
Impact of Preexisting Alcohol Use Disorder, Bipolar Disorder, and Schizophrenia on Ischemic Stroke Risk and Severity: A Lebanese Case-Control Study



Abstract
:1. Background
1.1. Ischemic Stroke: Etiology and Disease Burden
1.2. Overview of Bipolar Disease, Schizophrenia, and Alcohol Use Disorder
1.3. Studies Linking These Diseases to an Increased Ischemic Stroke Risk
1.4. Studies Linking These Diseases to an Increased Ischemic Stroke Severity
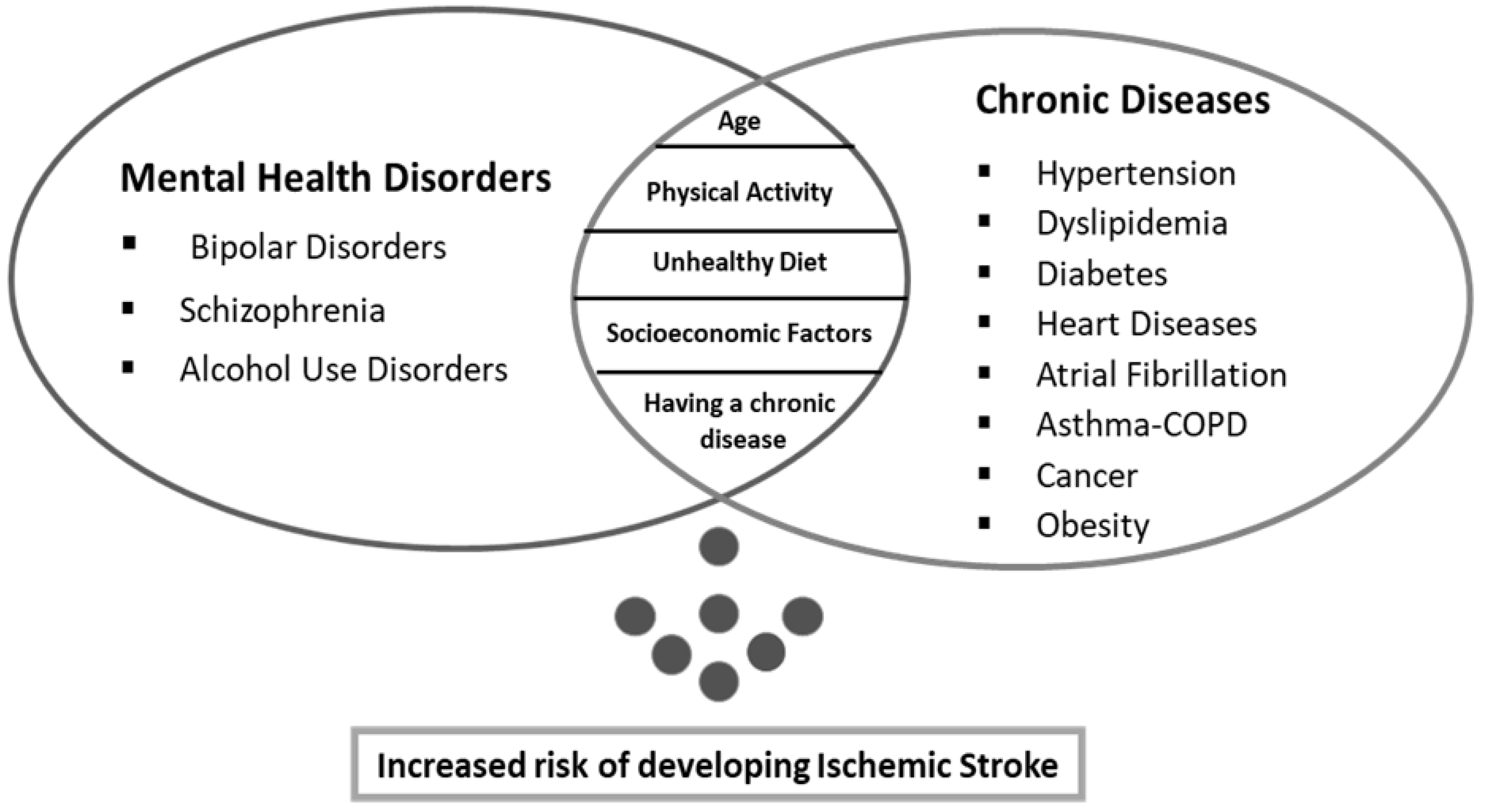
1.5. Rationale and Objectives of the Study
2. Methods
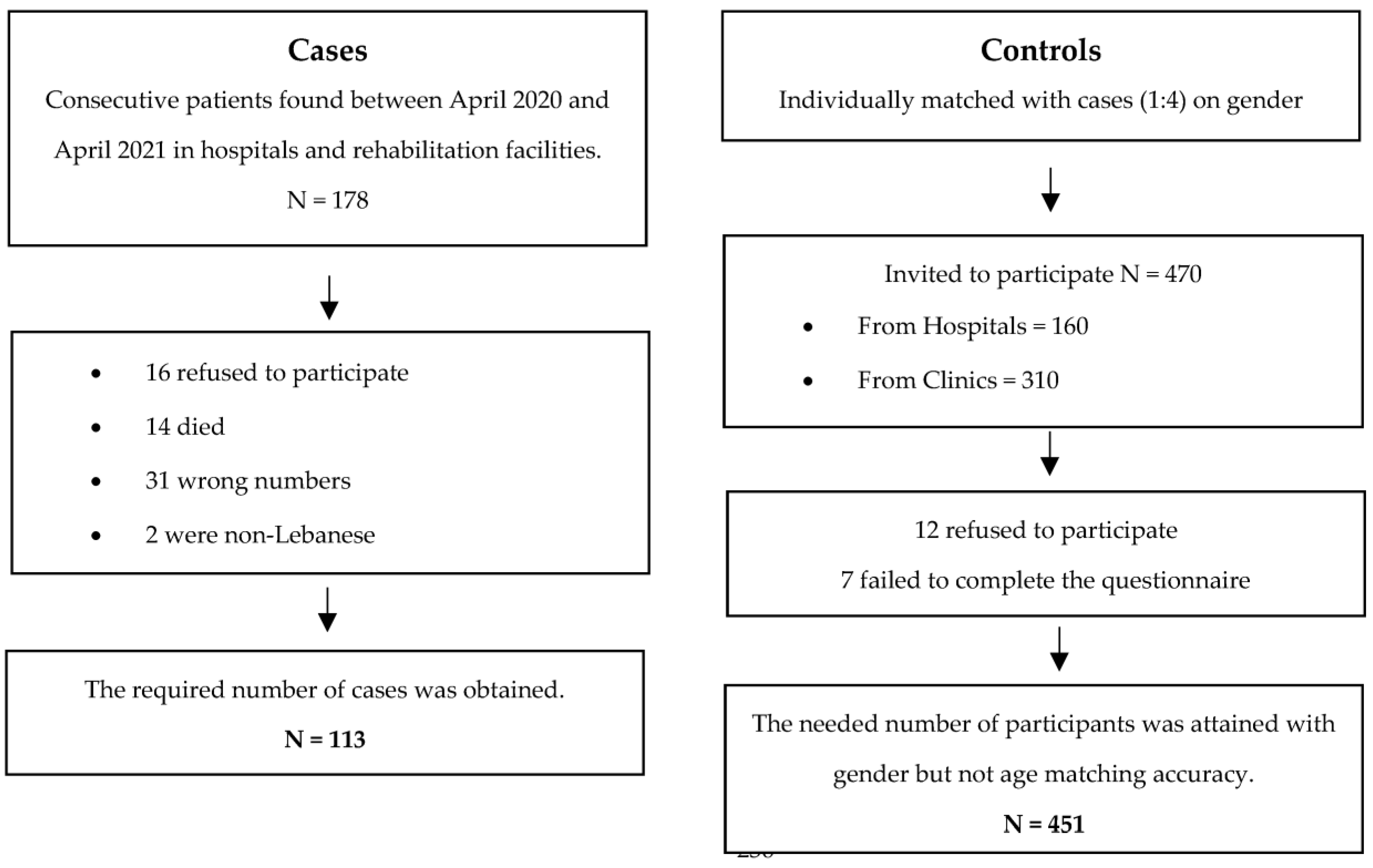
2.1. Study Design
2.2. Minimal Sample Size Calculation
2.3. Questionnaire and Variables
- maintaining a healthy body weight by assessing the body mass index (BMI),
- following a healthy diet, as measured by the Mediterranean diet (MeD) adherence:
- being physically active by evaluating the international physical activity questionnaire (IPAQ)–short version:
- ▪
- The alcohol use disorder (AUD) was evaluated using the alcohol use disorder identification test (AUDIT). This is a 10-item validated questionnaire developed by the World Health Organization (WHO) to assess alcohol consumption, drinking behaviors, and alcohol-related problems defined as risky or hazardous consumption or any AUD [51]. A score of 8 or higher indicates risky or harmful alcohol use [52] (Cronbach’s α in this study = 0.733).
- ▪
- The BD was assessed using the mood disorder questionnaire (MDQ). The MDQ is a 15-item self-report screening instrument that is most sensitive to bipolar I (depression and mania) disorder and less sensitive to bipolar II (depression and hypomania), or bipolar not otherwise specified (NOS) disorder [53]. It has 13 yes/no questions about bipolar symptoms and two more about symptom co-occurrence and impaired functioning. A total score is calculated for questions 1–13, with “Yes” providing a score of 1 and “No” providing a score of 0. The traditional scoring method for reaching the BD threshold is as follows:
- ○
- A score of 7 or higher on questions 1–13 AND,
- ○
- Select “yes” for the item requesting whether the symptoms occurred at the same time (Question 14) AND,
- ○
- Symptoms caused either “moderate” or “serious” problems (Question 15),
- ○
- (Cronbach’s α in this study = 0.887).
- ▪
- Schizophrenia was assessed using the mini international neuropsychiatric interview (MINI) for psychotic disorders studies for the DSM-5 diagnostic criteria for schizophrenia [54]. Questions are phrased to allow only “yes” or “no” answers. It describes the five major symptoms of psychotic disorders: (1) delusions, (2) hallucinations, (3) disorganized speech, (4) disorganized or catatonic behavior, and (5) negative symptoms. Schizophrenia diagnosis requires the detection of two (or more) of the aforementioned symptoms, each of which must be present for a significant portion of time during a one-month period (or less if successfully treated), with at least one of them being (1), (2), or (3).
2.4. Translation Procedure
2.5. Statistical Analysis
3. Results
3.1. Effect of the Variables on Ischemic Stroke Risk
3.1.1. Demographic Data of Patients with Ischemic Stroke and the Control Group (N = 564)
3.1.2. Bivariate Analysis of Other Factors Associated with Ischemic Stroke
3.1.3. Multivariable Analysis: Logistic Regression
3.2. Effect of the Variables on Stroke Severity
3.2.1. Bivariate Analysis of the Variables Associated with the Levels of Stroke Severity
3.2.2. Multivariable Analysis: Multinomial Regression
4. Discussion
5. Limitations and Strengths
6. Clinical Implications
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BD | Bipolar Disorder |
| AUD | Alcohol Use Disorder |
| MeD | Mediterranean Diet |
| SPSS | Statistical Package for Social Science |
Appendix A
Questionnaire Form: English Version
- I.
- Socio-Demographic Information:
- Gender: □ M □ F
- Age: ………….
- Weight: ……….
- Height: …………
- Marital status: □ Single □ Married □ Divorced □ Widower
- Educational Level: □ Elementary □ Intermediate □ Secondary □ University □ Illiterate
- Work Status: □ Works □ Jobless □ Retired/Housewife
- Monthly Income: □ <USD 1000 □ USD 1000–2000 □ USD >2000
- Health Coverage: □ Social Security □ Personal Medical Insurance □ State Employees Cooperative □ Personal Account
- Region: □ Beirut □ South □ Mount Lebanon □ Bekaa □ North
- II.
- Personal Clinical Factors
- Has a “physician” ever diagnosed you with:
- Hypertension:□ Yes □ No □ I don’t know/I’m not sure
- Dyslipidemia:□ Yes □ No □ I don’t know/I’m not sure
- Diabetes:□ Yes □ No □ I don’t know/I’m not sure
- Any type of heart disease:□ Yes □ No □ I don’t know/I’m not sure
- Atrial fibrillation:□ Yes □ No □ I don’t know/I’m not sure
- Respiratory problem (Specifically: Asthma, COPD):□ Yes □ No □ I don’t know/I’m not sure
- Cancer:□ Yes □ No □ I don’t know/I’m not sure
- Stroke:□ Yes □ No □ I don’t know/I’m not sureIf YES:h.1.Date of Stroke: From _____ week(s)h.2. Stroke Type:□ Ischemic stroke□ Hemorrhagic stroke□ Transient ischemic attackh.3. Diagnosis:□ Complete blood count□ Clotting time PT (prothrombin time) and PTT (partial thromboplastin time)□ Computerized tomography (CT) scan□ Magnetic resonance imaging (MRI)□ Carotid ultrasound□ Echocardiogram□ Transient ischemic attack□ Angiograms of your head and neckh.4. Stroke Severity: National Institutes of Health Stroke Scale (NIHSS):□ 0 = No stroke□ 1–4 = Minor stroke□ 5–15 = Moderate stroke□ 16–20 = Moderate to Severe stroke□ 21–42 = Severe strokeh.5. Time of Hospital Stay (if possible): _____ daysh.6. Stroke Complications:□ Paralysis or loss of ability to move muscles□ Difficulty speaking or swallowing□ Memory loss or problems with general comprehension□ Aches
- Questionnaire of Mediterranean Diet Adherence
Yes No 1.Is olive oil the main culinary fat used? 2. Are ≥ 4 tablespoons of olive oil used each day? 3. Are ≥ 2 servings (of 200 g each) of vegetables eaten each day? 4. Are ≥ 3 servings of fruit (of 80 g each) eaten each day? 5. Is < 1 serving (100–150 g) of red meat/hamburgers/other meat products eaten each day? 6. Is < 1 serving (12 g) of butter, margarine or cream eaten each day? 7. Is < 1 serving (330 mL) of sweet or sugar sweetened carbonated beverages consumed each day? 8. Are ≥ 3 glasses (of 125 mL) of wine consumed each week? 9. Are ≥ 3 servings (of 150 g) of legumes consumed each week? 10. Are ≥ 3 servings of fish (100–150 g) or seafood (200 g) eaten each week? 11. Are < 3 servings of commercial sweets/pastries eaten each week? 12. Is ≥ 1 serving (of 30 g) of nuts consumed each week? 13. Is chicken, turkey, or rabbit routinely eaten instead of veal, pork, hamburger, or sausage? 14. Are pasta, vegetables, or rice dishes flavoured with garlic, tomato, leek, or onion eaten ≥ twice a week? - (a)
- Have you exercised or been involved in sports or physical activity in the past 12 months?□ Y □ N
- (b)
- If your answer is yes to question a, what is the intensity of physical activity?
- Continuous heavy breathing with perspiration b. Heavy intermittent breathing with perspiration (tennis, basketball) c. Moderate to severe (recreational sports, cycling) d. Moderate (volleyball) e. Mild (fishing, walking).
- International Physical Activity Questionnaire (IPAQ)We are interested in finding out about the kinds of physical activities that you do as part of your everyday life. The questions will ask you about the time you spent being physically active in the last 7 days. Please answer each question even if you do not consider yourself to be an active person.
- During the last 7 days, on how many days did you do vigorous physical activities, such as heavy lifting, digging, aerobics, or fast bicycling?_____ days per week□ No vigorous physical activities → Skip to question 3
- How much time did you spend doing vigorous physical activities on one of those days?_____ hours per day _____ minutes per day□ Don’t know/Not sure
- During the last 7 days, on how many days did you do moderate physical activities, such as carrying light loads, bicycling at a regular pace, or doubles tennis? Do not include walking._____ days per week□ No moderate physical activities → Skip to question 5
- How much time did you spend doing moderate physical activities on one of those days?_____ hours per day _____ minutes per day□ Don’t know/Not sure
- During the last 7 days, on how many days did you walk for at least 10 min at a time?_____ days per week□ No walking → Skip to question 7
- How much time did you spend walking on one of those days?_____ hours per day _____ minutes per day□ Don’t know/Not sure
- During the last 7 days, how much time did you spend sitting on a week day?_____ hours per day _____ minutes per day□ Don’t know/Not sure
- III.
- Assessment of Mental Health- Do you have a psychiatrist diagnosis of:□ Alcohol Use Disorder □ Bipolar Disorder □ Schizophrenia- OR how often have you been bothered by any of the following problems?
- The Alcohol Use Disorders Identification Test (AUDIT)
How often do you have a drink containing alcohol?□ Never □ Monthly or less □ 2–4 times a month □ 2–3 times a week □ 4 or more times a week How many standard drinks containing alcohol do you have on a typical day when drinking? □ 1 or 2 □ 3 or 4 □ 5 or 6 □ 7 to 9 □ 10 or more How often do you have six or more drinks on one occasion?□ Never □ Less than monthly □ Monthly □ Weekly □ Daily or almost daily During the past year, how often have you found that you were not able to stop drinking once you had started?□ Never □ Less than monthly □ Monthly □ Weekly □ Daily or almost daily During the past year, how often have you failed to do what was normally expected of you because of drinking?□ Never □ Less than monthly □ Monthly □ Weekly □ Daily or almost daily During the past year, how often have you needed a drink in the morning to get yourself going after a heavy drinking session?□ Never □ Less than monthly □ Monthly □ Weekly □ Daily or almost daily During the past year, how often have you had a feeling of guilt or remorse after drinking?□ Never □ Less than monthly □ Monthly □ Weekly □ Daily or almost daily During the past year, have you been unable to remember what happened the night before because you had been drinking?□ Never □ Less than monthly □ Monthly □ Weekly □ Daily or almost daily Have you or someone else been injured as a result of your drinking?□ No □ Yes, but not in the past year □ Yes, during the past year Has a relative or friend, doctor, or other health worker been concerned about yourdrinking or suggested you cut down?□ No □ Yes, but not in the past year □ Yes, during the past year - The Mood Disorder Questionnaire (MDQ)
1.Has there ever been a period of time when you were not your usual self and Yes No you felt so good or so hyper that other people thought you were not your normal self, or you were so hyper that you got into trouble? you were so irritable that you shouted at people or started fights or arguments? you felt much more self-confident than usual? you had much less sleep than usual and found you didn’t really miss it? you were much more talkative or spoke much faster than usual? thoughts raced through your head or you couldn’t slow your mind down? you were so easily distracted by things around you that you had trouble concentrating or staying on track? you had much more energy than usual? you were much more active or did many more things than usual? you were much more social or outgoing than usual, for example, you telephoned friends in the middle of the night? you were much more interested in sex than usual? you did things that were unusual for you or that other people might have thought were excessive, foolish, or risky? spending money got you or your family into trouble? - 2.
If you checked YES to more than one of the above, have several of these ever happened during the same period of time?□ Yes □ No- 3.
How much of a problem did any of these cause you, such as being unable to work; having family, money or legal troubles; getting into arguments or fights? Please circle one response only.□ No Problem □ Minor Problem □ Moderate Problem □ Serious Problem- 4.
Have any of your blood relatives (i.e., children, siblings, parents, grandparents, aunts, uncles) had manic-depressive illness or bipolar disorder?□ Yes □ No- 5.
Has a health professional ever told you that you have manic-depressive illness or bipolar disorder?□ Yes □ No - Mini International Neuropsychiatric Interview (MINI) for Psychotic DisordersAsk for an example of each question answered positively. Code yes only if the examples clearly show a distortion of thought or of perception or if they are not culturally appropriate.Now I am going to ask you about unusual experiences that some people have.
- (a) Have you ever believed that people were spying on you, or that someone was plotting against you, or trying to hurt you? □ No □ Yes(b) IF YES: do you currently believe these things?
- (a) Have you ever believed that someone was reading your mind or could hear your thoughts, or that you could actually read someone’s mind or hear what another person was thinking? □ No □ Yes(b) IF YES: do you currently believe these things?
- (a) Have you ever believed that someone or some force outside of yourself put thoughts in your mind that were not your own, or made you act in a way that was not your usual self? Have you ever felt that you were possessed? □ No □ Yes(b) IF YES: do you currently believe these things?
- (a) Have you ever believed that you were being sent special messages through the TV, radio, internet, newspapers, books, or magazines or that a person you did not personally know was particularly interested in you? □ No □ Yes(b) IF YES: do you currently believe these things?
- (a) Have your relatives or friends ever considered any of your beliefs odd or unusual? □ No □ Yes(b) IF YES: do they currently consider your beliefs strange or unusual?
- (a) Have you ever heard things other people couldn’t hear, such as voices? □ No □ Yes(b) IF YES TO VOICE HALLUCINATION: Was the voice commenting on your thoughts or behavior or did you hear two or more voices talking to each other?(a) IF YES: have you heard sounds/voices in the past month?(b) IF YES: Was the voice commenting on your thoughts or behavior or did you hear two or more voices talking to each other? □ No □ Yes
- (a) Have you ever had visions when you were awake or have you ever seen things other people couldn’t see? □ No □ Yes(b) IF YES: have you seen these things in the past month? □ No □ YesCLINICIAN’S JUDGMENT:
- (a) Did the patient ever in the past exhibit disorganized, incoherent or derailed speech, or marked loosening of associations? □ No □ Yes(b) Is the patient currently exhibiting incoherence, disorganized or derailed speech, or marked loosening of associations? □ No □ Yes
- (a) Did the patient ever in the past exhibit disorganized or catatonic behavior? □ No □ Yes(b) Is the patient currently exhibiting disorganized or catatonic behavior? □ No □ Yes
- (a) Did the patient ever in the past have negative symptoms, e.g., significant reduction of emotional expression or affective flattening, poverty of speech (alogia) or an inability to initiate or persist in goal-directed activities (avolition)? □ No □ Yes(b) Are negative symptoms of schizophrenia, e.g., significant reduction of emotional expression or affective flattening, poverty of speech (alogia), or an inability to initiate or persist in goal-directed activities (avolition), prominent during the interview?□ No □ Yes
- (a) Are 1 or more “a” questions from 1a to 7a, coded YES?And is either:MAJOR DEPRESSIVE EPISODE, (current, recurrent, or past)ORMANIC OR HYPOMANIC EPISODE, (current or past) coded YES?ANDHow long has the mood episode lasted? _______________How long has the psychotic episode lasted? _______________If such a mood episode is present, code YES to 11a only if the mood disturbance is present for the majority of the total duration of the active and residual periods of the psychotic symptoms. Otherwise, code NO.□ No □ Yes
References
- Katan, M.; Luft, A. Global Burden of Stroke. Semin. Neurol. 2018, 38, 208–211. [Google Scholar] [CrossRef] [PubMed]
- American Stroke Association. Ischemic Strokes (Clots). Available online: https://www.stroke.org/en/about-stroke/types-of-stroke/ischemic-stroke-clots (accessed on 9 September 2022).
- Ntaios, G. Embolic Stroke of Undetermined Source: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2020, 75, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Pierik, R.; Algra, A.; van Dijk, E.; Erasmus, M.E.; van Gelder, I.C.; Koudstaal, P.J.; Luijckx, G.R.; Nederkoorn, P.J.; van Oostenbrugge, R.J.; Ruigrok, Y.M.; et al. Distri-bution of Cardioembolic Stroke: A Cohort Study. Cereb. Dis. 2020, 49, 97–104. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Mueser, K.T.; McGurk, S.R. Schizophrenia. Lancet 2004, 363, 2063–2072. [Google Scholar] [CrossRef]
- Harris, E.C.; Barraclough, B. Excess mortality of mental disorder. Br. J. Psychiatry 1998, 173, 11–53. [Google Scholar] [CrossRef]
- Meloni, D.; Miccinesi, G.; Bencini, A.; Conte, M.; Crocetti, E.; Zappa, M.; Ferrara, M. Mortality among discharged psychiatric patients in Florence, Italy. Psychiatr. Serv. 2006, 57, 1474–1481. [Google Scholar] [CrossRef]
- Miller, B.J.; Paschall, C.B., 3rd; Svendsen, D.P. Mortality and medical comorbidity among patients with serious mental illness. Psychiatr. Serv. 2006, 57, 1482–1487. [Google Scholar] [CrossRef]
- Brown, S.; Kim, M.; Mitchell, C.; Inskip, H. Twenty-five year mortality of a community cohort with schizo-phrenia. Br. J. Psychiatry 2010, 196, 116–121. [Google Scholar] [CrossRef]
- Saha, S.; Chant, D.; McGrath, J. A systematic review of mortality in schizophrenia: Is the differential mortality gap worsening over time? Arch. Gen. Psychiatry 2007, 64, 1123–1131. [Google Scholar] [CrossRef]
- Roshanaei-Moghaddam, B.; Katon, W. Premature mortality from general medical illnesses among persons with bipolar disorder: A review. Psychiatr. Serv. 2009, 60, 147–156. [Google Scholar] [CrossRef]
- Rosen, C.S.; Kuhn, E.; Greenbaum, M.A.; Drescher, K.D. Substance abuse-related mortality among middle-aged male VA psychiatric patients. Psychiatr. Serv. 2008, 59, 290–296. [Google Scholar] [CrossRef]
- Lawrence, D.; Kisely, S.; Pais, J. The Epidemiology of Excess Mortality in People with Mental Illness. Can. J. Psychiatry 2010, 55, 752–760. [Google Scholar] [CrossRef]
- Eringen, P.A.; Engh, J.A.; Birkenaes, A.B.; Edieset, I.; Andreassen, O.A. Increased Mortality in Schizophrenia Due to Cardiovascular Disease – A Non-Systematic Review of Epidemiology, Possible Causes, and Interventions. Front. Psychiatry 2014, 5, 137. [Google Scholar] [CrossRef]
- Correll, C.U.; Solmi, M.; Veronese, N.; Bortolato, B.; Rosson, S.; Santonastaso, P.; Thapa-Chhetri, N.; Fornaro, M.; Gallicchio, D.; Collantoni, E.; et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: A large-scale meta-analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry 2017, 16, 163–180, Erratum in: World Psychiatry 2018, 17, 120. [Google Scholar] [CrossRef]
- Zoghbi, M.; Haddad, C.; Salameh, P.; Haddad, G.; Hallit, S. Untreated Dyslipidemia in Lebanese Patients With Schizophrenia. Prim. Care Companion CNS Disord. 2017, 19, 26970. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, R.C.; Boire, M.D.; Lazo, R.G.; McKenzie, K.; Cohn, T. Schizophrenia and the incidence of cardiovascular morbidity: A population-based longitudinal study in Ontario, Canada. Schizophr. Res. 2009, 115, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Sharma, B.B.; Singh, S.; Sharma, V.K.; Choudhary, M.; Singh, V.; Lane, S.; Lepping, P.; Krishna, M.; Copeland, J. Psychiatric morbidity in chronic respiratory disorders in an Indian service using GMHAT/PC. Gen. Hosp. Psychiatry 2013, 35, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Nanda, S.; Chaudhary, S.C.; Tripathi, A.; Sawlani, K.K.; Gupta, K.K.; Himanshu, D.; Verma, A.K. Prevalence of psychiatric comorbidities in chronic obstructive pulmonary disease patients. Lung India 2016, 33, 174–178. [Google Scholar] [CrossRef]
- Krishnan, K.R. Psychiatric and medical comorbidities of bipolar disorder. Psychosom. Med. 2005, 67, 1–8. [Google Scholar] [CrossRef]
- Curkendall, S.M.; Mo, J.; Glasser, D.B.; Stang, M.R.; Jones, J.K. Cardiovascular Disease in Patients With Schizophrenia in Saskatchewan, Canada. J. Clin. Psychiatry 2004, 65, 715–720. [Google Scholar] [CrossRef]
- Chiu, Y.C.; Bai, Y.M.; Su, T.P.; Chen, T.J.; Chen, M.H. Ischemic Stroke in Young Adults and Preexisting Psychiatric Disorders: A Nationwide Case-Control Study. PubMed 2015, 94, e1520. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.-C.; Hsiao, F.-H.; Pfeiffer, S.; Hwang, Y.-T.; Lee, H.-C. An increased risk of stroke among young schizophrenia patients. Schizophr. Res. 2008, 101, 234–241. [Google Scholar] [CrossRef]
- Lin, H.-C.; Tsai, S.-Y.; Lee, H.-C. Increased risk of developing stroke among patients with bipolar disorder after an acute mood episode: A six-year follow-up study. J. Affect. Disord. 2007, 100, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, K.; Lewis, B.; Nolen, J.D.L.; Kinney, G.L.; Sathya, B.; He, J. Alcohol Consumption and Risk of Stroke: A Meta-analysis. JAMA 2003, 289, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.; Gandhi, Z.; Desai, R.; Raina, J.; Itare, V.; Haque, F.A.; Saeed, T.; Gupta, N.; Mansuri, Z.; Sachdeva, R.; et al. Impact of alcohol use disorder on stroke risk in geriatric patients with prediabetes: A nationwide analysis. Int. J. Clin. Pract. 2021, 75, e14477. [Google Scholar] [CrossRef]
- Li, M.; Fan, Y.-L.; Tang, Z.-Y.; Cheng, X.-S. Schizophrenia and risk of stroke: A meta-analysis of cohort studies. Int. J. Cardiol. 2014, 173, 588–590. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.-C.; Chou, F.H.-C.; Tsai, K.-Y.; Su, C.-Y.; Shen, S.-P.; Chung, T.-C. The Incidence and Relative Risk of Stroke among Patients with Bipolar Disorder: A Seven-Year Follow-Up Study. PLoS ONE 2013, 8, e73037. [Google Scholar] [CrossRef]
- Nilsson, F.M.; Kessing, L.V. Increased risk of developing stroke for patients with major affective disorder—A registry study. Eur. Arch. Psychiatry Clin. Neurosci. 2004, 254, 387–391. [Google Scholar] [CrossRef]
- Hoyer, C.; Schmidt, H.L.; Kranaster, L.; Alonso, A. Impact of psychiatric comorbidity on the severity, short-term functional outcome, and psychiatric complications after acute stroke. Neuropsychiatr. Dis. Treat. 2019, 15, 1823–1831. [Google Scholar] [CrossRef]
- Willers, C.; Sunnerhagen, K.S.; Lekander, I.; Von Euler, M. The Association of Pre-stroke Psychosis and Post-stroke Levels of Health, Resource Utilization, and Care Process: A Register-Based Study. Front. Neurol. 2018, 9, 1042. [Google Scholar] [CrossRef]
- Fleetwood, K.; Wild, S.H.; Smith, D.J.; Mercer, S.W.; Licence, K.; Sudlow, C.L.M.; Jackson, C.A. Association of severe mental illness with stroke outcomes and process-of-care quality indicators: Nationwide cohort study. Br. J. Psychiatry 2022, 221, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Shiotsuki, H.; Saijo, Y.; Ogushi, Y.; Kobayashi, S.; Japan Standard Stroke Registry Study Group. Relationships between Alcohol Intake and Ischemic Stroke Severity in Sex Stratified Analysis for Japanese Acute Stroke Patients. J. Stroke Cerebrovasc. Dis. 2019, 28, 1604–1617. [Google Scholar] [CrossRef] [PubMed]
- Shiotsuki, H.; Saijo, Y.; Ogushi, Y.; Kobayashi, S. Relationship between Alcohol Intake and Stroke Severity in Japanese Patients: A Sex- and Subtype-Stratified Analysis. J. Stroke Cerebrovasc. Dis. 2022, 31, 106513. [Google Scholar] [CrossRef] [PubMed]
- WHO Lebanon. 2019. Available online: http://www.who.int/countries/lbn/en/ (accessed on 30 September 2022).
- Lahoud, N.; Salameh, P.; Saleh, N.; Hosseini, H. Prevalence of Lebanese stroke survivors: A comparative pilot study. J. Epidemiol. Glob. Health 2016, 6, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Lahoud, N.; Abbas, M.H.; Salameh, P.; Saleh, N.; Abes, S.; Hosseini, H.; Gebeily, S. A retrospective analysis of 254 acute stroke cases admit-ted to two university hospitals in Beirut: Classification and associated factors. Funct. Neurol. 2017, 32, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Malek, E.G.; Elbejjani, M.; Abbas, R.; Al Ahad, M.A.; Isma’Eel, H.; Makki, A. TOAST classification and risk factors of ischemic stroke in Lebanon. Acta Neurol. Scand. 2020, 141, 294–300. [Google Scholar] [CrossRef]
- Matar, D.; Frangieh, A.H.; Abouassi, S.; Bteich, F.; Saleh, A.; Salame, E.; Kassab, R.; Azar, R.R. Prevalence, awareness, treatment, and control of hyper-tension in Lebanon. J. Clin. Hypertens. 2015, 17, 381–388. [Google Scholar] [CrossRef]
- Fahs, I.; Khalife, Z.; Malaeb, D.; Iskandarani, M.; Salameh, P. The prevalence and awareness of cardiovascular diseases risk fac-tors among the Lebanese population: A prospective study comparing urban to rural populations. Cardiol. Res. Pract. 2017, 2017, 10. [Google Scholar] [CrossRef]
- Czap, A.L.; Sheth, S.A. Overview of Imaging Modalities in Stroke. Neurology 2021, 97, S42–S51. [Google Scholar] [CrossRef]
- American Stroke Association. Together to End Stroke [Internet] American Stroke Association. 2013. Available online: http://www.strokeassociation.org/STROKEORG/AboutStroke/TypesofStroke/Types-of-Stroke_UCM_308531_SubHomePage.jsp (accessed on 1 October 2022).
- Maalouf, E.; Hallit, S.; Salameh, P.; Hosseini, H. Eating Behaviors, Lifestyle, and Ischemic Stroke: A Lebanese Case-Control Study. Int. J. Environ. Res. Public Health 2023, 20, 1487. [Google Scholar] [CrossRef]
- Karam, E.G.; Mneimneh, Z.N.; Karam, A.N.; Fayyad, J.A.; Nasser, S.; Chatterji, S.; Kessler, R.C. Prevalence and treatment of mental disorders in Lebanon: A national epidemiological survey. Lancet 2006, 367, 1000–1006. [Google Scholar] [CrossRef]
- Zuflacht, J.P.; Shao, Y.; Kronish, I.M.; Edmondson, D.; Elkind, M.S.; Kamel, H.; Boehme, A.K.; Willey, J.Z. Psychiatric Hospitalization Increases Short-Term Risk of Stroke. Stroke 2017, 48, 1795–1801. [Google Scholar] [CrossRef] [PubMed]
- Hage, V. The NIH stroke scale: A window into neurological status. Nurs. Spectr. 2011, 24, 44–49. [Google Scholar]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-Item Mediterranean Diet Assessment Tool and Obesity Indexes among High-Risk Subjects: The PREDIMED Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef]
- IPAQ. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ). [Online] The In-ternational Physical Activity Questionnaire. 2005. Available online: http://www.ipaq.ki.se/scoring.pdf (accessed on 1 August 2022).
- Hallit, J.; Salameh, P.; Haddad, C.; Sacre, H.; Soufia, M.; Akel, M.; Obeid, S.; Hallit, R.; Hallit, S. Validation of the AUDIT scale and factors associated with alcohol use disorder in adolescents: Results of a National Lebanese Study. BMC Pediatr. 2020, 20, 205. [Google Scholar] [CrossRef] [PubMed]
- Bohn, M.J.; Babor, T.F.; Kranzler, H.R. The Alcohol Use Disorders Identification Test (AUDIT): Validation of a screening instrument for use in medical settings. J. Stud. Alcohol 1995, 56, 423–432. [Google Scholar] [CrossRef]
- Hirschfeld, R.M.A. The Mood Disorder Questionnaire: A Simple, Patient-Rated Screening Instrument for Bipolar Disorder. Prim. Care Companion J. Clin. Psychiatry 2002, 4, 9–11. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Harnett-Sheehan, K.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G. The Mini International Neuropsychiatric Interview (MINI): The Development Vali-dation of a Structured Diagnostic Psychiatric Interview. J. Clin Psychiatry 1998, 59 (Suppl. S20), 22–33. [Google Scholar]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM), 2nd ed.; Sage Publications Inc.: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Ruiz, J.S.; García, J.B.; Ruiloba, J.V.; Ubago, J.G.; González, M.P. Consenso sobre la salud física del paciente con esquizofrenia de las Sociedades Es-pañolas de Psiquiatría y de Psiquiatría Biológica [Consensus on physical health of patients with schizophrenia from the Spanish Societies of Psychiatry and Biological Psychiatry]. Actas Esp. Psiquiatr. 2008, 36, 251–264. [Google Scholar]
- Brown, S.; Inskip, H.; Barraclough, B. Causes of the excess mortality of schizophrenia. Br. J. Psychiatry 2000, 177, 212–217. [Google Scholar] [CrossRef]
- Lahti, M.; Tiihonen, J.; Wildgust, H.; Beary, M.; Hodgson, R.; Kajantie, E.; Osmond, C.; Räikkönen, K.; Eriksson, J. Cardiovascular morbidity, mortality and pharmacotherapy in patients with schizophrenia. Psychol. Med. 2012, 42, 2275–2285. [Google Scholar] [CrossRef]
- Kang, J.H.; Xirasagar, S.; Lin, H.C. Lower mortality among stroke patients with schizophrenia: A na-tionwide population-based study. Psychosom. Med. 2011, 73, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Sokal, J.; Messias, E.; Dickerson, F.B.; Kreyenbuhl, J.; Brown, C.H.; Goldberg, R.W.; Dixon, L.B. Comorbid-ity of medical illnesses among adults with serious mental illness who are receiving community psy-chiatric services. J. Nerv. Ment. Dis. 2004, 192, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Huang, J.; Tian, J.; Cao, Y.; Zhang, G.; Wang, C.; Cao, Y.; Li, J. The prevalence and risk factors of stroke in patients with chronic schizophrenia. Neuropsychiatr. Dis. Treat. 2016, 12, 1131–1134. [Google Scholar] [CrossRef] [PubMed]
- Høyer, E.H.; Mortensen, P.B.; Olesen, A.V. Mortality and causes of death in a total national sample of patients with affective disorders admitted for the first time between 1973 and 1993. Br. J. Psychiatry 2000, 176, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Joukamaa, M.; Heliovaara, M.; Knekt, P.; Aromaa, A.; Raitasalo, R.; Lehtinen, V. Mental disor-ders cause-specific mortality. Br. J. Psychiatry 2001, 179, 498–502. [Google Scholar] [CrossRef]
- Tsai, S.Y.; Lee, C.H.; Kuo, C.J.; Chen, C.C. A retrospective analysis of risk protective factors for natural death in bipolar disorder. J. Clin. Psychiatry 2005, 66, 1586–1591. [Google Scholar] [CrossRef]
- BozkurtZincir, S.; Ozdilek, B.F.; Zincir, S. Association of quetiapine with ischemic brain stem stroke: A case report and discussion. Ther. Adv. Psychopharmacol. 2015, 5, 246–249. [Google Scholar] [CrossRef]
- Malarcher, A.M.; Giles, W.H.; Croft, J.B.; Wozniak, M.A.; Wityk, R.J.; Stolley, P.D.; Stern, B.J.; Sloan, M.A.; Sherwin, R.; Price, T.R.; et al. Alcohol intake, type of beverage, and the risk of cerebral in-farction in young women. Stroke 2001, 32, 77–83. [Google Scholar] [CrossRef]
- Hillbom, M. Alcohol consumption and stroke: Benefits and risks. Alcohol Clin. Exp Res. 1998, 22 (Suppl. S7), 352S–358S. [Google Scholar] [CrossRef]
- Zakhari, S. Alcohol and the cardiovascular system: Molecular mechanisms for beneficial and harmful action. Alcohol Health Res. World 1997, 21, 21. [Google Scholar] [PubMed]
- Chen, P.-H.; Tsai, S.-Y.; Pan, C.-H.; Chang, C.-K.; Su, S.-S.; Chen, C.-C.; Kuo, C.-J. Mood stabilisers and risk of stroke in bipolar disorder. Br. J. Psychiatry 2018, 215, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.-T.; Esmaily-Fard, A.; Lai, C.-C.; Zala, D.; Lee, S.-H.; Chang, S.-S.; Lee, C.-C. Antipsychotics and the Risk of Cerebrovascular Accident: A Systematic Review and Meta-Analysis of Observational Studies. J. Am. Med. Dir. Assoc. 2017, 18, 692–699. [Google Scholar] [CrossRef]
- Drevets, W.C.; Price, J.L.; Simpson, J.R., Jr.; Todd, R.D.; Reich, T.; Vannier, M.; Raichle, M.E. Subgenual prefrontal cortex abnormalities in mood disorders. Nature 1997, 386, 824–827. [Google Scholar] [CrossRef] [PubMed]
- Adler, C.M.; Levine, A.D.; DelBello, M.P.; Strakowski, S.M. Changes in Gray Matter Volume in Patients with Bipolar Disorder. Biol. Psychiatry 2005, 58, 151–157. [Google Scholar] [CrossRef]
- Lyoo, I.K.; Sung, Y.H.; Dager, S.R.; Friedman, S.; Lee, J.-Y.; Kim, S.J.; Kim, N.; Dunner, D.L.; Renshaw, P.F. Regional cerebral cortical thinning in bipolar disorder. Bipolar Disord. 2006, 8, 65–74. [Google Scholar] [CrossRef]
- Karlsgodt, K.H.; Sun, D.; Cannon, T.D. Structural and Functional Brain Abnormalities in Schizophrenia. Curr. Dir. Psychol. Sci. 2010, 19, 226–231. [Google Scholar] [CrossRef]
- Broome, M.V.; Hurley, R.A.; Taber, K.H. Substance Use Disorders: Do Males and Females Have Differential Vulnerability? J. Neuropsychiatry 2010, 22, iv. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Ovbiagele, B.; Feng, W. Diabetes and Stroke: Epidemiology, Pathophysiology, Pharmaceuticals and Outcomes. Am. J. Med. Sci. 2016, 351, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Arboix, A. Cardiovascular risk factors for acute stroke: Risk profiles in the different subtypes of is-chemic stroke. World J. Clin. Cases 2015, 3, 418–429. [Google Scholar] [CrossRef] [PubMed]
- Corlateanu, A.; Stratan, I.; Covantev, S.; Botnaru, V.; Siafakas, N. Asthma and stroke: A narrative review. Asthma Res. Pract. 2021, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.R.; Hwang, I.C.; Lee, Y.J.; Ham, E.B.; Park, D.K.; Kim, S. Stroke risk among patients with chronic obstruc-tive pulmonary disease: A systematic review and meta-analysis. Clinics (Sao Paulo) 2018, 73, e177. [Google Scholar] [CrossRef]
- Guasch, E.; Mont, L. Exercise and the heart: Unmasking Mr Hyde. Heart 2014, 100, 999–1000. [Google Scholar] [CrossRef]
- Mostofsky, E.; Laier, E.; Levitan, E.B.; Rosamond, W.D.; Schlaug, G.; Mittleman, M.A. Physical Activity and Onset of Acute Ischemic Stroke: The Stroke Onset Study. Am. J. Epidemiology 2010, 173, 330–336. [Google Scholar] [CrossRef]
- Hillbom, M.; Numminen, H. Alcohol and Stroke: Pathophysiologic Mechanisms. Neuroepidemiology 1998, 17, 281–287. [Google Scholar] [CrossRef]
- Hillbom, M.; Juvela, S.; Karttunen, V. Mechanisms of alcohol-related strokes. Novartis Found Symp 1998, 216, 193–207. [Google Scholar] [CrossRef] [PubMed]
- Vostrý, M.; Zilcher, L. Combined Therapy For Patients After Ischemic Stroke From The Point View Of Comprehensive Rehabilitation. J. Educ. Cult. Soc. 2020, 11, 119–125. [Google Scholar] [CrossRef]
- Bartík, P.; Vostrý, M.; Hudáková, Z.; Šagát, P.; Lesňáková, A.; Dukát, A. The Effect of Early Applied Robot-Assisted Physiotherapy on Functional Independence Measure Score in Post-Myocardial Infarction Patients. Healthcare 2022, 10, 937. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Ischemic Stroke Patients (N = 113) | Ischemic Stroke-Free Patients (N = 451) | p-Value |
|---|---|---|---|
| Mean ± SD | 0.035 | ||
| Age | 65.5 ± 11.9 | 62.9 ± 11.6 | |
| Gender | N (%) | 1 | |
| Male | 51 (45.1%) | 203 (45.0%) | |
| Female | 62 (54.9%) | 248 (55.0%) | |
| Marital Status | 0.020 | ||
| Single | 13 (11.5%) | 135 (29.9%) | |
| Married | 85 (75.2%) | 286 (63.4%) | |
| Divorced | 3 (2.7%) | 20 (4.4%) | |
| Widowed | 12 (10.6%) | 10 (2.2%) | |
| Educational Level | <0.001 | ||
| Primary-Complementary | 61 (54.0%) | 141 (31.3%) | |
| Secondary | 20 (17.7%) | 164 (36.4%) | |
| University | 32 (28.3%) | 146 (32.4%) | |
| Monthly Income | <0.001 | ||
| Low (<1000 USD) | 66 (58.4%) | 290 (64.3%) | |
| Intermediate (1000–2000 USD) | 25 (22.1%) | 147 (32.6%) | |
| High (>2000 USD) | 22 (19.5%) | 14 (3.1%) | |
| Preexisting Physical Disorders | |||
| Hypertension | 82 (72.6%) | 254 (56.3%) | 0.002 |
| Dyslipidemia | 65 (57.5%) | 205 (45.5%) | 0.027 |
| Diabetes | 41 (36.3%) | 120 (26.6%) | 0.048 |
| Heart Diseases | 48 (42.5%) | 53 (11.8%) | <0.001 |
| Atrial Fibrillation | 34 (30.1%) | 36 (8.0%) | <0.001 |
| Asthma-COPD | 44 (38.9%) | 118 (26.2%) | 0.008 |
| Cancer | 2 (1.8%) | 15 (3.3%) | 0.545 |
| Obesity | 70 (61.9%) | 229 (50.8%) | 0.035 |
| Mean ± SD | |||
| Physical Activity (IPAQ) | 163.83 ± 232.74 | 79.28 ± 139.31 | <0.001 |
| Mediterranean Diet Adherence(MeD) | 5.4 ± 3.1 | 7.6 ± 1.9 | <0.001 |
| Variable | Presence of Ischemic Stroke (N = 113) | Absence of Ischemic Stroke (N = 451) | p-Value |
|---|---|---|---|
| Mean ± SD | |||
| AUD | 3.8 ± 2.7 | 3.1 ± 1.8 | 0.014 |
| BD | 2.6 ± 2.8 | 1.8 ± 1.9 | 0.003 |
| N (%) | |||
| Schizophrenia | 4 (3.5%) | 3 (0.7%) | 0.033 |
| Logistic Regression Taking the Presence vs. Absence of Ischemic Stroke as the Dependent Variable and Taking AUD, BD, and Schizophrenia as Independent Variables. | |||
|---|---|---|---|
| Variables | p | aOR | 95% CI |
| Schizophrenia | 0.035 | 6.162 | 1.136–33.423 |
| BD | 0.025 | 4.653 | 1.214–17.834 |
| AUD | 0.003 | 3.918 | 1.584–9.689 |
| Obesity | 0.032 | 1.732 | 1.049–2.861 |
| Physical Activity (IPAQ) | <0.001 | 4.614 | 2.669–7.978 |
| Atrial Fibrillation | 0.010 | 2.415 | 1.235–4.721 |
| Diabetes | 0.017 | 1.865 | 1.117–3.115 |
| Heart Diseases | <0.001 | 9.890 | 5.099–19.184 |
| Asthma-COPD | 0.008 | 1.971 | 1.190–3.263 |
| Variable | Levels of Stroke Severity | p-Value | ||
|---|---|---|---|---|
| No Stroke | Minor/Moderate Stroke | Moderate to Severe/Severe Stroke | ||
| Mean ± SD | <0.001 | |||
| Age | 62.88 ± 11.6 | 59.40 ± 10.7 | 75.00 ± 6.2 | |
| Gender | N (%) | 0.772 | ||
| Male | 203 (45.0%) | 33 (47.8%) | 18 (40.9%) | |
| Female | 248 (55.0%) | 36 (52.2%) | 26 (59.1%) | |
| Marital Status | 0.027 | |||
| Single/Divorced/Widowed | 165 (36.6%) | 14 (20.3%) | 14 (31.8%) | |
| Married | 286 (63.4%) | 55 (79.7%) | 30 (68.2%) | |
| Educational Level | <0.001 | |||
| Primary-Complementary | 141 (31.3%) | 29 (42.0%) | 32 (72.7%) | |
| Secondary | 164 (36.4%) | 9 (13.0%) | 11 (25.0%) | |
| University | 146 (32.4%) | 31 (44.9%) | 1 (2.3%) | |
| Preexisting Physical Disorders | ||||
| Hypertension | 254 (56.3%) | 49 (71.0%) | 33 (75.0%) | 0.006 |
| Dyslipidemia | 205 (45.5%) | 36 (52.2%) | 29 (65.9%) | 0.025 |
| Diabetes | 120 (26.6%) | 24 (34.8%) | 17 (38.6%) | 0.109 |
| Heart Diseases | 53 (11.8%) | 19 (27.5%) | 29 (65.9%) | <0.001 |
| Atrial Fibrillation | 36 (8.0%) | 16 (23.2%) | 18 (40.9%) | <0.001 |
| Asthma-COPD | 118 (26.2%) | 25 (36.2%) | 19 (43.2%) | 0.019 |
| Cancer | 15 (3.3%) | 1 (1.4%) | 1 (2.3%) | 0.744 |
| Obesity | 229 (50.8%) | 43 (62.3%) | 27 (61.4%) | 0.105 |
| Mean ± SD | ||||
| Physical Activity (IPAQ) | 79.28 ± 139.31 | 253.95 ± 251.37 | 22.50 ± 87.68 | <0.001 |
| Mediterranean Diet Adherence | 7.60 ± 1.9 | 5.50 ± 3.3 | 5.20 ± 2.9 | <0.001 |
| Preexisting Psychological Disorders | ||||
| AUD | 1.42 ± 1.9 | 3.38 ± 3.2 | 2.70 ± 2.0 | <0.001 |
| BD | 1.78 ± 1.9 | 3.25 ± 3.2 | 1.68 ± 1.7 | <0.001 |
| N (%) | 0.039 | |||
| Schizophrenia | 3 (0.07%) | 2 (2.9%) | 2 (4.5%) | |
| Model 1: Levels of Stroke Severity (Minor/Moderate Stroke vs. No Stroke) | |||
|---|---|---|---|
| Variables | p | aOR | 95% CI |
| Age | 0.415 | 0.978 | 0.923–1.032 |
| Marital Status (married vs single *) | 0.078 | 2.121 | 0.920–4.893 |
| Educational Level (secondary vs primary-complementary *) | 0.187 | 0.519 | 0.196–1.374 |
| Educational Level (university vs primary-complementary *) | <0.001 | 0.130 | 0.044–0.383 |
| AUD | <0.001 | 1.466 | 1.260–1.706 |
| BD | 0.004 | 1.229 | 1.066–1.416 |
| Schizophrenia | 0.620 | 2.093 | 0.113–38.771 |
| Physical Activity (IPAQ) | <0.001 | 1.006 | 1.004–1.008 |
| Mediterranean Diet Adherence | <0.001 | 0.711 | 0.620–0.816 |
| Hypertension (yes vs. no *) | 0.037 | 2.380 | 1.055–5.372 |
| Dyslipidemia (yes vs. no *) | 0.043 | 2.220 | 1.024–4.811 |
| Heart Diseases (yes vs. no *) | 0.009 | 3.726 | 1.396–9.950 |
| Atrial Fibrillation (yes vs. no *) | 0.106 | 2.193 | 0.846–5.685 |
| Asthma-COPD (yes vs. no *) | 0.136 | 1.708 | 0.845–3.452 |
| Model 2: Levels of stroke severity (Moderate to Severe/Severe Stroke vs No Stroke) | |||
| Variables | p | aOR | 95% CI |
| Age | <0.001 | 1.321 | 1.173–1.488 |
| Marital Status (married vs single *) | 0.383 | 1.577 | 0.567–4.385 |
| Educational Level (secondary vs primary-complementary *) | 0.590 | 1.333 | 0.413–4.298 |
| Educational Level (university vs primary-complementary *) | 0.630 | 0.109 | 0.009–1.267 |
| AUD | <0.001 | 1.719 | 1.385–2.133 |
| BD | <0.001 | 1.656 | 1.281–2.141 |
| Schizophrenia | 0.006 | 6.884 | 3.294–11.492 |
| Physical Activity (IPAQ) | 0.663 | 1.001 | 0.995–1.008 |
| Mediterranean Diet Adherence | <0.001 | 0.573 | 0.470–0.698 |
| Hypertension (yes vs. no *) | 0.411 | 0.636 | 0.216–1.872 |
| Dyslipidemia (yes vs. no *) | 0.907 | 0.945 | 0.363–2.460 |
| Heart Diseases (yes vs. no *) | 0.002 | 6.486 | 1.955–21.525 |
| Atrial Fibrillation (yes vs. no *) | 0.271 | 1.788 | 0.636–5.031 |
| Asthma-COPD (yes vs. no *) | 0.134 | 1.958 | 0.813–4.719 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maalouf, E.; Hallit, S.; Salameh, P.; Hosseini, H. Impact of Preexisting Alcohol Use Disorder, Bipolar Disorder, and Schizophrenia on Ischemic Stroke Risk and Severity: A Lebanese Case-Control Study. Healthcare 2023, 11, 538. https://doi.org/10.3390/healthcare11040538
Maalouf E, Hallit S, Salameh P, Hosseini H. Impact of Preexisting Alcohol Use Disorder, Bipolar Disorder, and Schizophrenia on Ischemic Stroke Risk and Severity: A Lebanese Case-Control Study. Healthcare. 2023; 11(4):538. https://doi.org/10.3390/healthcare11040538
Chicago/Turabian StyleMaalouf, Elise, Souheil Hallit, Pascale Salameh, and Hassan Hosseini. 2023. "Impact of Preexisting Alcohol Use Disorder, Bipolar Disorder, and Schizophrenia on Ischemic Stroke Risk and Severity: A Lebanese Case-Control Study" Healthcare 11, no. 4: 538. https://doi.org/10.3390/healthcare11040538