
Systematic Review of Penetrating Cardiac Injury by a Firearm: Forensic Implications

 ,
,  , ,
, ,
Abstract
:1. Introduction
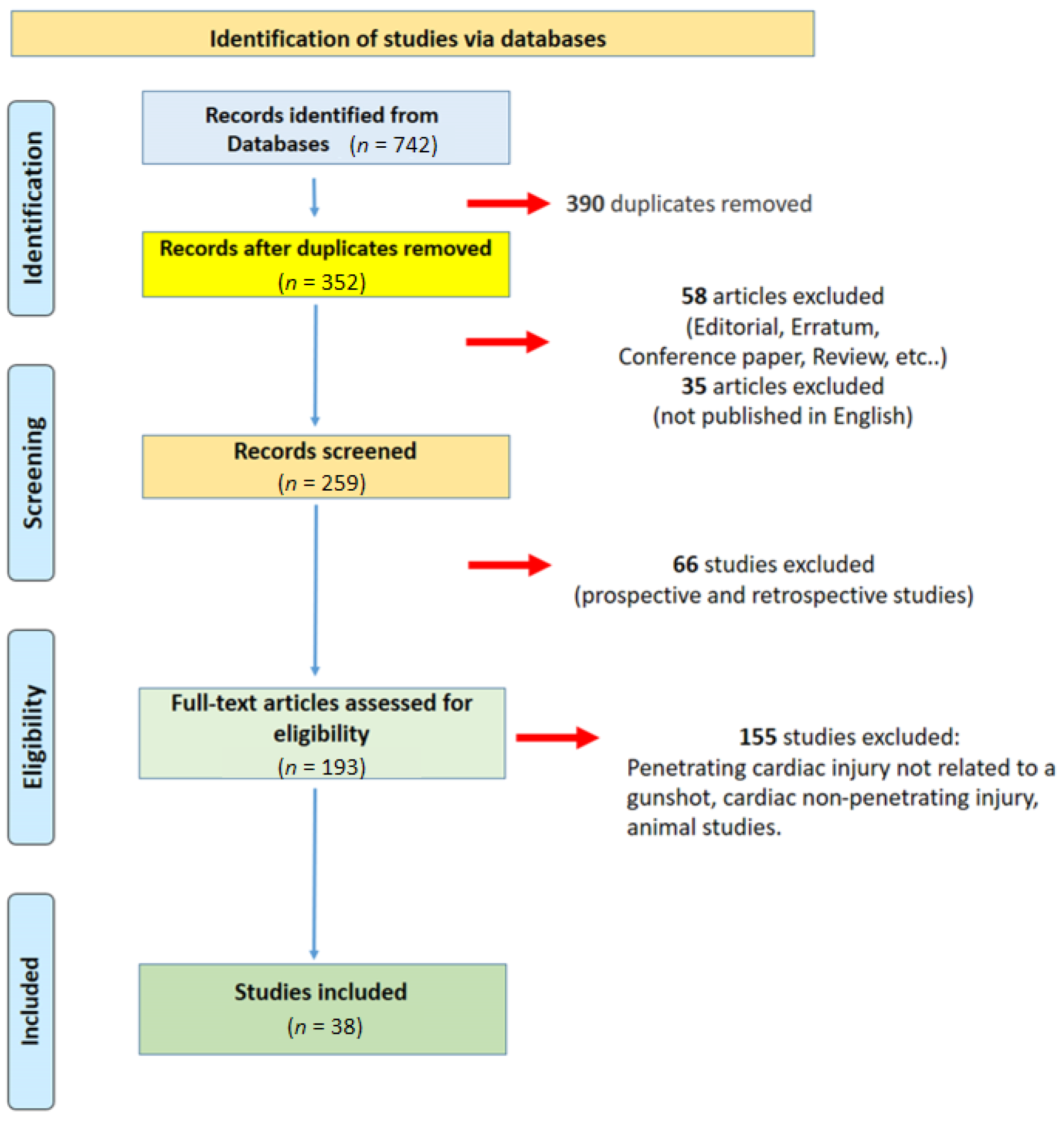
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Quality Assessment and Data Extraction
2.3. Characteristics of Eligible Studies
3. Results
4. Discussion
- √
- Area and severity of the heart injury;
- √
- Duration of transport and intervention;
- √
- Contemporary lesion to other organ/s;
- √
- The quantity of blood lost;
- √
- Presence/absence of cardiac tamponade.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Šimek, M.; Konečný, J.; Hájek, R.; Čižmář, I.; Kutěj, V.; Lonský, V. Penetrating Injuries of the Heart and Great Vessels-Fifteen Years of Experience of the Cardiac Surgery Service as a Part of the Major Trauma Centre. Acta Chir. Orthop. Traumatol. Cechoslov. 2018, 85, 144–148. [Google Scholar]
- Ingraham, A.; Sperry, J. Operative Management of Cardiac Injuries: Diagnosis, Technique, and Postoperative Complications. Curr. Trauma Rep. 2015, 1, 225–231. [Google Scholar] [CrossRef]
- Dokoupil, M.; Marecová, K.; Uvíra, M.; Joukal, M.; Mrázková, E.; Chmelová, J.; Handlos, P. Fatal delayed hemopericardium and hemothorax following blunt chest trauma. Forensic Sci. Med. Pathol. 2019, 15, 272–275. [Google Scholar] [CrossRef] [PubMed]
- Karaca, M.A. Evaluation of Gunshot Wounds in the Emergency Department. Turk. J. Trauma Emerg. Surg. 2015, 21, 248–255. [Google Scholar] [CrossRef] [Green Version]
- Mina, M.J.; Jhunjhunwala, R.; Gelbard, R.B.; Dougherty, S.D.; Carr, J.S.; Dente, C.J.; Nicholas, J.M.; Wyrzykowski, A.D.; Salomone, J.P.; Vercruysse, G.A.; et al. Factors affecting mortality after penetrating cardiac injuries: 10-year experience at urban level I trauma center. Am. J. Surg. 2017, 213, 1109–1115. [Google Scholar] [CrossRef]
- Topal, A.E.; Celik, Y.; Eren, M.N. Predictors of Outcome in Penetrating Cardiac Injuries. J. Trauma 2010, 69, 574–578. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Kang, N.; Hsee, L.; Rizoli, S.; Alison, P. Penetrating cardiac injury: Overcoming the limits set by Nature. Injury 2009, 40, 919–927. [Google Scholar] [CrossRef]
- Ovali, C.; Kocaoglu, A.S.; Demirdizen, G.; Aydar, Y. Penetrating Heart Injury Repaired with Peripheral Cannulation: Case Report. Prehosp. Disaster. Med. 2021, 36, 793–796. [Google Scholar] [CrossRef]
- Tran, D.; Jones, D.; Moore, R.; Guarneri, R. Abdominal Aorta Bullet Embolism: Presentation and Management. Ann. Vasc. Surg. 2021, 74, 524.e17–524.e21. [Google Scholar] [CrossRef]
- Lovasik, B.P.; Nauser, C.L.; Klingensmith, N.J.; Nguyen, J.H. Bullet Embolism into the Common Iliac Artery from a Gunshot Wound to the Heart. Am. Surg. 2021, 88, 1014–1015. [Google Scholar] [CrossRef] [PubMed]
- Romero-Velez, G.; Kaban, J.M.; Chao, E.; Lewis, E.R.; Stone, M.E.J.; Teperman, S.; Reddy, S.H. Use of the EVARREST Patch for Penetrating Cardiac Injury. Trauma Case Rep. 2020, 28, 100324. [Google Scholar] [CrossRef] [PubMed]
- Knowlin, L.T.; McAteer, J.P.; Kane, T.D. Cardiac Injury Following Penetrating Chest Trauma: Delayed Diagnosis and Successful Repair. J. Pediatr. Surg. Case Rep. 2018, 39, 45–47. [Google Scholar] [CrossRef]
- Cvetković, D.; Živković, V.; Juković, F.; Nikolić, S. Double suicidal gunshot wounds to the heart. Forensic Sci. Med. Pathol. 2017, 14, 248–250. [Google Scholar] [CrossRef] [PubMed]
- Rupprecht, H.; Gaab, K. Delayed Cardiac Rupture Induced by Traumatic Myocardial Infarction: Consequence of a 45-Magnum Blast Injury; A Comprehensive Case Review. Bull. Emerg. Trauma 2018, 6, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volpe, M.A.; Paredes, J.E.M.; Redigolo, L.C.; Sanchez, I.S.M.; Lanichek, F.; Silveira, L.Z.D. Heart Injury with Projectile Lodged Inside the Heart. Rev. Bras. de Cir. Cardiovasc. 2018, 33, 303–305. [Google Scholar] [CrossRef] [PubMed]
- Abou-Leila, A.; Voronov, G. The journey of harmless bullet: The perioperative care of penetrating cardiac injury. Anesthesia Essays Res. 2017, 11, 790–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, E.C.L.; Tchaick, R.M.; Ferraz, D.L.D.M.; Oliveira, J.P.S.D.P.; Figueira, F.A.M.D.S.; Lima, G.A.D.F.C.A. Embolization by Bullet Dislodged from the Heart. Rev. Bras. Cir. Cardiovasc. 2017, 32, 539–541. [Google Scholar] [CrossRef] [Green Version]
- Fu, H.-Y.; Ting, M.; Wang, Y.-C.; Yu, H.-Y. Intracardiac foreign body resulting from a transmediastinal gunshot mimics an extracardiac foreign body: An image presentation. J. Formos. Med. Assoc. 2017, 116, 815–818. [Google Scholar] [CrossRef]
- Imbert, P.-Y.; Goin, G.; Goudard, Y.; De La Villéon, B.; Bonnet, P.-M.; Sockeel, P.; Pauleau, G. Pulmonary Artery Bullet Embolism Following Cardiac Gunshot Wound. Ann. Vasc. Surg. 2016, 36, e11–e290. [Google Scholar] [CrossRef]
- Sapkota, R.; Koirala, B. Traumatic Pseudoaneurysm of the Heart. Gen. Thorac. Cardiovasc. Surg. 2016, 64, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Kaya, A.; Caliskan, E.; Tatlisu, M.A.; Hayiroglu, M.I.; Tekessin, A.I.; Cakilli, Y.; Avsar, S.; Oz, A.; Uzman, O. A Retained Bullet in Pericardial Sac: Penetrating Gunshot Injury of the Heart. Case Rep. Cardiol. 2016, 2016, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konecny, J.; Klvacek, A.; Simek, M.; Lonsky, V.; Santavy, P. Complex gunshot injury to the heart as a consequence of suicide attempt in a schizophrenic patient. Int. J. Surg. Case Rep. 2016, 24, 80–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obrador, L.Z.; Al-Lal, Y.M.; Palacios, J.D.T.; Prats, I.A.; Fuentes, F.T. Transmediastinal and Transcardiac Gunshot Wound with Hemodynamic Stability. Case Rep. Surg. 2014, 2014, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Siddiqui, F.A.; Kabeer, J.; Shahabuddin, S. Surviving shot through the heart: Management in two cases. J. Pak. Med Assoc. 2015, 65, 93–94. [Google Scholar]
- Suzuki, T.; Wada, T.; Funaki, S.; Abe, H.; Seki, I.; Imaki, S.; Nakazawa, A. Traumatic left ventricular free-wall laceration by a gunshot: Report of a case. Surg. Today 2012, 44, 1152–1155. [Google Scholar] [CrossRef]
- Rasool, S.H.; Arif, M.; Arain, G.M. Right Ventricle Injury by Stray Bullet. Pak. J. Med. Health Sci. 2014, 8, 1133–1134. [Google Scholar]
- Mills, E.E.; Birnbaum, P.L.; Davis, J.W. Asymptomatic Gunshot Wound to the Heart with Retained Intracardiac Pellet. Ann. Thorac. Surg. 2014, 97, e15–e16. [Google Scholar] [CrossRef]
- Bonsignore, A.; Bernucci, L.V.; Canepa, M.; Ventura, F. Suicide Due to Four Speargun Shots. Am. J. Forensic Med. Pathol. 2013, 34, 201–204. [Google Scholar] [CrossRef]
- Porcu, P.; Moreau-Gaudry, A.; Chavanon, O.; Blin, D. Haemostasis of a right ventricle-gunshot wound using a novel haemostatic vacuum device. Interact. Cardiovasc. Thorac. Surg. 2012, 15, 294–296. [Google Scholar] [CrossRef] [Green Version]
- Branch, C.F.; Adams, J. Left Ventricular Rupture with Resulting Cardiac Tamponade Due to Blast Force Trauma from Gunshot Wound. J. Emerg. Med. 2012, 43, 263–265. [Google Scholar] [CrossRef] [PubMed]
- Karigyo, C.J.T.; Fan, O.G.; Rodrigues, R.J.; Tarasiewich, M.J. Ferimento cardíaco transfixante por projétil de arma de fogo: Relato de caso. Rev. Bras. de Cir. Cardiovasc. 2011, 26, 298–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ustin, J.S.; Sinha, P.S.; Kelly, K.B. Sheehan-like syndrome in a pregnant patient with a cardiac gunshot wound. Inj. Extra 2011, 42, 61–63. [Google Scholar] [CrossRef]
- Hartert, M.; Dahm, M.; Neufang, A.; Vahl, C.-F. Minimum Cause--Maximum Effect: The Travelogue of a Bullet. Interact. Cardiovasc. Thorac. Surg. 2010, 11, 698–700. [Google Scholar] [CrossRef] [Green Version]
- Ellertson, D.G.; Johnson, S.B. Total Inflow Occlusion to Repair a Penetrating Cardiac Injury: Case Report. J. Trauma: Inj. Infect. Crit. Care 2008, 64, 1628–1629. [Google Scholar] [CrossRef]
- de Giorgio, F.; Rainio, J. Two Entrances, One Exit—An Atypical Shotgun Injury: A Case Report. Med. Sci. Law 2007, 47, 353–356. [Google Scholar] [CrossRef]
- Incorvaia, A.N.; Poulos, D.M.; Jones, R.N.; Tschirhart, J.M. Can a Falling Bullet Be Lethal at Terminal Velocity? Cardiac Injury Caused by a Celebratory Bullet. Ann. Thorac. Surg. 2007, 83, 283–284. [Google Scholar] [CrossRef]
- Faschingbauer, M.; Schulz, A.P.; Jürgens, C. Cardial Gunshot Injury: Treatment in a Trauma Hospital without a Cardiac Unit. Eur. J. Emerg. Med. 2006, 13, 238–241. [Google Scholar] [CrossRef]
- Meira, E.B.D.S.; Guidugli, R.B.; Meira, D.B.D.S.; Rocha, R.M.; Ghefter, M.C.; Richter, I. Abordagem terapêutica dos projéteis retidos no coração. Rev. Bras. de Cir. Cardiovasc. 2005, 20, 91–93. [Google Scholar] [CrossRef] [Green Version]
- Bali, H.K.; Vijayvergiya, R.; Banarjee, S.; Kumar, N. Gunshot injury of the heart: An unusual cause of acute myocardial infarction. Tex. Hear. Inst. J. 2003, 30, 158–160. [Google Scholar]
- Habdank, K.; Nolan, R.L. Gunshot Wound to the Thorax with Bullet Embolization to the External Carotid Artery. J. Thorac. Imaging 2003, 18, 42–44. [Google Scholar] [CrossRef]
- Kurt, N.; Küçük, H.F.; Celik, G.; Demirhan, R.; Celik, G.; Gül, O.; Ektirici, S.; Gülmen, M. Bullet Embolism of the Right External Iliac Artery Following Cardiac Gunshot Wound (a Case Report). Ulus. Travma Derg. 2001, 7, 131–133. [Google Scholar]
- Doty, J.R.; Cameron, D.E.; Elmaci, T.; Salomon, N.W. Penetrating Trauma to the Tricuspid Valve and Ventricular Septum: Delayed Repair. Ann. Thorac. Surg. 1999, 67, 252–253. [Google Scholar] [CrossRef]
- Kwan, T.; Salciccioli, L.; Elsakr, A.; Burack, J.; Feit, A. Coronary artery fistula coexisting with a ventricular septal defect due to a penetrating gunshot wound. Catheter. Cardiovasc. Diagn. 1995, 34, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Wait, M.A.; Mueller, M.; Barth, M.J.; Brickner, E.; Salman, T.; Jessen, M.E. Traumatic coronary sinocameral fistula from a penetrating cardiac injury. J. Trauma 1994, 36, 894–897. [Google Scholar] [CrossRef] [PubMed]
- Skipper, R.; Dębski, R. Intramyocardial Shotgun Pellets Diagnosed on Initial Emergency Room Chest X-ray. J. Trauma 1990, 30, 1609–1610. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Liberto, A.; Zuccarello, P.; Ministeri, F.; Licciardello, G.; Barbera, N.; Sessa, F.; Salerno, M. Heart rupture as an acute complication of cocaine abuse: A case report. Leg. Med. 2022, 58, 102084. [Google Scholar] [CrossRef]
- Montisci, M.; Thiene, G.; Ferrara, S.D.; Basso, C. Cannabis and Cocaine: A Lethal Cocktail Triggering Coronary Sudden Death. Cardiovasc. Pathol. 2008, 17, 344–346. [Google Scholar] [CrossRef]
- Sessa, F.; Esposito, M.; Messina, G.; Di Mizio, G.; Di Nunno, N.; Salerno, M. Sudden Death in Adults: A Practical Flow Chart for Pathologist Guidance. Healthcare 2021, 9, 870. [Google Scholar] [CrossRef]
- Turillazzi, E.; Bello, S.; Neri, M.; Pomara, C.; Riezzo, I.; Fineschi, V. Cardiovascular effects of cocaine: Cellular, ionic and molecular mechanisms. Curr. Med. Chem. 2012, 19, 5664–5676. [Google Scholar] [CrossRef]
- Cerretani, D.; Bello, S.; Cantatore, S.; Fiaschi, A.; Montefrancesco, G.; Neri, M.; Pomara, C.; Riezzo, I.; Fiore, C.; Bonsignore, A.; et al. Acute administration of 3,4-methylenedioxymethamphetamine (MDMA) induces oxidative stress, lipoperoxidation and TNFα-mediated apoptosis in rat liver. Pharmacol. Res. 2011, 64, 517–527. [Google Scholar] [CrossRef] [PubMed]
- Asensio, J.A.; Petrone, P.; Pereira, B.; Peña, D.; Prichayudh, S.; Tsunoyama, T.; Ruiz, F.; Marttos, A.; Capin, A.; De Marchena, E. Penetrating Cardiac Injuries: A Historic Perspective and Fascinating Trip Through Time. J. Am. Coll. Surg. 2009, 208, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Naughton, M.J.; Brissie, R.M.; Bessey, P.Q.; Mceachern, M.M.; Donald, J.M.; Laws, H.L. Demography of Penetrating Cardiac Trauma. Ann. Surg. 1989, 209, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Campbell, N.C.; Thomson, S.R.; Muckart, D.J.J.; Meumann, C.M.; Van Middelkoop, I.; Botha, J.B.C. Review of 1198 cases of penetrating cardiac trauma. Br. J. Surg. 1997, 84, 1737–1740. [Google Scholar] [CrossRef] [PubMed]
- Mittal, V.; McAleese, P.; Young, S.; Cohen, M. Penetrating Cardiac Injuries. Am. Surg. 1999, 65, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Asensio, J. Penetrating Cardiac Injuries: A Prospective Study of Variables Predicting Outcomes. J. Am. Coll. Surg. 1998, 186, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Asensio, J.A.; Berne, J.D.; Demetriades, D.; Chan, L.; Murray, J.; Falabella, A.; Gomez, H.; Chahwan, S.; Velmahos, G.; Cornwell, E.E.; et al. One Hundred Five Penetrating Cardiac Injuries: A 2-Year Prospective Evaluation. J. Trauma Acute Care Surg. 1998, 44, 1073–1082. [Google Scholar] [CrossRef]
- Asensio, J.A.; Soto, S.N.; Forno, W.; Roldan, G.; Petrone, P.; Salim, A.; Rowe, V.; Demetriades, D. Penetrating cardiac injuries: A complex challenge. Injury 2001, 32, 533–543. [Google Scholar] [CrossRef]
- Tyburski, J.G.; Astra, L.; Wilson, R.F.; Dente, C.; Steffes, C. Factors Affecting Prognosis with Penetrating Wounds of the Heart. J. Trauma Inj. Infect. Crit. Care 2000, 48, 587–591. [Google Scholar] [CrossRef]
- Mitchell, M.E.; Muakkassa, F.F.; Poole, G.V.; Rhodes, R.S.; Griswold, J.A. Surgical approach of choice for penetrating cardiac wounds. J. Trauma Inj. Infect. Crit. Care 1993, 34, 17–20. [Google Scholar] [CrossRef]
- Crandall, M.; Sharp, D.; Unger, E.; Straus, D.; Brasel, K.; Hsia, R.; Esposito, T. Trauma Deserts: Distance from a Trauma Center, Transport Times, and Mortality from Gunshot Wounds in Chicago. Am. J. Public Health 2013, 103, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Tanmoy, G.; Kumar, S.K.; Chaitali, S.; Chiranjib, B.; Manasij, M. Thoracic Gunshot Wound: A Report of 3 Cases and Review of Management [Heridas de Bala Torácicas: Informe de 3 Casos y Revisión de La Conducta a Seguir]. Prensa Med. Argent. 2016, 102, 471–476. [Google Scholar]
- Swaroop, M.; Straus, D.C.; Agubuzu, O.; Esposito, T.J.; Schermer, C.R.; Crandall, M.L. Pre-hospital transport times and survival for Hypotensive patients with penetrating thoracic trauma. J. Emergencies Trauma Shock. 2013, 6, 16–20. [Google Scholar] [CrossRef]
- Meizoso, J.P.; Ray, J.J.; Karcutskie, C.A.; Allen, C.J.; Zakrison, T.L.; Pust, G.D.; Koru-Sengul, T.; Ginzburg, E.; Pizano, L.R.; Schulman, C.I.; et al. Effect of Time to Operation on Mortality for Hypotensive Patients with Gunshot Wounds to the Torso: The Golden 10 Minutes. J. Trauma Acute Care Surg. 2016, 81, 685–691. [Google Scholar] [CrossRef]
- Gunay, C.; Cingoz, F.; Kuralay, E.; Demirkilic, U.; Tatar, H. Surgical Challenges for Urgent Approach in Penetrating Heart Injuries. Hear. Surg. Forum 2007, 10, E473–E477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina, E.J.; Gaughan, J.P.; Kulp, H.; McClurken, J.B.; Goldberg, A.J.; Seamon, M.J. Outcomes after emergency department thoracotomy for penetrating cardiac injuries: A new perspective. Interact. Cardiovasc. Thorac. Surg. 2008, 7, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.L.; Inaba, K.; Branco, B.C.; Oliver, M.; Bukur, M.; Salim, A.; Rhee, P.; Herrold, J.; Demetriades, D. Postdischarge Complications After Penetrating Cardiac Injury. Arch. Surg. 2011, 146, 1061–1066. [Google Scholar] [CrossRef] [Green Version]
- Kaljusto, M.-L.; Skaga, N.O.; Pillgram-Larsen, J.; Tønnessen, T. Survival predictor for penetrating cardiac injury; a 10-year consecutive cohort from a scandinavian trauma center. Scand. J. Trauma Resusc. Emerg. Med. 2015, 23, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, A.J.; Furlanetti, L.; Faidiga, G.B.; Scarpelini, S.; Evora, P.R.B.; Vicente, W. Penetrating cardiac injuries: A 13-year retrospective evaluation from a Brazilian trauma center. Interact. Cardiovasc. Thorac. Surg. 2005, 4, 212–215. [Google Scholar] [CrossRef] [Green Version]
- Thourani, V.H.; Feliciano, D.V.; Cooper, W.A.; Brady, K.M.; Adams, A.B.; Rozycki, G.S.; Symbas, P.N. Penetrating Cardiac Trauma at an Urban Trauma Center: A 22-Year Perspective. Am. Surg. 1999, 65, 811–818. [Google Scholar] [CrossRef]
- Shanmuganathan, K.; Matsumoto, J. Imaging of Penetrating Chest Trauma. Radiol. Clin. N. Am. 2006, 44, 225–238. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.; Quazi, M.A.; Reddy, K.; Thomson, S.R. Emergency operation for penetrating thoracic trauma in a metropolitan surgical service in South Africa. J. Thorac. Cardiovasc. Surg. 2011, 142, 563–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morse, B.C.; Mina, M.J.; Carr, J.S.; Jhunjhunwala, R.; Dente, C.J.; Zink, J.U.; Nicholas, J.M.; Wyrzykowski, A.D.; Salomone, J.P.; Vercruysse, G.A.; et al. Penetrating Cardiac Injuries: A 36-Year Perspective at an Urban, Level i Trauma Center. J. Trauma Acute Care Surg. 2016, 81, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Isaza-Restrepo, A.; Bolívar-Sáenz, D.J.; Tarazona-Lara, M.; Tovar, J.R. Penetrating cardiac trauma: Analysis of 240 cases from a hospital in Bogota, Colombia. World J. Emerg. Surg. 2017, 12, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Sessa, F.; Salerno, M.; Bertozzi, G.; Messina, G.; Ricci, P.; Ledda, C.; Rapisarda, V.; Cantatore, S.; Turillazzi, E.; Pomara, C. Touch DNA: Impact of handling time on touch deposit and evaluation of different recovery techniques: An experimental study. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Tozzo, P.; Giuliodori, A.; Rodriguez, D.; Caenazzo, L. Effect of Dactyloscopic Powders on DNA Profiling from Enhanced Fingerprints: Results from an Experimental Study. Am. J. Forensic Med. Pathol. 2014, 35, 68–72. [Google Scholar] [CrossRef]
- Tozzo, P.; Mazzobel, E.; Marcante, B.; Delicati, A.; Caenazzo, L. Touch DNA Sampling Methods: Efficacy Evaluation and Systematic Review. Int. J. Mol. Sci. 2022, 23, 15541. [Google Scholar] [CrossRef]
- Pereira, B.M.T.; Nogueira, V.B.; Calderan, T.R.A.; Villaça, M.P.; Petrucci, O.; Fraga, G.P. Penetrating cardiac trauma: 20-y experience from a university teaching hospital. J. Surg. Res. 2013, 183, 792–797. [Google Scholar] [CrossRef]
- Pomara, C.; Gianpaolo, D.P.; Monica, S.; Maglietta, F.; Sessa, F.; Guglielmi, G.; Turillazzi, E. “Lupara Bianca” a Way to Hide Cadavers after Mafia Homicides. A Cemetery of Italian Mafia. A Case Study. Leg. Med. 2015, 17, 192–197. [Google Scholar] [CrossRef]
- Sessa, F.; Maglietta, F.; Asmundo, A.; Pomara, C. Forensic Genetics and Genomic. In Forensic and Clinical Forensic Autopsy; Pomara, C., Fineschi, V., Eds.; CRC Press: Boca Raton, FL, USA, 2021; pp. 177–192. [Google Scholar]
- Salerno, M.; Cocimano, G.; Roccuzzo, S.; Russo, I.; Piombino-Mascali, D.; Márquez-Grant, N.; Zammit, C.; Esposito, M.; Sessa, F. New Trends in Immunohistochemical Methods to Estimate the Time since Death: A Review. Diagnostics 2022, 12. [Google Scholar] [CrossRef]
- Pennisi, G.; Torrisi, M.; Cocimano, G.; Esposito, M.; Salerno, M.; Sessa, F. Vitality markers in forensic investigations: A literature review. Forensic Sci. Med. Pathol. 2022; online ahead of print. [Google Scholar] [CrossRef]
- González-Hadad, A.; Ordoñez, C.A.; Parra, M.W.; Caicedo, Y.; Padilla, N.; Millán, M.; García, A.; Vidal-Carpio, J.M.; Pino, L.F.; Herrera, M.A.; et al. Damage Control in Penetrating Cardiac Trauma | El Control de Daños En El Trauma Cardíaco Penetrante. Colomb Med 2021, 52, e4034519. [Google Scholar] [CrossRef] [PubMed]
- Fais, P.; Giraudo, C.; Viero, A.; Amagliani, A.; Viel, G.; Montisci, M.; Miotto, D.; Cecchetto, G. Identification of Bullet Entrance in Different Type of Intermediate Firearm Wounds through Micro-Computed Tomography Analysis. J. Forensic Radiol. Imaging 2015, 3, 147–152. [Google Scholar] [CrossRef]
- Cecchetto, G.; Giraudo, C.; Amagliani, A.; Viel, G.; Fais, P.; Cavarzeran, F.; Feltrin, G.; Davide Ferrara, S.; Montisci, M. Estimation of the Firing Distance through Micro-CT Analysis of Gunshot Wounds. Int. J. Leg. Med. 2011, 125, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Giorgetti, A.; Giraudo, C.; Viero, A.; Bisceglia, M.; Lupi, A.; Fais, P.; Quaia, E.; Montisci, M.; Cecchetto, G.; Viel, G. Radiological Investigation of Gunshot Wounds: A Systematic Review of Published Evidence. Int. J. Leg. Med. 2019, 133, 1149–1158. [Google Scholar] [CrossRef] [PubMed]
- Agius, A.; Calleja, N.; Camenzuli, C.; Sultana, R.; Pullicino, R.; Zammit, C.; Calleja Agius, J.; Pomara, C. Perceptions of First-Year Medical Students towards Learning Anatomy Using Cadaveric Specimens through Peer Teaching. Anat. Sci. Educ. 2018, 11, 346–357. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors, Country, and Year | Sex/Age | Entrance Wound | Exit Wound | Heart Injuries | Hemodynamic Stability | Patient Evaluation | Additional Features/Toxicological Investigations | Survival |
|---|---|---|---|---|---|---|---|---|
| Ovali et al., Turkey (2021) [9] | Male (M), 46 years old (y.o.) | Gunshot with a bullet wound on his left cervical area (dimension: 1 cm × 1 cm) | No exit wound | Gunshot bullet lodged in the left ventricle (LV). | Stable hemodynamic condition. No cardiac tamponade | Ultrasonography; Computer tomography (CT); Transthoracic echocardiography (ECHO) | Not available (na)/na | Survivor |
| Tran et al., USA (2021) [10] | M, 34 y.o. | Gunshot wound to the left upper back, just below the left scapula | No exit wound | The bullet entered the posterior wall of the left atrium (LA). | No signs of shock, impending arrest, or cardiac tamponade | Chest X ray; CT scan; Abdominal ultrasound | The victim was discharged 10 days after admission/na. | Survivor |
| Lovasik et al., USA (2021) [11] | M, 15 y.o. | Single gunshot wound to right chest, just inferior to the mid-clavicle | No exit wound | Wound on the right atrial (RA) | Cardiac tamponade | Ultrasound of the heart; Chest X ray | The victim was discharged 14 days after admission/na. | Survivor |
| Romero-Velez et al., USA (2020) [12] | M, 30 y.o. | Multiple gunshot wounds. For heart injuries, the bullet had penetrated from the right gluteal fold and traversed the entire torso ending up lodged in the left scapula. | No exit wound | Two large injuries to the LV were reported. The bullet appeared to have entered the LV posteriorly and exited anteriorly. | Cardiac tamponade | Because from the severity of the wound, the victim was promptly operated. | The victim experienced a prolonged hospital recovery/na. | Survivor |
| Knowlin et al., USA (2018) [13] | M, 11 y.o. | Single gunshot wound close to the left posterior axillary line | Exit wound in the anterior chest just inferior and medial to the left nipple | The pericardium had a small hole from which blood came out under high pressure. Upon opening the pericardium to expose the injury adequately, a hole in the apex of the LV was identified. | Cardiac function was grossly normal | Focused abdominal sonogram from trauma (FAST); Chest X Ray | na/na | Survivor |
| Cvetkovic et al., Serbia (2018) [14] | M., 34 y.o. | Two gunshot entrance wounds in the left side of the chest | The bullets were found lodged under the skin of the back. | One bullet had passed through the left edge of the sternum, the pericardial sac, the anterior wall of the RV, the interventricular septum, the posterior wall of the LV, the rear aspect of the pericardial sac. The second bullet had passed through the fourth left costal cartilage, the pericardial sac, the upper anterior part of the interventricular septum, the anterior cusp of the mitral valve, the posterolateral wall of the left ventricle, and the pericardial sac. | Massive cardiac hemorrhage | Autopsy | Suicide/na | Deceased |
| Rupprecht and Gaab, Germany (2018) [15] | M., 49 y.o. | Single gunshot wound 2 cm below the left mammilla | 1 cm exit wound on the left-back | A 3 cm contusion lesion with a small bleeding perforation (3–4 mm) in the LV (dorsum of the ramus interventricularis anterior to the left coronary artery) was detected. | After the accident, there was a progressive instability of the victim’s vital signs, he was immediately transferred to surgery. | Sonography of the abdomen (FAST); CT scan | The bullet struck a rib, reducing its energy/na. | Survivor |
| Volpe et al., Brazil (2018) [16] | M, 34 y.o. | Two projectiles hit the subject in the thorax area, lateral side (subaxillary), at the height of the right hemithorax. | No exit wounds | One projectile was located inside the right ventricle (RV). | The critical condition started 16 days after the accident. | Chest X ray; CT scan; ECHO | The other projectile was located in the right rectus abdominis/na. | Survivor |
| Abou-Leila and Voronov, USA (2017) [17] | M., 17 y.o. | Single gunshot wound to the left costal margin | No exit wound | CT of the chest and abdomen showed retained foreign body in the interventricular septum. | Stable | Chest X ray; CT scan; ECHO | The victim was discharged on the 4th postoperative day/na. | Survivor |
| Santos et al., Brazil (2017) [18] | M, 26 y.o. | Single injury to the right hemithorax | No exit wound | CT showed an image suggestive of a projectile fragment in the intracardiac position, located in the membranous septum region, and close to the septal cusp of the tricuspid valve. | Stable | CT scan with and without contrast; ECHO | The victim was discharged on the 4th postoperative day/na. | Survivor |
| Fu et al., Taiwan (2017) [19] | M., 37 y.o. | One gunshot wound in the anterior chest wall | No exit wound | A penetrating hole identified in the RV wall; another penetrating hole was detected at the tricuspid septal leaflet, extending to the tricuspid annulus. | Stable | Chest X ray; CT scan; ECHO | Multiple lesions on heart (LV, LA, tricuspid leaflet)/na | Survivor |
| Imbert et al., France (2016) [20] | M, 59 y.o. | Penetrating gunshot wound to the left side of the chest caused by a rifle bullet a. An entrance wound was noted on the left side of the chest, parasternal, next to the fifth intercostal space. | No exit wound | Gunshot wound of the heart with migration of the projectile to the pulmonary artery are rare. | Non-Stable | Chest X ray; CT scan | He was admitted immediately after the accident. He was discharged 22 days after the first surgery/na. | Survivor |
| Sapkota and Koirala, Nepal (2016) [21] | M, 32 y.o. | The entry wound pierced the sternum laterally at the third intercostal level. | No exit wound. | The first cardiac perforation was seen near the RV outflow tract. The second perforation was at the inferior wall of the LV, 3 cm off the apex. | Stable | Chest X ray; CT scan; ECHO | He was admitted 9 h post shot. He was discharged 14 days after surgery/na. | Survivor |
| Kaya et al., Turkey (2016) [22] | M., 32 y.o. | A superficial wound on the left shoulder and another on the left side of the thorax at the 6th intercostal space | No exit wounds | A bullet in the pericardial sac with pericardial effusion compressing the heart was found. | Stable (discharged after 7 days) | CT scan; | The gunshot wound was noticed 1 day later/na. | Survivor |
| Konecny et al., Czech Republic (2016) [23] | Female (F), 39 y.o. | A gunshot wound in the lower third of the sternum | No exit wound | The projectile trajectory fractured the lower third of the chest bone, punctured the anterior walls of the RV and RA, and perforated the inferior vena cava. | Stable (discharged after 6 days). The projectile was found at the level of the right 9th rib paravertebrally. | CT scan | Attempted suicide, psychiatric treatment for two weeks/na. | Survivor |
| Obrador et al., Spain (2015) [24] | M, 43 y.o. | A wound below the left clavicle | No exit wound | Perforation of the RV and the RA. | Stable | Chest X ray | He was discharged on the 12th postoperative day/na. | Survivor |
| Siddiqui et al., Pakistan (2015) [25] | M., 48 y.o. | An entry wound medial to the left nipple, close to the midline on the left side | No exit wound | CT scan found hemopericardium and metallic bullet posterior to the heart. | Stable | CT scan | na/na | Survivor |
| M., 35 y.o. | A gunshot injury to his anterior chest | No exit wound | RV bullet wound anteriorly, and a LV wound posteriorly. | Cardiopulmonary bypass (CPB) was established. Both ventricular wounds and VSD repaired. | CT scan | na/na | Survivor | |
| Suzuki et al., Japan (2014) [26] | M., 47 y.o. | Single gunshot wound on the left anterior chest wall | 15 mm wound on the left posterior wall | The bullet damaged the pericardium and the heart from the apex to a portion of the left ventricular lateral wall. | Unstable | CT scan | Suicide attempt. The patient was discharged on the 18th postoperative day/na. | Survivor |
| Rasool et al., Pakistan (2014) [27] | M., 10 y.o. | A single gunshot entry wound in the region of the sternum at the level of the 5th intercostal space, with history of stray bullet injury | No exit wound | The cardiac damage resulting from the projectile observed in the anterior wall (entrance hole) and the inferior wall (exit hole) of the RV. | The patient was hemodynamically stable. Different organs were damaged (liver, stomach). | Chest X ray; CT scan | He was discharged on the 9th postoperative day/na. | Survivor |
| Mills et al., USA (2014) [28] | M., 20 y.o. | Intrathoracic gunshot | No exit wound | There was an entry wound to the left posterior ventricle approximately 1 cm from the atrioventricular groove. The left atrium opened, and the bullet was identified buried beneath the endocardium of the back left atrial wall. | Hemodynamically stable | Chest X ray; CT scan; ECHO | Medical history significant for schizophrenia. He was discharged after 3 weeks, but he was treated for other problems/na. | Survivor |
| Bonsignore et al., Italy (2013) [29] | M., 75 y.o. | One wound in the left chest in the second infracostal space | No exit wound | The bullet passed through the pericardium, left auricle, puncturing the anterior wall of the left coronary artery. | Hemopericardium | Autopsy | Suicide. After a thoracic wound, he shot another bullet to his head/na. | Deceased |
| Porcu et al., France (2012) [30] | M., 82 y.o. | One wound in the sub-mammary region, in the left 7th intercostal space | No exit wound | RV injury | Unstable | Chest X ray | He arrived at the emergency department 3 h after attempting suicide/na. | Subject died after 5 days from a multiorgan failure due to a prolonged preoperative low cardiac output. |
| Branch and Adams, USA (2012) [31] | F., 40 y.o. | A single entrance to the upper-left chest | No exit wound | The LV was lacerated secondary to blast forces, with resultant hemopericardium and subsequent cardiac tamponade. | Unstable | FAST | Suicide/na | Deceased |
| Karigyo et al., Brazil (2011) [32] | M, 40 y.o. | Left hemithorax | No exit wound | The cardiac injuries were observed in the anterior wall of the LV (inlet hole), and in the posterior region of the RV (outlet hole). | Stable | Chest X ray; CT scan | Victim of an attempted robbery; he was discharged 26 days after the operation/na. | Survivor |
| Ustin et al., USA (2011) [33] | F., 39 y.o.(pregnant) | A single gunshot wound to the right chest over the third intercostal space (approximately 5 cm right of the sternum) | No exit wound. | The bullet had fractured the sternum and entered the pericardial sac lacerating the myocardium just inferior to the atrioventricular groove. | Unstable | Chest X ray | Attempted suicide in a patient with a past medical history of substance abuse, hepatitis C, and gestational diabetes; Discharged on post-trauma day 17/toxicology screen was positive for cocaine and opioids. | Survivor; the baby was delivered at term |
| Hartert et al., Germany (2010) [34] | M, 57 y.o. | A single entrance wound in the left mid-paramanubrial area. | No exit wound | The bullet penetrated the anterior wall of the RV causing a pericardial tamponade. The exit hole was located in the posterior area of the RV. | Unstable | Chest X ray | Attempted suicide. The subject was discharged on the 28th postoperative day/na. | |
| Ellertson and Johnson, USA (2008) [35] | F., 48 y.o. | One gunshot wound entered the left anterior chest wall and appeared to cross the midline inferiorly to rest near the dome of her liver. | No exit wound | The inspection of the heart showed a relatively large (approximately 3 cm long) tangential injury to the RA near the right atrioventricular groove adjacent to the right coronary artery. | Unstable | Chest X ray; CT scan | Two months later, psychiatric issues related to the incident were recorded/na. | Survivor |
| De Giorgio and Raino, Italy (2007) [36] | M., 45 y.o. | 4 penetrating gunshot wounds and one tangential wound. 2 of the penetrating injuries in the chest: the upper bullet had entered the thoracic cavity between ribs III and IV, 3 cm to the right of the edge of the sternum, and the lower bullet entered between ribs IV and V, close to the sternum. | Only one oval exit wound on the posterior wall of the thorax between ribs VII and VIII, 3 cm to the right of the vertebral column. | Both bullets had made entrance wounds on the pericardial sac and the anterior wall of the RA. In the upper posterior atrial wall as well as in the posterior wall of the pericardium, only one wound was visible. | Died at the scene immediately after being shot. | Autopsy | Shotgun homicide/Alcohol use was considered a factor contributing to the death. | Deceased |
| Incorvaia et al., USA (2007) [37] | M., 47 y.o. | There was a bullet hole in his chest on the left side above the nipple line, in the fifth intercostal space, 2 cm to the left of the sternal edge. | No exit wound | Two holes were exposed in the right ventricle. | Unstable | FAST; | He was struck in the chest by a bullet that fell from the sky. Discharged 30 days postoperatively/na. | Survivor |
| Faschingbauer et al., Germany (2006) [38] | M., 43 y.o. | An entry wound was observed on the ventral chest just a few centimeters left to the midline at about the fourth rib. | No exit wound | 2 cm diameter rough-edged defect in the RA was found. The exit wound at the dorsal border of the superior vena cava to RA. | Unstable | Chest X ray; | Homicide attempt. After that, he was able to run 19 m before collapsing. The victim was discharged about 14 days later/na. | Survivor |
| Meira et al., Brazil (2005) [39] | M., 29 y.o. | The bullet passed through right arm and penetrated the thorax. | No exit wound | The bullet was lodged in the RV anterior wall. | Stable | Chest X ray | After the 11th day, he had a thoracotomy exploration with subsequent surgery/na. | Survivor |
| Bali et al., India (2003) [40] | M, 30 y.o. | Right upper anterior chest wall | No exit wound | Perforation of the RV outflow tract. | Stable | Chest X ray | Multiple bullet injuries in the chest and face after being shot. The victim was discharged after 2 days/na. | Survivor |
| Habdank and Nolan, Canada (2003) [41] | M, 33 y.o. | A single gunshot wound that initially penetrated his left arm and then entered the posterolateral mid left thorax. | No exit wound | Perforation of free wall of the LV. | Stable | Chest X ray; ECHO | The patient was discharged after 7 days/na. | Survivor |
| Kurt et al., Turkey (2001) [42] | M., 46 y.o. | Entry wound in the right chest at the second intercostal space on the midaxillary line. | No exit wound | Entrance wound in the LA. | Unstable | Chest X ray | The victim died 3 days after the operation for the cerebrovascular event/na. | Deceased |
| Doty et al., USA (1999) [43] | F., 27 y.o. | Single gunshot wound to the lateral left side of the chest (left fifth intercostal space). | No exit wound | Two cardiac perforations were noted, one in the LA and one in the LV. | Unstable | Chest X ray | Several complications after surgery/na. | Survivor |
| Kwan et al., USA (1995) [44] | M, 19 y. | Single gunshot wound to the chest | No exit wound | The bullet entered the RV and exited through the LV. | Stable | Chest X ray; ECHO | Dyspnea after surgery/na. | Survivor |
| Wait et al., USA (1994) [45] | M., 26 y. | Two close-range pistol gunshot wounds to the left chest | No exit wound | One bullet remained in the left upper lung field and was associated with massive hemothorax; another one transversed the mediastinum, entering the obtuse margin of the heart, and proceeding into the right upper quadrant of the abdomen. | Cardiopulmonary resuscitation | Chest X ray; CT scan | Several complications/na. | Survivor |
| Skipper and Debski, USA (1990) [46] | F., 21 y. | Shotgun blast to left chest and arm. | No exit wound | The pellet holes that were no longer bleeding were found in the myocardium of the LV. | Stable | Chest X ray; Arteriogram | Several complications/na. | Survivor |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sessa, F.; Cocimano, G.; Esposito, M.; Zuccarello, P.; Scoto, E.; Mazzeo, P.; Salerno, M. Systematic Review of Penetrating Cardiac Injury by a Firearm: Forensic Implications. Healthcare 2023, 11, 265. https://doi.org/10.3390/healthcare11020265
Sessa F, Cocimano G, Esposito M, Zuccarello P, Scoto E, Mazzeo P, Salerno M. Systematic Review of Penetrating Cardiac Injury by a Firearm: Forensic Implications. Healthcare. 2023; 11(2):265. https://doi.org/10.3390/healthcare11020265
Chicago/Turabian StyleSessa, Francesco, Giuseppe Cocimano, Massimiliano Esposito, Pietro Zuccarello, Edmondo Scoto, Pietro Mazzeo, and Monica Salerno. 2023. "Systematic Review of Penetrating Cardiac Injury by a Firearm: Forensic Implications" Healthcare 11, no. 2: 265. https://doi.org/10.3390/healthcare11020265