.2 | 12.0 ± 2.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macekova, Z.; Fazekas, T.; Krivosova, M.; Dragasek, J.; Zufkova, V.; Klimas, J.; Snopkova, M. Identification of a Link between Suspected Metabolic Syndrome and Cognitive Impairment within Pharmaceutical Care in Adults over 75 Years of Age. Healthcare 2023, 11, 718. https://doi.org/10.3390/healthcare11050718
Macekova Z, Fazekas T, Krivosova M, Dragasek J, Zufkova V, Klimas J, Snopkova M. Identification of a Link between Suspected Metabolic Syndrome and Cognitive Impairment within Pharmaceutical Care in Adults over 75 Years of Age. Healthcare. 2023; 11(5):718. https://doi.org/10.3390/healthcare11050718
Chicago/Turabian StyleMacekova, Zuzana, Tomas Fazekas, Michaela Krivosova, Jozef Dragasek, Viera Zufkova, Jan Klimas, and Miroslava Snopkova. 2023. "Identification of a Link between Suspected Metabolic Syndrome and Cognitive Impairment within Pharmaceutical Care in Adults over 75 Years of Age" Healthcare 11, no. 5: 718. https://doi.org/10.3390/healthcare11050718