
Neurological Soft Signs in Schizophrenia, a Picture of the Knowledge in the Last Decade: A Scoping Review
 , , ,
, , ,
Abstract
:1. Introduction
Aim of the Present Study
2. Methods
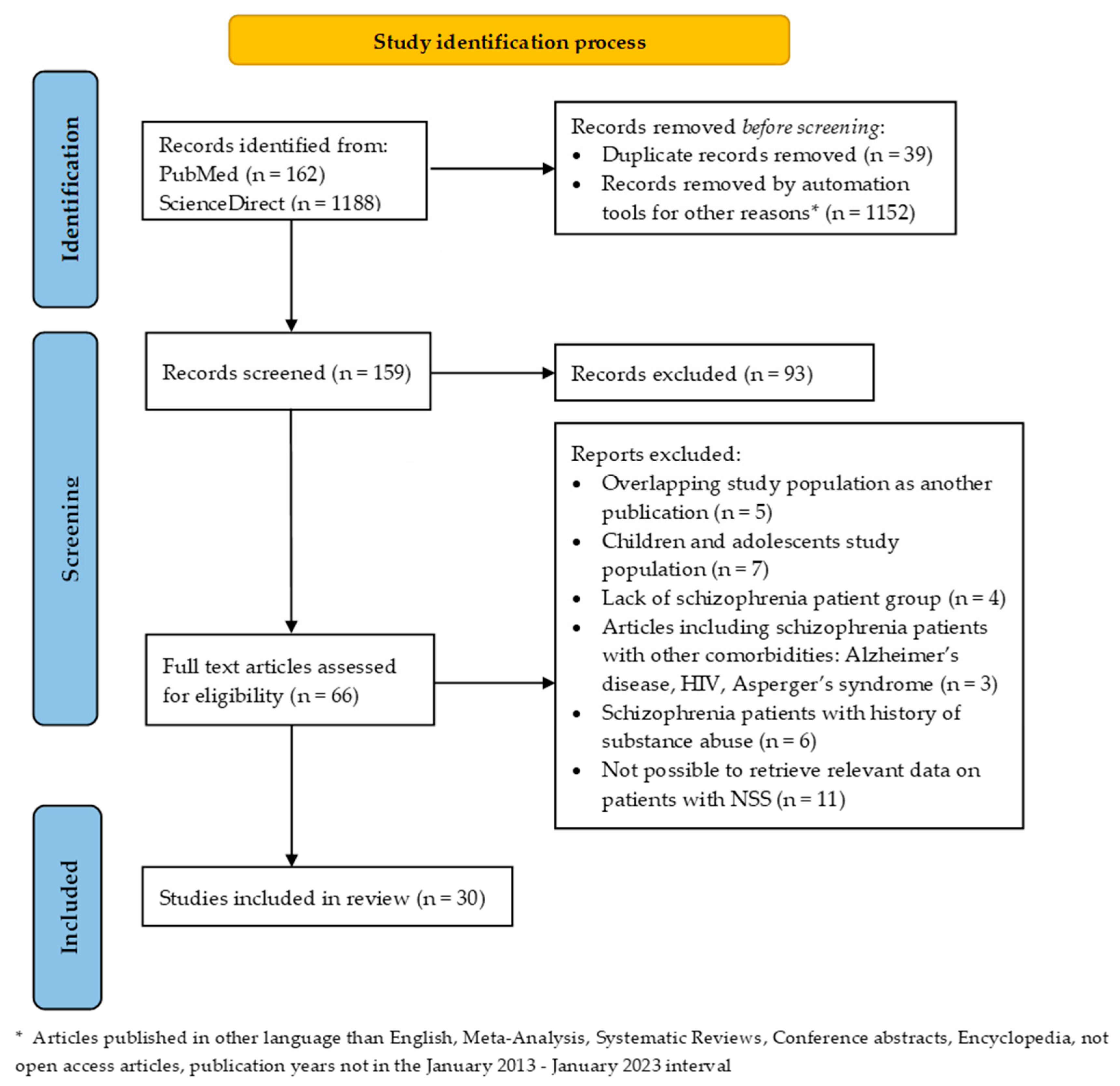
2.1. Screening and Selection Process
2.2. Exclusion Criteria
3. Results
4. Discussion
4.1. NSS Correlation with Symptoms, Demographic Characteristics, and Illness Stage
4.2. NSS Correlation with Medication and Side-Effects
4.3. NSS during Follow-Up
4.4. NSS and Imaging Findings
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baldessarini, R.J. Schizophrenia. N. Engl. J. Med. 1977, 297, 988–995. [Google Scholar] [CrossRef] [PubMed]
- Soares-Weiser, K.; Maayan, N.; Bergman, H.; Davenport, C.; Kirkham, A.J.; Grabowski, S.; Adams, E.C. First rank symptoms for schizophrenia. Cochrane Database Syst. Rev. 2015, 1, CD010653. [Google Scholar] [CrossRef] [PubMed]
- Tsapakis, E.M.; Dimopoulou, T.; Tarazi, F.I. Clinical management of negative symptoms of schizophrenia: An update. In Pharmacology and Therapeutics; Elsevier Inc.: Amsterdam, The Netherlands, 2015; Volume 153, pp. 135–147. [Google Scholar] [CrossRef]
- Huhn, M.; Nikolakopoulou, A.; Schneider-Thoma, J.; Krause, M.; Samara, M.; Peter, N.; Arndt, T.; Bäckers, L.; Rothe, P.; Cipriani, A.; et al. Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: A systematic review and network meta-analysis. Lancet 2019, 394, 939–951. [Google Scholar] [CrossRef] [PubMed]
- Ceraso, A.; Lin, J.J.; Schneider-Thoma, J.; Siafis, S.; Tardy, M.; Komossa, K.; Heres, S.; Kissling, W.; Davis, J.M.; Leucht, S. Maintenance treatment with antipsychotic drugs for schizophrenia. Cochrane Database Syst. Rev. 2020, 8, CD008016. [Google Scholar] [CrossRef]
- Bighelli, I.; Rodolico, A.; García-Mieres, H.; Pitschel-Walz, G.; Hansen, W.-P.; Schneider-Thoma, J.; Siafis, S.; Wu, H.; Wang, D.; Salanti, G.; et al. Psychosocial and psychological interventions for relapse prevention in schizophrenia: A systematic review and network meta-analysis. Lancet Psychiatry 2021, 8, 969–980. [Google Scholar] [CrossRef]
- Bachmann, S.; Schröder, J. Neurological Soft Signs in Schizophrenia: An Update on the State- versus Trait-Perspective. Front. Psychiatry 2018, 8, 272. [Google Scholar] [CrossRef]
- Schröder, J.; Niethammer, R.; Geider, F.-J.; Reitz, C.; Binkert, M.; Jauss, M.; Sauer, H. Neurological soft signs in schizophrenia. Schizophr. Res. 1991, 6, 25–30. [Google Scholar] [CrossRef]
- Boks, M.P.; Russo, S.; Knegtering, R.; Bosch, R.J.V.D. The specificity of neurological signs in schizophrenia: A review. Schizophr. Res. 2000, 43, 109–116. [Google Scholar] [CrossRef]
- Dazzan, P.; Murray, R.M. Neurological soft signs in first-episode psychosis: A systematic review. Br. J. Psychiatry 2002, 181, s50–s57. [Google Scholar] [CrossRef]
- Maatz, A.; Hoff, P.; Angst, J. Eugen Bleuler’s schizophrenia—A modern perspective. Dialog-Clin. Neurosci. 2015, 17, 43–49. [Google Scholar] [CrossRef]
- Compton, M.T.; Fantes, F.; Wan, C.R.; Johnson, S.; Walker, E.F. Abnormal movements in first-episode, nonaffective psychosis: Dyskinesias, stereotypies, and catatonic-like signs. Psychiatry Res. 2015, 226, 192–197. [Google Scholar] [CrossRef]
- Peralta, V.; Campos, M.S.; De Jalón, E.G.; Cuesta, M.J. Motor behavior abnormalities in drug-naïve patients with schizophrenia spectrum disorders. Mov. Disord. 2010, 25, 1068–1076. [Google Scholar] [CrossRef] [PubMed]
- Hirjak, D.; Thomann, P.A.; Kubera, K.M.; Wolf, N.D.; Sambataro, F.; Wolf, R.C. Motor dysfunction within the schizophrenia-spectrum: A dimensional step towards an underappreciated domain. Schizophr. Res. 2015, 169, 217–233. [Google Scholar] [CrossRef] [PubMed]
- Fink, M. Clinical Practice to Change with Divorce of Catatonia and Schizophrenia. J. Clin. Psychopharmacol. 2013, 33, 287–288. [Google Scholar] [CrossRef] [PubMed]
- Rathod, B.; Kaur, A.; Basavanagowda, D.M.; Mohan, D.; Mishra, N.; Fuad, S.; Nosher, S.; Alrashid, Z.A.; Heindl, S.E. Neurological Soft Signs and Brain Abnormalities in Schizophrenia: A Literature Review. Cureus 2020, 12, e11050. [Google Scholar] [CrossRef]
- Samson, G.D.; Lahti, A.C.; Kraguljac, N.V. The neural substrates of neurological soft signs in schizophrenia: A systematic review. Schizophrenia 2022, 8, 42. [Google Scholar] [CrossRef]
- Neelam, K.; Garg, D.; Marshall, M. A systematic review and meta-analysis of neurological soft signs in relatives of people with schizophrenia. BMC Psychiatry 2011, 11, 139. [Google Scholar] [CrossRef]
- Niethammer, R.; Weisbrod, M.; Schiesser, S.; Grothe, J.; Maier, S.; Peter, U.; Kaufmann, C.; Schröder, J.; Sauer, H. Genetic Influence on Laterality in Schizophrenia? A Twin Study of Neurological Soft Signs. Am. J. Psychiatry 2000, 157, 272–274. [Google Scholar] [CrossRef]
- Kelly, B.; Cotter, D.; Denihan, C.; Larkin, D.; Murphy, P.; Kinsella, A.; Walsh, D.; Waddington, J.; Larkin, C.; O’callaghan, E.; et al. Neurological soft signs and dermatoglyphic anomalies in twins with schizophrenia. Eur. Psychiatry 2004, 19, 159–163. [Google Scholar] [CrossRef]
- Picchioni, M.M.; Toulopoulou, T.; Landau, S.; Davies, N.; Ribchester, T.; Murray, R.M. Neurological Abnormalities in Schizophrenic Twins. Biol. Psychiatry 2006, 59, 341–348. [Google Scholar] [CrossRef]
- Baaré, W.F.C.; van Oel, C.; Pol, H.H.; Schnack, H.G.; Durston, S.; Sitskoorn, M.M.; Kahn, R.S. Volumes of Brain Structures in Twins Discordant for Schizophrenia. Arch. Gen. Psychiatry 2001, 58, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Pol, H.E.H.; Schnack, H.G.; Mandl, R.C.; Brans, R.G.; van Haren, N.E.; Baaré, W.F.; van Oel, C.; Collins, D.L.; Evans, A.C.; Kahn, R.S. Gray and white matter density changes in monozygotic and same-sex dizygotic twins discordant for schizophrenia using voxel-based morphometry. Neuroimage 2006, 31, 482–488. [Google Scholar] [CrossRef]
- Chan, R.C.; Xu, T.; Heinrichs, R.W.; Yu, Y.; Gong, Q.-Y. Neurological soft signs in non-psychotic first-degree relatives of patients with schizophrenia: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2010, 34, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, S.; Bottmer, C.; Schröder, J.; Schiffman, J.; Sorensen, M.H.J.; Maeda, M.J.; Mortensen, C.E.L.; Victoroff, M.J.; Hayashi, K.; Michelsen, M.N.M.; et al. Neurological Soft Signs in First-Episode Schizophrenia: A Follow-Up Study. Am. J. Psychiatry 2005, 162, 2337–2343. [Google Scholar] [CrossRef] [PubMed]
- Bombin, I.; Arango, C.; Buchanan, R.W. Significance and Meaning of Neurological Signs in Schizophrenia: Two Decades Later. Schizophr. Bull. 2005, 31, 962–977. [Google Scholar] [CrossRef]
- Chan, R.C.K.; Xu, T.; Heinrichs, R.W.; Yu, Y.; Wang, Y. Neurological Soft Signs in Schizophrenia: A Meta-analysis. Schizophr. Bull. 2009, 36, 1089–1104. [Google Scholar] [CrossRef]
- Dazzan, P.; Lloyd, T.; Morgan, K.D.; Zanelli, J.; Morgan, C.; Orr, K.; Hutchinson, G.; Fearon, P.; Allin, M.; Rifkin, L.; et al. Neurological abnormalities and cognitive ability in first-episode psychosis. Br. J. Psychiatry 2008, 193, 197–202. [Google Scholar] [CrossRef]
- Wolf, R.C.; Rashidi, M.; Schmitgen, M.M.; Fritze, S.; Sambataro, F.; Kubera, K.M.; Hirjak, D. Neurological Soft Signs Predict Auditory Verbal Hallucinations in Patients with Schizophrenia. Schizophr. Bull. 2020, 47, 433–443. [Google Scholar] [CrossRef]
- Biswas, P.; Malhotra, S.; Gupta, N. Comparative study of neurological soft signs in schizophrenia with onset in childhood, adolescence and adulthood. Acta Psychiatr. Scand. 2007, 115, 295–303. [Google Scholar] [CrossRef]
- Mayoral, M.; Bombín, I.; Castro-Fornieles, J.; González-Pinto, A.; Otero, S.; Parellada, M.; Moreno, D.; Baeza, I.; Graell, M.; Rapado, M.; et al. Longitudinal study of neurological soft signs in first-episode early-onset psychosis. J. Child Psychol. Psychiatry 2011, 53, 323–331. [Google Scholar] [CrossRef]
- Mittal, V.A.; Tessner, K.D.; Trottman, H.D.; Esterberg, M.; Dhruv, S.H.; Simeonova, D.I.; McMillan, A.L.; Murphy, E.; Saczawa, M.E.; Walker, E.F. Movement abnormalities and the progression of prodromal symptomatology in adolescents at risk for psychotic disorders. J. Abnorm. Psychol. 2007, 116, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Mittal, V.A.; Walker, E.F. Movement abnormalities predict conversion to Axis I psychosis among prodromal adolescents. J. Abnorm. Psychol. 2007, 116, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Krebs, M.-O.; Gut-Fayand, A.; Bourdel, M.-C.; Dischamp, J.; Olié, J.-P. Validation and factorial structure of a standardized neurological examination assessing neurological soft signs in schizophrenia. Schizophr. Res. 2000, 45, 245–260. [Google Scholar] [CrossRef] [PubMed]
- Schröder, J.; Toro, P. Neurological soft signs predict outcomes in schizophrenia. Nat. Rev. Neurol. 2020, 16, 659–660. [Google Scholar] [CrossRef]
- Chrobak, A.A.; Krupa, A.; Dudek, D.; Siwek, M. How soft are neurological soft signs? Content overlap analysis of 71 symptoms among seven most commonly used neurological soft signs scales. J. Psychiatr. Res. 2021, 138, 404–412. [Google Scholar] [CrossRef]
- Agid, O.; Mamo, D.; Ginovart, N.; Vitcu, I.; Wilson, A.A.; Zipursky, R.B.; Kapur, S. Striatal Vs Extrastriatal Dopamine D2 Receptors in Antipsychotic Response—A Double-Blind PET Study in Schizophrenia. Neuropsychopharmacology 2006, 32, 1209–1215. [Google Scholar] [CrossRef]
- Yu, C.; Zhou, Y.; Liu, Y.; Jiang, T.; Dong, H.; Zhang, Y.; Walter, M. Functional segregation of the human cingulate cortex is confirmed by functional connectivity based neuroanatomical parcellation. Neuroimage 2010, 54, 2571–2581. [Google Scholar] [CrossRef]
- Walther, S.; Strik, W. Motor Symptoms and Schizophrenia. Neuropsychobiology 2012, 66, 77–92. [Google Scholar] [CrossRef]
- Sienaert, P.; Rooseleer, J.; De Fruyt, J. Measuring catatonia: A systematic review of rating scales. J. Affect. Disord. 2011, 135, 1–9. [Google Scholar] [CrossRef]
- Miljević, D.; Nikolić-Kokić, A.; Blagojević, D.; Milovanović, M.; Munjiza, A.; Jukić, M.M.; Pešić, V.; Lečić-Toševski, D.; Spasić, M.B. Association between neurological soft signs and antioxidant enzyme activity in schizophrenic patients. Psychiatry Res. 2018, 269, 746–752. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Varambally, S.; Venkatasubramanian, G.; Gangadhar, B. Neurological soft signs in schizophrenia—The past, the present and the future. Indian J. Psychiatry 2012, 54, 73. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, A.; Rosenbloom, M.J.; Pfefferbaum, A.; Sullivan, E.V. Clinical signs of cerebellar dysfunction in schizophrenia, alcoholism, and their comorbidity. Schizophr. Res. 2002, 57, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Fountoulakis, K.N.; Panagiotidis, P.; Kimiskidis, V.; Nimatoudis, I. 12-Month stability of neurological soft signs in stabilized patients with schizophrenia. Nord. J. Psychiatry 2019, 73, 451–461. [Google Scholar] [CrossRef]
- Sambataro, F.; Fritze, S.; Rashidi, M.; Topor, C.E.; Kubera, K.M.; Wolf, R.C.; Hirjak, D. Moving forward: Distinct sensorimotor abnormalities predict clinical outcome after 6 months in patients with schizophrenia. Eur. Neuropsychopharmacol. 2020, 36, 72–82. [Google Scholar] [CrossRef]
- Chan, R.C.K.; Geng, F.-L.; Lui, S.S.Y.; Wang, Y.; Ho, K.K.Y.; Hung, K.S.Y.; Gur, R.E.; Gur, R.C.; Cheung, E.F.C. Course of neurological soft signs in first-episode schizophrenia: Relationship with negative symptoms and cognitive performances. Sci. Rep. 2015, 5, 11053. [Google Scholar] [CrossRef]
- Kong, L.; Herold, C.J.; Bachmann, S.; Schroeder, J. Neurological soft signs and structural network changes: A longitudinal analysis in first-episode schizophrenia. BMC Psychiatry 2023, 23, 20. [Google Scholar] [CrossRef]
- Buchanan, R.W.; Heinrichs, D.W. The neurological evaluation scale (NES): A structured instrument for the assessment of neurological signs in schizophrenia. Psychiatry Res. 1989, 27, 335–350. [Google Scholar] [CrossRef]
- Chen, E.; Shapleske, J.; Luque, R.; McKenna, P.; Hodges, J.R.; Calloway, S.; Hymas, N.F.; Dening, T.; Berrios, E.G. The Cambridge Neurological Inventory: A clinical instrument for assessment of soft neurological signs in psychiatric patients. Psychiatry Res. 1995, 56, 183–204. [Google Scholar] [CrossRef]
- Chen, B.-Y.; Tsai, I.-N.; Lin, J.-J.; Lu, M.-K.; Tan, H.-P.; Jang, F.-L.; Gan, S.-T. Risk Model Assessment in Early-Onset and Adult-Onset Schizophrenia Using Neurological Soft Signs. J. Clin. Med. 2019, 8, 1443. [Google Scholar] [CrossRef]
- Caldani, S.; Amado, I.; Bendjemaa, N.; Vialatte, F.; Mam-Lam-Fook, C.; Gaillard, R.; Krebs, M.-O.; Bucci, M.P. Oculomotricity and Neurological Soft Signs: Can we refine the endophenotype? A study in subjects belonging to the spectrum of schizophrenia. Psychiatry Res. 2017, 256, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.C.K.; Cui, H.-R.; Chu, M.-Y.; Zhang, T.-H.; Wang, Y.; Wang, Y.; Li, Z.; Lui, S.S.Y.; Wang, J.-J.; Cheung, E.F.C. Neurological soft signs precede the onset of schizophrenia: A study of individuals with schizotypy, ultra-high-risk individuals, and first-onset schizophrenia. Eur. Arch. Psychiatry Clin. Neurosci. 2017, 268, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Fountoulakis, K.N.; Panagiotidis, P.; Kimiskidis, V.; Nimatoudis, I.; Gonda, X. Neurological soft signs in familial and sporadic schizophrenia. Psychiatry Res. 2019, 272, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Fritze, S.; Sambataro, F.; Kubera, K.M.; Bertolino, A.L.; Topor, C.E.; Wolf, R.C.; Hirjak, D. Neurological soft signs in schizophrenia spectrum disorders are not confounded by current antipsychotic dosage. Eur. Neuropsychopharmacol. 2020, 31, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Gay, O.; Plaze, M.; Oppenheim, C.; Gaillard, R.; Olié, J.-P.; Krebs, M.-O.; Cachia, A. Cognitive control deficit in patients with first-episode schizophrenia is associated with complex deviations of early brain development. J. Psychiatry Neurosci. 2017, 42, 87–94. [Google Scholar] [CrossRef]
- Viher, P.V.; Stegmayer, K.; Bracht, T.; Federspiel, A.; Bohlhalter, S.; Strik, W.; Wiest, R.; Walther, S. Neurological Soft Signs Are Associated with Altered White Matter in Patients With Schizophrenia. Schizophr. Bull. 2022, 48, 220–230. [Google Scholar] [CrossRef]
- Cuesta, M.J.; Moreno-Izco, L.; Ribeiro, M.; López-Ilundain, J.M.; Lecumberri, P.; Cabada, T.; Lorente-Omeñaca, R.; Sánchez-Torres, A.M.; Gómez, M.S.; Peralta, V. Motor abnormalities and cognitive impairment in first-episode psychosis patients, their unaffected siblings and healthy controls. Schizophr. Res. 2018, 200, 50–55. [Google Scholar] [CrossRef]
- Feng, Y.; Wang, Z.; Lin, G.; Qian, H.; Gao, Z.; Wang, X.; Li, M.; Hu, X.; Li, Y. Neurological soft signs and neurocognitive deficits in remitted patients with schizophrenia, their first-degree unaffected relatives, and healthy controls. Eur. Arch. Psychiatry Clin. Neurosci. 2020, 270, 383–391. [Google Scholar] [CrossRef]
- Schäppi, L.; Stegmayer, K.; Viher, P.V.; Walther, S. Distinct Associations of Motor Domains in Relatives of Schizophrenia Patients—Different Pathways to Motor Abnormalities in Schizophrenia? Front. Psychiatry 2018, 9, 129. [Google Scholar] [CrossRef]
- Galindo, L.; Bergé, D.; Murray, G.; Mané, A.; Bulbena, A.; Pérez, V.; Vilarroya, O. Default Mode Network Aberrant Connectivity Associated with Neurological Soft Signs in Schizophrenia Patients and Unaffected Relatives. Front. Psychiatry 2018, 8, 298. [Google Scholar] [CrossRef]
- Kong, L.; Lui, S.S.; Wang, Y.; Hung, K.S.; Ho, K.K.; Wang, Y.; Huang, J.; Mak, H.K.; Sham, P.C.; Cheung, E.F.; et al. Structural network alterations and their association with neurological soft signs in schizophrenia: Evidence from clinical patients and unaffected siblings. Schizophr. Res. 2021, 248, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.A.; Buckley, P.F.; Meltzer, H.Y. The brief psychiatric rating scale: Effect of scaling system on clinical re-sponse assessment. J. Clin. Psychopharmacol. 1994, 14, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Guy, W. ECDEU Assessment Manual for Psychopharmacology. Abnormal Involuntary Movement Scale (AIMS); National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs: Rockville, MD, USA, 1976; Volume 1, pp. 534–537. [Google Scholar]
- Barnes, T.R.E. A Rating Scale for Drug-Induced Akathisia. Br. J. Psychiatry 1989, 154, 672–676. [Google Scholar] [CrossRef]
- Simpson, G.M.; Angus, J.W. A rating scale for extrapyramidal side effects. Acta Psychiatr. Scand. 1970, 45, 11–19. [Google Scholar] [CrossRef]
- Focseneanu, B.; Dobrescu, I.; Marian, G.; Rusanu, V. Neurological soft signs in early stage of schizophrenia associated with obsessive-compulsive disorder. J. Med. Life 2015, 8, 74–81. [Google Scholar]
- Zhao, Q.; Ma, Y.-T.; Lui, S.S.; Liu, W.-H.; Xu, T.; Yu, X.; Tan, S.-P.; Wang, Z.-R.; Qu, M.; Wang, Y.; et al. Neurological soft signs discriminate schizophrenia from major depression but not bipolar disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2013, 43, 72–78. [Google Scholar] [CrossRef]
- Petrescu, C.; Papacocea, I.R.; Vilciu, C.; Mihalache, O.A.; Vlad, D.M.; Marian, G.; Focseneanu, B.E.; Sima, C.T.; Ciobanu, C.A.; Riga, S.; et al. The Impact of Antipsychotic Treatment on Neurological Soft Signs in Patients with Predominantly Negative Symptoms of Schizophrenia. Biomedicines 2022, 10, 2939. [Google Scholar] [CrossRef]
- Herold, C.J.; Lässer, M.M.; Seidl, U.W.; Hirjak, D.; Thomann, P.A.; Schröder, J. Neurological Soft Signs and Psychopathology in Chronic Schizophrenia: A Cross-Sectional Study in Three Age Groups. Front. Psychiatry 2018, 9, 98. [Google Scholar] [CrossRef]
- Herold, C.J.; Duval, C.Z.; Lässer, M.M.; Schröder, J. Neurological soft signs (NSS) and cognitive impairment in chronic schizophrenia. Schizophr. Res. Cogn. 2018, 16, 17–24. [Google Scholar] [CrossRef]
- de Bartolomeis, A.; Prinzivalli, E.; Callovini, G.; D’Ambrosio, L.; Altavilla, B.; Avagliano, C.; Iasevoli, F. Treatment resistant schizophrenia and neurological soft signs may converge on the same pathology: Evidence from explanatory analysis on clinical, psychopathological, and cognitive variables. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 81, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Iasevoli, F.; Avagliano, C.; Altavilla, B.; Barone, A.; Ciccarelli, M.; D’Ambrosio, L.; Francesco, D.N.; Razzino, E.; Fornaro, M.; de Bartolomeis, A. Evaluation of a few discrete clinical markers may predict categorization of actively symptomatic non-acute schizophrenia patients as treatment resistant or responders: A study by ROC curve analysis and multivariate analyses. Psychiatry Res. 2018, 269, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Escudero, D.Q.; Herold, C.J.; Kong, L.; Schröder, J. Neurological soft signs (NSS) and gray matter volume (GMV) in first-episode psychosis: An analysis of NSS motor subscores. Psychiatry Res. Neuroimaging 2020, 300, 111067. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.-L.; Wang, Y.-M.; Wang, Y.; Zhou, H.-Y.; Huang, J.; Wang, Y.; Lui, S.S.Y.; Møller, A.; Hung, K.S.Y.; Mak, H.K.F.; et al. Neurological Soft Signs Are Associated with Altered Cerebellar-Cerebral Functional Connectivity in Schizophrenia. Schizophr. Bull. 2021, 47, 1452–1462. [Google Scholar] [CrossRef]
- Hirjak, D.; Rashidi, M.; Fritze, S.; Bertolino, A.L.; Geiger, L.S.; Zang, Z.; Kubera, K.M.; Schmitgen, M.M.; Sambataro, F.; Calhoun, V.D.; et al. Patterns of co-altered brain structure and function underlying neurological soft signs in schizophrenia spectrum disorders. Hum. Brain Mapp. 2019, 40, 5029–5041. [Google Scholar] [CrossRef] [PubMed]
- Hirjak, D.; Wolf, R.C.; Stieltjes, B.; Hauser, T.; Seidl, U.; Thiemann, U.; Schröder, J.; Thomann, P.A. Neurological Soft Signs and Brainstem Morphology in First-Episode Schizophrenia. Neuropsychobiology 2013, 68, 91–99. [Google Scholar] [CrossRef]
- Herold, C.J.; Essig, M.; Schröder, J. Neurological soft signs (NSS) and brain morphology in patients with chronic schizophrenia and healthy controls. PLoS ONE 2020, 15, e0231669. [Google Scholar] [CrossRef]
- Cuesta, M.J.; Lecumberri, P.; Moreno-Izco, L.; López-Ilundain, J.M.; Ribeiro, M.; Cabada, T.; Lorente-Omeñaca, R.; de Erausquin, G.; García-Martí, G.; Sanjuan, J.; et al. Motor abnormalities and basal ganglia in first-episode psychosis (FEP). Psychol. Med. 2020, 51, 1625–1636. [Google Scholar] [CrossRef]
- Hirjak, D.; Kubera, K.M.; Wolf, R.C.; Thomann, A.K.; Hell, S.K.; Seidl, U.; Thomann, P.A. Local brain gyrification as a marker of neurological soft signs in schizophrenia. Behav. Brain Res. 2015, 292, 19–25. [Google Scholar] [CrossRef]
- Bora, E.; Akgül, Ö.; Ceylan, D.; Özerdem, A. Neurological soft signs in bipolar disorder in comparison to healthy controls and schizophrenia: A meta-analysis. Eur. Neuropsychopharmacol. 2018, 28, 1185–1193. [Google Scholar] [CrossRef]
- Bachmann, S.; Degen, C.; Geider, F.J.; Schröder, J. Neurological Soft Signs in the Clinical Course of Schizophrenia: Results of a Meta-Analysis. Front. Psychiatry 2014, 5, 185. [Google Scholar] [CrossRef] [PubMed]
- Cantor-Graae, E.; McNeil, T.F.; Rickler, K.C.; Sjostrom, K.; Rawlings, R.; Higgins, E.S.; Hyde, T.M. Are neurological abnormalities in well discordant monozygotic co-twins of schizophrenic subjects the result of perinatal trauma? Am. J. Psychiatry 1994, 151, 1194–1199. [Google Scholar] [CrossRef] [PubMed]
- Tishler, T.A.; Bartzokis, G.; Lu, P.H.; Raven, E.P.; Khanoyan, M.; Kirkpatrick, C.J.; Pyle, M.H.; Villablanca, J.P.; Altshuler, L.L.; Mintz, J.; et al. Abnormal Trajectory of Intracortical Myelination in Schizophrenia Implicates White Matter in Disease Pathophysiology and the Therapeutic Mechanism of Action of Antipsychotics. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2017, 3, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Kraguljac, N.V.; Anthony, T.; Skidmore, F.M.; Marstrander, J.; Morgan, C.J.; Reid, M.A.; White, D.M.; Jindal, R.D.; Skefos, N.H.M.; Lahti, A.C. Micro- and Macrostructural White Matter Integrity in Never-Treated and Currently Unmedicated Patients With Schizophrenia and Effects of Short-Term Antipsychotic Treatment. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2019, 4, 462–471. [Google Scholar] [CrossRef]
- Papiol, S.; Fatjó-Vilas, M.; Schulze, T.G. Neurological soft signs in patients with schizophrenia: Current knowledge and future perspectives in the post-genomics era. Transl. Dev. Psychiatry 2016, 4, 30071. [Google Scholar] [CrossRef]
- Koning, J.P.; Tenback, D.E.; van Os, J.; Aleman, A.; Kahn, R.S.; van Harten, P.N. Dyskinesia and Parkinsonism in Antipsychotic-Naive Patients with Schizophrenia, First-Degree Relatives and Healthy Controls: A Meta-analysis. Schizophr. Bull. 2008, 36, 723–731. [Google Scholar] [CrossRef]
- Bohlken, M.M.; Mandl, R.C.; Brouwer, R.M.; Heuvel, M.P.D.; Hedman, A.M.; Kahn, R.S.; Pol, H.E.H. Heritability of structural brain network topology: A DTI study of 156 twins. Hum. Brain Mapp. 2014, 35, 5295–5305. [Google Scholar] [CrossRef]
- van Haren, N.E.; Rijsdijk, F.; Schnack, H.G.; Picchioni, M.M.; Toulopoulou, T.; Weisbrod, M.; Sauer, H.; van Erp, T.G.; Cannon, T.D.; Huttunen, M.O.; et al. The Genetic and Environmental Determinants of the Association between Brain Abnormalities and Schizophrenia: The Schizophrenia Twins and Relatives Consortium. Biol. Psychiatry 2012, 71, 915–921. [Google Scholar] [CrossRef]
- Shinn, A.K.; Baker, J.T.; Lewandowski, K.E.; Cohen, B.M. Aberrant cerebellar connectivity in motor and association networks in schizophrenia. Front. Hum. Neurosci. 2015, 9, 134. [Google Scholar] [CrossRef]
- Bombin, I.; Arango, C.; Buchanan, R.W. Assessment Tools for Soft Signs. Psychiatr. Ann. 2003, 33, 170–176. [Google Scholar] [CrossRef]


{kind=link}
| Author/Year/Country | Patients/Healthy Controls/Relatives | Age Mean (SD) | Follow-Up | Illness Stage | NSS Assessment Instrument | Clinical Course Assessment Instrument | Medication Mean (SD) | Side Effects/Parkinsonism | NSS Results Mean (SD) | Main Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| [45] Fountoulakis/2019/ Greece | Patients (n = 133) | 33.55 (11.22) | Longitudinal t0 baseline t1 12 months follow-up | stabilized | NES | PANSS PANSS-P t0:16.22 (5.81) t1:14.20 (4.61) PANSS-N t0:18.17 (7.37) t1: 20.02 (6.71) PANSS-G t0:26.20 (7.03) t1:26.16 (6.87) | 6.25 (6.05) mg/day haloperidol equivalents. 35 of the patients were not under medication at baseline. | SAS ESRS UKUS | NES-SI t0:4.29 (3.09) t1:5.12 (3.04) NES-MC t0:3.89 (2.84) t1:3.44 (2.59) NES-CMA t0:6.67 (3.50) t1:6.71 (3.35) NES-OS t0:4.68 (3.51) t1:5.18 (3.39) NES Total t0:19.54 (9.48) t1:20.45 (8.87) | NSS have been constant over a 12-month period except for SI, which deteriorated significantly despite improvements in the rest of the clinical picture. |
| [46] Sambataro/2020/Germany | Patients (n = 43) | 37.55 (10.39) | Longitudinal t0: baseline t1: 28 Weeks | partial remission | Heidelberg | PANSS PANSS-P t0:15.32 (7.32) t1:11.48 (5.68) PANSS-N t0:18.46 (8.27) t1:14.76 (5.71) PANSS-G t0:36.44 (12.62) t1:30.04 (9.0) PANSS-T t0:70.23 (23.39) t1:55.81 (17.49) BPRS Total score t0:39.23 (13.94) t1:30.06 (9.58) | t0:18.09 (9.89) OLZ t1: 18.75 (8.25) OLZ | AIMS t0:0.67 (1.5) t1:0.44 (1.14) SAS t0:2.74 (1.9) t1:1.83 (1.91) BARS t0:1.0 (1.25) t1:0.62 (1.0) | MC t0:8.18 (3.84) t1:6.51 (4.16) COMT t0:3.65 (2.23) t1:2.48 (2.34) IF t0:2.86 (1.56) t1:2.39 (1.46) RLSPO t0:2.72 (2.6) t1:6 2.2 (2.3) HS t0:3.25 (1.6) t1:2.67 (1.86) Total t0:20.19 (8.01) t1:15.97 (9.02) | With antipsychotic therapy, NSS, parkinsonism, and catatonic symptoms improved and displayed a substantial decline >6 months after the acute psychotic episode. NSS scores at baseline predicted PANSS positive and negative symptoms change at >6 months follow-up |
| [47] Chan/2015/China | PNS (N = 29) NPNS (N = 116) HC (N = 62) | 22.34 (4.06) 21.69 (3.768) 21.16 (1.89) | Longitudinal T1–baseline T2–6 months T3–12 months | first episode schizophrenia | CNI | PANSS PANSS-T 60.93 (13.91) 42.16 (14.91) PANSS-N 21.79 (5.22) 9.48 (3.51) PANSS-P 12.34 (5.44) 10.98 (5.05) | 14 patients receiving no treatment | SAS AIMS BARS | CNI-Total 7.13 (3.17) 5.61 (3.07) 2.76 (2.21) CNI-MC 3.68 (1.98) 2.64 (1.88) 1.34 (1.28) CNI-SI 2.26 (1.50) 1.99 (1.40) 0.74 (1.13) CNI-D 1.19 (0.97) 0.98 (0.93) 0.68 (0.65) | PNS had significantly more motor coordination impairment and total NSS than NPNS. |
| [51] Chen/2019/Taiwan | Total (N = 205) EOS (N = 82) AOS (N = 123) FS (N = 134) HC (N = 243) | 41.89 (9.58) 36.85 (9.91) 43.59 (9.19) 56.52 (14.97) 42.10 (10.95) | cross-sectional | stabilized | NES 2 Raters | DIGS | NA | NA | NES Total EOS 9.95 (6.91) AOS 7.58 (5.44) C 1.43 (1.69) NES-SI EOS 1.43 (1.71) AOS 0.59 (0.85) C 0.15 (0.43) NES-MC EOS 0.93 (1.69) AOS 0.38 (0.54) C 0.02 (0.13) NES-CMA EOS 2.17 (1.84) AOS 1.99 (1.69) C 0.43 (0.68) NES-OS EOS 4.26 (2.97) AOS 3.10 (1.87) C 0.43 (0.68) | EOS patients had more severe SI and MC scores than AOS patients. On the SI and MC NSS subscales, there were substantial differences between non-psychotic relatives of EOS and AOS patients. |
| [52] Caldani/2017/ France | HC (n = 48) FS (n = 41) SZ (n = 49) UHR (n = 24) | 25 (5) 28 (9) 28 (6) 21 (3) | cross-sectional | stabilized symptoms | Krebs Scale | PANSS PANSS- P 13 (5) PANSS- N 18 (6) PANSS- G 31 (9) PANSS-T 61 (19) BPRS | 41 patients treated with anti- psychotics; 7 patients received no treatment | SAS AIMS | NSS total 5 (4) 6 (4) 12 (8) 11 (5) | Patients had more intrusive saccade eye movements than siblings or controls. In smooth pursuit, patients with high NSS ratings made more intrusive saccades than patients with low NSS scores and controls |
| [53] Chan/2018/China | HC (N = 39) Schizotypy (N = 39) UHR (N = 39) Patients (N = 39) | 18.36 (2.08) 19.31 (2.54) 18.03 (5.01) 18.00 (3.75) | cross-sectional | first episode schizophrenia | CNI | PANSS PANSS-P 11.17 (4.49) PANSS-N 15.17 (6.62) PANSS-G 24.33 (7.02) SIPS | antipsychotic-naïve | not specified | CNI-SI 1.44 (1.37) 1.51 (1.34) 2.36 (1.35) 2.03 (1.37) CNI-MC 0.79 (1.36) 0.74 (1.12) 0.67 (1.13) 2.92 (2.17) CNI-D 0.74 (0.99) 0.92 (0.98) 0.92 (1.46) 1.00 (1.03) CNI-Total 2.97 (2.32) 3.18 (2.35) 3.95 (2.48) 5.95 (3.41) | UHR patients had a greater prevalence of NSS than healthy controls. Individuals with first-episode schizophrenia had a greater frequency of NSS than HC and UHR. |
| [54] Fountoulakis/2019/ Greece | HC (n = 110) Patients (n = 120) | 33.38 (10.14) 32.79 (11.11) | cross sectional | NA | NES | NA | 6.07 (6.12) mg/day haloperidol equivalents 33 patients receiving no medication. | NA | NES-SI 0.12 (0.40) 4.33 (3.18) NES-MC 0.20 (0.54) 3.93 (2.77) NES-CMA 0.54 (0.83) 6.61 (3.53) NES-OS 0.19 (0.61) 4.53 (3.49) NES Total 1.05 (1.42) 19.40 (9.44) | The patients had greater NES scores than controls, but sporadic cases of schizophrenia had lower MC scores than familiar cases. |
| [55] Fritze/2019/Germany | Total (n = 105) schizophrenia (n = 94) schizoaffective (n = 6) Schizotypal (n = 5) | 38.02 (12.07) | cross-sectional | partial remission | Heidelberg | PANSS PANSS-P 16.1 (7.34) PANSS-N 17.49 (7.91) PANSS-G 36.46 (11.22) PANSS-T 70.04 (21.65) CGI-S 3.94 (1.05) | 17.68 (10.49) OLZ equivalent 8 patients with no antipsychotic treatment 63 patients receiving one antipsychotic 34 patients receiving two antipsychotics | AIMS SAS BARS | MC 8.01 (4.12) IF 2.71 (1.57) COMT 3.47 (2.24) RLSPO 2.83 (2.6) HS 3.06 (1.74) | The dose of antipsychotic medication had no significant impact on NSS values. |
| [58] Cuesta/2018/Spain | Patients (n = 50) FS (n = 21) HC (n = 24) | 25.5 (5.7) 24.9 (6.6) 23.2 (5.7) | cross-sectional | first- episode psychosis | NES 3 Raters | CASH positive 0.48 (0.64) negative 0.68 (0.83) disorganization 0.39 (0.57) mania 0.46 (0.81) depression 0.68 (0.93) | 428.15 (299.87) CPZ | SAS 4.20 (3.82) 1.57 (1.66) 0.58 (1.13) BARS 0.48 (0.86) 0.00 (0.00) 0.00 (0.00) BFCRS 2.26 (3.89) 0.33 (0.96) 0.13 (0.61) | NES total 13.42 (6.44) 8.57 (6.09) 5.75 (4.46) NES-SI 2.5 (1.82) 1.71 (2.02) 1.33 (1.37) NES-MC 2.04 (2.26) 0.81 (1.03) 0.33 (0.86) NES-CMA 2.86 (2.24) 1.38 (1.68) 1.13 (1.26) NES-OS 6.02 (3.79) 4.66 (4.21) 2.95 (2.61) | In all three subgroups, higher NSS scores were associated with worse cognitive performance. Extrapyramidal symptoms were associated with cognitive impairment in FEP patients but not in unaffected relatives or healthy controls. In FEP patients, the NES total score was associated with poor attention performance. |
| [59] Feng/ 2020/ China | Patients (n = 86) FS (n = 86) HC (n = 86) | 30.79 (8.17) 33.92 (10.07) 30.01 (7.47) | cross-sectional | patients with a remission course. | CNI | BPRS 2 Raters 25.23 (5.53) | 104.41 (68.84) CPZ | NA | CNI-D 0.65 (1.08) 0.53 (0.98) 0.58 (0.94) CNI-MC 5.12 (4.01) 4.16 (2.84) 2.41 (1.85) CNI-SI 2.86 (2.94) 1.14 (1.43) 1.43 (1.44) CNI Total 8.63 (5.98) 5.84 (4.44) 4.42 (2.78) | In all subscales except disinhibition and motor coordination, patients had more NSS than first-degree relatives. NSS revealed significantly greater abnormalities in FDR than in controls. |
| [60] Schäppi/2018/Switzerland | HC N: 29 FS N: 34 Patients (N = 43) | 40.86 (14.38) 42.74 (15.73) 37.98 (11.37) | cross-sectional | NA | NES | PANSS PANSS-T 71.14 (16) PANSS-P 17.98 (6.28) PANSS-N 18.14 (5.15) | NA | AIMS Total 0.14 (0.52) 1.15 (2.36) 1.91 (2.7) | NES Total 3.90 (3.59) 11.65 (8.18) 13.74 (11.75) NES-SI 1.14 (1.19) 2.94 (2.15) 3.58 (5.12) NES-MC 0.55 (0.78) 1.79 (1.82) 2.60 (2.84) NES-CMA 1.03 (1.96) 3.21 (2.72) 2.60 (2.96) NES-OS 1.14 (1.43) 3.71 (3.44) 4.88 (4.73) | The patients’ relatives had higher NSS ratings than healthy controls. Complex fine motor function was normal in relatives but impaired in patients. |
| [68] Focseneanu/2015/ Romania | Schizophrenia patients (n = 26) Schizophrenia + OCD Patients (n = 17) | aged up to 26 years | cross-sectional | recent relapse requiring hospitalization or corrective therapeutic intervention | NES | SCID-I/P (the Structured Clinical Interview for DSM IV Axis, I Disorders | NA | NA | NES Total 6.65 (5.04) 10.00 (4.89) NES-MC 0.80 (0.98) 1.05 (1.29) NES-SI 1.50 (1.55) 2.23 (1.32) NES-CMA 2.34 (1.85) 4.64 (2.08) NES-OS 2.00 (1.93) 2.05 (1.98) | NSS scores distinguished patients with schizophrenia associated with OCD from those with schizophrenia, with variations most noticeable in the subscale of CMA. |
| [69] Zhao/2013/China | Patients (n = 30) HC (n = 30) | 26.20 (5.78) 26.60 (5.97) | cross-sectional | NA | CNI 2 Raters | 2 Raters PANSS-T 50.87 (12.74) | 316.36 (252.61) CPZ | NA | CNI-MC 2.03 (1.88) 0.77 (1.10) CNI-SI 1.23 (1.07) 0.77 (0.82) CNI-D 1.77 (1.45) 0.80 (0.81) Total NSS 5.03 (2.88) 2.33 (1.81) | Schizophrenia patients had more NSS signs than healthy subjects. Antipsychotic dose did not influence NSS total and subscales scores. |
| [70] Petrescu/2022/ Romania | Patients (n = 99) | 30.6 (10.4) | cross-sectional | Mixed (non-predominantly negative symptoms patients and Patients with predominantly negative symptoms) | NES | PANSS PANSS-P 21.6 (6.06) PANSS-N 21.4 (6.32) PANSS-G 41.8 (8.66) PANSS-T 84.8 (16.8) | Typical and atypical antipsychotics 424 (219) mg CPZ | SAS 3.04 (2.01) | NES-SI 1.67 (1.52) NES-MC 2.08 (1.60) NES-CMA 3.12 (1.98) NES-OS 3.57 (2.62) NES Total 10.5 (5.50) | Patients with predominantly negative symptoms had higher overall NES and PANSS scores, needed higher daily doses of antipsychotic medications, and were hospitalized for extended lengths of time. |
| [71] Herold/2018/Germany | Patients (n = 90) HC (n = 60) | Y: 23.71 (3.18) M: 40.76 (5.85) O: 61.15 (7.46) Y: 21.60 (3.06) M: 42.41 (5.30) O: 58.00 (7.08) | cross-sectional | Chronic + Subchronic in three age groups (18–29 Young, 30–49 Middle, +50 Older) | 3 Raters Heidelberg | BPRS (Patients) TOTAL Y: 41.53 (9.42) M: 39.82 (9.57) O: 34.85 (7.23) SAPS SANS AES (Patients) TOTAL Y: 25.14 (12.94) M: 27.41(10.80) O: 28.19(13.18) | Y: 726.00 (730.14) CPZ M: 730.42 (698.41) CPZ O: 577.42 (552.16) CPZ | NA | NSS Total (Patients) Y: 12.10 (8.56) M: 13.42 (10.82) O: 27.58 (15.36) NSS Total (HC) Y: 2.30 (1.64) M: 3.00 (2.40) O: 5.76 (3.73) | NSS increases with age in both schizophrenia patients and healthy controls, with the effect being more pronounced in the patients group. In patients with chronic schizophrenia, increased NSS scores are associated with illness duration, positive symptoms disorder, and apathy. |
| [72] Herold/2019/ Germany | Patients (n = 80) HC (n = 60) | 43.36 (15.00) 47.52 (14.80) | cross-sectional | Chronic + Subchronic | Heidelberg | BPRS Total = 38.60 (9.17) SAPNS AES Total = 27.05 (12.15) | 718.15 (691.43) CPZ | NA | Total 17.96 (13.94) 4.40 (3.44) MC 7.00 (6.15) 1.73 (1.73) SI 2.71 (2.23) 0.85 (1.13) COMT 3.05 (2.61) 1.08 (1.21) RLSPO 3.56 (3.62) 0.37 (0.78) HS 1.73 (2.04) 0.38 (0.83) | ToM (theory of mind) overall scores and the subscores “questions” and “order” were significantly linked with NSS total score and NSS subscales. NSS scores were considerably higher in older individuals with chronic schizophrenia who also had severe neurocognitive deficits. There were no substantial correlations between CPZ equivalents and NSS scores. |
| [73] de Bartolomeis/2018/ Italy | TRS (n = 26) SZ (n = 29) | 39.7 (11.7) 35.0 (9.0) | cross-sectional | stabilized symptoms | NES | PANSS 2 Raters CGI-S | 547.8 (210.4) CPZ (mg) 352.9 (217.3) CPZ (mg) | AIMS BARS NRS | NES-SI 5.6 (2.8) 3.6 (2.4) NES-MC 4.7 (2.9) 3.1 (2.1) NES-CMA 5.7 (3.5) 5.3 (3.3) NES-OS 11.5 (5.4) 6.9 (2.6) NES total 27.5 (12.1) 18.8 (6.6) | The more meaningful predictors of TRS diagnosis were higher SI and OS subscale scores, greater disease severity, and higher antipsychotic doses. NSSs were more severe in TRS patients than in SZ patients. |
| [74] Iasevoli/2018/Italy | TRS (n = 28) ARS (n = 32) | 39.79 (11.31) 35.09 (9.02) | cross sectional | stabilized | NES | PANSS PANSS-P 19.41 (5.49) 18.51 (6.09) PANSS-N 26.61 (5.46) 22.56 (5.51) PANSS-G 49.26 (9.91) 45.34 (9.86) PANSS-T 96.03 (16.43) 86.72 (17.63) | CPZ 539.93 (214.51) 369.45 (215.41) | NA | NES Total 27.14 (11.74) 18.19 (6.72) | NSS is suggestive of TRS being a distinct subtype of schizophrenia with its own neurobiology and clinical course, possibly related to abnormal neurodevelopment. |
| Author/Year/Country | Patients/Healthy Controls/Relatives | Age | Illness Stage | NSS Assessment | Clinical Course Assessment | Medication | Structural Assessment | Region of Interest | NSS Results | Main Finding |
|---|---|---|---|---|---|---|---|---|---|---|
| [48] Kong/2023/Germany | Patients (n = 20) [NSS decreasing subgroup (n = 10) NSS persisting subgroup (n = 10)] HC (n = 20) | 25.6 (7.2) 24.1 (3.5) | First episode + follow-up after a mean of 13.8 months | Heidelberg | PANSS | baseline 549.3 (271.3) CPZ follow-up 443.8 (137.7) CPZ | T1- weighted magnetization-prepared rapid gradient echo (MP-RAGE) | Whole Brain | Decreasing NSS (n = 10) NSS baseline 15.9 (3.9) NSS Follow-up 7.2 (3.5) Persisting NSS (n = 10) NSS baseline 14.6 (9.2) NSS Follow-Up 14 (9.5) | Compared to the NSS-decreasing subgroup, the NSS-persisting subgroup displayed more widespread local alterations at follow-up affecting frontal and temporal cortices, the insula, the putamen, and the cerebellum |
| [56] Gay/2017/France | Patients (n = 41) | 25.8 (6.0) | first episode | Krebs scale | PANSS | 16 patients with no treatment 25 Low dosage of anti- psychotics 522 (414) mg CPZ | T1- weighted images | Cortex CSF | Total score 10.6 (6.3) | Anterior cingulate cortex (ACC) morphology’s impact on cognition is moderated by ventricle/sulcal enlargement, meaning that greater enlargement correlates with worse cognitive function. NSS are associated with executive impairments and handedness and correlates with ACC morphology. |
| [57] Viher/2022/Switzerland | HC (n = 42) Patients (n = 41) | 39.3 (13.7) 37.9 (11.6) | NA | NES | PANSS-P 18.2 (6.3) PANSS-N 18.2 (5.2) PANSS-T 71.7 (17.1) | 90% received antipsychotic treatment. 419.0 (362.9) CPZ | Diffusion tensor imaging Diffusion-weighted image | Whole Brain | NES total 3.7 (3.7) 12.2 (10.9) NES-SI 1.1 (1.2) 2.5 (2.6) NES-MC 0.6 (1.2) 2.2 (2.6) NES-CMA 0.9 (1.8) 3.0 (2.9) NES-OS 1.0 (1.4) 4.6 (4.6) | Patients had decreased fractional anisotropy (FA) values in various white matter regions, particularly the corpus callosum and anterior corona radiata, compared to HC. The total score of the NES scale was not associated with FA values |
| [61] Galindo/2017/Spain | HC (n = 35) FS (n = 23) Patients (n = 27) | 36.60 (8.0) 41.39 (10.3) 37.60 (7.0) | clinically stable for the last 6 months | NES | PANSS | atypical antipsychotics | T1-weighted images default mode network (DMN) | Medial prefrontal cortex Posterior cingulate cortex Precuneus Anterior cingulate cortexes Angular gyruses Inferior parietal lobes Dorsolateral prefrontal cortex Angular gyruses | NES-MC 1.16 (1.05) 2.54 (2.55) 3.83 (2.2) NES-SI 1.18 (0.93) 1.67 (0.92) 3.03 (2.28) NES-SCMA 0.84 (1.22) 4.29 (1.55) 4.31 (1.81) NES-OS 1.5 (1.66) 2.42 (2.0) 5.79 (6.44) Total NES 4.68 (3.35) 10.92 (3.87) 16.97 (6.44) | Left caudate nucleus connectivity correlated significantly with NSS Schizophrenia patients and their unaffected relatives have greater NSS scores than controls. |
| [62] Kong/2022/ China | HC (n = 60) FS (n = 25) Patients (n = 62) | 27.20 (6.21) 27.12 (7.26) 27.39 (6.37) | First-episode | CNI | NA | CPZ 329.44 (166.12) | T1-weighted MP-RAGE | Whole Brain | CNI-MC 1.50 (1.42) 2.40 (2.36) 3.71 (2.34) CNI-SI 0.42 (0.77) 0.96 (1.17) 1.24 (1.36) CNI-D 1.00 (0.61) 1.28 (0.68) 1.00 (0.91) CNI Total 2.92 (1.98) 4.64 (3.24) 5.95 (3.16) | Similar grey matter characteristics were observed in IC-5 (superior temporal gyrus, inferior frontal gyrus, and insula network) and IC-10 (parahippocampal gyrus, fusiform, thalamus, and insula network) in unaffected siblings and healthy controls. NSS were negatively associated with aberrant grey matter covarying networks in schizophrenia patients (IC-1 and IC-5), unaffected siblings (IC-3), and healthy controls (IC-5), indicating distinct NSS-related grey matter covarying patterns in each of the three groups. |
| [75] Quispe/2020/Spain | Patients = 102 | 24.9 (4.8) | Schizophrenia spectrum psychoses after remission of acute symptoms. | Heidelberg | BPRS 37.5 (15.8) | CPZ 722.2 (429) | T1- weighted 3D magnetization prepared rapid gradient echo sequence (MP- RAGE) | All brain structures | Total 14.2 (6.7) | The motor subscores of NSS were negatively correlated with the right superior frontal gyrus, thalamus, right caudate, and left precentral gyrus. |
| [76] Cai/2021/China | HC (n = 49) SZ (n = 50) | 27.45 (6.42) 27.68 (6.27) | NA | CNI | PANSS PANSS-P 9.72 (3.09) PANSS-N 11.38 (5.96) PANSS-G 20.70 (5.09) SANS SANS Alogia 1.78 (2.92) SANS Avolition 1.58 (2.32) SANS Anhedonia 2.72 (4.08) SANS Attention 2.38 (2.22) | CPZ mg 340.83 (174.32) | Cerebellar- cerebral resting- state functional connectivity | Whole Brain | CNI-MC 1.33 (1.28) 3.04 (1.93) CNI-SI 0.37 (0.70) 1.18 (1.38) CNI-D 1.18 (0.69) 1.90 (1.27) CNI Total 2.86 (1.93) 6.14 (3.30) | In schizophrenia patients, cerebellar-prefrontal resting-state functional connectivity was substantially associated with motor coordination deficits and negative symptoms. |
| [77] Hirjak/2019/Germany | HC (n = 37) Patients (n = 37) | 34.08 (11.83) 34.41 (11.00) | Partial remission schizophrenia and schizoaffective disorder | Heidelberg | PANSS PANSS-P 16.03 (8.51) PANSS-N 16.35 (8.02) PANSS-G 35.62 (10.44) PANSS-T 68.00 (22.49) (BPRS) | 15.81 (9.27) mg OLZ | Three measurements resting-state scan T1-weighted three-dimensional magnetization- prepared rapid gradient-echo (3D-MPRAGE) diffusion-tensor imaging | Whole Brain | MC 7.62 (3.73) SI 2.43 (1.44) COMT 3.08 (2.37) RLSPO 2.43 (2.18) HS 2.92 (1.72) | There were no significant differences in age, gender, or years of education between SCHIZO and HC patients. Frontocerebellar and frontoparietal networks correlated negatively with motor coordination scores in patients. |
| [78] Hirjak/2013/Germany | Patients (n = 21) | 22.6 (3.6) | First-episode schizophrenia | Heidelberg | BPRS 24.0 (7.9) SAPS 21.8 (14.8) SANS 29.3 (21.3) | Atypical Antipsychotics 504.8 (327.6) CPZ | 3D T1-weighted images | Brainstem | Total 12.5 (9.7) MC 5.2 (4.5) SI 1.8 (1.5) COMT 1.2 (1.6) RLSPO 1.0 (1.8) HS 2.0 (1.8) | Higher NSS scores, and particularly higher scores on the subscales of motor coordination, complex motor tasks, and hard signs, are correlated with structural modifications of the brainstem, predominantly in the pons and midbrain, rather than to general atrophy of the brainstem as a whole. |
| [79] Herold/2020/Germany | Patients (n = 49) HC (n = 29) | 42.33 (13.93) 48.21 (13.56) | Chronic Subchronic | Heidelberg | 3 RATERS BPRS TOTAL 38.08 (9.66) SAPNS AES 26.67 (11.96) | CPZ 638.37 (569.57) | T1-weighted magnetization prepared rapid gradient echo (MP-RAGE) | Occipital Lobe Frontal Lobe Lingual Gyrus Parahippocampal Gyrus Superior Temporal Gyrus Thalamus Cerebellum | Total NSS 16.90 (12.37) 3.79 (3.29) MC 6.67 (5.60) 1.69 (1.44 SI 2.51 (2.12) 0.52 (0.79) COMT 2.82 (2.51) 0.66 (1.17) RLSPO 3.47 (3.39) 0.48 (0.95) HS 1.61 (1.69) 0.45 (0.74) | No significant associations between CPZ NSS scores. NSS significantly correlated to cerebral volume loss in patients. |
| [80] Cuesta/2021/Spain | Patients (n = 48) HC (n = 23) | 25.7 (5.8) 23.4 (5.9) | first episode | NES | CASH | CPZ mg 413.62 (280.65) | 3D axial T1-weighted sequence shape analysis of subcortical structures | Left and right puta- men Globus pallidus Caudate nucleus Accumbens | NA | First episode (FEP) patients’ CPZ equivalent antipsychotic medication exposure did not exhibit any significant correlations in imaging measures. However, CPZ was found to have a substantial relationship with NES total scores in FEP. Significant shape changes occurred in the right accumbens of FEP patients with high scores on the tremor subscale and in the left caudate of FEP patients with high scores on the NES sensory integration subscale. |
| [81] Hirjak/2015/Germany | Patients (n = 33) | 23.12 (4.24) | Recent-onset schizophrenia | Heidelberg | BPRS 24.57 (10.48) SAPS 20.78 (15.07) SANS 32.3 (21.25) | SAA 489.21 (310.28) mg CPZ | T1-weighted 3D magnetization prepared a rapid gradient echo sequence. (MP-RAGE) local gyrification index (LGI) | Cortex | Total NSS 13.57 (9.13) MC 6.18 (4.57) SI 1.72 (1.37) COMT 1.6 (1.76) RLSPO 1.24 (1.73) HS 1.78 (1.76) | Higher sensory and spatial NSS are negatively associated with LGI alterations in the left precentral gyrus and left precuneus. Higher motor NSS are associated with LGI alterations in the supramarginal gyrus bilaterally, the right superior parietal region, and the left superior temporal gyrus. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrescu, C.; Petrescu, D.M.; Marian, G.; Focseneanu, B.E.; Iliuta, F.P.; Ciobanu, C.A.; Papacocea, S.; Ciobanu, A.M. Neurological Soft Signs in Schizophrenia, a Picture of the Knowledge in the Last Decade: A Scoping Review. Healthcare 2023, 11, 1471. https://doi.org/10.3390/healthcare11101471
Petrescu C, Petrescu DM, Marian G, Focseneanu BE, Iliuta FP, Ciobanu CA, Papacocea S, Ciobanu AM. Neurological Soft Signs in Schizophrenia, a Picture of the Knowledge in the Last Decade: A Scoping Review. Healthcare. 2023; 11(10):1471. https://doi.org/10.3390/healthcare11101471
Chicago/Turabian StylePetrescu, Cristian, Diana M. Petrescu, Gabriela Marian, Brindusa E. Focseneanu, Floris Petru Iliuta, Constantin Alexandru Ciobanu, Serban Papacocea, and Adela M. Ciobanu. 2023. "Neurological Soft Signs in Schizophrenia, a Picture of the Knowledge in the Last Decade: A Scoping Review" Healthcare 11, no. 10: 1471. https://doi.org/10.3390/healthcare11101471