

Listen to the Whispers before They Become Screams: Addressing Black Maternal Morbidity and Mortality in the United States


{kind=link}
{kind=link}
Abstract
:1. Introduction
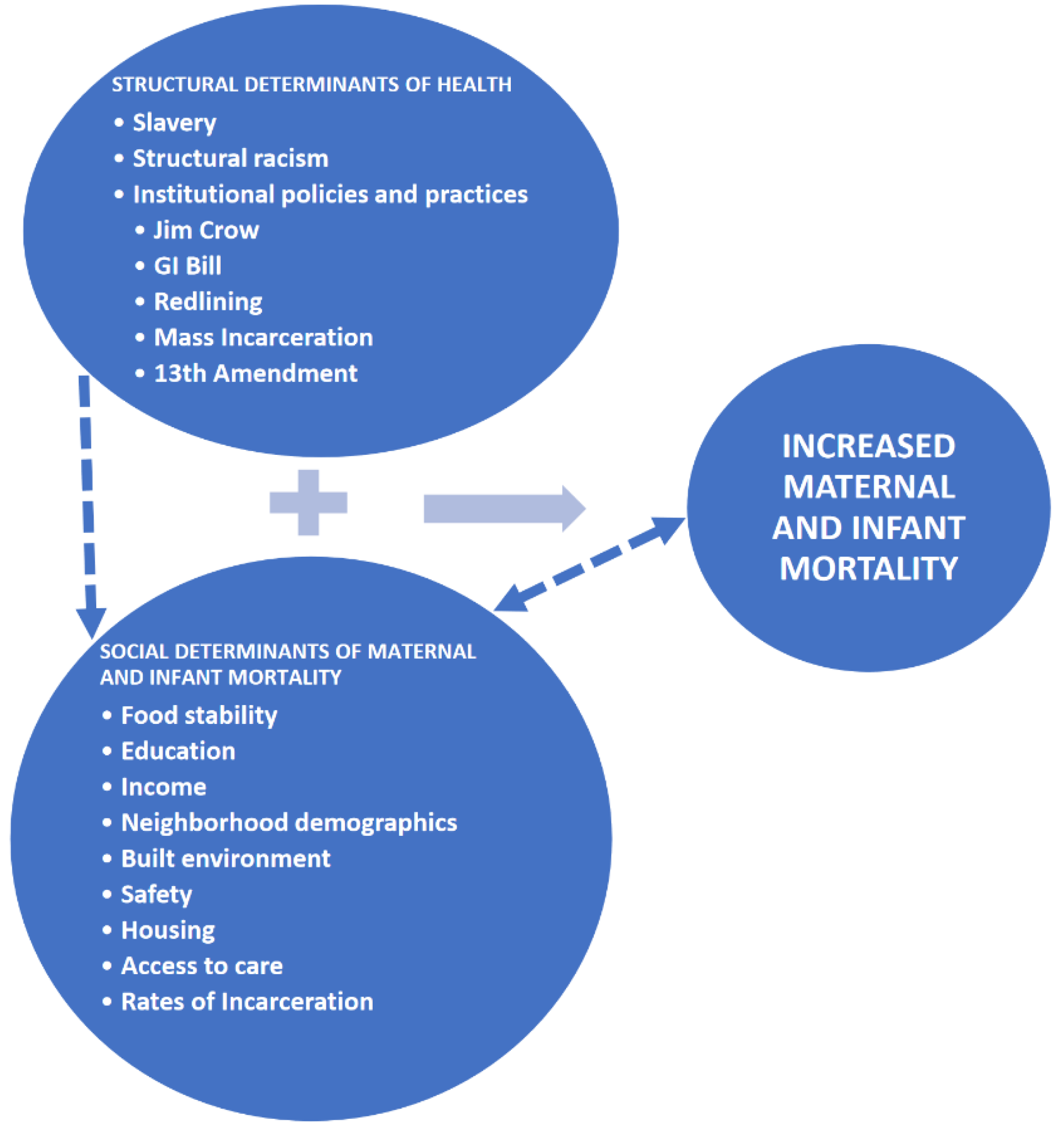
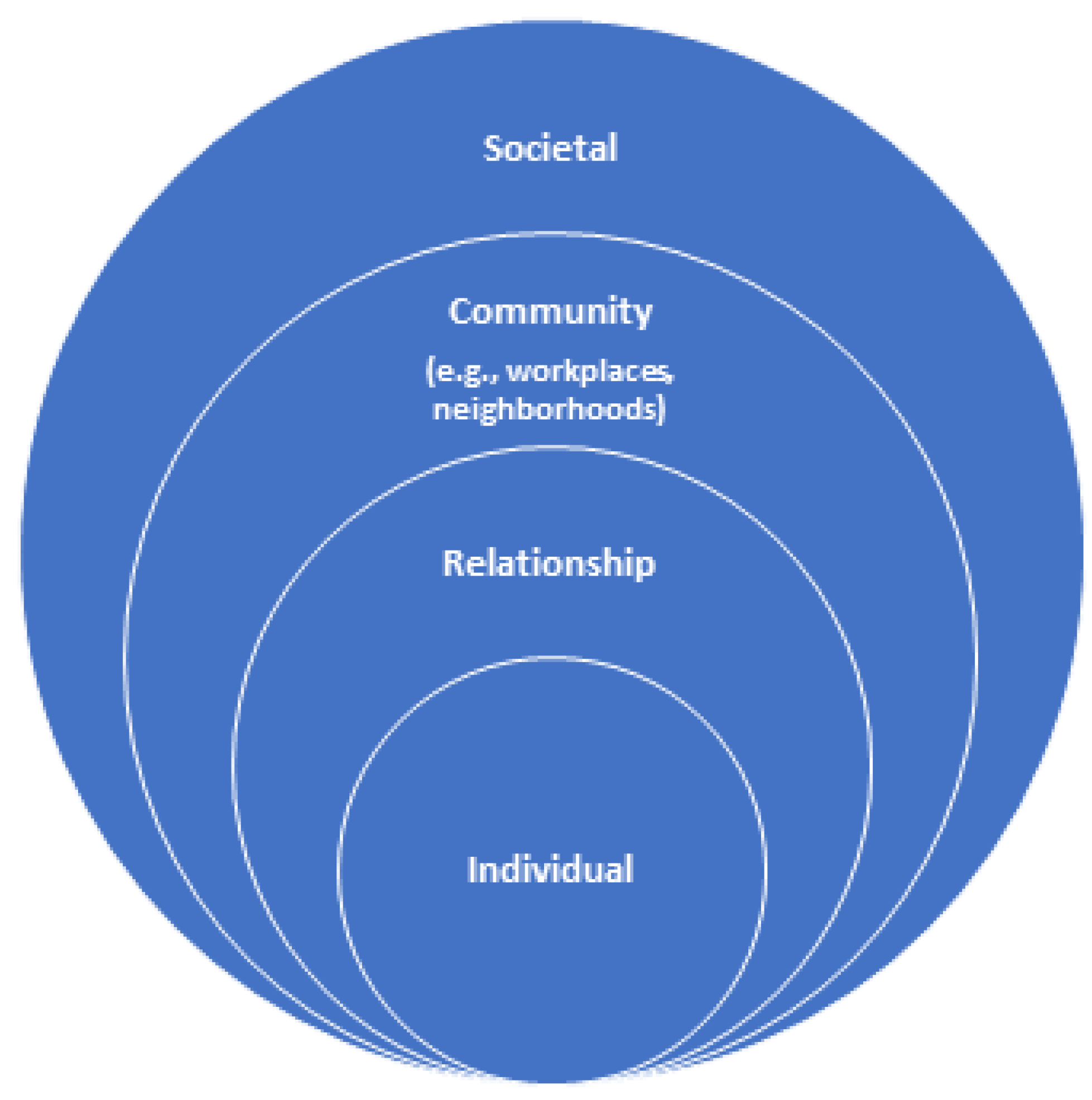
Theoretical Framework
2. Social Determinants of Health
3. Black Maternal Morbidity and Mortality
3.1. Contributing Factors
3.1.1. Individual Factors
3.1.2. Interpersonal Factors
3.1.3. Organizational Factors
3.1.4. Community Factors
3.1.5. Societal Factors
4. Discussion
4.1. Enhance Curriculum and Diversify the Workforce to Address Implicit Bias and to Improve Cultural Humility
4.2. Explore the Impact of Environmental and Occupational Exposures on Maternal Morbidity and Mortality
4.3. Address Social Determinants of Health by Exploring the Impact of Structural Racism on Maternal Health Outcomes
4.4. Improve Social Policies and Programs
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- CDC. Available online: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/severematernalmorbidity.html (accessed on 7 June 2022).
- CDC. Available online: https://www.cdc.gov/healthequity/features/maternal-mortality/index.html (accessed on 28 August 2022).
- CDC. Available online: https://www.cdc.gov/nchs/data/hestat/maternal-mortality/2020/maternal-mortality-rates-2020.htm (accessed on 7 June 2022).
- The American Journal of Managed Care. Available online: https://www.ajmc.com/view/us-ranks-worst-in-maternal-care-mortality-compared-with-10-other-developed-nations (accessed on 7 June 2022).
- Berg, C.J.; Callaghan, W.M.; Syverson, C.; Henderson, Z. Pregnancy-related mortality in the United States, 1998 to 2005. Obs. Gynecol. 2010, 116, 1302–1309. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.W., Jr.; David, R.J.; Handler, A.; Wall, S.; Andes, S. Very low birthweight in African American infants: The role of maternal exposure to interpersonal racial discrimination. Am. J. Public Health 2004, 94, 2132–2138. [Google Scholar] [CrossRef]
- Krieger, N.; Van Wye, G.; Huynh, M.; Waterman, P.D.; Maduro, G.; Li, W.; Gwynn, R.C.; Barbot, O.; Bassett, M.T. Structural Racism, Historical Redlining, and Risk of Preterm Birth in New York City 2013–2017. Am. J. Public Health 2020, 110, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Thompson, T.A.M.; Young, Y.Y.; Bass, T.M.; Baker, S.; Njoku, O.; Norwood, J.; Simpson, M. Racism Runs Through It: Examining the Sexual And Reproductive Health Experience of Black Women in the South: Study examines the sexual and reproductive health experiences of Black women in the South. Health Aff. 2022, 41, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Crear-Perry, J.; Correa-de-Araujo, R.; Lewis Johnson, T.; McLemore, M.R.; Neilson, E.; Wallace, M. Social and structural determinants of health inequities in maternal health. J. Women’s Health 2021, 30, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Center for Infectious Disease Research and Policy. Available online: https://www.cidrap.umn.edu/news-perspective/2022/06/maternal-deaths-climbed-33-during-covid-19 (accessed on 7 June 2022).
- Wakeel, F.; Njoku, A. Application of the Weathering Framework: Intersection of Racism, Stigma, and COVID-19 as a Stressful Life Event among African Americans. Healthcare 2021, 9, 145. [Google Scholar] [CrossRef] [PubMed]
- Kotlar, B.; Gerson, E.; Petrillo, S.; Langer, A.; Tiemeier, H. The impact of the COVID-19 pandemic on maternal and perinatal health: A scoping review. Reprod. Health 2021, 18, 10. [Google Scholar] [CrossRef] [PubMed]
- Geronimus, A.T. The weathering hypothesis and the health of African-American women and infants: Evidence and speculations. Ethn. Dis. 1992, 2, 207–221. [Google Scholar] [PubMed]
- NPR. Available online: https://www.npr.org/sections/codeswitch/2018/91/14/577664626/making-the-case-that-discrimination-is-bad-for-your-health (accessed on 7 June 2022).
- Geronimus, A.T.; Hickens, M.; Keene, D.; Bound, J. “Weathering” and Age Patterns of Allostatic Load Scores among Black and Whites in the United States. Am. J. Public. Health 2006, 96, 826–833. [Google Scholar] [CrossRef]
- Medical News Today. Available online: https://www.medicalnewstoday.com/articles/weathering-what-are-the-effects-of-stress-and-discrimination (accessed on 7 June 2022).
- Roach, J. ROOTT’s theoretical framework of the web of causation between structural and social determinants of health and wellness—2016. Restoring Our Own Through Transformation (ROOTT). 2016. Available online: https://www.roottrj.org/web-causation (accessed on 2 September 2022).
- Collins, P.H. Intersectionality’s definitional dilemmas. Annu. Rev. Sociol. 2015, 41, 1–20. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Social determinants of health. 2022. Available online: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1 (accessed on 1 March 2022).
- World Health Organization. Equity. 2022. Available online: http://www.who.int/healthsystems/topics/equity/en/ (accessed on 1 March 2022).
- Alvidrez, J.; Castille, D.; Laude-Sharp, M.; Rosario, A.; Tabor, D. The national institute on minority health and health disparities research framework. Am. J. Public Health 2019, 109, S16–S20. [Google Scholar] [CrossRef]
- World Health Organization. 2017. Available online: https://www.who.int/news-room/fact-sheets/detail/human-rights-and-health (accessed on 1 March 2022).
- Dagher, R.K.; Linares, D.E. A Critical Review on the Complex Interplay between Social Determinants of Health and Maternal and Infant Mortality. Children 2022, 9, 394. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.; Glazer, K.B.; Howell, E.A.; Janevic, T.M. Social Determinants of Pregnancy-Related Mortality and Morbidity in the United States: A Systematic Review. Obs. Gynecol. 2020, 135, 896–915. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.B.; Moniz, M.H.; Davis, M.M. Population-level factors associated with maternal mortality in the United States, 1997–2012. BMC Public Health 2018, 18, 1007. [Google Scholar] [CrossRef] [PubMed]
- Mehra, R.; Boyd, L.M.; Ickovics, J.R. Racial Residential Segregation and Adverse Birth Outcomes: A Systematic Review and Meta-Analysis. Soc. Sci. Med. 2017, 191, 237–250. [Google Scholar] [CrossRef]
- Ncube, C.N.; Enquobahrie, D.A.; Albert, S.M.; Herrick, A.L.; Burke, J.G. Association of Neighborhood Context with Offspring Risk of Preterm Birth and Low Birthweight: A Systematic Review and Meta-Analysis of Population-Based Studies. Soc. Sci. Med. 2016, 153, 156–164. [Google Scholar] [CrossRef]
- Howe, C.G.; Henn, B.C.; Eckel, S.P.; Farzan, S.F.; Grubbs, B.H.; Chavez, T.A.; Hodes, T.L.; Faham, D.; Al-Marayati, L.; Lerner, D.; et al. Prenatal Metal Mixtures and Birth Weight for Gestational Age in a Predominately Lower-Income Hispanic Pregnancy Cohort in Los Angeles. Environ. Health Perspect. 2020, 128, 117001. [Google Scholar] [CrossRef]
- Owens, D.C.; Fett, S.M. Black Maternal and Infant Health: Historical Legacies of Slavery. Am. J. Public Health 2019, 109, 1342–1345. [Google Scholar] [CrossRef]
- Morgan, J.; Morgan, J.L. Laboring Women: Reproduction and Gender in New World Slavery; University of Pennsylvania Press: Philadelphia, PA, USA, 2004. [Google Scholar]
- Haines, M. Fertility and Mortality in the United States. Available online: https://eh.net/encyclopedia/fertility-and-mortality-in-the-united-states/ (accessed on 1 September 2022).
- Centers for Disease Control and Prevention. User guide to the 2016 Period Linked Birth/Infant Death Public Use File. Available online: http://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/DVS/periodlinked/LinkPE16Guide.pdf (accessed on 30 August 2022).
- Miranda, M.L.; Swamy, G.K.; Edwards, S.; Maxson, P.; Gelfand, A.; James, S. Disparities in maternal hypertension and pregnancy outcomes: Evidence from North Carolina, 1994–2003. Public Health Rep. 2010, 125, 579–587. [Google Scholar] [CrossRef]
- Hicken, M.T.; Kravitz-Wirtz, N.; Durkee, M.; Jackson, J.S. Racial Inequalities in Health: Framing Future Research. Soc. Sci. Med. 2018, 199, 11–18. [Google Scholar] [CrossRef]
- Williams, D.R.; Lawrence, J.A.; Davis, B.A. Racism and Health: Evidence and Needed Research. Annu. Rev. Public Health 2019, 40, 105–125. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.J. Intersection of Bias, Structural Racism, and Social Determinants With Health Care Inequities. Pediatrics 2020, 146, e2020003657. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.P. Levels of Racism: A Theoretic Framework and a Gardener’s Tale. Am. J. Public Health 2000, 90, 1212–1215. [Google Scholar] [CrossRef]
- Boyles, A.L.; Beverly, B.E.; Fenton, S.E.; Jackson, C.L.; Jukic, A.M.Z.; Sutherland, V.L.; Baird, D.D.; Collman, G.W.; Dixon, D.; Ferguson, K.K. Environmental factors involved in maternal morbidity and mortality. J. Women’s Health 2021, 30, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Giurgescu, C.; Misra, D.P. Structural Racism and Maternal Morbidity among Black Women. West. J. Nurs. Res. 2022, 44, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Giscombé, C.L.; Lobel, M. Explaining Disproportionately High Rates of Adverse Birth Outcomes among African Americans: The Impact of Stress, Racism, and Related Factors in Pregnancy. Psychol. Bull. 2005, 131, 662–683. [Google Scholar] [CrossRef] [PubMed]
- Mustillo, S.; Krieger, N.; Gunderson, E.P.; Sidney, S.; McCreath, H.; Kiefe, C.I. Self-Reported Experiences of Racial Discrimination and Black–White Differences in Preterm and Low-Birthweight Deliveries: The CARDIA Study. Am. J. Public Health 2004, 94, 2125–2131. [Google Scholar] [CrossRef]
- Rosenberg, L.; Palmer, J.R.; Wise, L.A.; Horton, N.J.; Corwin, M.J. Perceptions of Racial Discrimination and the Risk of Preterm Birth. Epidemiology 2002, 13, 646–652. Available online: https://www.jstor.org/stable/3703477 (accessed on 1 September 2022). [CrossRef]
- Witt, W.P.; Litzelman, K.; Cheng, E.R.; Wakeel, F.; Barker, E.S. Measuring Stress Before and During Pregnancy: A Review of Population-Based Studies of Obstetric Outcomes. Matern. Child Health J. 2014, 18, 52–63. [Google Scholar] [CrossRef]
- Bailey, Z.D.; Krieger, N.; Agénor, M.; Graves, J.; Linos, N.; Bassett, M.T. Structural racism and health inequities in the USA: Evidence and interventions. Lancet 2017, 389, 1453–1463. [Google Scholar] [CrossRef]
- Krieger, N.; Chen, J.T.; Coull, B.; Waterman, P.D.; Beckfield, J. The unique impact of abolition of Jim Crow laws on reducing inequities in infant death rates and implications for choice of comparison groups in analyzing societal determinants of health. Am. J. Public Health 2013, 103, 2234–2244. [Google Scholar] [CrossRef] [PubMed]
- Gee, G.C.; Walsemann, K.M.; Brondolo, E. A life course perspective on how racism may be related to health inequities. Am. J. Public Health 2012, 102, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Humes, E. How the GI Bill Shunted Blacks into Vocational Training. J. Blacks High. Educ. 2006, 53, 92–104. [Google Scholar]
- Alexander, M. The New Jim Crow: Mass Incarceration in the Age of Colorblindness; The New Press: New York, NY, USA, 2020. [Google Scholar]
- Dongarwar, D.; Ajewole, V.B.; Oduguwa, E.; Ngujede, A.; Harris, K.; Ofili, T.U.; Olaleye, O.A.; Salihu, H.M. Role of Social Determinants of Health in Widening Maternal and Child Health Disparities in the Era of COVID-19 Pandemic. Int. J. MCH AIDS 2020, 9, 316–319. [Google Scholar] [CrossRef] [PubMed]
- Njoku, A.; Ahmed, Y.; Bolaji, B. Police brutality against Blacks in the United States and ensuing protests: Implications for social distancing and Black health during COVID-19. J. Hum. Behav. Soc. Environ. 2021, 31, 262–270. [Google Scholar] [CrossRef]
- Bray, S.R.; McLemore, M.R. Demolishing the myth of the default human that is killing Black mothers. Front. Public Health 2021, 9, 630. [Google Scholar] [CrossRef]
- CDC. Available online: https://www.cdc.gov/violenceprevention/about/social-ecologicalmodel.html (accessed on 15 June 2022).
- Kaiser Family Foundation. Available online: https://www.kff.org/report-section/racial-disparities-in-maternal-and-infant-health-an-overview-issue-brief/ (accessed on 1 September 2022).
- Oribhabor, G.I.; Nelson, M.L.; Buchanan-Peart, K.A.R.; Cancarevic, I. A mother’s cry: A race to eliminate the influence of racial disparities on maternal morbidity and mortality rates among Black women in America. Cureus 2020, 12. [Google Scholar] [CrossRef]
- Coussons-Read, M.E. Effects of prenatal stress on pregnancy and human development: Mechanisms and pathways. Obstet. Med. 2013, 6, 52–57. [Google Scholar] [CrossRef]
- Jackson, F.M.; Hogue, C.R.; Phillips, M.T. The development of a race and genderspecific stress measure for African-American women: Jackson, Hogue, Phillips contextualized stress measure. Ethn. Dis. 2005, 15, 594–600. [Google Scholar]
- March of Dimes. Available online: https://www.marchofdimes.org/stress-and-pregnancy.aspx (accessed on 15 June 2022).
- Jackson, F.M.; James, S.A.; Owens, T.C.; Bryan, A.F. Anticipated Negative Police-Youth Encounters and Depressive Symptoms among Pregnant African American Women: A Brief Report. J. Urban Health 2017, 94, 259–265. [Google Scholar] [CrossRef]
- Courchesne, N.S.; Smith, L.R.; Zúñiga, M.L.; Chambers, C.D.; Reed, M.B.; Ballas, J.; Marienfeld, C.B. Association of alcohol and other substance-related diagnoses with severe maternal morbidity. Alcoholism, clinical and experimental research 2021, 45, 1829–1839. [Google Scholar] [CrossRef]
- Chakhtoura, N.; Chinn, J.J.; Grantz, K.L.; Eisenberg, E.; Dickerson, S.A.; Lamar, C.; Bianchi, D.W. Importance of research in reducing maternal morbidity and mortality rates. Am. J. Obstet. Gynecol. 2019, 221, 179–182. [Google Scholar] [CrossRef] [PubMed]
- Diana, S.; Wahyuni, C.U.; Prasetyo, B. Maternal complications and risk factors for mortality. J. Public Health Res. 2020, 9, 1842. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.; Mamun, A.; Kitzman, H.; Mandapati, S.R.; Dodgen, L. Neighborhood disadvantage and allostatic load in African American women at risk for obesity-related diseases. Prev. Chronic Dis. 2017, 14, E119. [Google Scholar] [CrossRef]
- Schulz, A.J.; Mentz, G.; Lachance, L.; Johnson, J.; Gaines, C.; Israel, B.A. Associations between socioeconomic status and allostatic load: Effects of neighborhood poverty and tests of mediating pathways. Am. J. Public Health 2012, 102, 1706–1714. [Google Scholar] [CrossRef]
- Cozier, Y.C.; Albert, M.A.; Castro-Webb, N.; Coogan, P.F.; Ridker, P.; Kaufman, H.W.; Palmer, J.R.; Rosenberg, L. Neighborhood socioeconomic status in relation to serum biomarkers in the Black Women’s Health Study. J. Urban Health 2016, 93, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Robinette, J.W.; Charles, S.T.; Almeida, D.M.; Gruenewald, T.L. Neighborhood features and physiological risk: An examination of allostatic load. Health Place 2016, 41, 110–118. [Google Scholar] [CrossRef] [PubMed]
- O’Campo, P.; Schetter, C.D.; Guardino, C.M.; Vance, M.R.; Hobel, C.J.; Ramey, S.L.; Network, C.C.H. Explaining racial and ethnic inequalities in postpartum allostatic load: Results from a multisite study of low to middle income woment. SSM-Popul. Health 2016, 2, 850–858. [Google Scholar] [CrossRef]
- Howell, E.A. Reducing Disparities in Severe Maternal Morbidity and Mortality. Clin. Obstet. Gynecol. 2018, 61, 387–399. [Google Scholar] [CrossRef] [PubMed]
- Mannava, P.; Durrant, K.; Fisher, J.; Chersich, M.; Luchters, S. Attitudes and behaviours of maternal health care providers in interactions with clients: A systematic review. Glob. Health 2015, 11, 36. [Google Scholar] [CrossRef] [PubMed]
- Kumari, A.; Ranjan, P.; Sharma, K.A.; Sahu, A.; Bharti, J.; Zangmo, R.; Bhatla, N. Impact of COVID-19 on psychosocial functioning of peripartum women: A qualitative study comprising focus group discussions and in-depth interviews. Int. J. Gynecol. Obstet. 2021, 152, 321–327. [Google Scholar] [CrossRef]
- Singh, G.K. Maternal Mortality in the United States, 1935–2007: Substantial Racial/Ethnic, Socioeconomic, and Geographic Disparities Persist; US Department of Health and Human Services, Health Resources and Services Administration: Washington, DC, USA, 2010.
- Saluja, B.; Bryant, Z. How Implicit Bias Contributes to Racial Disparities in Maternal Morbidity and Mortality in the United States. J. Women’s Health 2021, 30, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Villarosa, L. “Why America’s Black Mothers and Babies Are in a Life-or-Death Crisis,” New York Times Magazine, 11 April 2018. Available online: https://www.nytimes.com/2018/04/11/magazine/black-mothers-babies-death-maternal-mortality.html (accessed on 1 September 2022).
- Vedam, S.; Stoll, K.; Taiwo, T.K.; Rubashkin, N.; Cheyney, M.; Strauss, N.; Declercq, E. The Giving Voice to Mothers study: Inequity and mistreatment during pregnancy and childbirth in the United States. Reprod. Health 2019, 16, 77. [Google Scholar] [CrossRef] [PubMed]
- National Partnership for Women & Families, “Listening to Black Mothers in California,” September 2018. Available online: https://www.nationalpartnership.org/our-work/resources/health-care/maternity/listening-to-black-mothers-in-california.pdf (accessed on 1 September 2022).
- Lassi, Z.S.; Kumar, R.; Bhutta, Z.A. Community-Based Care to Improve Maternal, Newborn, and Child Health. Dis. Control. Priorities 2016, 2, 263–284. [Google Scholar]
- Mayne, S.L.; Yellayi, D.; Pool, L.R.; Grobman, W.A.; Kershaw, K.N. Racial residential segregation and hypertensive disorder of pregnancy among women in Chicago: Analysis of electronic health record data. Am. J. Hypertens. 2018, 31, 1221–1227. [Google Scholar] [CrossRef]
- CDC. Clinical Tools and Resources. Available online: https://www.cdc.gov/hearher/healthcare-providers/clinical-resources-tools.html (accessed on 1 September 2022).
- Yusuf, K.K.; Dongarwar, D.; Ibrahimi, S.; Ikedionwu, C.; Maiyegun, S.O.; Salihu, H.M. Expected surge in maternal mortality and severe morbidity among African-Americans in the era of COVID-19 pandemic. Int. J. Matern. Child Health AIDS 2020, 9, 386. [Google Scholar] [CrossRef] [PubMed]
- Gur, R.E.; White, L.K.; Waller, R.; Barzilay, R.; Moore, T.M.; Kornfield, S.; Elovitz, M.A. The disproportionate burden of the COVID-19 pandemic among pregnant black women. Psychiatry Res. 2020, 293, 113475. [Google Scholar] [CrossRef] [PubMed]
- Shaw, E.; Levitt, C.; Wong, S.; Kaczorowski, J.; McMaster University Postpartum Research Group. Systematic review of the literature on postpartum care: Effectiveness of postpartum support to improve maternal parenting, mental health, quality of life, and physical health. Birth 2006, 33, 210–220. [Google Scholar] [CrossRef]
- Howell, E.A.; Egorova, N.N.; Janevic, T.; Brodman, M.; Balbierz, A.; Zeitlin, J.; Hebert, P.L. Race and ethnicity, medical insurance, and within-hospital severe maternal morbidity disparities. Obs. Gynecol. 2020, 135, 285–293. [Google Scholar] [CrossRef]
- Chan, A.L.; Guo, N.; Popat, R.; Robakis, T.; Blumenfeld, Y.Y.; Main, E.; Scott, K.A.; Butwick, A.J. Racial and ethnic disparities in hospital-based care associated with postpartum depression. J. Racial. Ethn. Health Disparities. 2021, 8, 220–229. [Google Scholar] [CrossRef]
- Brousseau, E.C.; Danilack, V.; Cai, F.; Matteson, K.A. Emergency department visits for postpartum complications. J. Womens Health 2018, 27, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, A.; Levi, E.E.; Garrett, J.M. Predictors of non-attendance to the postpartum follow-up visit. Matern. Child Health J. 2016, 20, 22–27. [Google Scholar] [CrossRef]
- Mi, T.; Hung, P.; Li, X.; McGregor, A.; He, J.; Zhou, J. Racial and ethnic disparities in postpartum care in the greater Boston area during the COVID-19 pandemic. JAMA Netw. Open 2022, 5, e2216355. [Google Scholar] [CrossRef]
- Mollard, E.; Kupzyk, K.; Moore, T. Postpartum stress and protective factors in women who gave birth in the United States during the COVID-19 pandemic. Women’s Health 2021, 17, 17455065211042190. [Google Scholar] [CrossRef] [PubMed]
- CDC. Working Together to Reduce Black Maternal Mortality. Available online: https://www.cdc.gov/healthequity/features/maternal-mortality/index.h (accessed on 1 September 2022).
- Kaiser Family Foundation. Available online: https://www.kff.org/racial-equity-and-health-policy/issue-brief/racial-disparities-in-maternal-and-infant-health-current-status-and-efforts-to-address-them/ (accessed on 26 December 2022).
- Solomon, J. Closing the Coverage Gap Would Improve Black Maternal Health. Retrieved from: Penalizing Abortion Providers Will Have Ripple Effects Across Pregnancy Care. Available online: https://www.cbpp.org/research/health/closing-the-coverage-gap-would-improve-black-maternal-health (accessed on 1 September 2022).
- Bond, R.; Gaither, K.; Nasser, S.; Albert, M.; Ferdinand, K.; Njoroge, J.; Parapid, B.; Hayes, S.; Pegus, C.; Sogade, B.; et al. Working Agenda for Black Mothers: A Position Paper from the Association of Black Cardiologists on Solutions to Improving Black Maternal Health. Cardiovasc. Qual. Outcomes 2021, 14, e007643. [Google Scholar] [CrossRef] [PubMed]
- Lucey, C.R.; Johnston, S.C. The transformational effects of COVID-19 on medical education. JAMA 2020, 324, 1033–1034. [Google Scholar] [CrossRef]
- Association of American Medical Colleges. Available online: https://www.aamc.org/news-insights/medical-students-569%need-learn-about-health-disparities-combat-future-pandemics (accessed on 7 June 2022).
- Njoku, A. COVID-19 and Health Disparities Opportunities for Public Health Curriculum Enhancement. In COVID-19 and Higher Education in the Global Context: Exploring Contemporary Issues and Challenges (pp. 139–153); Ammigan, R., Chan, R., Bista, K., Eds.; STAR Scholars: New York, NY, USA, 2022; Available online: https://ojed.org/index.php/gsm/article/view/2835 (accessed on 5 September 2022).
- Ahn, R.; Gonzalez, G.P.; Anderson, B.; Vladutiu, C.J.; Fowler, E.R.; Manning, L. Initiatives to reduce maternal mortality and severe maternal morbidity in the United States: A narrative review. Ann. Intern. Med. 2020, 173, S3–S10. [Google Scholar] [CrossRef]
- D’Alton, M.E.; Friedman, A.M.; Bernstein, P.S.; Brown, H.L.; Callaghan, W.M.; Clark, S.L.; Grobman, W.A.; Kilpatrick, S.J.; O’Keeffe, D.F.; Montgomery, D.M.; et al. Putting the “M” back in maternal-fetal medicine: A 5-year report card on a collaborative effort to address maternal morbidity and mortality in the United States. Am. J. Obstet. Gynecol. 2019, 221, 311–317.e1. [Google Scholar] [CrossRef]
- The Commonwealth Fund. Policies for Reducing Maternal Morbidity and Mortality and Enhancing Equity in Maternal Health. Available online: https://www.commonwealthfund.org/publications/fund-reports/2021/nov/policies-reducing-maternal-morbidity-mortality-enhancing-equity (accessed on 1 September 2022).
- Njoku, A.U. COVID-19 and environmental racism: Challenges and recommendations. Eur. J. Environ. Public Health 2021, 5, em0079. [Google Scholar] [CrossRef]
- Joe, J.R.; Shillingford-Butler, M.A.; Oh, S. The Experiences of African American Mothers Raising Sons in the Context of #BlackLivesMatter. TPC 2019, 9, 67–79. [Google Scholar]
- Malone Gonzalez, S. Making It Home: An Intersectional Analysis of the Police Talk. Gender Soc. 2019, 33, 363–386. [Google Scholar] [CrossRef]
- Dreyer, B.P. The Toll of Racism on African American Mothers and Their Infants. JAMA Netw. Open 2021, 4, e2138828. [Google Scholar] [CrossRef] [PubMed]
- Foundations of Critical Race Theory in Education; Critical Educator; Taylor, E.; Gillborn, D.; Ladson-Billings, G. (Eds.) Routledge: New York, NY, USA, 2009. [Google Scholar]
- Njoku, A.; Evans, M. Black women faculty and administrators navigating COVID-19, social unrest, and academia: Challenges and strategies. Int. J. Environ. Res. Public Health 2022, 19, 2220. [Google Scholar] [CrossRef]
- Yeter, D.; Banks, E.C.; Aschner, M. Disparity in Risk Factor Severity for Early Childhood Blood Lead among Predominantly African-American Black Children: The 1999 to 2010 US NHANES. Int. J. Environ. Res. Public Health 2020, 17, 1552. [Google Scholar] [CrossRef] [Green Version]
- Donley, N.; Bullard, R.D.; Economos, J.; Figueroa, I.; Lee, J.; Liebman, A.K.; Martinez, D.N.; Shafiei, F. Pesticides and environmental injustice in the USA: Root causes, current regulatory reinforcement and a path forward. BMC Public Health 2022, 22, 1–23. [Google Scholar] [CrossRef]
- Hillier, A.E. Redlining and the home owners’ loan corporation. J. Urban Hist. 2003, 29, 394–420. [Google Scholar] [CrossRef]
- Yearby, R. Racial disparities in health status and access to healthcare: The continuation of inequality in the United States due to structural racism: Continuing racial health disparities. Am. J. Econ. Sociol. 2018, 77, 1113–1152. [Google Scholar] [CrossRef]
- Kramer, M.R.; Hogue, C.R. Is segregation bad for your health? Epidemiol. Rev. 2009, 31, 178–194. [Google Scholar] [CrossRef]
- USA Today. Available online: https://www.usatoday.com/story/news/health/2022/05/03/people-color-most-impacted-if-roe-v-wade-overturned/9626866002/ (accessed on 7 June 2022).
- Strasser, J.; Chen, C.; Rosenbaum, S.; Schenk, E.; Dewhurst, E. Penalizing Abortion Providers Will Have Ripple Effects Across Pregnancy Care. 2022. Available online: https://www.healthaffairs.org/do/10.1377/forefront.20220503.129912/ (accessed on 1 September 2022).
- Ogunwole, S.M.; Bozzi, D.G.; Bower, K.M.; Cooper, L.A.; Hardeman, R.; Kozhimannil, K. Health Equity Considerations in State Bills Related to Doula Care (2015–2020). Women’s Health Issues 2022, 32, 440–449. [Google Scholar] [CrossRef]
- Van Eijk, M.S.; Guenther, G.A.; Kett, P.M.; Jopson, A.D.; Frogner, B.K.; Skillman, S.M. Addressing Systemic Racism in Birth Doula Services to Reduce Health Inequities in the United States. Health Equity 2022, 6, 98–105. [Google Scholar] [CrossRef]
- Kaiser Family Foundation. Medicaid Postpartum Coverage Extension Tracker. Available online: https://www.kff.org/medicaid/issue-brief/medicaid-postpartum-coverage-extension-tracker/ (accessed on 1 September 2022).
- Gordon, S.H.; Sommers, B.D.; Wilson, I.B.; Trivedi, A.N. Effects Of Medicaid Expansion On Postpartum Coverage And Outpatient Utilization. Health Aff. 2020, 39, 77–84. [Google Scholar] [CrossRef]
- Taylor, J.K. Structural Racism and Maternal Health Among Black Women. J. Law Med. Ethics 2020, 48, 506–517. [Google Scholar] [CrossRef]
- Joyce, A.; Tierney, L. What It’s Like to Have a Baby in the States Most Likely to Ban Abortion. Available online: https://www.washingtonpost.com/parenting/2022/05/06/support-in-states-banning-abortion/?utm_source=NIHCM+Foundation&utm_campaign=0ee168971f-nihcm-newsletter-may-2022&utm_medium=email (accessed on 14 June 2022).


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Njoku, A.; Evans, M.; Nimo-Sefah, L.; Bailey, J. Listen to the Whispers before They Become Screams: Addressing Black Maternal Morbidity and Mortality in the United States. Healthcare 2023, 11, 438. https://doi.org/10.3390/healthcare11030438
Njoku A, Evans M, Nimo-Sefah L, Bailey J. Listen to the Whispers before They Become Screams: Addressing Black Maternal Morbidity and Mortality in the United States. Healthcare. 2023; 11(3):438. https://doi.org/10.3390/healthcare11030438
Chicago/Turabian StyleNjoku, Anuli, Marian Evans, Lillian Nimo-Sefah, and Jonell Bailey. 2023. "Listen to the Whispers before They Become Screams: Addressing Black Maternal Morbidity and Mortality in the United States" Healthcare 11, no. 3: 438. https://doi.org/10.3390/healthcare11030438