

Influence of Transcranial Direct Current Stimulation and Exercise on Fatigue and Quality of Life in Multiple Sclerosis
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
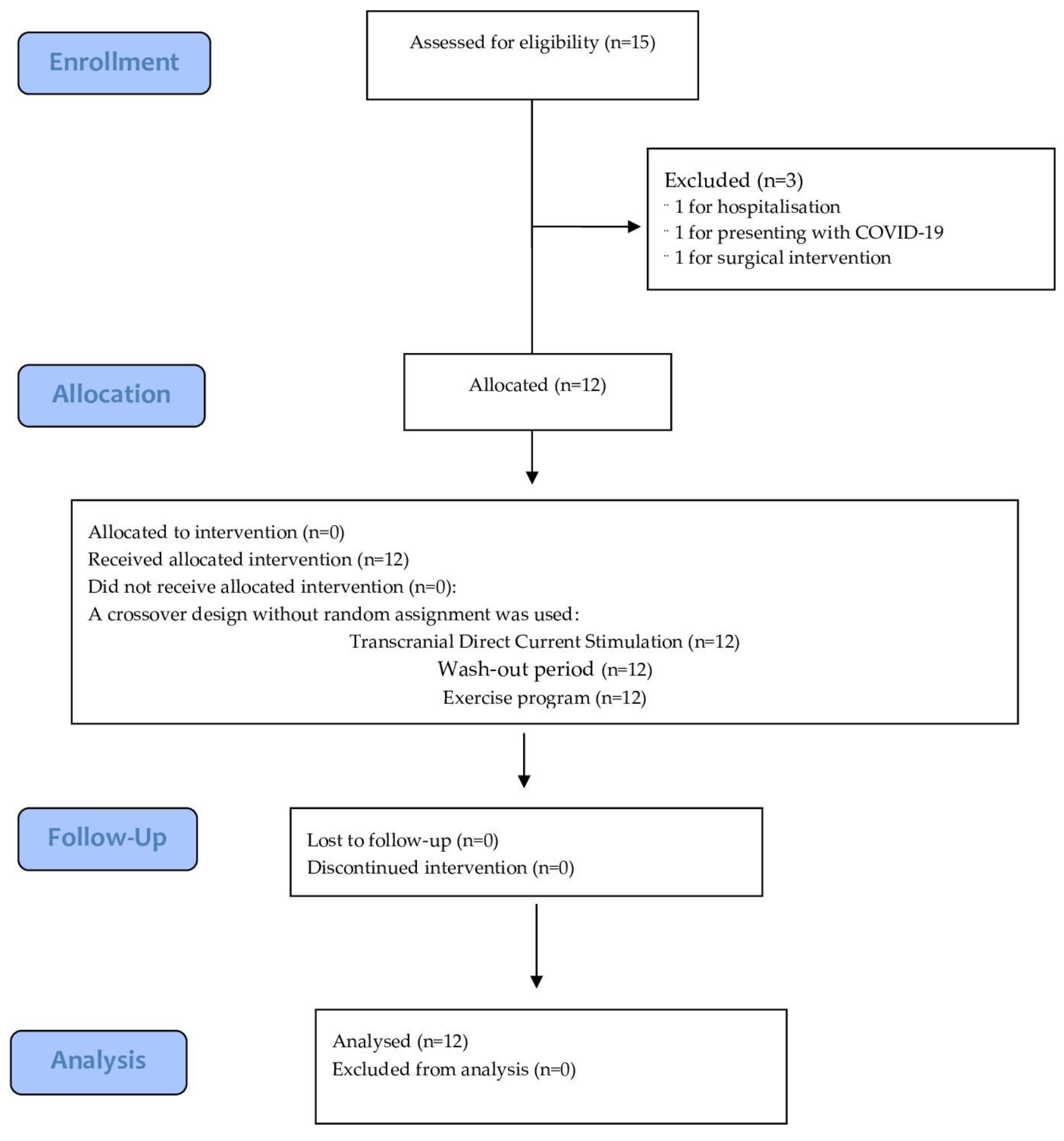
2.1. Study Design
2.2. Participants
2.3. Ethical Considerations
2.4. Interventions
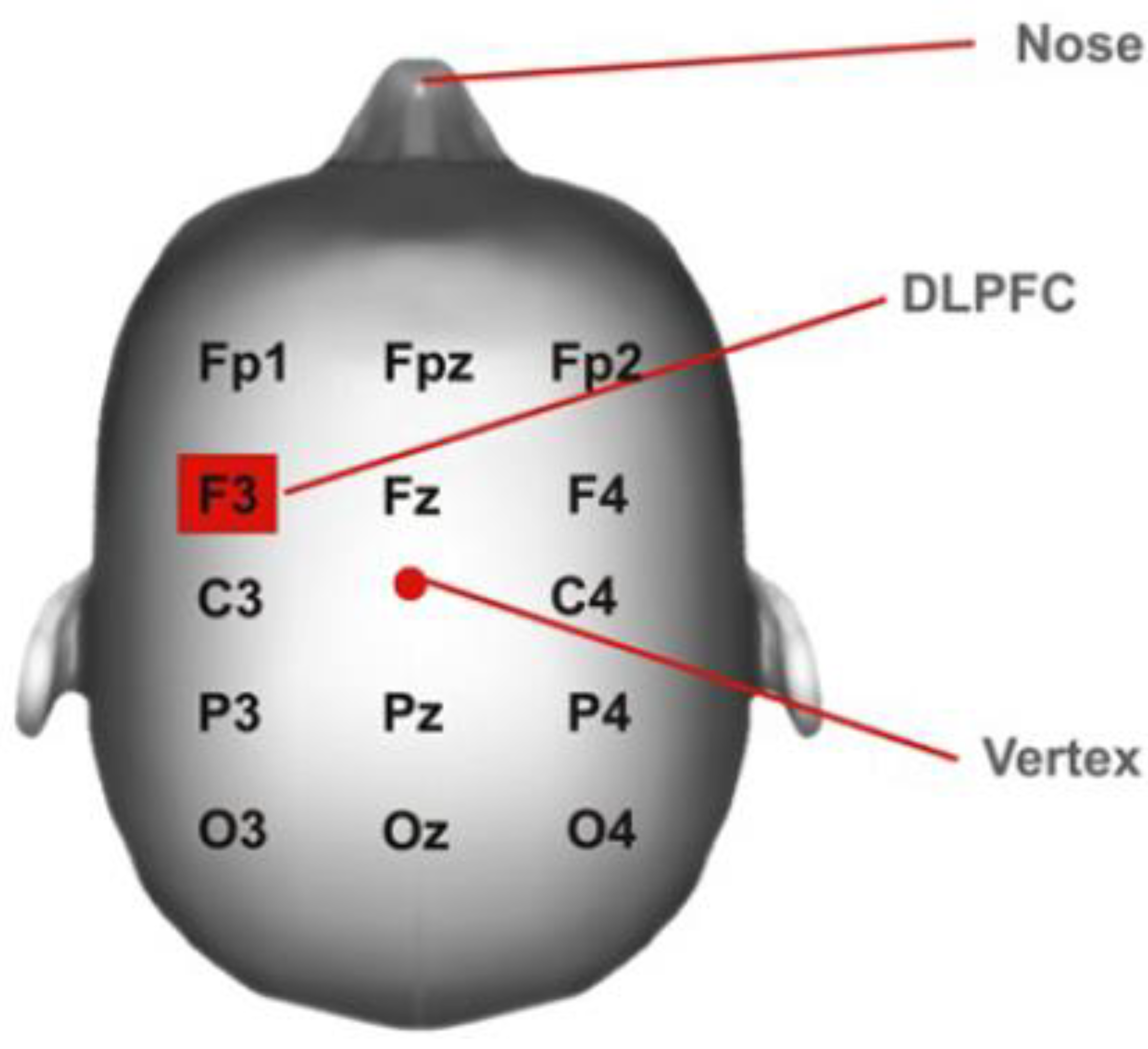
2.4.1. Transcranial Direct Current
2.4.2. Exercise Program
2.5. Outcome Measures
2.6. Procedure
2.7. Statistical Analysis
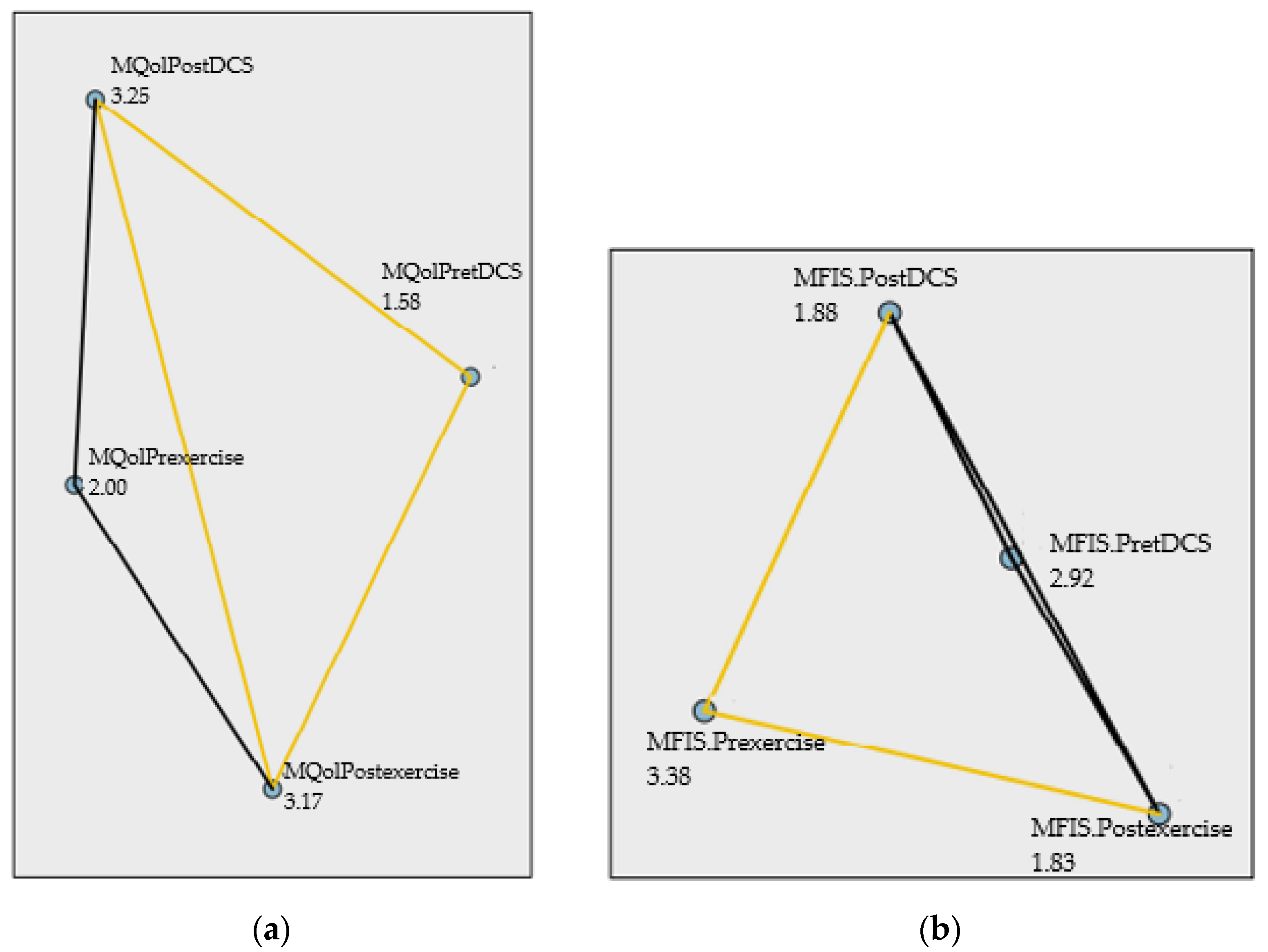
3. Results
4. Discussion
4.1. Practical Application
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Week 1 | Week 2 | Week 3 | Week 4 | |
|---|---|---|---|---|
| Endurance | 1 Session | 2 Sessions | 2 Sessions | 2-3 Sessions |
| 10 min | 15 min | 10 min + 10 min (5 min of rest) | 15 min + 15 min (5 min of rest) | |
| 3–5 RPE | 3–5 RPE | 3–5 RPE | 3–5 RPE | |
| MOTOmed/static bike | MOTOmed/static bike | MOTOmed/static bike | MOTOmed/static bike | |
| Strength | 2 Sessions (A, B) | 2 Sessions (A, B) | 3 Sessions (circuit to choose) | 3 Sessions (circuit to choose) |
| 6 Exercise in each circuit | 6 Exercise in each circuit | 6 Exercise in each circuit | 6 Exercise in each circuit | |
| 15 Rep (rest: 2 min) | 15 Rep (rest: 2 min) | 10 Rep (rest: 3 min) | 10 Rep (rest: 3 min) | |
| 2Circuits (rest: 3 min) | 2 Circuits (rest: 3 min) | 3 Circuits (rest: 5 min) | 3 Circuits (rest: 5 min) |
| Exercise | Circuit A | Circuit B |
|---|---|---|
| MMSS PULL |  |  |
| MMSS PUSH |  |  |
| KNEE EXTENSION |  |  |
| KNEE FLEXION |  |  |
| HIP EXTENSION |  |  |
| HIP FLEXION |  |  |
| CORE |  |  |
References
- Fernández Fernández, Ó.; Arroyo González, R.V.; Rodríguez Antigüedad, A.; García Merino, J.A.; Comabella López, M.; Villar, L.M.; Izquierdo Ayuso, G.; Tintoré Subirana, M.d.M.; Oreja Guevara, C.; Álvarez Cermeño, J.C.; et al. Biomarcadores En Esclerosis Múltiple. Rev. Neurol. 2013, 56, 375. [Google Scholar] [CrossRef]
- Tremlett, H.; Zhao, Y.; Rieckmann, P.; Hutchinson, M. New Perspectives in the Natural History of Multiple Sclerosis. Neurology 2010, 74, 2004–2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abad, P.; Pérez, M.; Castro, E.; Alarcón, T.; Santibáñez, R.; Díaz, F. Prevalence of Multiple Sclerosis in Ecuador. Neurología 2010, 25, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Jordana, A.; Montalban, X. Multiple Sclerosis: Epidemiologic, Clinical, and Therapeutic Aspects. Neuroimaging Clin. N. Am. 2017, 27, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Pilutti, L.A.; Platta, M.E.; Motl, R.W.; Latimer-Cheung, A.E. The Safety of Exercise Training in Multiple Sclerosis: A Systematic Review. J. Neurol. Sci. 2014, 343, 3–7. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Benito-León, J.; González, J.M.M.; Rivera-Navarro, J. Quality of Life and Its Assessment in Multiple Sclerosis: Integrating Physical and Psychological Components of Wellbeing. Lancet Neurol. 2005, 4, 556–566. [Google Scholar] [CrossRef]
- Tallner, A.; Waschbisch, A.; Hentschke, C.; Pfeifer, K.; Mäurer, M. Mental Health in Multiple Sclerosis Patients without Limitation of Physical Function: The Role of Physical Activity. Int. J. Mol. Sci. 2015, 16, 14901–14911. [Google Scholar] [CrossRef] [Green Version]
- Motl, R.W.; Arnett, P.A.; Smith, M.M.; Barwick, F.H.; Ahlstrom, B.; Stover, E.J. Worsening of Symptoms Is Associated with Lower Physical Activity Levels in Individuals with Multiple Sclerosis. Mult. Scler. 2008, 14, 140–142. [Google Scholar] [CrossRef]
- Grazioli, E.; Tranchita, E.; Borriello, G.; Cerulli, C.; Minganti, C.; Parisi, A. The Effects of Concurrent Resistance and Aerobic Exercise Training on Functional Status in Patients with Multiple Sclerosis. Curr. Sports Med. Rep. 2019, 18, 452–457. [Google Scholar] [CrossRef]
- Akcali, A.; Zengin, F.; Aksoy, S.N.; Zengin, O. Fatigue in Multiple Sclerosis: Is It Related to Cytokines and Hypothalamic-Pituitary-Adrenal Axis? Mult. Scler. Relat. Disord. 2017, 15, 37–41. [Google Scholar] [CrossRef]
- Mortezanejad, M.; Ehsani, F.; Masoudian, N.; Zoghi, M.; Jaberzadeh, S. Comparing the Effects of Multi-Session Anodal Trans-Cranial Direct Current Stimulation of Primary Motor and Dorsolateral Prefrontal Cortices on Fatigue and Quality of Life in Patients with Multiple Sclerosis: A Double-Blind, Randomized, Sham-Controlled Trial. Clin. Rehabil. 2020, 34, 1103–1111. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Paredes, I.; Herrero, A.J.; Llamas-Ramos, R.; Rodríguez-Pérez, V.; Seco-Calvo, J. The Effect of Combining Transcranial Direct Current Stimulation Treatment and an Exercise Program on Fragility in a Population with Multiple Sclerosis: Cross-Over Design Trial. Int. J. Environ. Res. Public Health 2022, 19, 12747. [Google Scholar] [CrossRef] [PubMed]
- Kos, D.; Kerckhofs, E.; Carrea, I.; Verza, R.; Ramos, M.; Jansa, J. Evaluation of the Modified Fatigue Impact Scale in Four Different European Countries. Mult. Scler. 2005, 11, 76–80. [Google Scholar] [CrossRef] [PubMed]
- DaSilva, A.F.; Volz, M.S.; Bikson, M.; Fregni, F. Electrode Positioning and Montage in Transcranial Direct Current Stimulation. J. Vis. Exp. 2011, 51, e2744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heine, M.; van de Port, I.; Rietberg, M.B.; van Wegen, E.E.; Kwakkel, G. Exercise Therapy for Fatigue in Multiple Sclerosis. Cochrane Database Syst. Rev. 2015, 9, CD009956. [Google Scholar] [CrossRef]
- Latimer-Cheung, A.E.; Pilutti, L.A.; Hicks, A.L.; Martin Ginis, K.A.; Fenuta, A.M.; MacKibbon, K.A.; Motl, R.W. Effects of Exercise Training on Fitness, Mobility, Fatigue, and Health-Related Quality of Life among Adults with Multiple Sclerosis: A Systematic Review to Inform Guideline Development. Arch. Phys. Med. Rehabil. 2013, 94, 1800–1828.e3. [Google Scholar] [CrossRef]
- White, L.J.; McCoy, S.C.; Castellano, V.; Gutierrez, G.; Stevens, J.E.; Walter, G.A.; Vandenborne, K. Resistance Training Improves Strength and Functional Capacity in Persons with Multiple Sclerosis. Mult. Scler. 2004, 10, 668–674. [Google Scholar] [CrossRef]
- Dalgas, U.; Stenager, E.; Ingemann-Hansen, I. Multiple Sclerosis and Physical Exercise: Recommendations for the Application of Resistance-, Endurance- and Combined Training. Mult. Scler. 2008, 14, 35–53. [Google Scholar] [CrossRef]
- Halabchi, F.; Alizadeh, Z.; Sahraian, M.A.; Abolhasani, M. Exercise Prescription for Patients with Multiple Sclerosis; Potential Benefits and Practical Recommendations. BMC Neurol. 2017, 17, 185. [Google Scholar] [CrossRef] [Green Version]
- Simeoni, M.C.; Auquier, P.; Fernandez, O.; Flachenecker, P.; Stecchi, S.; Constantinescu, C.S.; Idiman, E.; Boyko, A.; Beiske, A.G.; Vollmer, T.; et al. Validation of the Multiple Sclerosis International Quality of Life Questionnaire. Mult. Scler. 2008, 14, 219–230. [Google Scholar] [CrossRef]
- Fernández, O.; Fernández, V.; Baumstarck-Barrau, K.; Muñoz, L.; Gonzalez Alvarez, M.D.M.; Arrabal, J.C.; León, A.; Alonso, A.; López-Madrona, J.C.; Bustamante, R.; et al. Validation of the Spanish Version of the Multiple Sclerosis International Quality of Life (Musiqol) Questionnaire. BMC Neurol. 2011, 11, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gosney, J.L.; Scott, J.A.; Snook, E.M.; Motl, R.W. Physical Activity and Multiple Sclerosis: Validity of Self-Report and Objective Measures. Fam. Community Health 2007, 30, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hobart, J.; Freeman, J.; Thompson, A. Kurtzke Scales Revisited: The Application of Psychometric Methods to Clinical Intuition. Brain 2000, 123, 1027–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer-Moock, S.; Feng, Y.S.; Maeurer, M.; Dippel, F.W.; Kohlmann, T. Systematic Literature Review and Validity Evaluation of the Expanded Disability Status Scale (EDSS) and the Multiple Sclerosis Functional Composite (MSFC) in Patients with Multiple Sclerosis. BMC Neurol. 2014, 14, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Learmonth, Y.C.; Dlugonski, D.; Pilutti, L.A.; Sandroff, B.M.; Klaren, R.; Motl, R.W. Psychometric Properties of the Fatigue Severity Scale and the Modified Fatigue Impact Scale. J. Neurol. Sci. 2013, 331, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Ferruci, R.; Vergari, M.; Cogiamanian, F.; Bocci, T.; Ciocca, M.; Tomasini, E.; De Riz, M.; Scarpin, E.; Priori, A. Transcranial Direct Current Stimulation (TDCS) for Fatigue in Multiple Sclerosis. NeuroRehabilitation 2014, 34, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Associated, L.E., Ed.; Elsevier Science: Morristown, NJ, USA, 1988; ISBN 9781483276489. [Google Scholar]
- Olascoaga, J. Quality of Life and Multiple Sclerosis. Rev. Neurol. 2010, 51, 279–288. [Google Scholar] [CrossRef]
- Brenner, P.; Piehl, F. Fatigue and Depression in Multiple Sclerosis: Pharmacological and Non-Pharmacological Interventions. Acta Neurol. Scand. 2016, 134, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Benito-León, J.; Morales, J.M.; Rivera-Navarro, J.; Mitchell, A.J. A Review about the Impact of Multiple Sclerosis on Health-Related Quality of Life. Disabil. Rehabil. 2003, 25, 1291–1303. [Google Scholar] [CrossRef]
- Ayache, S.S.; Chalah, M.A. Fatigue and Affective Manifestations in Multiple Sclerosis—A Cluster Approach. Brain Sci. 2019, 10, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayache, S.S.; Chalah, M.A. Fatigue in Multiple Sclerosis–Insights into Evaluation and Management. Neurophysiol. Clin. 2017, 47, 139–171. [Google Scholar] [CrossRef] [PubMed]
- Ayache, S.S.; Chalah, M.A. Fatigue in Multiple Sclerosis: Pathophysiology and Emergent Interventions. Arch. Ital. Biol. 2018, 156, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Dalgas, U.; Stenager, E. Exercise and Disease Progression in Multiple Sclerosis: Can Exercise Slow down the Progression of Multiple Sclerosis? Ther. Adv. Neurol. Disord. 2012, 5, 81–95. [Google Scholar] [CrossRef] [Green Version]
- Tallner, A.; Waschbisch, A.; Wenny, I.; Schwab, S.; Hentschke, C.; Pfeifer, K.; Mäurer, M. Multiple Sclerosis Relapses Are Not Associated with Exercise. Mult. Scler. J. 2012, 18, 232–235. [Google Scholar] [CrossRef] [Green Version]
- Alpa, P.; Leslie, B.; Anusila, D.; Heather, F.; Peter, C.; Susan, G.; Graham, C.; Michael, T. Leisure Time Spent Sitting in Relation to Total Mortality in a Prospective Cohort of US Adults. Am. J. Epidemiol. 2010, 172, 419–429. [Google Scholar] [CrossRef] [Green Version]
- Cavanaugh, J.; Gappmaier, V.; Dibble, L.; Gappmaier, E. Ambulatory Activity in Individuals with Multiple Sclerosis. J. Neurol. Phys. Ther. 2011, 35, 26–33. [Google Scholar] [CrossRef]
- Owen, N. Sedentary Behavior: Understanding and Influencing Adults’ Prolonged Sitting Time. Prev. Med. 2012, 55, 535–539. [Google Scholar] [CrossRef]
- Tarakci, E.; Yeldan, I.; Huseyinsinoglu, B.; Zenginler, Y.; Eraksoy, M. Group Exercise Training for Balance, Functional Status, Spasticity, Fatigue and Quality of Life in Multiple Sclerosis: A Randomized Controlled Trial. Clin. Rehabil. 2013, 27, 813–822. [Google Scholar] [CrossRef]
- Aydin, T.; Taşpinar, Ö.; Sariyildiz, M.A.; Güneşer, M.; Keskin, Y.; Canbaz, N.; Gök, M.; Camli, A.; Kiziltan, H.; Eris, A.H. Evaluation of the Effectiveness of Home Based or Hospital Based Calisthenic Exercises in Patients with Ankylosing Spondylitis. J. Back Musculoskelet. Rehabil. 2016, 29, 723–730. [Google Scholar] [CrossRef]
- Cancelli, A.; Cottone, C.; Giordani, A.; Migliore, S.; Lupoi, D.; Porcaro, C.; Mirabella, M.; Rossini, P.M.; Filippi, M.M.; Tecchio, F. Personalized, Bilateral Whole-Body Somatosensory Cortex Stimulation to Relieve Fatigue in Multiple Sclerosis. Mult. Scler. 2018, 24, 1366–1374. [Google Scholar] [CrossRef] [PubMed]
- Chalah, M.A.; Riachi, N.; Ahdab, R.; Mhalla, A.; Abdellaoui, M.; Créange, A.; Lefaucheur, J.P.; Ayache, S.S. Effects of Left DLPFC versus Right PPC TDCS on Multiple Sclerosis Fatigue. J. Neurol. Sci. 2017, 372, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Chalah, M.A.; Grigorescu, C.; Padberg, F.; Kümpfel, T.; Palm, U.; Ayache, S.S. Bifrontal Transcranial Direct Current Stimulation Modulates Fatigue in Multiple Sclerosis: A Randomized Sham-Controlled Study. J. Neural Transm. 2020, 127, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Palm, U.; Chalah, M.; Padberg, F.; Al-Ani, T.; Abdellaoui, M.; Sorel, M.; Dimitri, D.; Créange, A.; Lefaucheur, J.; SS, A. Effects of Transcranial Random Noise Stimulation (TRNS) on Affect, Pain and Attention in Multiple Sclerosis. Restor. Neurol. Neurosci. 2016, 34, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Pilloni, G.; Choi, C.; Shaw, M.T.; Coghe, G.; Krupp, L.; Moffat, M.; Cocco, E.; Pau, M.; Charvet, L. Walking in Multiple Sclerosis Improves with TDCS: A Randomized, Double-Blind, Sham-Controlled Study. Ann. Clin. Transl. Neurol. 2020, 7, 2310–2319. [Google Scholar] [CrossRef] [PubMed]



| VARIABLES | N [MIN–MAX]; MEAN ± (SD) | FREQUENCY (%) |
|---|---|---|
| Age | 12 [35–66]; 48.08 ± 8.55 | |
| Years of diagnosis | 12 [0.8–28]; 16.65 ± 7.44 | |
| Outbreaks per year | 11 [0–2]; 0.36 ± 0.67 | |
| Walking time (minutes) | 9 [0.0–120]; 51.11 ± 41.06 | |
| Sitting time (minutes) | 9 [0–960]; 466.667 ± 304.13 | |
| Type of sclerosis | ||
| Relapsing–remitting Progressive secondary | 7 (58.3%) | |
| 5 (41.7%) | ||
| Outbreak intensity | ||
| Mild Moderate Intense No outbreaks | 2 (18.2%) | |
| 1 (9.1%) | ||
| 1 (9.1%) | ||
| 7 (63.6%) | ||
| Medical recommendation | ||
| Physical activity | 6 (11.3%) | |
| Other | 1 (8.3%) | |
| No recommendation | 5 (41.7%) | |
| Fatigue medication | ||
| Yes No | 5 (41.7%) | |
| 7 (58.3%) | ||
| Type of medication fatigue | ||
| LioresalLioresal + Avonex Lioresal + Rebif 44 Other medication No medication | 1 (9.1%) | |
| 1 (9.1%) | ||
| 1 (9.1%) | ||
| 2 (16.7%) | ||
| 7 (58.3%) | ||
| Rehabilitation | ||
| Yes | 11 (91.7%) | |
| No | 1 (8.3%) | |
| Intensity rehabilitation | ||
| Occasional | 5 (41.7%) | |
| Periodic | 7 (58.3%) | |
| Exercise habits | ||
| Occasional Regularly | 2 (16.7%) | |
| 10 (83.3%) | ||
| Education level | ||
| Primary education Secondary studies Vocational training University studies | 1 (8.3%) | |
| 1 (8.3%) | ||
| 6 (50%) | ||
| 4 (33.3%) | ||
| Employment situation | ||
| Homemaker Part-time employee Full-time employee Retired Permanently disabled | 1 (8.3%) | |
| 1 (8.3%) | ||
| 5 (41.7%) | ||
| 3 (25%) | ||
| 2 (16.7%) | ||
| Pre tDCS Median [Range] | Post tDCS Median [Range] | p | Size Effect Hedges’ g | Pre-Exercise Median [Range] | Post-Exercise Median [Range] | p | Size Effect Hedges’ g | |
|---|---|---|---|---|---|---|---|---|
| MQOL | 68.04 [25.28] | 75.19 [32.23] | 0.015 * | 0.646 | 70.07 [28.99] | 74.94 [27.2] | 0.003 ** | 0.56 |
| MQOLADL | 58.9 [6.25] | 64.80 [6.55] | 0.037 * | 0.465 | 57.73 [1.5] | 68.09 [6.95] | 0.003 ** | 0.570 |
| MQOLPWB | 66.24 [3] | 80.42 [6.82] | 0.004 ** | 0.727 | 65 [2] | 72.5 [4.33] | 0.41 * | 0.417 |
| MQOLSYM | 72.5 [4] | 77.5 [5.8] | 0.438 | 0.258 | 72.5 [6.17] | 74.58 [4.42] | 0.625 | 0.122 |
| MQOLSOREL | 76.93 [4.88] | 78.31 [5.92] | 0.413 | 0.055 | 84.98 [2] | 87.2 [3.67] | 0.336 | 0.120 |
| MQOLRFAREL | 81.65 [6.25] | 83.32 [3.92] | 0.44 | 0.066 | 88.88 [2.3] | 90.53 [3.4] | 0.102 | 0.104 |
| MQOLSEXLIFE | 73.75 [5] | 75 [3.25] | 0.865 | 0.045 | 73.33 [2] | 77.5 [2.67] | 0.257 | 0.129 |
| MQOLCOP | 50.83 [3] | 61.67 [5.25] | 0.018 * | 0.376 | 51.67 [5.75] | 56.66 [4.79] | 0.177 | 0.266 |
| MQOLREJEC | 68.33 [3] | 79.17 [6] | 0.103 | 0.475 | 75 [3.5] | 80 [4.08] | 0.058 | 0.221 |
| MQOLREHEALTH | 79.41 [3.38] | 78.88 [4.83] | 0.933 | 0.036 | 78.87 [2.3] | 82.07 [2.67] | 0.269 | 0.152 |
| MFIS | 39.5 [31] | 38.5 [45] | 0.028 * | 0.525 | 43 [33] | 36 [52] | 0.003 ** | 0.742 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Paredes, I.; Herrero, A.J.; Román-Nieto, N.; Peña-Gomez, A.M.; Seco-Calvo, J. Influence of Transcranial Direct Current Stimulation and Exercise on Fatigue and Quality of Life in Multiple Sclerosis. Healthcare 2023, 11, 84. https://doi.org/10.3390/healthcare11010084
Muñoz-Paredes I, Herrero AJ, Román-Nieto N, Peña-Gomez AM, Seco-Calvo J. Influence of Transcranial Direct Current Stimulation and Exercise on Fatigue and Quality of Life in Multiple Sclerosis. Healthcare. 2023; 11(1):84. https://doi.org/10.3390/healthcare11010084
Chicago/Turabian StyleMuñoz-Paredes, Inés, Azael J. Herrero, Natalia Román-Nieto, Alba M. Peña-Gomez, and Jesús Seco-Calvo. 2023. "Influence of Transcranial Direct Current Stimulation and Exercise on Fatigue and Quality of Life in Multiple Sclerosis" Healthcare 11, no. 1: 84. https://doi.org/10.3390/healthcare11010084