

The Mediating Role of Depression and of State Anxiety οn the Relationship between Trait Anxiety and Fatigue in Nurses during the Pandemic Crisis

 ,
,  ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design and Procedure
2.2. Study Participants
2.3. Measures and Instruments
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mukhtar, S. Psychological health during the coronavirus disease 2019 pandemic outbreak. Int. J. Soc. Psychiatry 2020, 66, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab Syndr. 2020, 14, 779–788. [Google Scholar] [CrossRef]
- Tselebis, A.; Pachi, A. Primary Mental Health Care in a New Era. Healthcare 2022, 10, 2025. [Google Scholar] [CrossRef] [PubMed]
- El-Hage, W.; Hingray, C.; Lemogne, C.; Yrondi, A.; Brunault, P.; Bienvenu, T.; Etain, B.; Paquet, C.; Gohier, B.; Bennabi, D.; et al. Health professionals facing the coronavirus disease 2019 (COVID-19) pandemic: What are the mental health risks? Encephale 2020, 46, S73–S80. [Google Scholar] [CrossRef]
- Tselebis, A.; Lekka, D.; Sikaras, C.; Tsomaka, E.; Tassopoulos, A.; Ilias, I.; Bratis, D.; Pachi, A. Insomnia, Perceived Stress, and Family Support among Nursing Staff during the Pandemic Crisis. Healthcare 2020, 8, 434. [Google Scholar] [CrossRef] [PubMed]
- Batra, K.; Singh, T.; Sharma, M.; Batra, R.; Schvaneveldt, N. Investigating the Psychological Impact of COVID-19 among Healthcare Workers: A Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 9096. [Google Scholar] [CrossRef]
- Muller, A.E.; Hafstad, E.V.; Himmels, J.P.W.; Smedslund, G.; Flottorp, S.; Stensland, S.Ø.; Stroobants, S.; Van De Velde, S.; Vist, G.E. The mental health impact of the covid-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatr. Res. 2020, 293, 113441. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Sasangohar, F.; Jones, S.L.; Masud, F.N.; Vahidy, F.S.; Kash, B.A. Provider Burnout and Fatigue During the COVID-19 Pandemic: Lessons Learned from a High-Volume Intensive Care Unit. Obstet. Anesthesia Dig. 2020, 131, 106–111. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Marvaldi, M.; Mallet, J.; Dubertret, C.; Moro, M.R.; Guessoum, S.B. Anxiety, depression, trauma- related, and sleep disorders among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2021, 126, 252–264. [Google Scholar] [CrossRef]
- Zhan, Y.-X.; Zhao, S.-Y.; Yuan, J.; Liu, H.; Liu, Y.-F.; Gui, L.-L.; Zheng, H.; Zhou, Y.-M.; Qiu, L.-H.; Chen, J.-H.; et al. Prevalence and Influencing Factors on Fatigue of First-line Nurses Combating with COVID-19 in China: A Descriptive Cross-Sectional Study. Curr. Med. Sci. 2020, 40, 625–635. [Google Scholar] [CrossRef]
- Graham, K.C.; Cvach, M. Monitor Alarm Fatigue: Standardizing Use of Physiological Monitors and Decreasing Nuisance Alarms. Am. J. Crit. Care 2010, 19, 28–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chand, S.P.; Marwaha, R. Anxiety. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Kessing, L.V.; Bukh, J.D.; Bock, C.; Vinberg, M.; Gether, U. Does bereavement-related first episode depression differ from other kinds of first depressions? Soc. Psychiatry Psychiatr. Epidemiol. 2009, 45, 801–808. [Google Scholar] [CrossRef]
- Chand, S.P.; Arif, H. Depression. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Kendler, K.S.; Kuhn, J.; Prescott, C.A. The Interrelationship of Neuroticism, Sex, and Stressful Life Events in the Prediction of Episodes of Major Depression. Am. J. Psychiatry 2004, 161, 631–636. [Google Scholar] [CrossRef]
- Hettema, J.M. What is the genetic relationship between anxiety and depression? Am. J. Med. Genet. Part C: Semin. Med. Genet. 2008, 148C, 140–146. [Google Scholar] [CrossRef]
- Bittner, A.; Goodwin, R.D.; Wittchen, H.-U.; Beesdo, K.; Höfler, M.; Lieb, R. What characteristics of primary anxiety disorders predict subsequent major depressive disorder? J. Clin. Psychiatry 2004, 65, 618–626. [Google Scholar] [CrossRef]
- Sandi, C.; Richter-Levin, G. From high anxiety trait to depression: A neurocognitive hypothesis. Trends Neurosci. 2009, 32, 312–320. [Google Scholar] [CrossRef]
- Weger, M.; Sandi, C. High anxiety trait: A vulnerable phenotype for stress-induced depression. Neurosci. Biobehav. Rev. 2018, 87, 27–37. [Google Scholar] [CrossRef]
- Lockefeer, J.P.M.; De Vries, J. What is the relationship between trait anxiety and depressive symptoms, fatigue, and low sleep quality following breast cancer surgery? Psycho-Oncology 2012, 22, 1127–1133. [Google Scholar] [CrossRef]
- De Vries, J.; Van Der Steeg, A.F.; Roukema, J.A. Trait anxiety determines depressive symptoms and fatigue in women with an abnormality in the breast. Br. J. Health Psychol. 2009, 14, 143–157. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.A.; Beck, A.T. Cognitive theory and therapy of anxiety and depression: Convergence with neurobiological findings. Trends Cogn. Sci. 2010, 14, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Li, M.; Xu, S.; Liu, B.; Wu, T.; Lu, F.; Xie, J.; Peng, L.; Wang, J. Relations between trait anxiety and depression: A mediated moderation model. J. Affect. Disord. 2019, 244, 217–222. [Google Scholar] [CrossRef]
- Mor, N.; Haran, D. Cognitive-behavioral therapy for depression. Isr. J. Psychiatry Relat. Sci. 2009, 46, 269–273. [Google Scholar] [PubMed]
- COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/country/greece/ (accessed on 22 March 2022).
- Health at a Glance: Europe 2020 State of Health in the EU Cycle. Available online: https://ec.europa.eu/health/system/files/2020-12/2020_healthatglance_rep_en_0.pdf (accessed on 22 March 2022).
- Sikaras, C.; Ilias, I.; Tselebis, A.; Pachi, A.; Zyga, S.; Tsironi, M.; Gil, A.P.R.; Panagiotou, A. Nursing staff fatigue and burnout during the COVID-19 pandemic in Greece. AIMS Public Health 2021, 9, 94–105. [Google Scholar] [CrossRef]
- De Vries, J.; Michielsen, H.; Van Heck, G.L.; Drent, M. Measuring fatigue in sarcoidosis: The Fatigue Assessment Scale (FAS). Br. J. Health Psychol. 2004, 9, 279–291. [Google Scholar] [CrossRef] [Green Version]
- Alikari, V.; Fradelos, E.; Sachlas, A.; Panoutsopoulos, G.; Lavdaniti, M.; Palla, P.; Lappa, T.; Giatrakou, S.; Stathoulis, J.; Babatsikou, F.; et al. Reliability and validity of the Greek version of “The Fatigue Assessment Scale”. Arch. Hell. Med. 2016, 33, 231–238. [Google Scholar]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbauch, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Donias, S.; Demertzis, I. Validation of the Beck depression inventory. In 10th Hellenic Congress of Neurology and Psychiatry; Varfis, G., Ed.; University Studio Press: Thessaloniki, Greece, 1983; pp. 486–492. (In Greek) [Google Scholar]
- Pachi, A.; Sikaras, C.; Ilias, I.; Panagiotou, A.; Zyga, S.; Tsironi, M.; Baras, S.; Tsitrouli, L.A.; Tselebis, A. Burnout, Depression and Sense of Coherence in Nurses during the Pandemic Crisis. Healthcare 2022, 10, 134. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, P.R.; Vagg, P.R.; Jacobs, G.A. Manual for the State–Trait Spielberger Anxiety Inventory (Form Y); Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Fountoulakis, K.N.; Papadopoulou, M.; Kleanthous, S.; Papadopoulou, A.; Bizeli, V.; Nimatoudis, I.; Iacovides, A.; Kaprinis, G.S. Reliability and psychometric properties of the Greek translation of the State-Trait Anxiety Inventory form Y: Preliminary data. Ann. Gen. Psychiatry 2006, 5, 2. [Google Scholar] [CrossRef] [Green Version]
- Tselebis, A.; Gournas, G.; Tzitzanidou, G.; Panagiotou, A.; Ilias, I. Anxiety and Depression in Greek Nursing and Medical Personnel. Psychol. Rep. 2006, 99, 93–96. [Google Scholar] [CrossRef]
- World Health Organization. Pandemic fatigue: Reinvigorating the Public to Prevent COVID-19. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/335820/WHO-EURO-2020-1160-40906-55390-eng.pdf (accessed on 3 April 2022).
- Labrague, L.J. Pandemic fatigue and clinical nurses’ mental health, sleep quality and job contentment during the COVID-19 pandemic: The mediating role of resilience. J. Nurs. Manag. 2021, 29, 1992–2001. [Google Scholar] [CrossRef] [PubMed]
- Johnston, D.W.; Allan, J.L.; Powell, D.J.H.; Jones, M.C.; Farquharson, B.; Bell, C.; Johnston, M. Why does work cause fatigue? A real-time investigation of fatigue, and determinants of fatigue in nurses working 12-hour shifts. Ann. Behav. Med. 2018, 53, 551–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wittchen, H.-U.; Zhao, S.; Kessler, R.C.; Eaton, W.W. DSM-III-R Generalized Anxiety Disorder in the National Comorbidity Survey. Arch. Gen. Psychiatry 1994, 51, 355–364. [Google Scholar] [CrossRef]
- Leach, L.S.; Christensen, H.; Mackinnon, A.J. Gender differences in the endorsement of symptoms for depression and anxiety: Are gender-biased items responsible? J. Nerv. Ment. Dis. 2008, 196, 128–135. [Google Scholar] [CrossRef]
- Weissman, M.M.; Klerman, G.L. Sex differences and the epidemiology of depression. Arch. Gen. Psychiatry 1977, 34, 98–111. [Google Scholar] [CrossRef] [PubMed]
- Jorm, A. Sex and Age Differences in Depression: A Quantitative Synthesis of Published Research. Aust. New Zealand J. Psychiatry 1987, 21, 46–53. [Google Scholar] [CrossRef]
- Kuehner, C. Gender differences in unipolar depression: An update of epidemiological findings and possible explanations. Acta Psychiatr. Scand. 2003, 108, 163–174. [Google Scholar] [CrossRef]
- Faravelli, C.; Alessandra Scarpato, M.; Castellini, G.; Lo Sauro, C. Gender differences in depression and anxiety: The role of age. Psychiatry Res. 2013, 210, 1301–1303. [Google Scholar] [CrossRef]
- Leach, L.S.; Christensen, H.; Mackinnon, A.J.; Windsor, T.D.; Butterworth, P. Gender differences in depression and anxiety across the adult lifespan: The role of psychosocial mediators. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 983–998. [Google Scholar] [CrossRef]
- Jang, H.J.; Kim, O.; Kim, S.; Kim, M.S.; Choi, J.A.; Kim, B.; Dan, H.; Jung, H. Factors Affecting Physical and Mental Fatigue among Female Hospital Nurses: The Korea Nurses’ Health Study. Healthcare 2021, 9, 201. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.F.; Kroenke, K. Cancer-related fatigue and its associations with depression and anxiety: A systematic review. Psychosomatics 2009, 50, 440–447. [Google Scholar] [CrossRef]
- Polikandrioti, M.; Tzirogiannis, K.; Zyga, S.; Koutelekos, I.; Vasilopoulos, G.; Theofilou, P.; Panoutsopoulos, G. Effect of anxiety and depression on the fatigue of patients with a permanent pacemaker. Arch. Med. Sci. Atheroscler. Dis. 2018, 3, 8–17. [Google Scholar] [CrossRef]
- Kim, S.C.; Rankin, L.; Ferguson, J. Nurses’ mental health from early COVID-19 pandemic to vaccination. J. Nurs. Scholarsh. 2021, 54, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Heath, C.; Sommerfield, A.; Von Ungern-Sternberg, B.S. Resilience strategies to manage psychological distress among healthcare workers during the COVID-19 pandemic: A narrative review. Anaesthesia 2020, 75, 1364–1371. [Google Scholar] [CrossRef] [PubMed]
- Querstret, D.; O’Brien, K.; Skene, D.J.; Maben, J. Improving fatigue risk management in healthcare: A systematic scoping review of sleep-related/fatigue-management interventions for nurses and midwives. Int. J. Nurs. Stud. 2019, 106, 103513. [Google Scholar] [CrossRef]
- Martin-Anatias, N.; Simpson, N.; Sterling, R.; Trnka, S.; Tunufa’i, L. Community healthcare workers’ experiences during and after COVID-19 lockdown: A qualitative study from Aotearoa New Zealand. Health Soc. Care Community 2022, 30, e2761–e2771. [Google Scholar]
- Steege, L.M.; Pinekenstein, B.J.; Rainbow, J.G.; Arsenault Knudsen, É. Addressing Occupational Fatigue in Nurses: Current State of Fatigue Risk Management in Hospitals, Part 1. J. Nurs. Adm. 2017, 47, 426–433. [Google Scholar] [CrossRef]
- Tselebis, A.; Bratis, D.; Karkanias, A.; Apostolopoulou, E.; Gournas, G.; Moussas, G.; Ilias, I. Associations on Dimensions of Burnout and Family Support for a Sample of Greek Nurses. Psychol. Rep. 2008, 103, 63–66. [Google Scholar] [CrossRef]
- Bratis, D.; Tselebis, A.; Sikaras, C.; Moulou, A.; Giotakis, K.; Zoumakis, E.; Ilias, I. Alexithymia and its association with burnout, depression and family support among Greek nursing staff. Hum. Resour. Heath 2009, 7, 72. [Google Scholar] [CrossRef] [Green Version]
- Tiger, M.; Wesselhoeft, R.; Karlsson, P.; Handal, M.; Bliddal, M.; Cesta, C.E.; Skurtveit, S.; Reutfors, J. Utilization of antidepressants, anxiolytics, and hypnotics during the COVID-19 pandemic in Scandinavia. J. Affect. Disord. 2023, 323, 292–298. [Google Scholar] [CrossRef] [PubMed]
- González-López, M.D.C.; Díaz-Calvo, V.; Ruíz-González, C.; Nievas-Soriano, B.J.; Rebollo-Lavado, B.; Parrón-Carreño, T. Consumption of Psychiatric Drugs in Primary Care during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 4782. [Google Scholar] [CrossRef] [PubMed]
- Knap, M.; Maciąg, D.; Trzeciak-Bereza, E.; Knap, B.; Czop, M.; Krupa, S. Sleep Disturbances and Health Consequences Induced by the Specificity of Nurses’ Work. Int. J. Environ. Res. Public Health 2022, 19, 9802. [Google Scholar] [CrossRef] [PubMed]
- Tselebis, A.; Zoumakis, E.; Ilias, I. Dream Recall/Affect and the Hypothalamic–Pituitary–Adrenal Axis. Clocks Sleep 2021, 3, 403–408. [Google Scholar] [CrossRef]
- Cho, H.; Steege, L.M. Nurse Fatigue and Nurse, Patient Safety, and Organizational Outcomes: A Systematic Review. West. J. Nurs. Res. 2021, 43, 1157–1168. [Google Scholar] [CrossRef]
- Thorsteinsson, E.B.; Brown, R.F.; Owens, M.T. Modeling the Effects of Stress, Anxiety, and Depression on Rumination, Sleep, and Fatigue in a Nonclinical Sample. J. Nerv. Ment. Dis. 2019, 207, 355–359. [Google Scholar] [CrossRef]
- Dragioti, E.; Tsartsalis, D.; Mentis, M.; Mantzoukas, S.; Gouva, M. Impact of the COVID-19 pandemic on the mental health of hospital staff: An umbrella review of 44 meta-analyses. Int. J. Nurs. Stud. 2022, 131, 104272. [Google Scholar] [CrossRef]
- Italia, S.; Costa, C.; Briguglio, G.; Mento, C.; Muscatello, M.R.A.; Alibrandi, A.; Filon, F.L.; Spatari, G.; Teodoro, M.; Fenga, C. Quality of Life, Insomnia and Coping Strategies during COVID-19 Pandemic in Hospital Workers. A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 12466. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Participants | Descriptive Statistics | Age | Work Experience (in Years) | Fatigue Assessment Scale | State Anxiety Inventory | Trait Anxiety Inventory | Beck Depression Inventory |
|---|---|---|---|---|---|---|---|
| Male N = 69 | Mean | 41.16 | 15.60 | 21.25 ** | 35.47 ** | 36.32 ** | 7.06 * |
| SD | 11.37 | 11.67 | 7.43 | 12.14 | 11.35 | 7.15 | |
| Female N = 335 | Mean | 43.23 | 18.45 | 24.66 ** | 40.18 ** | 40.30 ** | 9.33 * |
| SD | 10.79 | 12.02 | 7.20 | 11.59 | 10.52 | 7.48 | |
| Total N = 404 | Mean | 42.88 | 17.96 | 24.08 | 39.38 | 39.62 | 8.94 |
| SD | 10.90 | 12.00 | 7.35 | 11.80 | 10.76 | 7.46 |
| Pearson Correlation N = 404 | AGE | Work Experience (in Years) | Fatigue Assessment Scale | State Anxiety Inventory | Trait Anxiety Inventory | |
|---|---|---|---|---|---|---|
| Work Experience (in Years) | r | 0.885 ** | ||||
| p | 0.001 | |||||
| Fatigue Assessment Scale | r | −0.096 | −0.082 | |||
| p | 0.055 | 0.104 | ||||
| Spielberger State Anxiety Inventory | r | −0.056 | −0.06 | 0.635 ** | ||
| p | 0.258 | 0.232 | 0.001 | |||
| Spielberger Trait Anxiety Inventory | r | −0.101 * | −0.094 | 0.715 ** | 0.789 ** | |
| p | 0.043 | 0.064 | 0.001 | 0.001 | ||
| Beck Depression Inventory | r | 0.003 | 0.001 | 0.707 ** | 0.603 ** | 0.750 ** |
| p | 0.951 | 0.991 | 0.001 | 0.001 | 0.001 | |
| Dependent Variable: Fatigue Assessment Scale | R Square | R Square Change | Beta | t | p | Durbin-Watson |
|---|---|---|---|---|---|---|
| Spielberger Trait Anxiety Inventory | 0.517 | 0.517 | 0.297 | 4.68 | 0.01 * | 1.945 |
| Beck Depression Inventory | 0.577 | 0.062 | 0.373 | 7.58 | 0.01 * | |
| Spielberger State Anxiety Inventory | 0.591 | 0.012 | 0.180 | 3.43 | 0.01 * |
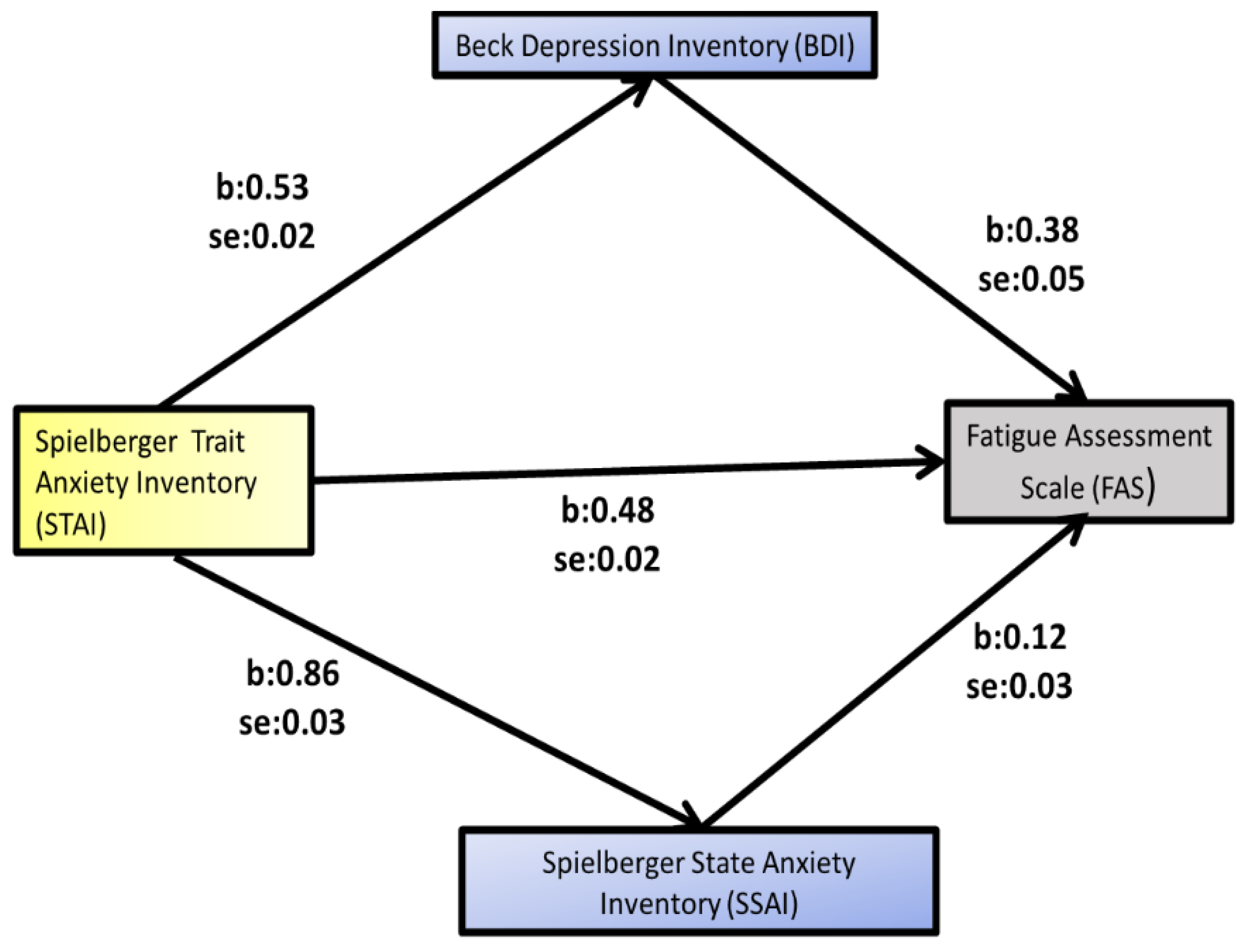
| Variable | b | SE | t | p | 95% Confidence Interval | ||
|---|---|---|---|---|---|---|---|
| LLCI | ULCI | ||||||
| STAI → BDI | 0.5256 | 0.0233 | 22.5438 | 0.001 | 0.4798 | 0.5715 | |
| STAI → SSAI | 0.8575 | 0.0347 | 24.7243 | 0.001 | 0.7993 | 0.9257 | |
| STAI → BDI → FAS | 0.3744 | 0.0484 | 7.7436 | 0.001 | 0.2794 | 0.4695 | |
| STAI → SSAI → FAS | 0.1107 | 0.0325 | 3.4066 | 0.001 | 0.0468 | 0.1747 | |
| STAI → FAS | 0.4803 | 0.0242 | 19.8655 | 0.001 | 0.4237 | 0.5278 | |
| Effects | |||||||
| Direct | 0.1885 | 0.0433 | 4.3516 | 0.001 | 0.1033 | 0.2736 | |
| Indirect ** | Total | 0.2918 | 0.0399 | 0.2158 | 0.3689 | ||
| BDI | 0.1968 | 0.0311 | 0.1368 | 0.2587 | |||
| SSAI | 0.095 | 0.0262 | 0.0446 | 0.1471 | |||
| Total (STAI → FAS) | 0.4803 | 0.0242 | 19.8655 | 0.001 | 0.4327 | 0.5278 | |
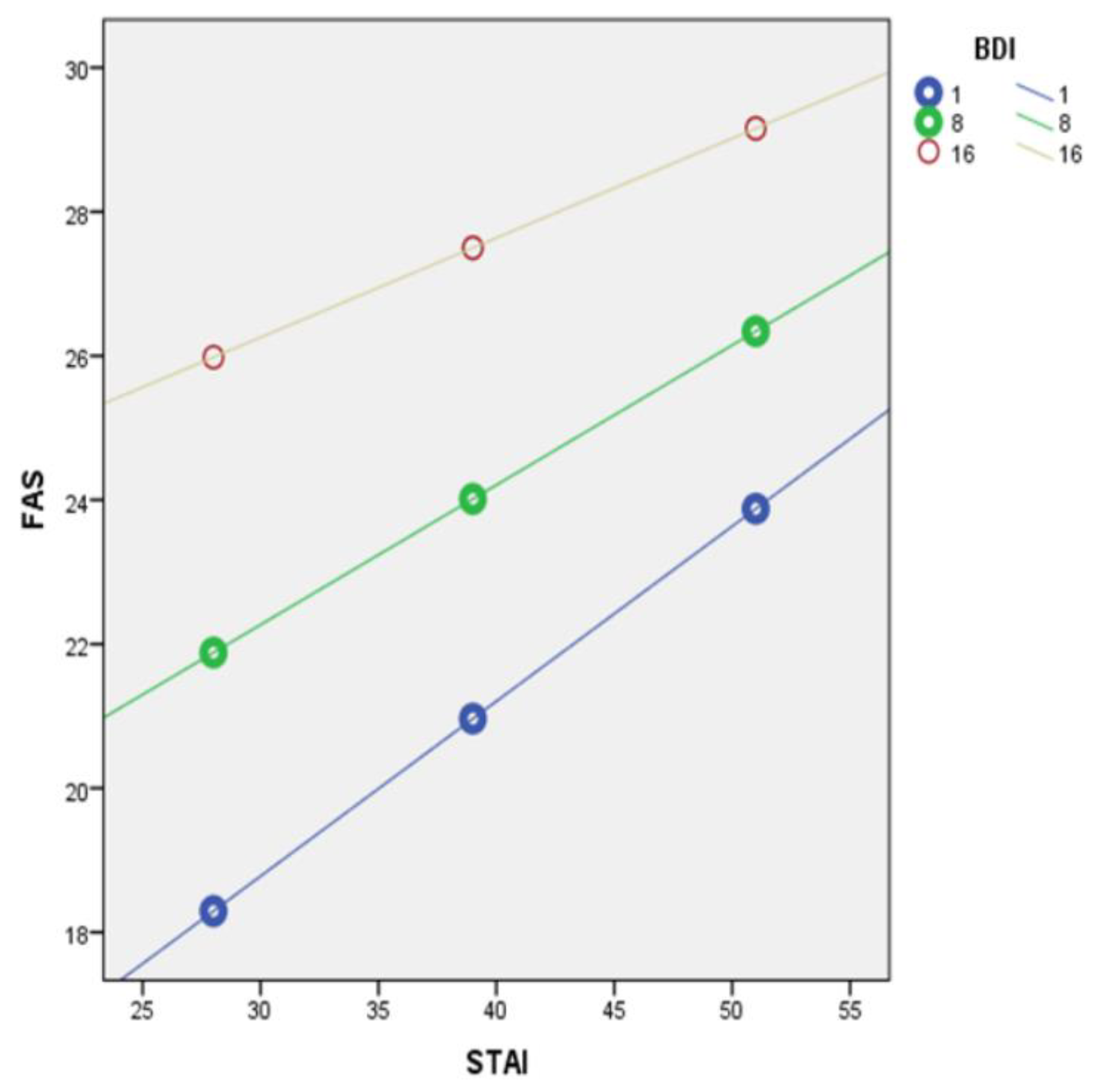
| Outcome Variable: Fatigue Assessment Scale (FAS) | b | SE | t | p |
|---|---|---|---|---|
| Constant | 7.3902 [3.1924, 11.5880] | 2.1351 | 3.4614 | 0.01 |
| Spielberger Trait Anxiety Inventory (STAI) | 0.2498 [0.1563, 0.3432] | 0.0475 | 5.2561 | 0.01 |
| Beck Depression Inventory (BDI) | 0.7079 [0.4694, 0.9465] | 0.1213 | 5.834 | 0.01 |
| Interaction(STAI × BDI) | −0.0070 [−0.0116, −0.0024] | 0.0023 | −2.9908 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sikaras, C.; Zyga, S.; Tsironi, M.; Tselebis, A.; Pachi, A.; Ilias, I.; Panagiotou, A. The Mediating Role of Depression and of State Anxiety οn the Relationship between Trait Anxiety and Fatigue in Nurses during the Pandemic Crisis. Healthcare 2023, 11, 367. https://doi.org/10.3390/healthcare11030367
Sikaras C, Zyga S, Tsironi M, Tselebis A, Pachi A, Ilias I, Panagiotou A. The Mediating Role of Depression and of State Anxiety οn the Relationship between Trait Anxiety and Fatigue in Nurses during the Pandemic Crisis. Healthcare. 2023; 11(3):367. https://doi.org/10.3390/healthcare11030367
Chicago/Turabian StyleSikaras, Christos, Sofia Zyga, Maria Tsironi, Athanasios Tselebis, Argyro Pachi, Ioannis Ilias, and Aspasia Panagiotou. 2023. "The Mediating Role of Depression and of State Anxiety οn the Relationship between Trait Anxiety and Fatigue in Nurses during the Pandemic Crisis" Healthcare 11, no. 3: 367. https://doi.org/10.3390/healthcare11030367