
Measurement Properties’ Evaluation of the Arabic Version of the Patient-Specific Functional Scale in Patients with Multiple Sclerosis
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Settings and Participants
2.3. Outcome Measures
2.3.1. The Patient-Specific Functional Scale (PSFS)
2.3.2. RAND 36-Item Health Survey (RAND-36)
2.3.3. Global Rating of Change (GRC)
2.4. Procedure
3. Statistical Analysis
3.1. Test–Retest Reliability
3.2. Measurement Error
3.3. Floor and Ceiling Effects
3.4. Construct Validity
3.5. Sample Size Estimation
4. Results
4.1. Test–Retest Reliability
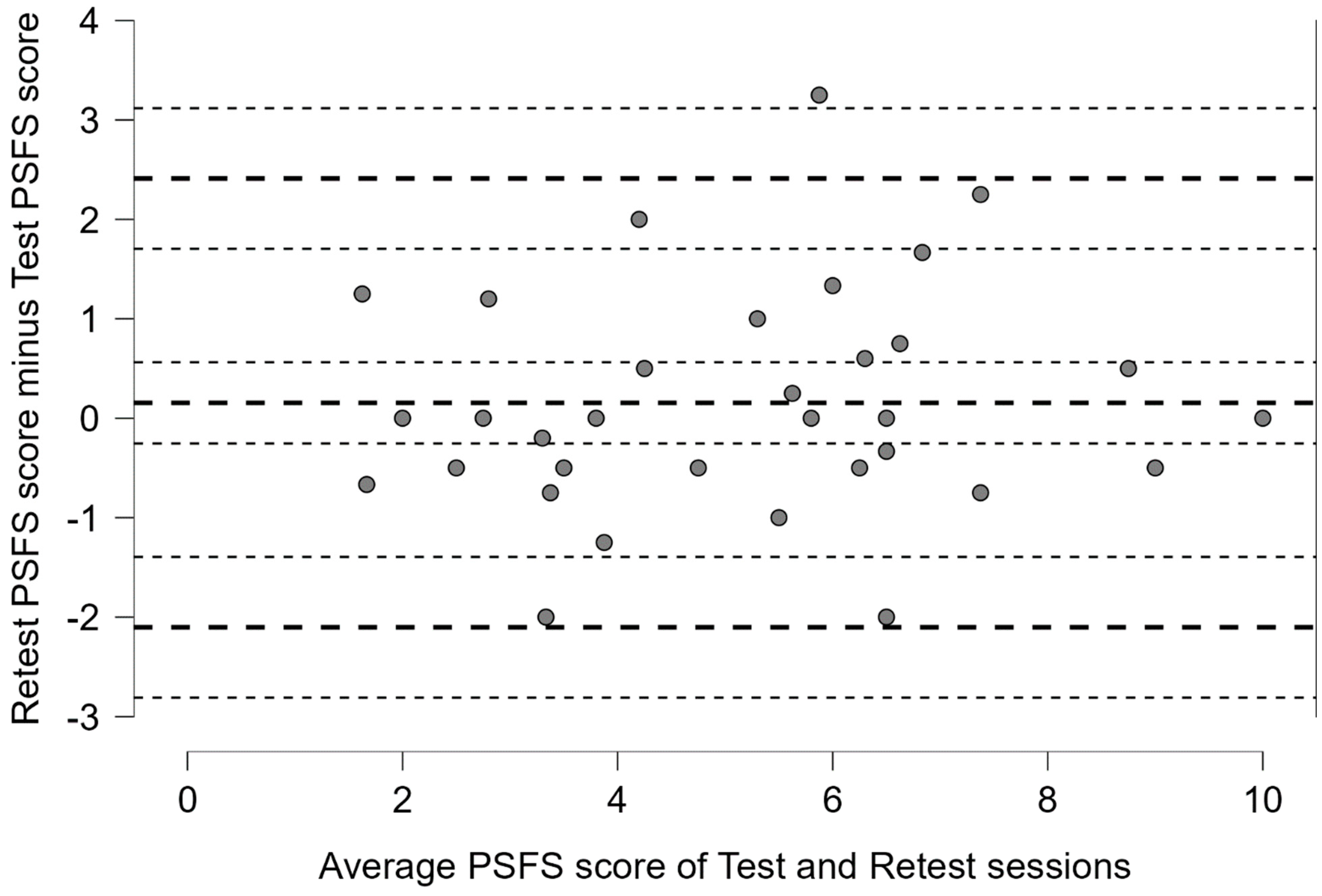
4.2. Measurement Error
4.3. Construct Validity
4.4. Floor and Ceiling Effects
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baum, H.M.; Rothschild, B.B. Multiple sclerosis and mobility restriction. Arch. Phys. Med. Rehabil. 1983, 64, 591–596. [Google Scholar]
- Myhr, K.M.; Riise, T.; Vedeler, C.; Nortvedt, M.W.; Grønning, R.; Midgard, R.; Nyland, H.I. Disability and prognosis in multiple sclerosis: Demographic and clinical variables important for the ability to walk and awarding of disability pension. Mult. Scler. 2001, 7, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; La Rocca, N.; Uitdehaag, B.; van der Mei, I.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult. Scler. 2020, 26, 1816–1821. [Google Scholar] [CrossRef] [PubMed]
- Kalb, R.; Brown, T.R.; Coote, S.; Costello, K.; Dalgas, U.; Garmon, E.; Giesser, B.; Halper, J.; Karpatkin, H.; Keller, J.; et al. Exercise and lifestyle physical activity recommendations for people with multiple sclerosis throughout the disease course. Mult. Scler. 2020, 26, 1459–1469. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, E.R.; Ashbaugh, A.D.; Hockenberry, B.J.; McGrew, C.A. Multiple Sclerosis and Exercise: A Literature Review. Curr. Sport. Med. Rep. 2018, 17, 31–35. [Google Scholar] [CrossRef]
- Latimer-Cheung, A.E.; Pilutti, L.A.; Hicks, A.L.; Martin Ginis, K.A.; Fenuta, A.M.; MacKibbon, K.A.; Motl, R.W. Effects of exercise training on fitness, mobility, fatigue, and health-related quality of life among adults with multiple sclerosis: A systematic review to inform guideline development. Arch. Phys. Med. Rehabil. 2013, 94, 1800–1828.e3. [Google Scholar] [CrossRef] [PubMed]
- Papuć, E.; Stelmasiak, Z. Factors predicting quality of life in a group of Polish subjects with multiple sclerosis: Accounting for functional state, socio-demographic and clinical factors. Clin. Neurol. Neurosurg. 2012, 114, 341–346. [Google Scholar] [CrossRef]
- Hermann, B.P.; Vickrey, B.; Hays, R.D.; Cramer, J.; Devinsky, O.; Meador, K.; Perrine, K.; Myers, L.W.; Ellison, G.W. A comparison of health-related quality of life in patients with epilepsy, diabetes and multiple sclerosis. Epilepsy Res. 1996, 25, 113–118. [Google Scholar] [CrossRef]
- Braley, T.J.; Chervin, R.D. Fatigue in multiple sclerosis: Mechanisms, evaluation, and treatment. Sleep 2010, 33, 1061–1067. [Google Scholar] [CrossRef]
- Krupp, L. Fatigue is intrinsic to multiple sclerosis (MS) and is the most commonly reported symptom of the disease. Mult. Scler. 2006, 12, 367–368. [Google Scholar] [CrossRef]
- Lerdal, A.; Celius, E.G.; Krupp, L.; Dahl, A.A. A prospective study of patterns of fatigue in multiple sclerosis. Eur. J. Neurol. 2007, 14, 1338–1343. [Google Scholar] [CrossRef] [PubMed]
- Janardhan, V.; Bakshi, R. Quality of life in patients with multiple sclerosis: The impact of fatigue and depression. J. Neurol. Sci. 2002, 205, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.M.; Arnett, P.A. Factors related to employment status changes in individuals with multiple sclerosis. Mult. Scler. 2005, 11, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Zwibel, H.L.; Smrtka, J. Improving quality of life in multiple sclerosis: An unmet need. Am. J. Manag. Care 2011, 17 (Suppl. S5), S139–S145. [Google Scholar] [PubMed]
- Compston, A.; Coles, A. Multiple sclerosis. Lancet 2008, 372, 1502–1517. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Pallant, J.F. Use of International Classification of Functioning, Disability and Health (ICF) to describe patient-reported disability in multiple sclerosis and identification of relevant environmental factors. J. Rehabil. Med. 2007, 39, 63–70. [Google Scholar] [CrossRef]
- Coenen, M.; Cieza, A.; Freeman, J.; Khan, F.; Miller, D.; Weise, A.; Kesselring, J. The development of ICF Core Sets for multiple sclerosis: Results of the International Consensus Conference. J. Neurol. 2011, 258, 1477–1488. [Google Scholar] [CrossRef]
- Conrad, A.; Coenen, M.; Schmalz, H.; Kesselring, J.; Cieza, A. Validation of the comprehensive ICF core set for multiple sclerosis from the perspective of occupational therapists. Scand. J. Occup. Ther. 2012, 19, 468–487. [Google Scholar] [CrossRef]
- Conrad, A.; Coenen, M.; Schmalz, H.; Kesselring, J.; Cieza, A. Validation of the comprehensive ICF core set for multiple sclerosis from the perspective of physical therapists. Phys. Ther. 2012, 92, 799–820. [Google Scholar] [CrossRef]
- Isaksson, A.K.; Ahlström, G.; Gunnarsson, L.G. Quality of life and impairment in patients with multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2005, 76, 64–69. [Google Scholar] [CrossRef]
- Kyte, D.G.; Calvert, M.; van der Wees, P.J.; ten Hove, R.; Tolan, S.; Hill, J.C. An introduction to patient-reported outcome measures (PROMs) in physiotherapy. Physiotherapy 2015, 101, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Reeves, M.; Lisabeth, L.; Williams, L.; Katzan, I.; Kapral, M.; Deutsch, A.; Prvu-Bettger, J. Patient-Reported Outcome Measures (PROMs) for Acute Stroke: Rationale, Methods and Future Directions. Stroke 2018, 49, 1549–1556. [Google Scholar] [CrossRef] [PubMed]
- Stratford, P.; Gill, C.; Westaway, M.; Binkley, J. Assessing Disability and Change on Individual Patients: A Report of a Patient Specific Measure. Physiother. Can. 1995, 47, 258–263. [Google Scholar] [CrossRef]
- Barten, J.A.; Pisters, M.F.; Huisman, P.A.; Takken, T.; Veenhof, C. Measurement properties of patient-specific instruments measuring physical function. J. Clin. Epidemiol. 2012, 65, 590–601. [Google Scholar] [CrossRef]
- Fairbairn, K.; May, K.; Yang, Y.; Balasundar, S.; Hefford, C.; Abbott, J.H. Mapping Patient-Specific Functional Scale (PSFS) items to the International Classification of Functioning, Disability and Health (ICF). Phys. Ther. 2012, 92, 310–317. [Google Scholar] [CrossRef]
- Mann, M.; Musabyemariya, I.; Harding, L.; Braxley, B. Using Patient-Reported Outcome Measures to Promote Patient-Centered Practice: Building Capacity Among Pediatric Physiotherapists in Rwanda. Glob. Health Sci. Pr. 2020, 8, 596–605. [Google Scholar] [CrossRef]
- Horn, K.K.; Jennings, S.; Richardson, G.; Vliet, D.V.; Hefford, C.; Abbott, J.H. The patient-specific functional scale: Psychometrics, clinimetrics, and application as a clinical outcome measure. J. Orthop. Sport. Phys. Ther. 2012, 42, 30–42. [Google Scholar] [CrossRef]
- Alnahdi, A.H.; Murtada, B.A.; Zawawi, A.T.; Omar, M.T.; Alsobayel, H.I. Cross-cultural adaptation and measurement properties of the Arabic version of the Patient-Specific Functional Scale in patients with lower extremity musculoskeletal disorders. Disabil. Rehabil. 2022, 44, 4104–4110. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Nair, P.; Green, M. Feasibility and informativeness of the Patient-Specific Functional Scale with patients with Parkinson’s disease. Physiother. Theory Pr. 2020, 36, 1241–1244. [Google Scholar] [CrossRef]
- Costa, L.O.; Maher, C.G.; Latimer, J.; Ferreira, P.H.; Ferreira, M.L.; Pozzi, G.C.; Freitas, L.M. Clinimetric testing of three self-report outcome measures for low back pain patients in Brazil: Which one is the best? Spine 2008, 33, 2459–2463. [Google Scholar] [CrossRef]
- Rosengren, J.; Brodin, N. Validity and reliability of the Swedish version of the Patient Specific Functional Scale in patients treated surgically for carpometacarpal joint osteoarthritis. J. Hand Ther. 2013, 26, 53–60, quiz 61. [Google Scholar] [CrossRef] [PubMed]
- Nakamaru, K.; Aizawa, J.; Koyama, T.; Nitta, O. Reliability, validity, and responsiveness of the Japanese version of the Patient-Specific Functional Scale in patients with neck pain. Eur. Spine J. 2015, 24, 2816–2820. [Google Scholar] [CrossRef] [PubMed]
- Puga, V.O.; Lopes, A.D.; Shiwa, S.R.; Alouche, S.R.; Costa, L.O. Clinimetric testing supports the use of 5 questionnaires adapted into Brazilian Portuguese for patients with shoulder disorders. J. Orthop. Sport. Phys. Ther. 2013, 43, 404–413. [Google Scholar] [CrossRef]
- Sharma, S.; Palanchoke, J.; Abbott, J.H. Cross-cultural Adaptation and Validation of the Nepali Translation of the Patient-Specific Functional Scale. J. Orthop. Sport. Phys. Ther. 2018, 48, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Lehtola, V.; Kaksonen, A.; Luomajoki, H.; Leinonen, V.; Gibbons, S.; Airaksinen, O. Content validity and responsiveness of a Finnish version of the Patient-Specific Functional Scale. Eur. J. Physiother. 2013, 15, 134–138. [Google Scholar] [CrossRef]
- Yalçinkaya, G.; Kara, B.; Arda, M.N. Cross-cultural adaptation, reliability and validity of the Turkish version of Patient-Specific Functional Scale in patients with chronic neck pain. Turk. J. Med. Sci. 2020, 50, 824–831. [Google Scholar] [CrossRef]
- Pathak, A.; Wilson, R.; Sharma, S.; Pryymachenko, Y.; Ribeiro, D.C.; Chua, J.; Abbott, J.H. Measurement Properties of the Patient-Specific Functional Scale and Its Current Uses: An Updated Systematic Review of 57 Studies Using COSMIN Guidelines. J. Orthop. Sport. Phys. Ther. 2022, 52, 262–275. [Google Scholar] [CrossRef]
- Halabchi, F.; Alizadeh, Z.; Sahraian, M.A.; Abolhasani, M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurol. 2017, 17, 185. [Google Scholar] [CrossRef]
- Krokavcova, M.; van Dijk, J.P.; Nagyova, I.; Rosenberger, J.; Gavelova, M.; Gdovinova, Z.; Groothoff, J.W. Perceived health status as measured by the SF-36 in patients with multiple sclerosis: A review. Scand. J. Caring Sci. 2009, 23, 529–538. [Google Scholar] [CrossRef]
- Coons, S.J.; Alabdulmohsin, S.A.; Draugalis, J.R.; Hays, R.D. Reliability of an Arabic version of the RAND-36 Health Survey and its equivalence to the US-English version. Med. Care 1998, 36, 428–432. [Google Scholar] [CrossRef]
- Kamper, S.J.; Maher, C.G.; Mackay, G. Global rating of change scales: A review of strengths and weaknesses and considerations for design. J. Man. Manip. Ther. 2009, 17, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Watkins, M.P.; Portney, L.G. Foundations of Clinical Research: Applications to Practice; McGraw-Hill Education LLC: New York, NY, USA, 2015. [Google Scholar]
- Fuhro, F.F.; Fagundes, F.R.C.; Manzoni, A.C.T.; Costa, L.O.P.; Cabral, C.M.N. Örebro Musculoskeletal Pain Screening Questionnaire Short-Form and STarT Back Screening Tool: Correlation and Agreement Analysis. Spine 2016, 41, E931–E936. [Google Scholar] [CrossRef] [PubMed]
- Terwee, C.B.; Mokkink, L.B.; Knol, D.L.; Ostelo, R.W.; Bouter, L.M.; de Vet, H.C. Rating the methodological quality in systematic reviews of studies on measurement properties: A scoring system for the COSMIN checklist. Qual. Life Res. 2012, 21, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Prinsen, C.A.C.; Mokkink, L.B.; Bouter, L.M.; Alonso, J.; Patrick, D.L.; de Vet, H.C.W.; Terwee, C.B. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual. Life Res. 2018, 27, 1147–1157. [Google Scholar] [CrossRef] [PubMed]
- Hobart, J.C.; Riazi, A.; Lamping, D.L.; Fitzpatrick, R.; Thompson, A.J. Measuring the impact of MS on walking ability: The 12-Item MS Walking Scale (MSWS-12). Neurology 2003, 60, 31–36. [Google Scholar] [CrossRef]
- Manjaly, Z.M.; Harrison, N.A.; Critchley, H.D.; Do, C.T.; Stefanics, G.; Wenderoth, N.; Lutterotti, A.; Müller, A.; Stephan, K.E. Pathophysiological and cognitive mechanisms of fatigue in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2019, 90, 642–651. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Mean ± SD or N (%) |
|---|---|
| Age (years) | 33.73 ± 8.87 |
| Gender | Male = 34 (34%) |
| Female = 66 (66%) | |
| Handedness | Right = 61 (61%) |
| Left = 15 (15%) | |
| Ambidextrous = 24 (24%) | |
| Height (cm) | 163.2 ± 9.24 |
| Weight (kg) | 73.65 ± 24.30 |
| Body Mass Index (kg/m2) | 27.51 ± 8.35 |
| Family history with MS | Yes: 16 (16%) |
| No: 84 (84%) | |
| Marital status | Single: 45 (45%) |
| Married 45 (45%) | |
| Divorced 10 (10%) | |
| Level of education | Elementary school: 2 (2%) |
| Middle school: 14 (14%) | |
| High-school: 14 (14%) | |
| Bachelor degree: 68 (68%) | |
| Post-graduate study: 2 (2%) | |
| Onset of MS (months) ** | 62.00 (95.00) * |
| Variable | Mean ± SD |
|---|---|
| PSFS-Ar | 5.43 ± 2.19 |
| RAND-36 physical functioning | 69.35 ± 27.17 |
| RAND-36 role limitation due physical health problems | 51.25 ± 43.42 |
| RAND-36 energy/fatigue | 50.40 ± 25.88 |
| RAND-36 emotional well-being | 60.92 ± 24.16 |
| Mean ± SD | Mean Difference a (95% CI) | ICC2,1 (95% CI) | SEM | MDC95 | |
|---|---|---|---|---|---|
| Test | 5.43 ± 2.19 | 0.155 (−0.25 to 0.56) | 0.87 (0.75–0.93) | 0.80 | 1.87 |
| Retest | 5.33 ± 2.10 | ||||
| Variable | rho (95% CI) | p |
|---|---|---|
| RAND-36 physical functioning | 0.50 (0.33 to 0.64) | <0.001 |
| RAND-36 role limitations due to physical health problems | 0.37 (0.19 to 0.53) | <0.001 |
| RAND-36 energy/fatigue | 0.35 (0.14 to 0.52) | <0.001 |
| RAND-36 emotional well-being | 0.19 (−0.13 to 0.39) | 0.053 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsubiheen, A.M.; Alzain, N.A.; Albishi, A.M.; Shaheen, A.A.M.; Aldaihan, M.M.; Almurdi, M.M.; Alqahtani, A.S.; Alderaa, A.A.; Alnahdi, A.H. Measurement Properties’ Evaluation of the Arabic Version of the Patient-Specific Functional Scale in Patients with Multiple Sclerosis. Healthcare 2023, 11, 1560. https://doi.org/10.3390/healthcare11111560
Alsubiheen AM, Alzain NA, Albishi AM, Shaheen AAM, Aldaihan MM, Almurdi MM, Alqahtani AS, Alderaa AA, Alnahdi AH. Measurement Properties’ Evaluation of the Arabic Version of the Patient-Specific Functional Scale in Patients with Multiple Sclerosis. Healthcare. 2023; 11(11):1560. https://doi.org/10.3390/healthcare11111560
Chicago/Turabian StyleAlsubiheen, Abdulrahman M., Nawaf A. Alzain, Alaa M. Albishi, Afaf A. M. Shaheen, Mishal M. Aldaihan, Muneera M. Almurdi, Abdulfattah S. Alqahtani, Asma A. Alderaa, and Ali H. Alnahdi. 2023. "Measurement Properties’ Evaluation of the Arabic Version of the Patient-Specific Functional Scale in Patients with Multiple Sclerosis" Healthcare 11, no. 11: 1560. https://doi.org/10.3390/healthcare11111560