

Are Health Information Systems Ready for the Digital Transformation in Portugal? Challenges and Future Perspectives

Abstract
:1. Introduction
2. Theoretical Framework
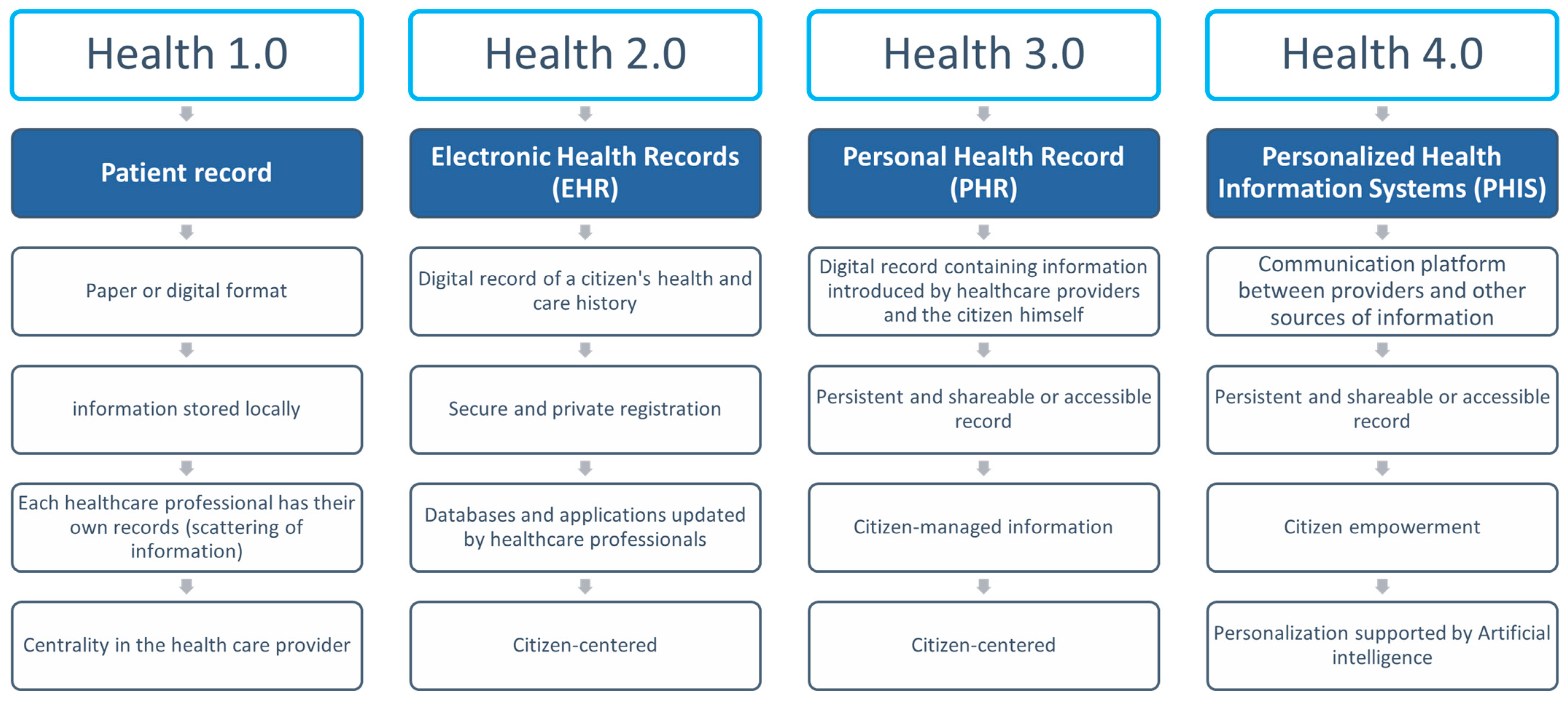
2.1. Evolution of HIS to Date
2.2. The Fourth Industrial Revolution and the HIS
- Triage of patients—LLMs, such as ChatGTP, can be used as primary points of contact between the patient and the healthcare system, triaging patients and decreasing the burden on the healthcare system. Moreover, these tools can also reduce clinical biases, providing a standard of consideration to every patient, independent of personal characteristics.
- Medical scribe functions—modern healthcare systems require the input by the physicians or their assistants of large amounts of data. LLMs can be used to help or reduce this workload, performing note-taking tasks and writing brief patient summaries and presentations. One such example is a recent Microsoft announcement that Teams would provide note-taking features for meetings [47].
- Diagnosis assistance—LLMs can become important tools to help clinicians to make an evidence-based differential diagnosis as unbiased tools that can be trained not only with large amounts of medical information but which can also be updated with the latest relevant data, including innovative academic studies or clinical trials.
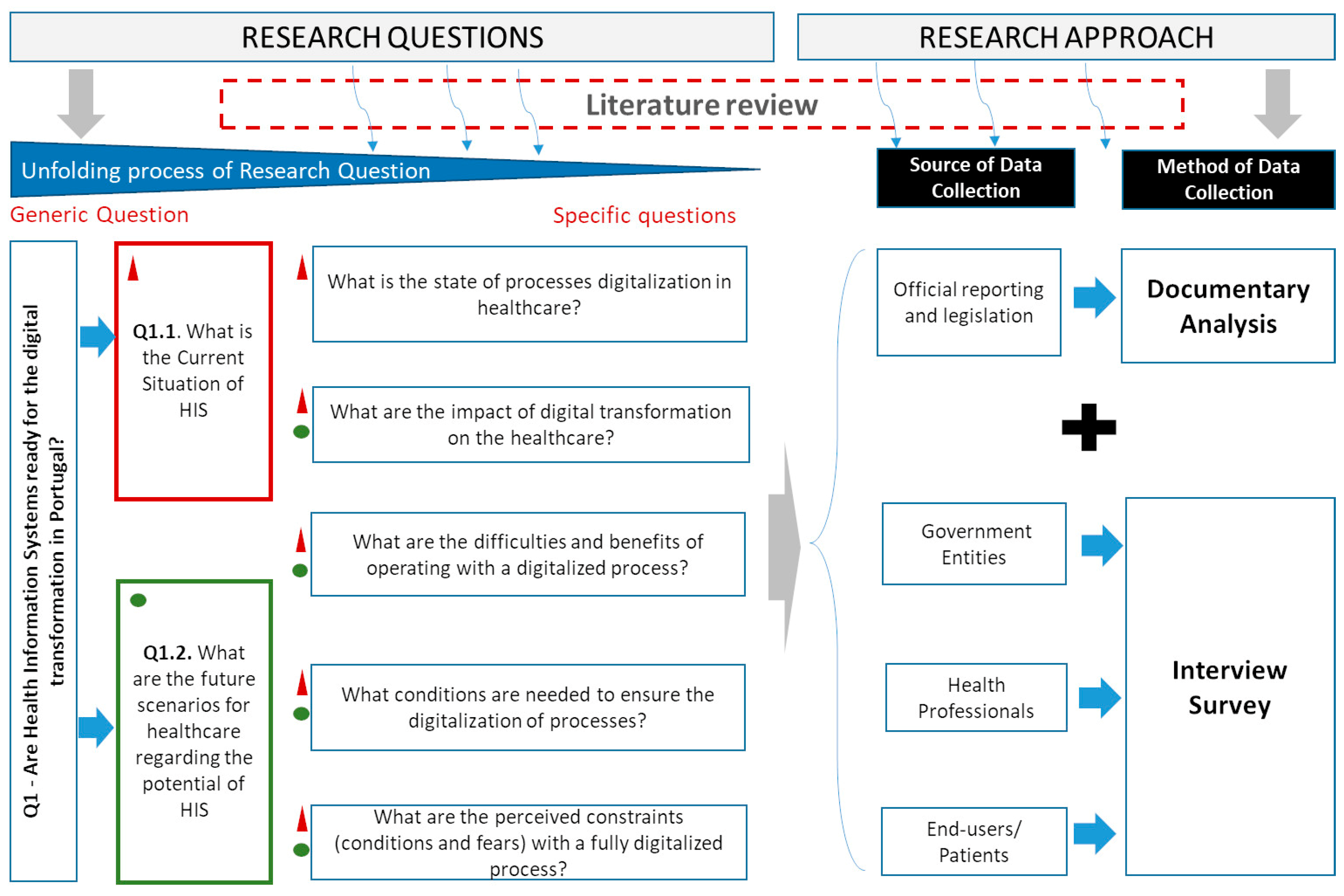
3. Materials and Methods
3.1. Data Collection Methods and Procedures
3.2. Data Analysis Methods
3.3. The Sample Profile of Respondents
4. Results
4.1. Analysis and Reflection on the Current HIS
4.1.1. Current HIS Situation: Document Analysis
4.1.2. Findings from Interviews
The State of Processes’ Digitalization
The process of digitalization is almost consolidated in the public sector, (…), we have problems with very large hospitals with very old and poorly computerized systems, both at the regional and national levels that delay the process as a whole.(E13-GE)
We are taking steps towards full integration in terms of system development (…). Portugal is far ahead, compared to many countries, in Europe.(E11-M)
We are even implementing the paperless hospital project which is a project that has had good and referenced results, our hospital can get 70% of patients to leave the hospital without paper.(E10-M)
(…) it has evolved into a strategic concept, but there is a long way to go, there is a lack of clinical information in the interaction between private and public institutions (…)(E6-P)
(…) there is still a lot of lack of communication between hospitals and health centers. A lot of time is spent transcribing the analyses (…) it is necessary to continuously improve the software (…)(E3-M)
Impact of Digital Transformation on the Healthcare
Digital health is another type of (…) health service, and another way of doing health” (…) to telehealth, but is connected for example with preventive medicine, with precision drugs.(E13-GE)
These platforms can complement and help diagnosis (…)(E1-U)
The potential to do good, to change health (…) the transformation of health, from one-on-one health practice to a population health practice(E11-M)
There are already positive impacts, but the centrality of the patient in the system does not exist(E6-P)
Difficulties and Benefits of Operating with Digitalized Processes
(…) it has more to do with people than with technology (resistance to change, stability of teams, continuous training)(E11-M)
(…) lack of integration of systems between institutions(E2-P)
(…) there is no standardization of the systems themselves, they are always different systems(E4-P)
Conditions for Digital Transformation
(…) it is necessary to create legitimacy to define the use of digital technology [wearables] because it is different if I use it to record my health data, or if the data generated by these technologies can be used to make diagnoses or suggest therapy. This is too important to be seen at an international level to define interoperability standards and rules(E13-EG)
Conditions Required for the Reduction of Info Exclusion
(…) the current population is very ageing (…) it does not easily adapt to IT. The state should ensure minimal training, monitoring, and simplify the development of these technologies (…)(E1-U)
(…) we have pioneering projects such as Citizen HOSP that, through our social workers, support users to take advantage of the use of IT in access to health services (…)(E10-M)
4.2. Prospects for HIS in Portugal and Scenarios
4.2.1. Medicine Practices
(…) Reduction of doctor-patient contact because computer solutions will compare certain standards by AI and allow diagnostics, without the patient presence. (…) a great combination of general medical knowledge with computer knowledge(E1-U)
The practice of medicine in the future will be more dematerialized, remote[telemedicine], a preventive and precision medicine (…) the citizen will be more involved in his/her health/disease and the decisions about it, he/she will now his/her test results, and he will already bring the data stored in digital media.(E13-GE)
(…) technology is evolving and the way we organize ourselves to supply healthcare is not advancing at the same pace.(E13-GE)
4.2.2. Technologies
(…) there has been a decrease in doctor-patient confidence and (…), this system, although useful, can aggravate even more this situation(E9-P)
(…) we need robust systems to treat this information, such as Business Intelligence or Data Mining, which are being implemented in our hospital (…) technologies allow us to innovate health, better manage resources, know patients (…)(E10-M)
In ten years, I think it will be possible to computerize almost total medical information(E9-P)
4.2.3. Fears and Challenges
(…) lose the patients’ data (…)(E2-P)
(…) who has access to this information and what are you going to do with it?(E11-M)
Some of the pointed-out fears and negative opinions about ICT evolution can be seen as challenges by HIS developers. The following comments can be illustrative:
(…) doctors must rediscover themselves, as coachers, people who guide reading(E13-GE)
(…) the data still cannot sustain the psychological reality of the patient in the interpretation of his disease (…) we must not forget that we have biological complexity and that the Human being is not purely data. We do not treat data, we treat people(E6-P)
4.2.4. Possible Scenarios
- (i)
- Medical Practices—the following concepts were found:
- Precision Medicine/Individualized—a medicine whose treatment is specific to a particular patient.
- Preventive Medicine—in which the focus is to keep healthy instead of curing the disease.
- Point-of-Care (Telemedicine)—allowing citizens to be physically distant from medical centers to have access to expert diagnoses.
- Assisted Medical Practices—in which machines (robots) with AI embedded start to help or even replace health professionals in various medical acts.
- (ii)
- Technologies—the concepts found are:
- Interoperability—integration of HIS with intra- and inter-organizational information exchange between public and private and national and international entities.
- Digital Health Transformation—health processes are aided by technologies.
- Technology to Assist Medical Practices—such as robots and AI, among others, helping health professionals.
- Use of electronic devices (wearables), robotics, and intra-devices—used by citizens to monitor their health, with the possibility of collecting data and sending these data to health entities/health professionals.
- (iii)
- Challenges and Risks—the concepts are:
- Resistance to change (people, users, and health professionals)
- Information exclusion (Training/Monitoring)
- Information (privacy, quality, and security—access and loss)
5. Discussion and Reflection
5.1. Theoretical Implications
5.2. Managerial and Societal Implications
6. Conclusions and Recommendations
Limitations and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gökalp, E.; Kayabay, K.; Gökalp, M.O. Leveraging Digital Transformation Technologies to Tackle COVID-19: Proposing a Privacy-First Holistic Framework. In Emerging Technologies During the Era of COVID-19 Pandemic; Arpaci, I., Al-Emran, M., Al-Sharafi, M.A., Marques, G., Eds.; Studies in Systems, Decision and Control; Springer: Cham, Switzerland, 2021; Volume 348, pp. 149–166. [Google Scholar] [CrossRef]
- Loeza-Mejía, C.-I.; Sánchez-DelaCruz, E.; Pozos-Parra, P.; Landero-Hernández, L.-A. The potential and challenges of Health 4.0 to face COVID-19 pandemic: A rapid review. Health Technol. 2021, 11, 1321–1330. [Google Scholar] [CrossRef]
- Nomura, S.; Siesjö, V.; Tomson, G.; Mohr, W.; Fukuchi, E.; Shibuya, K.; Tangcharoensathien, V.; Miyata, H. Contributions of information and communications technology to future health systems and Universal Health Coverage: Application of Japan’s experiences. Health Res. Policy Syst. 2020, 18, 73. [Google Scholar] [CrossRef]
- WHO. Global Observatory for eHealth, World Health Organization. 2019. Available online: http://www.who.int/goe/en/ (accessed on 22 March 2019).
- El-Sherif, D.M.; Abouzid, M.; Elzarif, M.T.; Ahmed, A.A.; Albakri, A.; Alshehri, M.M. Telehealth and Artificial Intelligence Insights into Healthcare during the COVID-19 Pandemic. Healthcare 2022, 10, 385. [Google Scholar] [CrossRef]
- Epizitone, A.; Moyane, S.P.; Agbehadji, I.E. Health Information System and Health Care Applications Performance in the Healthcare Arena: A Bibliometric Analysis. Healthcare 2022, 10, 2273. [Google Scholar] [CrossRef]
- Massaro, M. Digital transformation in the healthcare sector through blockchain technology. Insights from academic research and business developments. Technovation 2023, 120, 102386. [Google Scholar] [CrossRef]
- Haux, R. Health Information Systems—From Present to Future? The German Medical Informatics Initiative. Methods Inf. Med. 2018, 57, e43–e45. [Google Scholar] [CrossRef] [Green Version]
- Can, O.; Sezer, E.; Bursa, O.; Unalir, M.O. Comparing Relational and Ontological Triple Stores in Healthcare Domain. Entropy 2017, 19, 30. [Google Scholar] [CrossRef] [Green Version]
- Haarbrandt, B.; Schreiweis, B.; Rey, S.; Sax, U.; Scheithauer, S.; Rienhoff, O.; Knaup-Gregori, P.; Bavendiek, U.; Dieterich, C.; Brors, B.; et al. HiGHmed—An Open Platform Approach to Enhance Care and Research across Institutional Boundaries. Methods Inf. Med. 2018, 57, e66–e81. [Google Scholar] [CrossRef] [Green Version]
- Al-Jaroodi, J.; Mohamed, N.; Abukhousa, E. Health 4.0: On the Way to Realizing the Healthcare of the Future. IEEE Access 2020, 8, 211189–211210. [Google Scholar] [CrossRef]
- Marinelli, S.; Basile, G.; Zaami, S. Telemedicine, Telepsychiatry and COVID-19 Pandemic: Future Prospects for Global Health. Healthcare 2022, 10, 2085. [Google Scholar] [CrossRef]
- Haddara, M.; Staaby, A. RFID Applications and Adoptions in Healthcare: A Review on Patient Safety. Procedia Comput. Sci. 2018, 138, 80–88. [Google Scholar] [CrossRef]
- Prasser, F.; Kohlbacher, O.; Mansmann, U.; Bauer, B.; Kuhn, K.A. Data Integration for Future Medicine (DIFUTURE). Methods Inf. Med. 2018, 57, e57–e65. [Google Scholar] [CrossRef] [Green Version]
- Cavallone, M.; Palumbo, R. Debunking the myth of industry 4.0 in health care: Insights from a systematic literature review. TQM J. 2020, 32, 849–868. [Google Scholar] [CrossRef]
- Nayak, S.; Patgiri, R. A Vision on Intelligent Medical Service for Emergency on 5G and 6G Communication Era. EAI Endorsed Trans. Internet Things 2020, 6. [Google Scholar] [CrossRef]
- Nayak, S.; Patgiri, R. 6G Communication Technology: A Vision on Intelligent Healthcare. In Health Informatics: A Computational Perspective in Healthcare; Patgiri, R., Biswas, A., Roy, P., Eds.; Studies in Computational Intelligence; Springer: Singapore, 2021; Volume 932, pp. 1–18. [Google Scholar] [CrossRef]
- Gehring, S.; Eulenfeld, R. German Medical Informatics Initiative: Unlocking Data for Research and Health Care. Methods Inf. Med. 2018, 57, e46–e49. [Google Scholar] [CrossRef] [Green Version]
- Tummers, J.; Tekinerdogan, B.; Tobi, H.; Catal, C.; Schalk, B. Obstacles and features of health information systems: A systematic literature review. Comput. Biol. Med. 2021, 137, 104785. [Google Scholar] [CrossRef]
- Khubone, T.; Tlou, B.; Mashamba-Thompson, T.P. Electronic Health Information Systems to Improve Disease Diagnosis and Management at Point-of-Care in Low and Middle Income Countries: A Narrative Review. Diagnostics 2020, 10, 327. [Google Scholar] [CrossRef]
- Tabaeeian, R.A.; Hajrahimi, B.; Khoshfetrat, A. A systematic review of telemedicine systems use barriers: Primary health care providers’ perspective. J. Sci. Technol. Policy Manag. 2022. [Google Scholar] [CrossRef]
- SPMS. ENESIS-2020. 2017. Available online: https://enesis.spms.min-saude.pt (accessed on 29 December 2019).
- Marutha, N.S. Landscaping health-care system using functional records management activities. Collect. Curation 2020, 40, 9–14. [Google Scholar] [CrossRef]
- Hawthorne, K.H.; Richards, L. Personal health records: A new type of electronic medical record. Rec. Manag. J. 2017, 27, 286–301. [Google Scholar] [CrossRef]
- Carolina, A.; Monteiro, B.; França, R.P.; Estrela, V.V.; Iano, Y.; Khelassi, A.; Razmjooy, N. Health 4.0: Applications, Management Technologies and Review. Med. Technol. J. 2019, 2, 262–276. [Google Scholar] [CrossRef]
- Alcácer, V.; Cruz-Machado, V. Scanning the Industry 4.0: A Literature Review on Technologies for Manufacturing Systems. Eng. Sci. Technol. Int. J. 2019, 22, 899–919. [Google Scholar] [CrossRef]
- Karatas, M.; Eriskin, L.; Deveci, M.; Pamucar, D.; Garg, H. Big Data for Healthcare Industry 4.0: Applications, challenges and future perspectives. Expert Syst. Appl. 2022, 200, 116912. [Google Scholar] [CrossRef]
- Javaid, M.; Haleem, A. Industry 4.0 applications in medical field: A brief review. Curr. Med. Res. Pract. 2019, 9, 102–109. [Google Scholar] [CrossRef]
- Ciasullo, M.V.; Orciuoli, F.; Douglas, A.; Palumbo, R. Putting Health 4.0 at the service of Society 5.0: Exploratory insights from a pilot study. Socio-Econ. Plan. Sci. 2022, 80, 101163. [Google Scholar] [CrossRef]
- Cáceres, C.; Rosário, J.M.; Amaya, D. Towards Health 4.0: e-Hospital Proposal Based Industry 4.0 and Artificial Intelligence Concepts. In Artificial Intelligence in Medicine; Riaño, D., Wilk, S., ten Teije, A., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2019; Volume 11526. [Google Scholar] [CrossRef]
- Liu, Z.; Ren, L.; Xiao, C.; Zhang, K.; Demian, P. Virtual Reality Aided Therapy towards Health 4.0: A Two-Decade Bibliometric Analysis. Int. J. Environ. Res. Public Health 2022, 19, 1525. [Google Scholar] [CrossRef]
- Wehde, M. Healthcare 4.0. IEEE Eng. Manag. Rev. 2019, 47, 24–28. [Google Scholar] [CrossRef]
- Schnurr, H.-P.; Aronsky, D.; Wenke, D. MEDICINE 4.0—Interplay of Intelligent Systems and Medical Experts. In Knowledge Management in Digital Change; North, K., Maier, R., Haas, O., Eds.; Springer: Cham, Switzerland, 2018; pp. 51–63. [Google Scholar] [CrossRef]
- Chute, C.; French, T. Introducing Care 4.0: An Integrated Care Paradigm Built on Industry 4.0 Capabilities. Int. J. Environ. Res. Public Health 2019, 16, 2247. [Google Scholar] [CrossRef] [Green Version]
- Afferni, P.; Merone, M.; Soda, P. Hospital 4.0 and Its Innovation in Methodologies and Technologies. In Proceedings of the 2018 IEEE 31st International Symposium on Computer-Based Medical Systems (CBMS), Karlstad, Sweden, 18–21 June 2018; pp. 333–338. [Google Scholar] [CrossRef]
- Unterhofer, M.; Rauch, E.; Matt, D.T. Hospital 4.0 roadmap: An agile implementation guideline for hospital manager. Int. J. Agil. Syst. Manag. 2021, 14, 635. [Google Scholar] [CrossRef]
- Feussner, H.; Ostler, D.; Kranzfelde, M.; Kohn, N.; Koller, S.; Wilhelm, D.; Thuemmler, C.; Schneider, A. Surgery 4.0. In Health 4.0: How Virtualization and Big Data Are Revolutionizing Healthcare; Thuemmler, C., Bai, C., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 91–107. [Google Scholar] [CrossRef]
- Kickbusch, I. Health promotion 4.0. Health Promot. Int. 2019, 34, 179–181. [Google Scholar] [CrossRef] [Green Version]
- Hou, Y.; Wang, W.; Bartolo, P. Application of additively manufactured 3D scaffolds for bone cancer treatment: A review. Bio-Des. Manuf. 2022; in press. [Google Scholar] [CrossRef]
- Siuly, S.; Aickelin, U.; Kabir, E.; Huang, Z.; Zhang, Y. Guest Editorial: Special issue on “Artificial Intelligence in Health Informatics”. Health Inf. Sci. Syst. 2021, 9, 23. [Google Scholar] [CrossRef] [PubMed]
- Lohr, S. What Ever Happened to IBM’s Watson? The New York Times. 17 July 2021. Available online: https://www.nytimes.com/2021/07/16/technology/what-happened-ibm-watson.html (accessed on 18 February 2023).
- Zou, F.W.; Tang, Y.F.; Liu, C.Y.; Ma, J.A.; Hu, C.H. Concordance Study between IBM Watson for On-cology and Real Clinical Practice for Cervical Cancer Patients in China: A Retrospective Analysis. Front. Genet. 2020, 11, 200. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.N.N.; He, Z.; Leung, K.L.; To, C.C.K.; Wong, C.Y.; Wong, S.C.C.; Yoo, J.S.; Chan, C.K.R.; Chan, A.Z.; Lacambra, M.D.; et al. Current Developments of Artificial Intelligence in Digital Pathology and Its Future Clinical Applications in Gastrointestinal Cancers. Cancers 2022, 14, 3780. [Google Scholar] [CrossRef]
- Koh, D.M.; Papanikolaou, N.; Bick, U.; Illing, R.; Kahn, C.E.; Kalpathi-Cramer, J.; Matos, C.; Martí-Bonmatí, L.; Miles, A.; Mun, S.K.; et al. Artificial intelligence and machine learning in cancer imaging. Commun. Med. 2022, 2, 133. [Google Scholar] [CrossRef]
- Oren, O.; Gersh, B.J.; Bhatt, D.L. Artificial intelligence in medical imaging: Switching from radiographic pathological data to clinically meaningful endpoints. Lancet Digit. Health 2020, 2, e486–e488. [Google Scholar] [CrossRef]
- Kung, T.H.; Cheatham, M.; Medenilla, A.; Sillos, C.; De Leon, L.; Elepaño, C.; Madriaga, M.; Aggabao, R.; Diaz-Candido, G.; Maningo, J.; et al. Performance of ChatGPT on USMLE: Potential for AI-Assisted Medical Education Using Large Language Models. medRxiv 2022. [Google Scholar] [CrossRef]
- Clayton, B.J. Microsoft Unveils New Bing with ChatGPT Powers. BBC News. 7 February 2023. Available online: https://www.bbc.com/news/business-64562672?at_medium=RSS (accessed on 18 February 2023).
- Eurostat. One in Two EU Citizens Look for Health Information Online. 6 April 2021. Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/edn-20210406-1 (accessed on 18 February 2023).
- Sam Altman on. (11 December 2022). Twitter. Available online: https://mobile.twitter.com/sama/status/1601731295792414720?cxt=HHwWgICq9ZGIv7osAAAA (accessed on 18 February 2023).
- SPMS. ENESIS-20/22. 2019. Available online: https://www.spms.min-saude.pt/wp-content/uploads2019/10/ENESIS2022_VersaoParaConsultaPublicaOut2019.pdf (accessed on 29 December 2022).
- Krippendorf, K. Content Analysis: An Introduction to Its Methodology, 4th ed.; Sage Publication: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- PCM. Resolução do Conselho de Ministros 62/2016, 2016-10-17—DRE. 2016. Available online: https://dre.pt/dre/detalhe/resolucao-conselho-ministros/62-2016-7554212413/2/2023 (accessed on 18 February 2023).
- PCM. Resolução do Conselho de Ministros 108/2017, 2017-07-26—DRE. 2017. Available online: https://dre.pt/dre/detalhe/resolucao-conselho-ministros/108-2017-107757007 (accessed on 18 February 2023).
- SPMS. Sobre os Sistemas de Informação. 2023. Available online: https://www.spms.min-saude.pt/sobre-os-sistemas-de-informacao/ (accessed on 18 February 2023).
- Rahi, S.; Khan, M.M.; Alghizzawi, M. Factors influencing the adoption of telemedicine health services during COVID-19 pandemic crisis: An integrative research model. Enterp. Inf. Syst. 2021, 15, 769–793. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Interv. | Region | Organization | Regime | Profile (Position) | Profession | Age |
|---|---|---|---|---|---|---|
| E1-U | Azores | Praia and Vitoria Health Centre | Public | User | Computer Technician | -- |
| E2-P | Azores | Praia and Vitoria Health Centre | Public | Professional | Doctor | 41–51 |
| E3-M | Azores | Praia and Vitória Health Centre | Public | Professional (Clinical Director) | Doctor | <40 |
| E4-P | Azores | Praia and Vitória Health Centre | Public | Professional | Physician | <40 |
| E5-M | Algarve | Family Health Unit Sol Nascente | Public | Professional (Hospital Coordinator) | Doctor | >51 |
| E6-P | Algarve | Lusíadas Hospital | Private | Professional | Doctor | >51 |
| E7-M | Aveiro | Finess Medical Clinic | Private | Professional (Clinical Director) | Doctor | >51 |
| E8-P | Aveiro | Finess Medical Clinic | Private | Professional | Nurse | <40 |
| E9-P | Aveiro | Tâmega e Sousa Hospital Centre | Public | Professional | Doctor | <40 |
| E10-M | Aveiro | Ovar Hospital | Public | Professional (Chairman of the Board of Directors) | Manager | 41–51 |
| E11-M | Lisbon | Cascais Hospital | PPP | Professional (Chief Medical Information Officer) | Doctor | 41–51 |
| E12-M | Lisbon | Cascais Hospital | PPP | Professional (Chief Nursing Information Officer) | Nurse | 41–51 |
| E13-GE | Lisbon | Shared Services of the Ministry of Health | Public | Government Entity (President) | Manager/Doctor | 41–51 |
| E14-U | Faro | Retired | Public | User | Nurse | >51 |
| Categories of Ecosystem of His (ESIS) | Designation | Description |
|---|---|---|
| Transversal of all NHS (National health service) | RNU; SER; SNS24; SINAVE | These HIS have the role of centralizing and distribution of information for NHS users |
| Life Cycle—Birth | Birth News; to Birth Citizen, Health Child’s Bulletin and Youth’s Health Bulletin and, eBulletin of Vaccines. | To receive a new citizen in society and, to monitor him/she in terms of surveillance and/or monitoring of public health |
| Life Cycle—Health and Wellness | Daily of My Health, SISO, SIIMA; SClínic CSP, RENTEV and others | This cycle comprises the systems that accompany citizens in a perspective of prevention and promotion of health |
| Life Cycle—Acute or Chronic Disease | ICC, Sclinic Hospital, SClinic CSP; RCU2, SINAVE, PEM, SI VIDA; RNCCI; and, CNTS | These HIS serve to accompany the user in his/her disease process, allowing the recording, diagnosis, and treatments, in all clinical episodes |
| Life Cycle—Aging | RECM; RNCCI. | HIS is intended to support clinical practice in the adoption and maintenance of healthy life models by the elderly |
| Life Cycle—Death | SICO | The main objective is dematerializing the process of certification of deaths and better articulation between the entities involved in the process. |
| Medical Practices | Pessimist | Realist | Optimistic |
|---|---|---|---|
| Precision Medicine/Individualized | The costs (financial and adaptation) are enormous, and for this reason, it will not be the usual practice. | It will be used to solve serious and critical diseases, where the cost/benefit justifies it. | Medicine will be fully focused on the citizen, with better accuracy in the personalized diagnoses and treatments. |
| Preventive medicine | Those responsible for the health area still have difficulties adapting to a reality focused on prevention. | Health officials will try to make health digital, with a focus on health rather than a disease, optimizing the entire HS. | The practice of medicine is focused on prevention and health promotion. |
| Point-of-Care (Telemedicine) | It is already a current practice when distance obliges. One should bet on its development. | Telemedicine will be used regularly, regardless of distance, and more focused on solving the problems of the citizen. | Telemedicine will be used frequently, facilitating the sharing of information between professionals for cases of complex diagnosis, and the citizen will have privileged consultations with healthcare professionals through Telemedicine and Telehealth. |
| Assisted Medical Practices | Healthcare professionals will have digital assistants who will help make diagnoses, but the presence of the health professional will be required. | Healthcare professionals, in some diagnoses, will be replaced by machines. The use of machines (robots) to help some medical practices (e.g., surgeries) will be more common. | The diagnoses will be made by machines, and these machines (robots) will replace healthcare professionals in clinical practices, such as surgeries. |
| Technologies | Pessimist | Realist | Optimistic |
|---|---|---|---|
| Interoperability (integration) | Health organizations (public and private), due to the existence of legacy systems or heterogeneous HISs, do not allow interoperability of the systems. Thus, the sharing of a citizen’s health data between several entities will be a distant reality. | Health organizations (public and private) collaborate in defining a set of shared services that allows the integration and access of a citizen’s EHRs. | HIS providers adopt international, European, and national recommendations, enabling interoperability between existing HISs and facilitating the sharing of EHR between different health organizations, respecting existing (legislation) standards. |
| Digital Health Transformation | It will occur when health organizations/entities (public and private) can change/innovate their processes, improve their leadership, and reduce resistance. | There are health organizations/entities (public and private) that innovate their processes, achieving significant efficiency gains. These cases will be examples to follow by other entities. | Health organizations/entities (public and private) present advanced dematerialization with significant gains in process performance. Success stories are shared and replicated. |
| Technology to Assist Medical Practices | Gradually technology that incorporates intelligence will be applied in the HIS; there is a need to create legitimacy for this to happen. Health professionals will resist but will eventually adopt the technologies. | The technology is currently able to assist professionals in medical practices. However, there are still obstacles to overcome: legitimation (legislation) and acceptance by all involved (health professionals and citizens) of the existed possibilities and limitations. | Health organizations and professionals perceive the positive side of incorporating intelligent technology and force legitimation (legislation) to occur. Intelligent technology, being incorporated into all medical processes and practices, leads to a huge efficiency gain and cost reduction. |
| Use of wearables | There are more and more devices able to collect data on citizens’ health. However, these data will not be used without regulation to process it. On the other hand, the existent healthcare services do not have the capacity to treat such data. | The collection of device-generated data is already a reality, and it does not raise technical issues; it is a matter of work, standards, and interoperability. The legitimacy of these systems and devices will occur, and healthcare models will adapt to this reality. | In the short term, legislation will be created to enable the collection and use of health data from electronic devices. Clinical practices will already use these data to promote models of healthy living for citizens. |
| Challenges and Risks | Pessimist | Realist | Optimistic |
|---|---|---|---|
| Changing the existing culture (resistance to change among users and health professionals) | It will only occur when all stakeholders can understand the benefits to be obtained and realize that they will have to change/innovate their processes, and this will be a time-consuming process. | Health and care processes need to be innovated. There is little research and literature in this area. It is necessary to study the way care is organized and identify advantages and benefits causing changes in culture. Technology is a means and not the solution. | Healthcare delivery models will be studied and changed by accommodating emerging technologies with a positive and high impact on citizens’ health. |
| Info Exclusion (Training) | There is a need to simplify and disseminate the HIS, mainly those that are in place and those that will appear in the future, and the advantage of their use (to health professionals and citizens). It will be necessary to reduce digital illiteracy, mainly among older people. | Copying good practices successfully implemented by some organizations (training, monitoring, and involving all stakeholders), showing the advantages/benefits of using it. | All entities realize the advantages/benefits of using technological solutions and increasingly seek technological solutions to solve their problems. |
| Information (privacy, quality, security) | Legislation is needed to regulate the collection, access, treatment, and security of health information. This will be one of the biggest challenges of the next years. | The question of legitimacy (legislation) will be resolved quickly (by national or European directives). The next step will be to ensure the quality and security of this information so that all stakeholders maintain confidence in it. | The collection, access, and sharing of health data will already be sufficiently regulated to maintain high standards of data security and privacy. All stakeholders (within their legitimacy) can add and share health information with confidence with other entities. |
| Key Factors to Address | Number of Interviewers Who Referenced It |
|---|---|
| Interoperability | 4 (29%) |
| Standardization | 3 (21%) |
| Privacy | 6 (43%) |
| Security | 7 (50%) |
| Actions to address info exclusion | 12 (86%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teixeira, L.; Cardoso, I.; Oliveira e Sá, J.; Madeira, F. Are Health Information Systems Ready for the Digital Transformation in Portugal? Challenges and Future Perspectives. Healthcare 2023, 11, 712. https://doi.org/10.3390/healthcare11050712
Teixeira L, Cardoso I, Oliveira e Sá J, Madeira F. Are Health Information Systems Ready for the Digital Transformation in Portugal? Challenges and Future Perspectives. Healthcare. 2023; 11(5):712. https://doi.org/10.3390/healthcare11050712
Chicago/Turabian StyleTeixeira, Leonor, Irene Cardoso, Jorge Oliveira e Sá, and Filipe Madeira. 2023. "Are Health Information Systems Ready for the Digital Transformation in Portugal? Challenges and Future Perspectives" Healthcare 11, no. 5: 712. https://doi.org/10.3390/healthcare11050712