
Effect of Intramuscular Tramadol on the Duration of Clinically Relevant Sciatic Nerve Blockade in Patients Undergoing Calcaneal Fracture Fixation: A Randomized Controlled Trial
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Anesthetic Procedure and Intervention
2.2. Intramedullary Nailing
2.3. Study Endpoints
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vosoughi, A.R.; Borazjani, R.; Ghasemi, N.; Fathi, S.; Mashhadiagha, A.; Hoveidaei, A.H. Different types and epidemiological patterns of calcaneal fractures based on reviewing CT images of 957 fractures. Foot Ankle Surg. 2021, 28, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Razik, A.; Harris, M.; Trompeter, A. Calcaneal fractures: Where are we now? Strateg. Trauma Limb Reconstr. 2018, 13, 1–11. [Google Scholar]
- Gerbershagen, H.J.; Aduckathil, S.; van Wijck, A.J.M.; Peelen, L.M.; Kalkman, C.; Meissner, W. Pain Intensity on the First Day after Surgery. Anesthesiology 2013, 118, 934–944. [Google Scholar] [CrossRef] [PubMed]
- Pehora, C.; Pearson, A.M.; Kaushal, A.; Crawford, M.; Johnston, B.C. Dexamethasone as an adjuvant to peripheral nerve block. Cochrane Database Syst. Rev. 2017, 11, CD011770. [Google Scholar] [CrossRef]
- Kirksey, M.A.; Haskins, S.C.; Cheng, J.; Liu, S.S. Local Anesthetic Peripheral Nerve Block Adjuvants for Prolongation of Analgesia: A Systematic Qualitative Review. PLoS ONE 2015, 10, e0137312. [Google Scholar] [CrossRef]
- Desai, N.; Albrecht, E.; El-Boghdadly, K. Perineural adjuncts for peripheral nerve block. BJA Educ. 2019, 19, 276–282. [Google Scholar] [CrossRef]
- Abdallah, F.W.; Dwyer, T.; Chan, V.W.S.; Niazi, A.U.; Ogilvie-Harris, D.J.; Oldfield, S.; Patel, R.; Oh, J.; Brull, R. IV and Perineural Dexmedetomidine Similarly Prolong the Duration of Analgesia after Interscalene Brachial Plexus Block: A Randomized, Three-arm, Triple-masked, Placebo-controlled Trial. Anesthesiology 2016, 124, 683–695. [Google Scholar] [CrossRef]
- Sousa, A.M.; Ashmawi, H.A.; Costa, L.S.; Posso, I.P.; Slullitel, A. Percutaneous sciatic nerve block with tramadol induces analgesia and motor blockade in two animal pain models. Braz. J. Med. Biol. Res. 2012, 45, 147–152. [Google Scholar]
- Güven, M.; Mert, T.; Günay, I. Effects of Tramadol on Nerve Action Potentials in Rat: Comparisons with Benzocaine and Lidocaine. Int. J. Neurosci. 2005, 115, 339–349. [Google Scholar] [CrossRef]
- Beyazova, M.; Öztürk, E.; Zinnuroğlu, M.; Gökyar, I.; Babacan, A.; Kaya, K. Effects of perineural tramadol on nerve conduction of sural nerve. AĞRI 2011, 23, 51–56. [Google Scholar]
- Alemanno, F.; Ghisi, D.; Fanelli, A.; Faliva, A.; Pergolotti, B.; Bizzarri, F.; Fanelli, G. Tramadol and 0.5% levobupivacaine for single-shot interscalene block: Effects on postoperative analgesia in patients undergoing shoulder arthroplasty. Minerva Anestesiol. 2012, 78, 291–296. [Google Scholar] [PubMed]
- Kaabachi, O.; Ouezini, R.; Koubaa, W.; Ghrab, B.; Zargouni, A.; Ben Abdelaziz, A. Tramadol as an Adjuvant to Lidocaine for Axillary Brachial Plexus Block. Obstet. Anesth. Dig. 2009, 108, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Robaux, S.; Blunt, C.; Viel, E.; Cuvillon, P.; Nouguier, P.; Dautel, G.; Boileau, S.; Girard, F.; Bouaziz, H. Tramadol Added to 1.5% Mepivacaine for Axillary Brachial Plexus Block Improves Postoperative Analgesia Dose-Dependently. Obstet. Anesth. Dig. 2004, 98, 1172–1177. [Google Scholar] [CrossRef]
- Tang, Q.-F.; Li, X.-L.; Yu, L.-X.; Hao, Y.-F.; Lu, G.-H. Preoperative Ropivacaine with or without Tramadol for Femoral Nerve Block in Total Knee Arthroplasty. J. Orthop. Surg. 2016, 24, 183–187. [Google Scholar] [CrossRef]
- Soulioti, E.; Tsaroucha, A.; Makris, A.; Koutsaki, M.; Sklika, E.; Mela, A.; Megaloikonomos, P.D.; Mavrogenis, A.F.; Fassoulaki, A. Addition of 100 mg of Tramadol to 40 mL of 0.5% Ropivacaine for Interscalene Brachial Plexus Block Improves Postoperative Analgesia in Patients Undergoing Shoulder Surgeries as Compared to Ropivacaine Alone-A Randomized Controlled Study. Medicina 2019, 55, 399. [Google Scholar] [CrossRef]
- Shin, H.W.; Ju, B.J.; Jang, Y.K.; You, H.S.; Kang, H.; Park, J.Y. Effect of tramadol as an adjuvant to local anesthetics for brachial plexus block: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0184649. [Google Scholar]
- Kapral, S.; Gollmann, G.; Waltl, B.; Likar, R.; Sladen, R.N.; Weinstabl, C.; Lehofer, F. Tramadol added to mepivacaine prolongs the duration of an axillary brachial plexus blockade. Anesth. Analg. 1999, 88, 853–856. [Google Scholar]
- Sen, H.; Seckiner, I.; Bayrak, O.; Sen, E.; Erturhan, S.; Yagci, F. Combination of Tramadol and Lidocaine for Pain Control During Transrectal Ultrasound-guided Prostate Biopsy: A Randomized Double-blinded Study. Urology 2015, 85, 1247–1251. [Google Scholar] [CrossRef]
- Rodríguez, W.L.; Pozos, G.A.; Silva, H.D.; Chavarría, B.D. Efficacy of mepivacaine-tramadol combination on the success of inferior alveolar nerve blocks in patients with symptomatic irreversible pulpitis: A randomized clinical trial. Int. Endod. J. 2016, 49, 325–333. [Google Scholar]
- Casati, A.; Vinciguerra, F.; Santorsola, R.; Aldegheri, G.; Putzu, M.; Fanelli, G. Sciatic nerve block with 0.5% levobupivacaine, 0.75% levobupivacaine or 0.75% ropivacaine: A double-blind, randomized comparison. Eur. J. Anaesthesiol. 2005, 22, 452–456. [Google Scholar]
- Fanelli, G.; Casati, A.; Beccaria, P.; Aldegheri, G.; Berti, M.; Tarantino, F.; Torri, G. A Double-Blind Comparison of Ropivacaine, Bupivacaine, and Mepivacaine During Sciatic and Femoral Nerve Blockade. Anesth. Analg. 1998, 87, 597–600. [Google Scholar] [CrossRef] [PubMed]
- Doleman, B.; Leonardi-Bee, J.; Heinink, T.P.; Bhattacharjee, D.; Lund, J.N.; Williams, J.P. Pre-emptive and preventive opioids for postoperative pain in adults undergoing all types of surgery. Cochrane Database Syst. Rev. 2018, 2018, CD012624. [Google Scholar] [CrossRef] [PubMed]
- Wordliczek, J.; Banach, M.; Garlicki, J.; Jakowicka-Wordliczek, J.; Dobrogowski, J. Influence of pre- or intraoperational use of tramadol (preemptive or preventive analgesia) on tramadol requirement in the early postoperative period. Pol. J. Pharmacol. 2002, 54, 693–697. [Google Scholar]
- Shen, X.; Wang, F.; Xu, S.; Ma, L.; Liu, Y.; Feng, S.; Wang, W.; Zhao, Q.; Li, X.; Zhao, L.; et al. Comparison of the analgesic efficacy of preemptive and preventive tramadol after lumpectomy. Pharmacol. Rep. 2008, 60, 415–421. [Google Scholar] [PubMed]
- Solmaz, F.A.; Kovalak, E. Comparison of tramadol/acetaminophen fixed-dose combination, tramadol, and acetaminophen in patients undergoing ambulatory arthroscopic meniscectomy. Acta Orthop. Traumatol. Turc. 2018, 52, 222–225. [Google Scholar] [CrossRef] [PubMed]
- Aweke, Z.; Seyoum, F.; Shitemaw, T.; Doba, D.N. Comparison of preemptive paracetamol, paracetamol-diclofenac & paracetamol-tramadol combination on postoperative pain after elective abdominal surgery under general anesthesia, Ethiopia: A randomized control trial study, 2018. BMC Anesthesiol. 2020, 20, 191. [Google Scholar] [CrossRef]
- Metry, A.A.; Wahba, R.M.; Nakhla, G.M.; Abdelmalek, F.A.; Ragaei, M.Z.; Fahmy, N.G. Comparative Study between Preemptive and Postoperative Intra-Articular Injection of Levobupivacaine and Tramadol for Control of Postoperative Pain. Anesth. Essays Res. 2019, 13, 84–90. [Google Scholar] [CrossRef]
- Jabalameli, M.; Hazegh, P.; Talakoub, R. Preemptive subcutaneous tramadol for post-operative pain in lower abdomen surgeries: A randomized double blinded placebo-control study. Adv. Biomed. Res. 2013, 2, 68. [Google Scholar] [CrossRef]
- Grond, S.; Sablotzki, A. Clinical Pharmacology of Tramadol. Clin. Pharmacokinet. 2004, 43, 879–923. [Google Scholar] [CrossRef]
- Thippeswamy, T.; Krishnaswamy, B.; Bengalorkar, G.M.; Mariyappa, N. Comparison of Efficacy and Safety of Intramuscular Piroxicam and Tramadol for Post-operative Pain in Patients Undergoing Caesarean Delivery. J. Clin. Diagn. Res. JCDR 2016, 10, FC01–FC04. [Google Scholar] [CrossRef]
- Ugur, M.B.; Yılmaz, M.; Altunkaya, H.; Cinar, F.; Ozer, Y.; Beder, L. Effects of intramuscular and peritonsillar injection of tramadol before tonsillectomy: A double blind, randomized, placebo-controlled clinical trial. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Zeidan, A.; Kassem, R.; Nahleh, N.; Maaliki, H.; El-Khatib, M.; Struys, M.M.; Baraka, A. Intraarticular Tramadol-Bupivacaine Combination Prolongs the Duration of Postoperative Analgesia After Outpatient Arthroscopic Knee Surgery. Obstet. Anesth. Dig. 2008, 107, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Axelsson, K.H.; Edström, H.H.; Sundberg, A.E.A.; Widman, G.B. Spinal Anaesthesia with Hyperbaric 0.5 % Bupivacaine: Effects of Volume. Acta Anaesthesiol. Scand. 1982, 26, 439–445. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
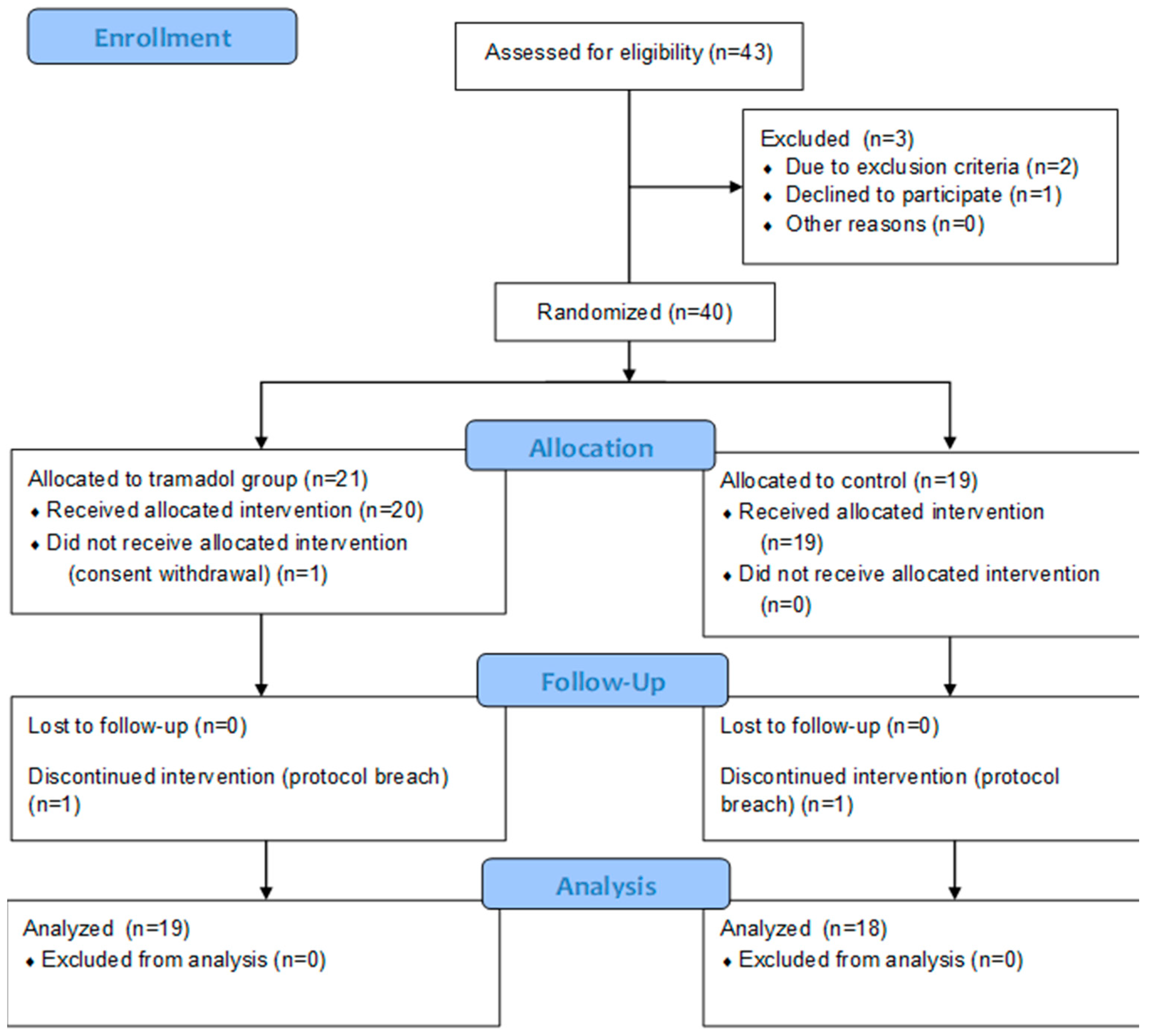
| Variables | Tramadol Group N = 19 | Control Group N = 18 | p Value |
|---|---|---|---|
| Age (years) | 51 ± 10.28 (31–66) | 45 ± 15.8 (21–80) | p = 0.22 (t-test) |
| Height (cm) | 172.2 ± 12.26 (140–189) | 171.1 ± 8.11 (169–190) | p = 0.74 (t-test) |
| Weight (kg) | 77.2 ± 15.22 (57–132) | 72.4 ± 12.68 (48–95) | p = 0.31 (t-test) |
| ASA physical status (I/II/III) | 9/10/0 | 8/9/1 | p = 0.99 (Chi2) |
| Duration of surgery (minutes) | 50 [45–55] | 58 [50–70] | p = 0.15 (Mann–Whitney U) |
| Sex (M/F) | 4/15 (21%/78%) | 6/12 (33%/57%) | p = 0.4 (Chi2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janiak, M.; Gorniewski, G.; Kowalczyk, R.; Wasilewski, P.; Nowakowski, P.; Trzebicki, J. Effect of Intramuscular Tramadol on the Duration of Clinically Relevant Sciatic Nerve Blockade in Patients Undergoing Calcaneal Fracture Fixation: A Randomized Controlled Trial. Healthcare 2023, 11, 498. https://doi.org/10.3390/healthcare11040498
Janiak M, Gorniewski G, Kowalczyk R, Wasilewski P, Nowakowski P, Trzebicki J. Effect of Intramuscular Tramadol on the Duration of Clinically Relevant Sciatic Nerve Blockade in Patients Undergoing Calcaneal Fracture Fixation: A Randomized Controlled Trial. Healthcare. 2023; 11(4):498. https://doi.org/10.3390/healthcare11040498
Chicago/Turabian StyleJaniak, Marek, Grzegorz Gorniewski, Rafal Kowalczyk, Piotr Wasilewski, Piotr Nowakowski, and Janusz Trzebicki. 2023. "Effect of Intramuscular Tramadol on the Duration of Clinically Relevant Sciatic Nerve Blockade in Patients Undergoing Calcaneal Fracture Fixation: A Randomized Controlled Trial" Healthcare 11, no. 4: 498. https://doi.org/10.3390/healthcare11040498