

The Evaluation of Clinical Signs and Symptoms of Malignant Tumors Involving the Maxillary Sinus: Recommendation of an Examination Sieve and Risk Alarm Score

 , ,
, ,  , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Sample Size
2.2. Ethical Consideration and Participants Recruitment
2.3. Data Collection
2.4. Statistical Analysis
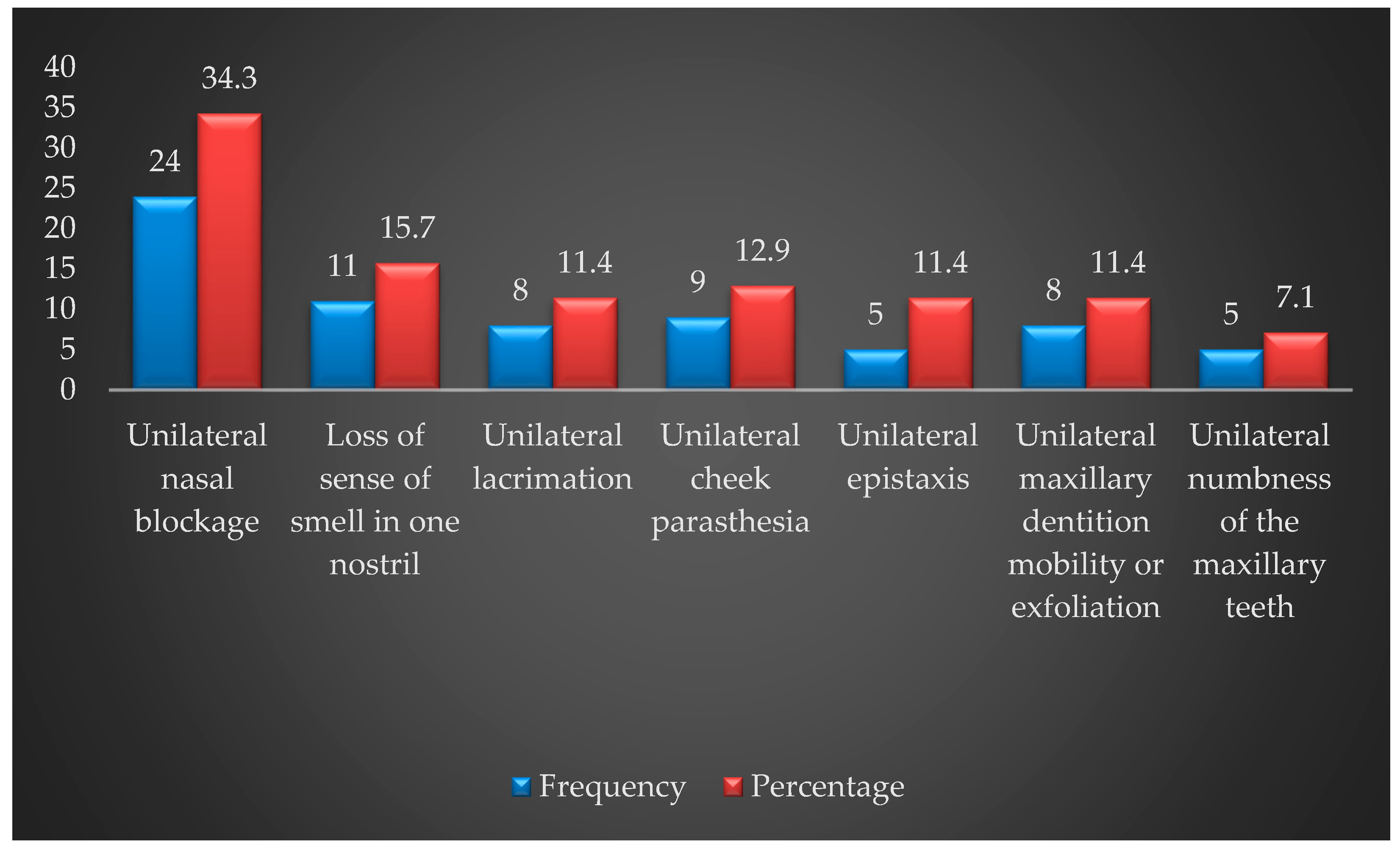
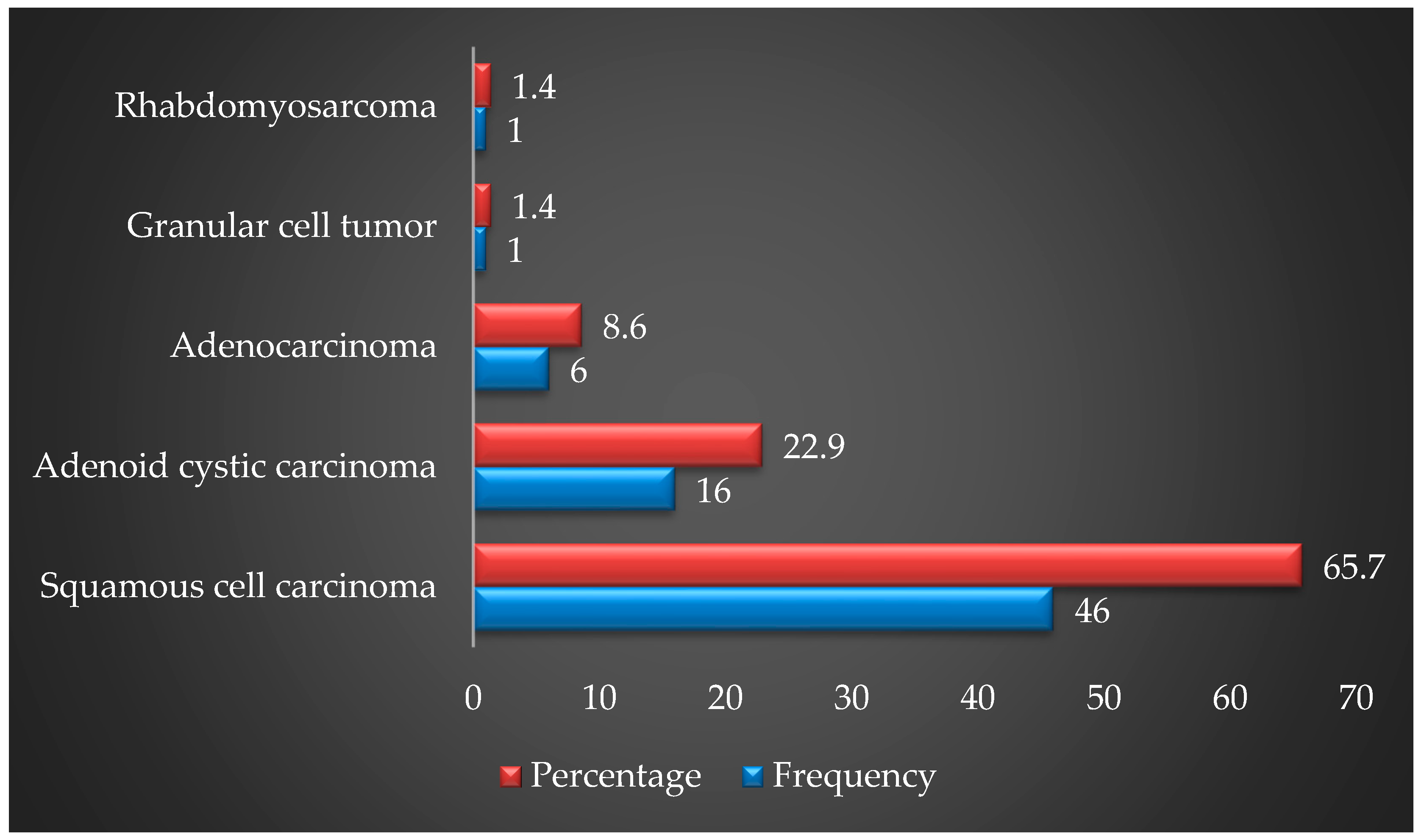
3. Results
4. Discussion
5. Limitation
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Item No | Recommendation | ||
|---|---|---|---|
| Title and abstract | 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract | √ |
| (b) Provide in the abstract an informative and balanced summary of what was done and what was found | √ | ||
| Introduction | |||
| Background/rationale | 2 | Explain the scientific background and rationale for the investigation being reported | √ |
| Objectives | 3 | State specific objectives, including any prespecified hypotheses | √ |
| Methods | |||
| Study design | 4 | Present key elements of study design early in the paper | √ |
| Setting | 5 | Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection | √ |
| Participants | 6 | (a) Give the eligibility criteria, and the sources and methods of selection of participants | √ |
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable | √ |
| Data sources/measurement | 8 | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group | √ |
| Bias | 9 | Describe any efforts to address potential sources of bias | ---------- |
| Study size | 10 | Explain how the study size was arrived at | √ |
| Quantitative variables | 11 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why | √ |
| Statistical methods | 12 | (a) Describe all statistical methods, including those used to control for confounding | √ |
| (b) Describe any methods used to examine subgroups and interactions | ---------- | ||
| (c) Explain how missing data were addressed | ---------- | ||
| (d) If applicable, describe analytical methods taking account of sampling strategy | √ | ||
| (e) Describe any sensitivity analyses | √ | ||
| Results | |||
| Participants | 13 | (a) Report numbers of individuals at each stage of study—e.g., numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed | √ |
| (b) Give reasons for non-participation at each stage | ---------- | ||
| (c) Consider use of a flow diagram | ---------- | ||
| Descriptive data | 14 | (a) Give characteristics of study participants (e.g., demographic, clinical, social) and information on exposures and potential confounders | √ |
| (b) Indicate number of participants with missing data for each variable of interest | ---------- | ||
| Outcome data | 15 | Report numbers of outcome events or summary measures | √ |
| Main results | 16 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (e.g., 95% confidence interval). Make clear which confounders were adjusted for and why they were included | √ |
| (b) Report category boundaries when continuous variables were categorized | √ | ||
| (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period | ---------- | ||
| Other analyses | 17 | Report other analyses done—e.g., analyses of subgroups and interactions, and sensitivity analyses | √ |
| Discussion | |||
| Key results | 18 | Summarise key results with reference to study objectives | √ |
| Limitations | 19 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias | √ |
| Interpretation | 20 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence | √ |
| Generalisability | 21 | Discuss the generalisability (external validity) of the study results | √ |
| Other information | |||
| Funding | 22 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based | √ |
References
- Waldrona, J.N.; O’Sullivana, B.; Gullaneb, P.; Witterick, I.J.; Liua, F.F.; Paynea, D.; Wardea, P.; Cummings, B. Carcinoma of the maxillary antrum: A retrospective analysis of 110 cases. Radiother. Oncol. 2000, 57, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Bobinskas, A.M.; Wiesenfeld, D.; Chandu, A. Influence of the site of origin on the outcome of squamous cell carcinoma of the maxilla—Oral versus sinus. Int. J. Oral Maxillofac. Surg. 2014, 43, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Carrillo, J.F.; Guemes, A.; Ramirez-Ortega, M.C.; Onate-Ocana, L.F. Prognostic factors in maxillary sinus and nasal cavity carcinoma. Eur. J. Surg. Oncol. 2005, 31, 1206–1212. [Google Scholar] [CrossRef]
- Zolfaghar, M.; Amoozegar, M.A.; Khajeh, K.; Babavalian, H.; Tebyanian, H. Isolation and screening of extracellular anticancer enzymes from halophilic and halotolerant bacteria from different saline environments in Iran. Mol. Biol. Rep. 2019, 46, 3275–3286. [Google Scholar] [CrossRef]
- Stavrianos, I.; Camellieri, I.; Mclean, N.; Piggot, T.; Kelly, C.; Soames, J.V. Malignant Tuomrs of the Maxillary Sinus: An 18 Year Review. Br. J. Plast. Surg. 1998, 51, 584–588. [Google Scholar] [CrossRef]
- Lee, D.J.; Lee, M.J.; Kwon, K.H.; Chung, E.J.; Yoon, D.Y.; Rho, Y.S. Discrepancy between preoperative MRI evaluation and intraoperative or postoperative pathological findings for the extent of local invasion in maxillary squamous cell carcinoma. Int. J. Oral Maxillofac. Surg. 2014, 43, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Jégoux, F.; Métreau, A.; Louvel, G.; Bedfert, C. Paranasal sinus cancer. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2013, 130, 327–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Natalia, M.R.; Barona, D.C.; Cortés, B.J.; Martín, A.M.; Sanz, A.J.; Martínez, J.M. Dental considerations in diagnosis of maxillary sinus carcinoma: A patient series of 24 cases. J. Am. Dent. Assoc. 2018, 149, 976–982. [Google Scholar] [CrossRef]
- Wang, Y.; Yang, R.; Zhao, M.; Guo, W.; Zhang, L.; Zhang, W.; Wang, X. Retrospective analysis of 98 cases of maxillary sinus squamous cell carcinoma and therapeutic exploration. World J. Surg. Oncol. 2020, 18, 90. [Google Scholar] [CrossRef]
- Zheng, W.; McLaughlin, J.K.; Chow, W.; Chien, H.T.C.; Blot, W.J. Risk Factors for Cancers of the Nasal Cavity and Paranasal Sinuses among White Men in the United States. Am. J. Epidemiol. 1993, 138, 965–972. [Google Scholar] [CrossRef]
- WHO. WHO Report on the Global Tobacco Epidemic, 2019; World Health Organization: Geneva, Switzerland, 2019. Available online: https://www.who.int/tobacco/global_report/en// (accessed on 12 December 2022).
- International Agency for Research on Cancer (IARC). IARC Monographs on the Evaluation of Carcinogenic Risks to Humans: Wood Dust and Formaldehyde; IARC: Lyon, France; World Health Organization: Lyon, France, 1995; Volume 62.
- Fullerton, D.G.; Bruce, N.; Gordon, S.B. Indoor air pollution from biomass fuel smoke is a major health concern in the developing world. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 843–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, Y.X.; Cha, Q.; Chen, X.W.; Chen, Y.Z.; Huang, L.F.; Feng, Z.Z.; Wu, X.F.; Wu, J.M. An epidemiological study of risk factors for lung cancer in Guangzhou, China. Lung Cancer 1996, 14 (Suppl. 1), S9–S37. [Google Scholar] [CrossRef] [PubMed]
- Colbeck, I.; Nasir, Z.A.; Ali, Z. The state of indoor air quality in Pakistan—A review. Environ. Sci. Pollut. Res. 2010, 17, 1187–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammond, S.; Ellen, G.; Robin, F. Respiratory health effect related to occupational Spray painting and welding. J. Occup. Environ. Med. 2005, 47, 728–739. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.; Malik, R.N. Hematological evidence of occupational exposure to chemicals and other factors among auto-repair workers in Rawalpindi, Pakistan. Osong. Public Health Res. Perspect. 2012, 3, 229–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awodele, O.; Popoola, T.D.; Ogbudu, B.S.; Akinyede, A.; Coker, H.A.; Akintonwa, A. Occupational hazards and safety measures amongst the paint factory workers in lagos, Nigeria. Saf. Health Work. 2014, 5, 106–111. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.H.; Kim, S.Y.; Son, M.K.; Yang, H.S.; Lee, S.W.; Kim, J.I.; Jung, K.Y. Malignant fibrous histiocytoma of the maxillary sinus in a spray painter from an automobile repair shop. Ann. Occup. Environ. Med. 2013, 25, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreppel, M.; Safi, A.F.; Scheer, M.; Nickenig, H.J.; Zöller, J.; Preuss, S.; Meyer, M.; Rothamel, D.; Dreiseidler, T. The importance of early diagnosis in patients with maxillary sinus carcinoma. Eur. Arch. Otorhinolaryngol. 2016, 273, 2629–2635. [Google Scholar] [CrossRef]
- Mosaddad, S.A.; Beigi, K.; Doroodizadeh, T.; Haghnegahdar, M.; Golfeshan, F.; Ranjbar, R.; Tebyanian, H. Therapeutic applications of herbal/synthetic/bio-drug in oral cancer: An update. Eur. J. Pharmacol. 2021, 890, 173657. [Google Scholar] [CrossRef]
- Hajmohammadi, E.; Molaei, T.; Mowlaei, S.H.; Alam, M.; Abbasi, K.; Khayatan, D.; Rahbar, M.; Tebyanian, H. Sonodynamic therapy and common head and neck cancers: In vitro and in vivo studies. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5113–5121. [Google Scholar]
- Hajmohammadi, E.; Ghahremanie, S.; Alam, M.; Abbasi, K.; Mohamadian, F.; Khayatan, D. Biomarkers and common oral cancers: Clinical trial studies. JBUON 2021, 26, 2227–2237. [Google Scholar]
- Andrade, M.F.; De Faria, P.R.; Cardoso, S.V.; Santos, M.R.M.; Dias, F.L.; Eisenberg, A.L.A.; Santos, I.C.; Loyola, A.M. Adenoid cystic carcinoma of the maxillary sinus: A clinical–pathological report of 10 years of experience from a single institution. Int. J. Oral Maxillofac. Surg. 2014, 43, 1313–1318. [Google Scholar] [CrossRef]
- Hussain, A.; Tebyaniyan, H.; Khayatan, D. The Role of Epigenetic in Dental and Oral Regenerative Medicine by Different Types of Dental Stem Cells: A Comprehensive Overview. Stem Cells Int. 2022, 2022, 5304860. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, R.; Hardillo, J.A.; Mehta, D.; Slotman, B.; Tobi, H.; Croonenburg, E.; van der Waal, I.; Snow, G.B. Squamous cell carcinoma of maxillary sinus. Head Neck 2000, 22, 164–169. [Google Scholar]
- Qureshi, S.S.; Chaukar, D.A.; Talole, S.D.; Dcruz, A.K. Clinical Characteristics and Outcome of Non-Squamous Cell Malignancies of the Maxillary Sinus. J. Surg. Oncol. 2006, 93, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Slinger, C.A.; McGarry, G.W. Nose and sinus tumours: Red flags and referral. Br. J. Gen. Pract. 2018, 68, 247–248. [Google Scholar] [CrossRef] [Green Version]
- Rashid, H.; Bashir, A. Surgical and prosthetic management of maxillary odontogenic myxoma. Eur. J. Dent. 2015, 9, 277–283. [Google Scholar] [CrossRef] [Green Version]
- Praveena, N.; Maragathavalli, G. Carcinoma of the Maxillary Antrum: A Case Report. Cureus 2018, 10, e2614. [Google Scholar] [CrossRef] [Green Version]
- Tahmasebi, E.; Alikhani, M.; Yazdanian, A.; Yazdanian, M.; Tebyanian, H.; Seifalian, A. The current markers of cancer stem cell in oral cancers. Life Sci. 2020, 249, 117483. [Google Scholar] [CrossRef]
- Rezaeeyan, Z.; Safarpour, A.; Amoozegar, M.A.; Babavalian, H.; Tebyanian, H.; Shakeri, F. High carotenoid production by a halotolerant bacterium, Kocuria sp. strain QWT-12 and anticancer activity of its carotenoid. EXCLI J. 2017, 16, 840–851. [Google Scholar]
- Kafshgari, H.S.; Yazdanian, M.; Ranjbar, R.; Tahmasebi, E.; Mirsaeed, S.; Tebyanian, H.; Ebrahimzadeh, M.; Goli, H. The effect of Citrullus colocynthis extracts on Streptococcus mutans, Candida albicans, normal gingival fibroblast and breast cancer cells. J. Biol. Res. 2019, 92, 8201. [Google Scholar] [CrossRef]


| Sign and Symptoms | Gender | N | Total N (%) | p-Value |
|---|---|---|---|---|
| Exophthalmos | Male | 20 | 35 (50.0) | 0.571 |
| Female | 15 | |||
| Loss of sense of smell | Male | 18 | 37 (52.9) | 0.391 |
| Female | 19 | |||
| Oroantral fistula | Male | 20 | 39 (55.7) | 0.683 |
| Female | 19 | |||
| Palpable mass in the upper buccal sulcus | Male | 30 | 66 (94.3) | 0.287 |
| Female | 36 | |||
| Palpable lymph nodes in the neck | Male | 14 | 25 (35.7) | 0.189 |
| Female | 11 | |||
| Obstruction of the nose | Male | 39 | 67 (95.7) | 0.941 |
| Female | 28 | |||
| Bleeding from the nose | Male | 30 | 56 (80.0) | 0.582 |
| Female | 26 | |||
| Asymmetry of the face | Male | 39 | 69 (98.6) | 0.382 |
| Female | 30 | |||
| Swelling of the cheek | Male | 41 | 69 (98.6) | 0.918 |
| Female | 28 | |||
| Double vision | Male | 14 | 24 (34.3) | 0.118 |
| Female | 10 | |||
| Numbness of the cheek and infraorbital skin | Male | 23 | 41 (58.6) | 0.372 |
| Female | 18 |
| History of Hazard Exposure | Final Diagnosis of Pathology | Total (N) | ||||
|---|---|---|---|---|---|---|
| SCC (N) | ACC (N) | AC (N) | GCT (N) | RMS (N) | ||
| Wood dust | 13 | 9 | 3 | 0 | 1 | 26 |
| Tobacco smoke exposure (first or secondhand) | 22 | 5 | 0 | 0 | 0 | 27 |
| Wood and/or cow dung smoke | 5 | 0 | 2 | 1 | 0 | 8 |
| Coal dust | 3 | 2 | 1 | 0 | 0 | 6 |
| Spray paint/chromium | 3 | 0 | 0 | 0 | 0 | 3 |
| Chi-square | 1.412 | 3.035 | 2.717 | 2.4764 | 1.763 | - |
| df | 1 | 4 | 3 | 2 | 6 | - |
| Standard error | 0.365 | 0.231 | 0.268 | 0.274 | 0.194 | - |
| Spearman correlation | 0.064 | 0.078 | 0.015 | 0.048 | 0.018 | - |
| p-value | * 0.001 | * 0.021 | 0.725 | 0.427 | 0.825 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bashir, A.; Khan, Z.A.; Maqsood, A.; Prabhu, N.; Saleem, M.M.; Alzarea, B.K.; Issrani, R.; Khan, S.R.; Ahmed, N.; Abbasi, M.S.; et al. The Evaluation of Clinical Signs and Symptoms of Malignant Tumors Involving the Maxillary Sinus: Recommendation of an Examination Sieve and Risk Alarm Score. Healthcare 2023, 11, 194. https://doi.org/10.3390/healthcare11020194
Bashir A, Khan ZA, Maqsood A, Prabhu N, Saleem MM, Alzarea BK, Issrani R, Khan SR, Ahmed N, Abbasi MS, et al. The Evaluation of Clinical Signs and Symptoms of Malignant Tumors Involving the Maxillary Sinus: Recommendation of an Examination Sieve and Risk Alarm Score. Healthcare. 2023; 11(2):194. https://doi.org/10.3390/healthcare11020194
Chicago/Turabian StyleBashir, Atif, Zafar Ali Khan, Afsheen Maqsood, Namdeo Prabhu, Muhammad Mudassar Saleem, Bader K. Alzarea, Rakhi Issrani, Shammas Raza Khan, Naseer Ahmed, Maria Shakoor Abbasi, and et al. 2023. "The Evaluation of Clinical Signs and Symptoms of Malignant Tumors Involving the Maxillary Sinus: Recommendation of an Examination Sieve and Risk Alarm Score" Healthcare 11, no. 2: 194. https://doi.org/10.3390/healthcare11020194