
Can Acupuncture Improve the Flexibility of Hamstring Muscles? A Randomized, Blinded, and Controlled Pilot Study


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection Instruments
- Socio-demographic questionnaire: This tool is used to characterize the sample regarding social data, such as gender, age, profession, and current professional situation;
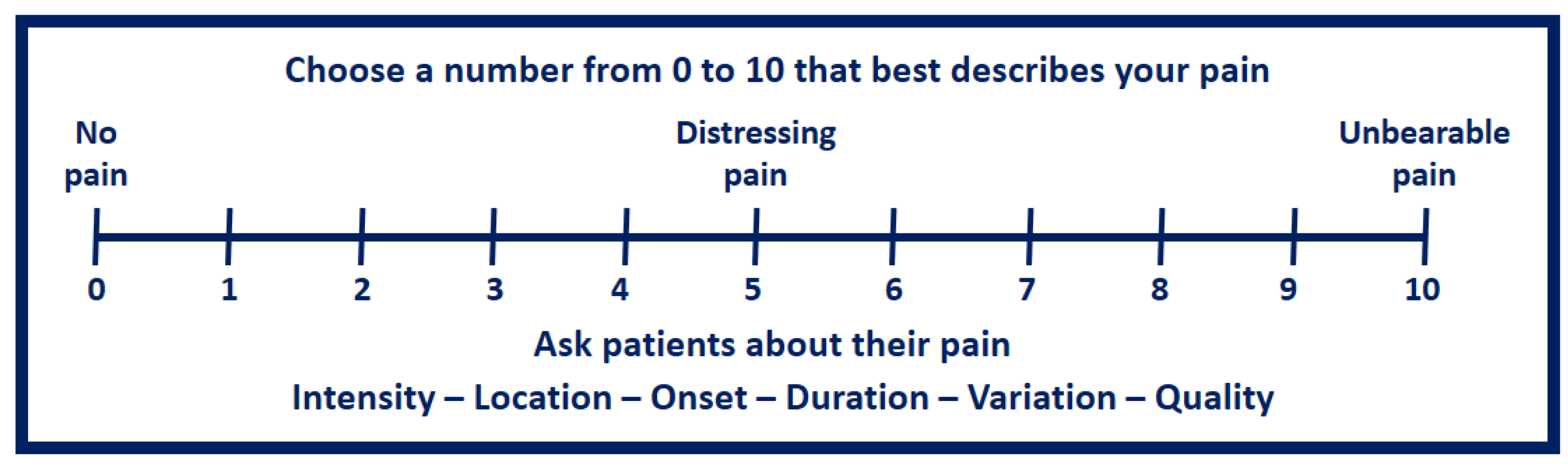
- VAS Questionnaire: The Visual Analogue Scale (VAS) is a measurement instrument used to measure a characteristic or attitude that changes across a continuum of values that cannot be easily quantified. Pain can be assessed using VAS with a numeric linear scale from 0 to 10. On this scale, “zero” is defined as “no pain”, and the extreme value of “ten” is considered “very severe pain or unbearable pain”.
- Muscle flexibility test: The sit and reach (SR) test, based on the procedure proposed by Ayala et al. (2012), was employed to measure the flexibility of the hamstring muscles. A wooden box measuring 30.5 cm in height, equipped with a centrally located sliding ruler, was utilized for this test [30]. The zero point was established as the 35 cm mark on the ruler, where the subjects’ feet made contact with the box. This apparatus allows a scoring range from 0 cm (indicating very low flexibility) to 50 cm (indicating very high flexibility). The test was performed with the participants sitting on the floor, with their knees extended in a straight line with bare feet against the vertical edge of the SR box. They were instructed to perform forward hip flexion, with overlapping hands, to reach the maximum point on the scale and maintain the position for 2 s. Two attempts were made, and the result was considered the average of the two evaluations (Figure 2).
2.2. Procedures
2.3. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davis, D.S.; Ashby, P.E.; McCale, K.L.; McQuain, J.A.; Wine, J.M. The effectiveness of 3stretching techniques on hamstring flexibility using consistent stretching parameters. J. Strength Cond. Res. 2005, 19, 27–32. [Google Scholar]
- Medeiros, D.M.; Cini, A.; Sbruzzi, G.; Lima, C.S. Influence of static stretching on hamstring flexibility in healthy young adults: Systematic review and meta-analysis. Physiother. Theory Pract. 2016, 32, 438–445. [Google Scholar] [CrossRef]
- Witvrouw, E.; Danneels, L.; Asselman, P.; D’Have, T.; Cambier, D. Muscle flexibility as a risk factor for developing muscle injuries in male professional soccer players: A prospective study. Am. J. Sports Med. 2003, 31, 41–46. [Google Scholar]
- Visnes, H.; Bahr, R. The evolution of eccentric training as treatment for patellar tendinopathy (jumper’s knee): A critical review of exercise programmes. Br. J. Sports Med. 2007, 41, 217–223. [Google Scholar] [CrossRef]
- Jonhagen, S.; Nemeth, G.; Eriksson, E. Hamstring injuries in sprinters: The role of concentric and eccentric hamstring muscle strength and flexibility. Am. J. Sports Med. 1994, 22, 262–266. [Google Scholar]
- Witvrouw, E.; Lysens, R.; Bellemans, J.; Cambier, D.; Vanderstraeten, G. Intrinsic Risk Factors for the Development of Anterior Knee Pain in an Athletic Population: A Two-Year Prospective Study. Am. J. Sports Med. 2000, 28, 480–489. [Google Scholar] [CrossRef]
- Delvaux, F.; Schwartz, C.; Decréquy, T.; Devalckeneer, T.; Paulus, J.; Bornheim, S.; Kaux, J.-F.; Croisier, J.-L. Influence of a Field Hamstring Eccentric Training on Muscle Strength and Flexibility. Int. J. Sports Med. 2020, 41, 233–241. [Google Scholar] [CrossRef]
- Li, S.; Garrett, W.E.; Best, T.M.; Li, H.; Wan, X.; Liu, H.; Yu, B. Effects of flexibility and strength interventions on optimal lengths of hamstring muscle-tendon units. J. Sci. Med. Sport 2020, 23, 200–205. [Google Scholar] [CrossRef]
- Alter, M.J. Science of Flexibility; Human Kinetics: Champaign, IL, USA, 2004. [Google Scholar]
- Babič, J.; Lenarčič, J. In vivo determination of triceps surae muscle?tendon complex viscoelastic properties. Eur. J. Appl. Physiol. 2004, 92, 477–484. [Google Scholar] [CrossRef]
- Ho, R.S.; Wong, C.H.; Wu, J.C.; Wong, S.Y.; Chung, V.C. Non-specific effects of acupuncture and sham acupuncture in clinical trials from the patient’s perspective: A systematic review of qualitative evidence. Acupunct. Med. 2020, 39, 3–19. [Google Scholar] [CrossRef]
- Cassidy, C.M. Contemporary Chinese Medicine and Acupuncture; Churchill Livingstone: Philadelphia, PA, USA, 2002. [Google Scholar]
- Vincent, C.; Lewith, G. Placebo controls for acupuncture studies. J. R. Soc. Med. 1995, 88, 199–202. [Google Scholar]
- Yuan, Q.-L.; Wang, P.; Liu, L.; Sun, F.; Cai, Y.-S.; Wu, W.-T.; Ye, M.-L.; Ma, J.-T.; Xu, B.-B.; Zhang, Y.-G. Acupuncture for musculoskeletal pain: A meta-analysis and meta-regression of sham-controlled randomized clinical trials. Sci. Rep. 2016, 6, 30675. [Google Scholar] [CrossRef]
- Hübscher, M.; Vogt, L.; Ziebart, T.; Banzer, W. Immediate effects of acupuncture on strength performance: A randomized, controlled crossover trial. Eur. J. Appl. Physiol. 2010, 110, 353–358. [Google Scholar] [CrossRef]
- Sandberg, M.; Larsson, B.; Lindberg, L.-G.; Gerdle, B. Different patterns of blood flow response in the trapezius muscle following needle stimulation (acupuncture) between healthy subjects and patients with fibromyalgia and work-related trapezius myalgia. Eur. J. Pain 2005, 9, 497. [Google Scholar] [CrossRef]
- Zijlstra, F.J.; Lange, I.V.D.B.-D.; Huygen, F.J.P.M.; Klein, J. Anti-inflammatory actions of acupuncture. Mediat. Inflamm. 2003, 12, 59–69. [Google Scholar] [CrossRef]
- Ikeda, H.; Asai, T.; Murase, K. Robust changes of afferent-induced excitation in the rat spinal dorsal horn after conditioning high-frequency stimulation. J. Neurophysiol. 2000, 83, 2412–2420. [Google Scholar] [CrossRef]
- Cardoso, R.; Lumini-Oliveira, J.A.; Santos, M.J.; Ramos, B.; Matos, L.; Machado, J.; Greten, H.J.; Franconi, G. Acupuncture can be beneficial for exercise-induced muscle soreness: A randomised controlled trial. J. Bodyw. Mov. Ther. 2020, 24, 8–14. [Google Scholar] [CrossRef]
- Itoh, K.; Ochi, H.; Kitakoji, H. Effects of tender point acupuncture on delayed onset muscle soreness (DOMS)—A pragmatic trial. Chin. Med. 2008, 3, 14. [Google Scholar] [CrossRef]
- Lin, J.-G.; Yang, S.-H. Effects of Acupuncture on Exercise-Induced Muscle Soreness and Serum Creatine Kinase Activity. Am. J. Chin. Med. 1999, 27, 299–305. [Google Scholar] [CrossRef]
- Barlas, P.; Robinson, J.; Allen, J.; Baxter, G.D. Lack of effect of acupuncture upon signs and symptoms of delayed onset muscle soreness. Clin. Physiol. Funct. Imaging 2000, 20, 449–456. [Google Scholar] [CrossRef]
- Matos, L.; Machado, J.; Monteiro, F.; Greten, H. Can Traditional Chinese Medicine Diagnosis Be Parameterized and Standardized? A Narrative Review. Healthcare 2021, 9, 177. [Google Scholar] [CrossRef]
- Matos, L.; Machado, J.; Monteiro, F.; Greten, H. Understanding Traditional Chinese Medicine Therapeutics: An Overview of the Basics and Clinical Applications. Healthcare 2021, 9, 257. [Google Scholar] [CrossRef]
- Matos, L.C.; Sousa, C.M.; Gonçalves, M.; Gabriel, J.; Machado, J.; Greten, H.J. Qigong as a Traditional Vegetative Biofeedback Therapy: Long-Term Conditioning of Physiological Mind-Body Effects. BioMed Res. Int. 2015, 2015, 1–6. [Google Scholar]
- Matos, L.; Goncalves, M.; Silva, A.; Mendes, J.; Machado, J.; Greten, H. Assessment of Qigong-related effects by infrared thermography=a case study. J. Chin. Integr. Med. 2012, 10, 663–666. [Google Scholar] [CrossRef]
- Greten, H.J. Understanding TCM. The Fundamentals of Chinese Medicine. Volume Part II; Heidelberg School: Heidelberg, Germany, 2014. [Google Scholar]
- Wewers, M.E.; Lowe, N.K. A critical review of visual analogue scales in the measurement of clinical phenomena. Res. Nurs. Health 1990, 13, 227–236. [Google Scholar] [CrossRef]
- Ghaderi, F.; Banakar, S.; Rostami, S. Effect of pre-cooling injection site on pain perception in pediatric dentistry: “A randomized clinical trial”. Dent. Res. J. 2013, 10, 790–794. [Google Scholar]
- Ayala, F.; de Baranda, P.S.; Croix, M.D.S.; Santonja, F. Criterion-related validity of four clinical tests used to measure hamstring flexibility in professional futsal players. Phys. Ther. Sport 2011, 12, 175–181. [Google Scholar] [CrossRef]
- Lam, Y.C.; Kum, W.F.; Durairajan, S.S.K.; Lu, J.H.; Man, S.C.; Xu, M.; Zhang, X.F.; Huang, X.Z.; Li, M. Efficacy and safety of acupuncture for idiopathic Parkinson’s disease: A systematic review. J. Altern. Complement. Med. 2008, 14, 663–671. [Google Scholar] [CrossRef]
- Jang, S.I.; So, W.-Y. Effects of acupuncture therapy on the electromyography activity of the rectus femoris and tibialis anterior during maximal voluntary isometric contraction in college students. JOMH 2018, 14, 1–5. [Google Scholar]
- Greten, H.J. Chinese Medicine as a Model of System Biology: Diagnosis as the Foundation of Acupoint Selection. In Current Research in Acupuncture; Springer: New York, NY, USA, 2012; pp. 621–657. [Google Scholar] [CrossRef]
- Matos, L.C.; Lopes, L.T.; Freire, V.A.; Machado, J.P.; Monteiro, F.J.; Greten, H.J. Can the electrical potential of acupoints be used to assess the functional state of meridians and the effects of therapeutics? An exploratory data analysis. J. Bodyw. Mov. Ther. 2020, 26, 309–317. [Google Scholar] [CrossRef]
- Ha, G.; Tian, Z.; Chen, J.; Wang, S.; Luo, A.; Liu, Y.; Tang, J.; Lai, N.; Zeng, F.; Lan, L. Coordinate-based (ALE) meta-analysis of acupuncture for musculoskeletal pain. Front. Neurosci. 2022, 16, 1–10. [Google Scholar] [CrossRef]
- Cao, L.; Zhang, X.-L.; Gao, Y.-S.; Jiang, Y. Needle acupuncture for osteoarthritis of the knee. A systematic review and updated meta-analysis. Saudi Med. J. 2012, 33, 526–532. [Google Scholar]
- Selfe, T.K.; Taylor, A.G. Acupuncture and osteoarthritis of the knee: A review of randomized, controlled trials. Fam. Community Health 2008, 31, 247. [Google Scholar]
- Pawling, R.; Cannon, P.R.; McGlone, F.P.; Walker, S.C. C-tactile afferent stimulating touch carries a positive affective value. PLoS ONE 2017, 12, e0173457. [Google Scholar] [CrossRef]
- Pawling, R.; Trotter, P.D.; McGlone, F.P.; Walker, S.C. A positive touch: C-tactile afferent targeted skin stimulation carries an appetitive motivational value. Biol. Psychol. 2017, 129, 186–194. [Google Scholar] [CrossRef]
- Lund, I.; Lundeberg, T. Are minimal, superficial or sham acupuncture procedures acceptable as inert placebo controls? Acupunct. Med. 2006, 24, 13–15. [Google Scholar]
- Meireles, A.; Rocha, B.P.; Rosa, C.T.; Silva, L.I.; Bonfleur, M.L.; Bertolini, G.R.F. Avaliação do papel de opioides endógenos na analgesia do laser de baixa potência, 820 nm, em joelho de ratos Wistar. Rev. Dor. 2012, 13, 152–155. [Google Scholar] [CrossRef]
- Goddard, G.; Karibe, H.; McNeill, C.; Villafuerte, E. Acupuncture and sham acupuncture reduce muscle pain in myofascial pain patients. J. Orofac. Pain 2002, 16, 71–76. [Google Scholar]
- Huang, C.; Wang, Z.; Xu, X.; Hu, S.; Zhu, R.; Chen, X. Does Acupuncture Benefit Delayed-Onset Muscle Soreness After Strenuous Exercise? A Systematic Review and Meta-Analysis. Front. Physiol. 2020, 11, 666. [Google Scholar] [CrossRef]
- da Costa, M.F.B. The Immediate Effect of Acupuncture on Improving Pain and Range of Motion in Patients with Shoulder Pain. Master’s Thesis, University of Porto, Porto, Portugal, 2014. [Google Scholar]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carvalho, R.M.; Machado, J.; Santos, M.J.; Matos, L.C. Can Acupuncture Improve the Flexibility of Hamstring Muscles? A Randomized, Blinded, and Controlled Pilot Study. Healthcare 2023, 11, 490. https://doi.org/10.3390/healthcare11040490
Carvalho RM, Machado J, Santos MJ, Matos LC. Can Acupuncture Improve the Flexibility of Hamstring Muscles? A Randomized, Blinded, and Controlled Pilot Study. Healthcare. 2023; 11(4):490. https://doi.org/10.3390/healthcare11040490
Chicago/Turabian StyleCarvalho, Rui Miguel, Jorge Machado, Maria João Santos, and Luís Carlos Matos. 2023. "Can Acupuncture Improve the Flexibility of Hamstring Muscles? A Randomized, Blinded, and Controlled Pilot Study" Healthcare 11, no. 4: 490. https://doi.org/10.3390/healthcare11040490