
Septoplasty Effect on the Enhancement of Airflow Distribution and Particle Deposition in Nasal Cavity: A Numerical Study


Abstract
:1. Introduction
2. Methodology
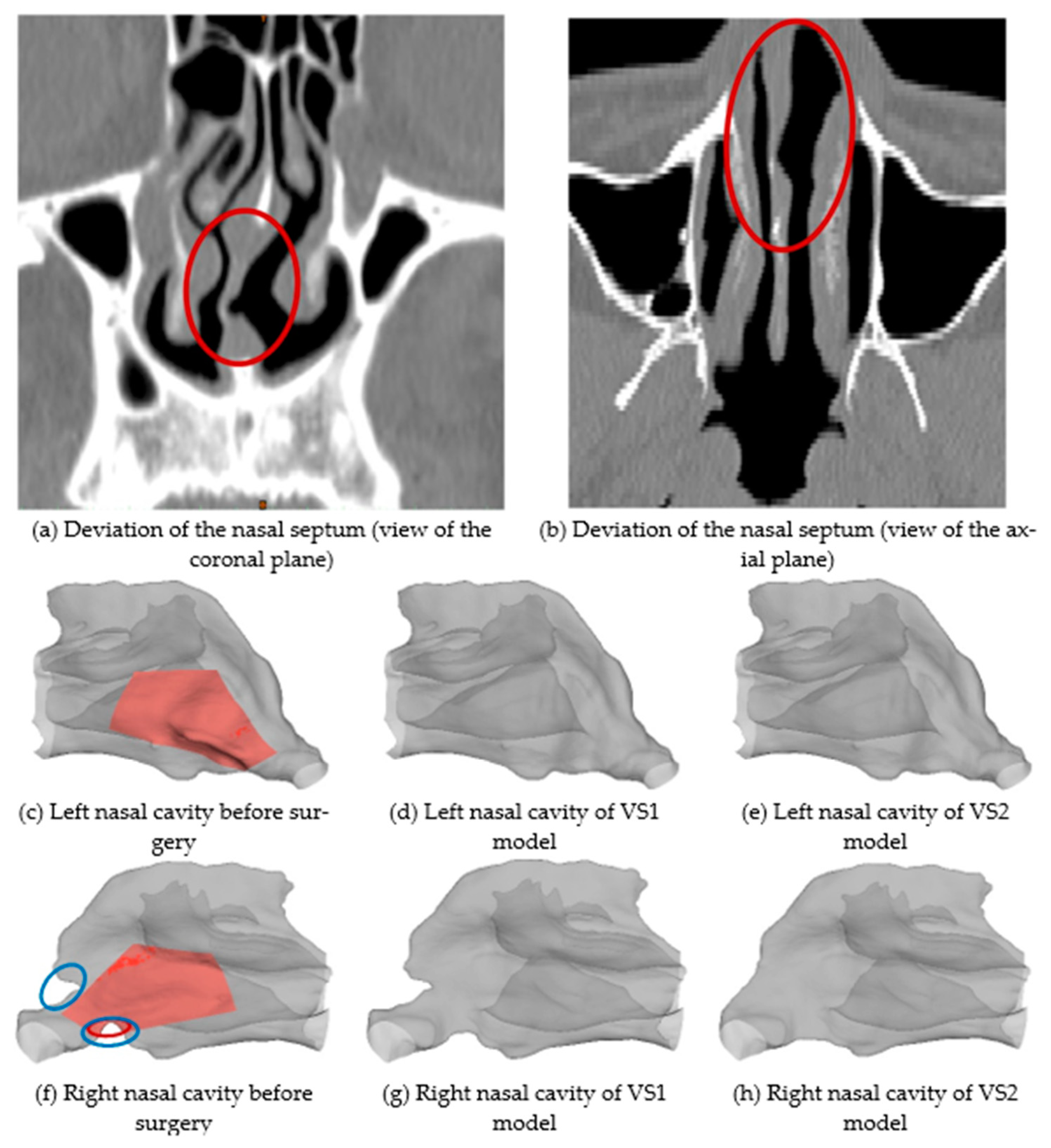
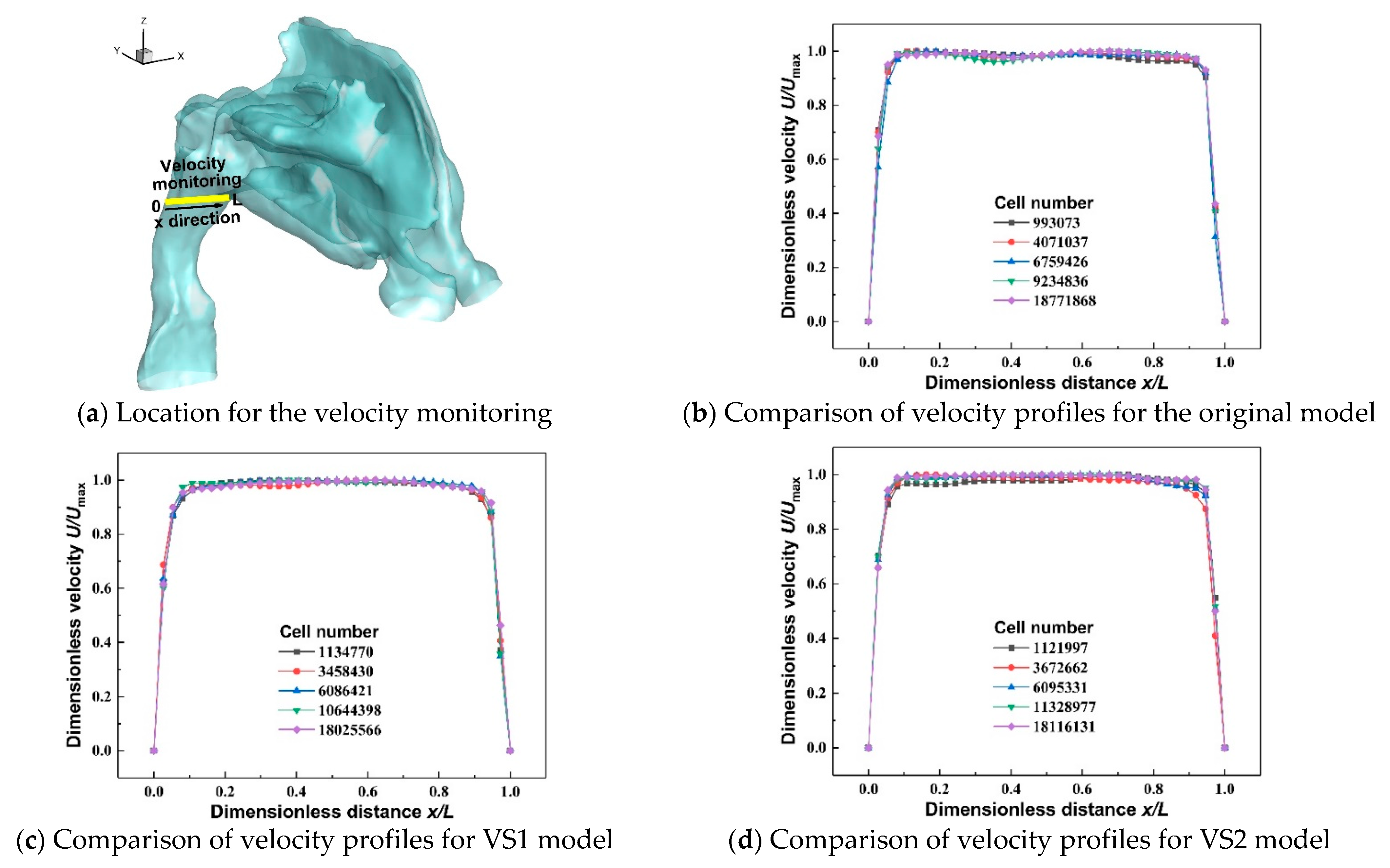
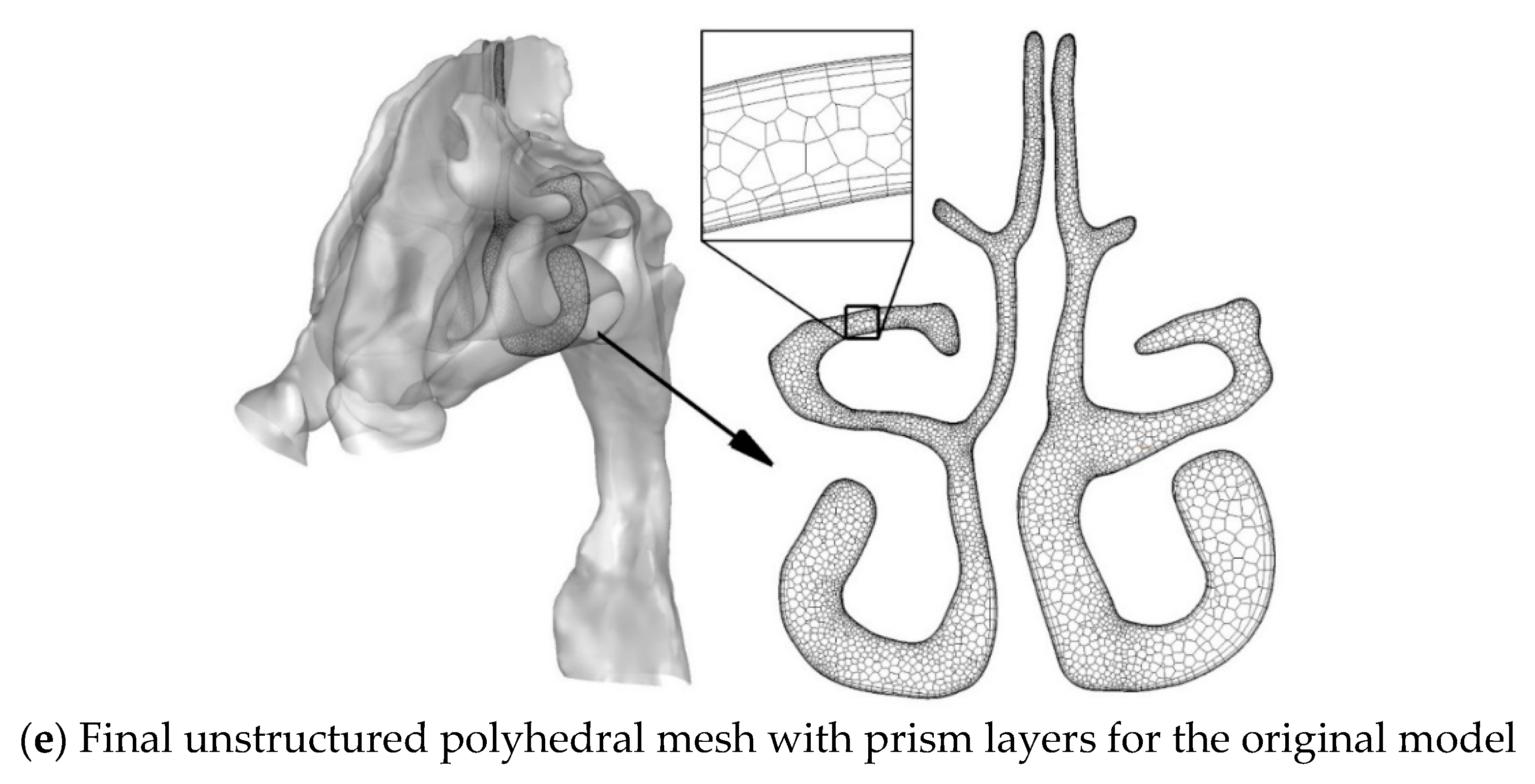
2.1. Nasal Cavity Geometries and Meshes
2.2. Governing Equations
2.2.1. Continuous Airflow Phase
2.2.2. Discrete Particle Phase
2.3. Numerical Setup
2.4. Validation of Model
3. Results and Discussion
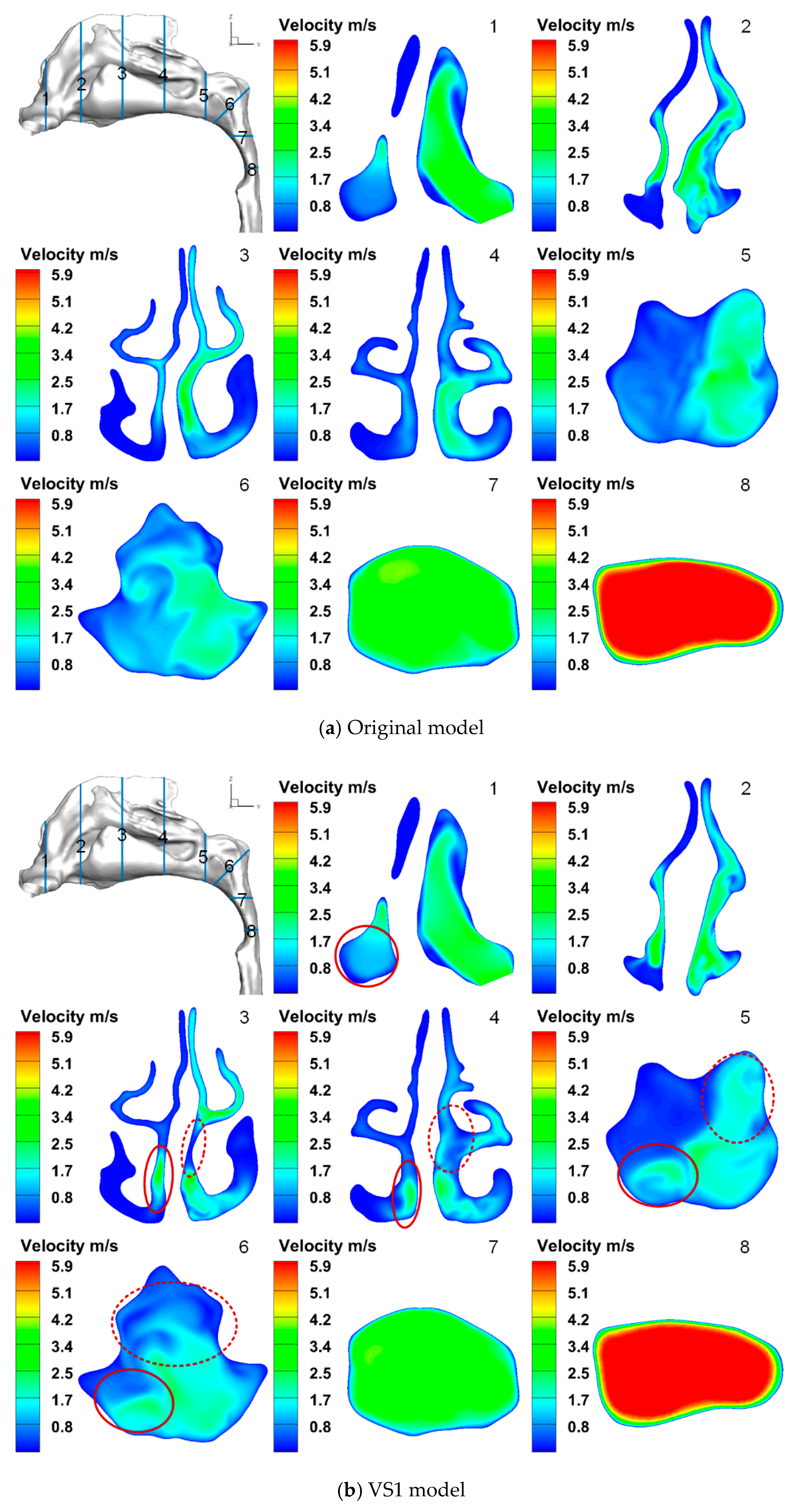
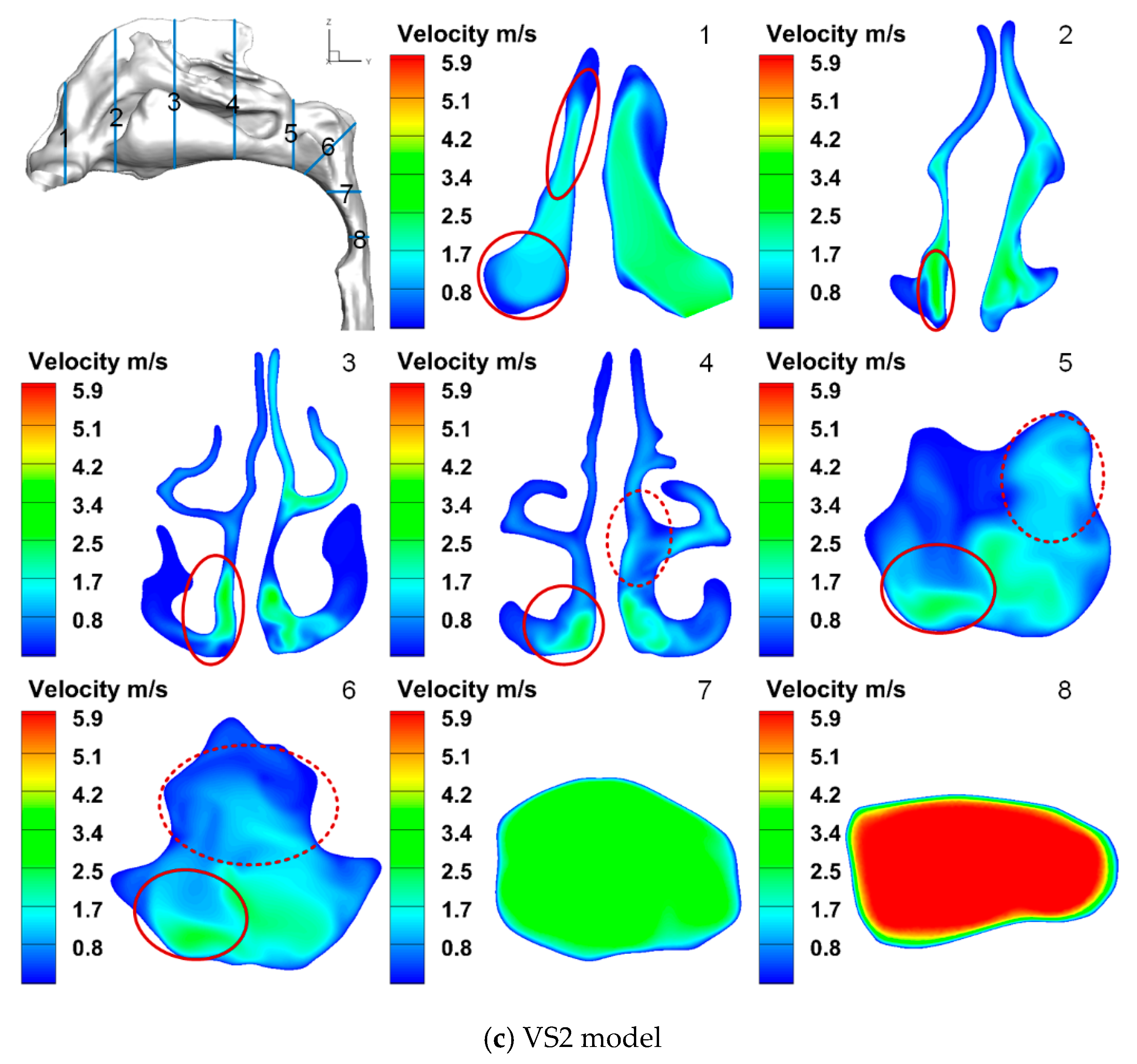
3.1. Airflow Characteristics
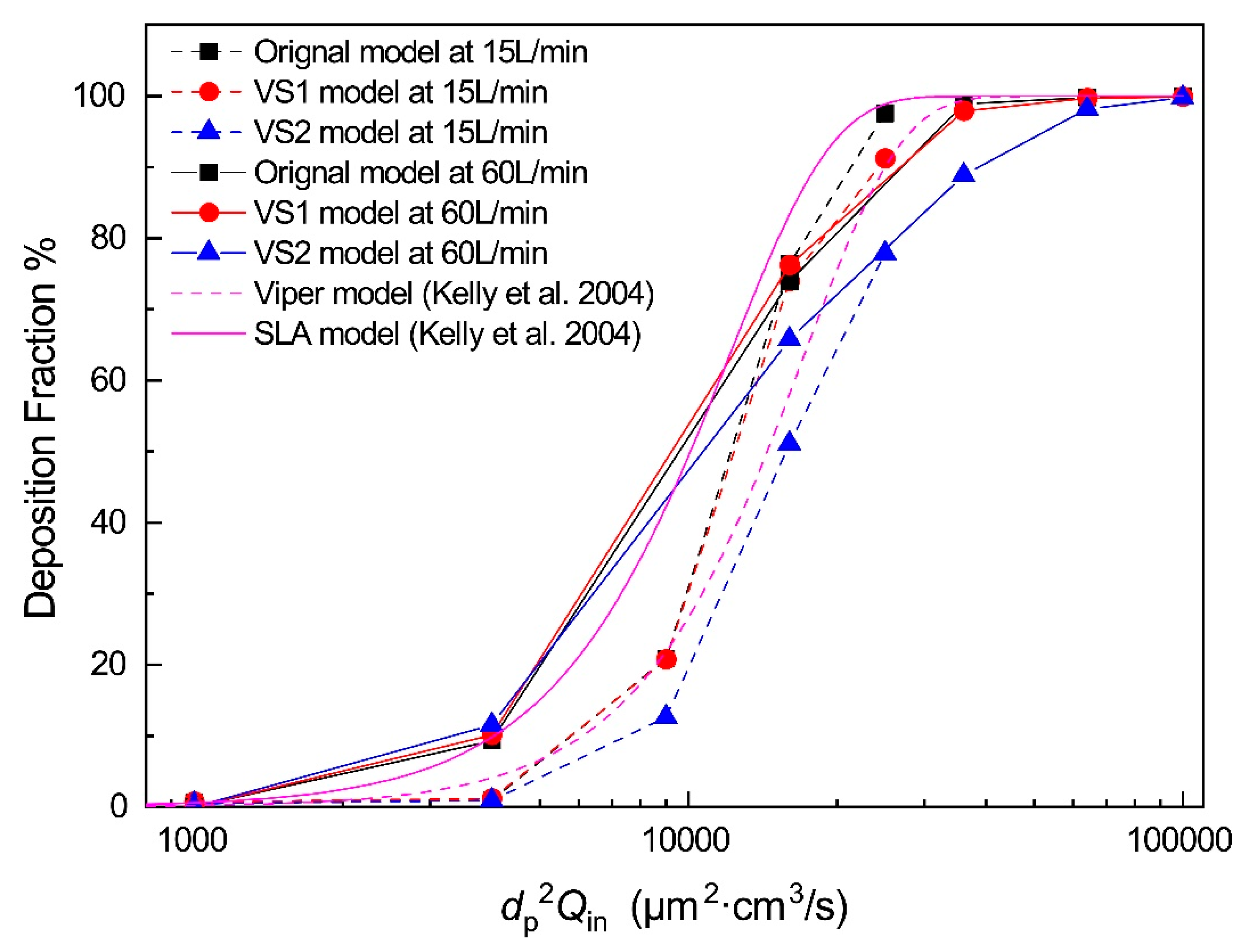
3.2. Particle Deposition Fractions (DFs)
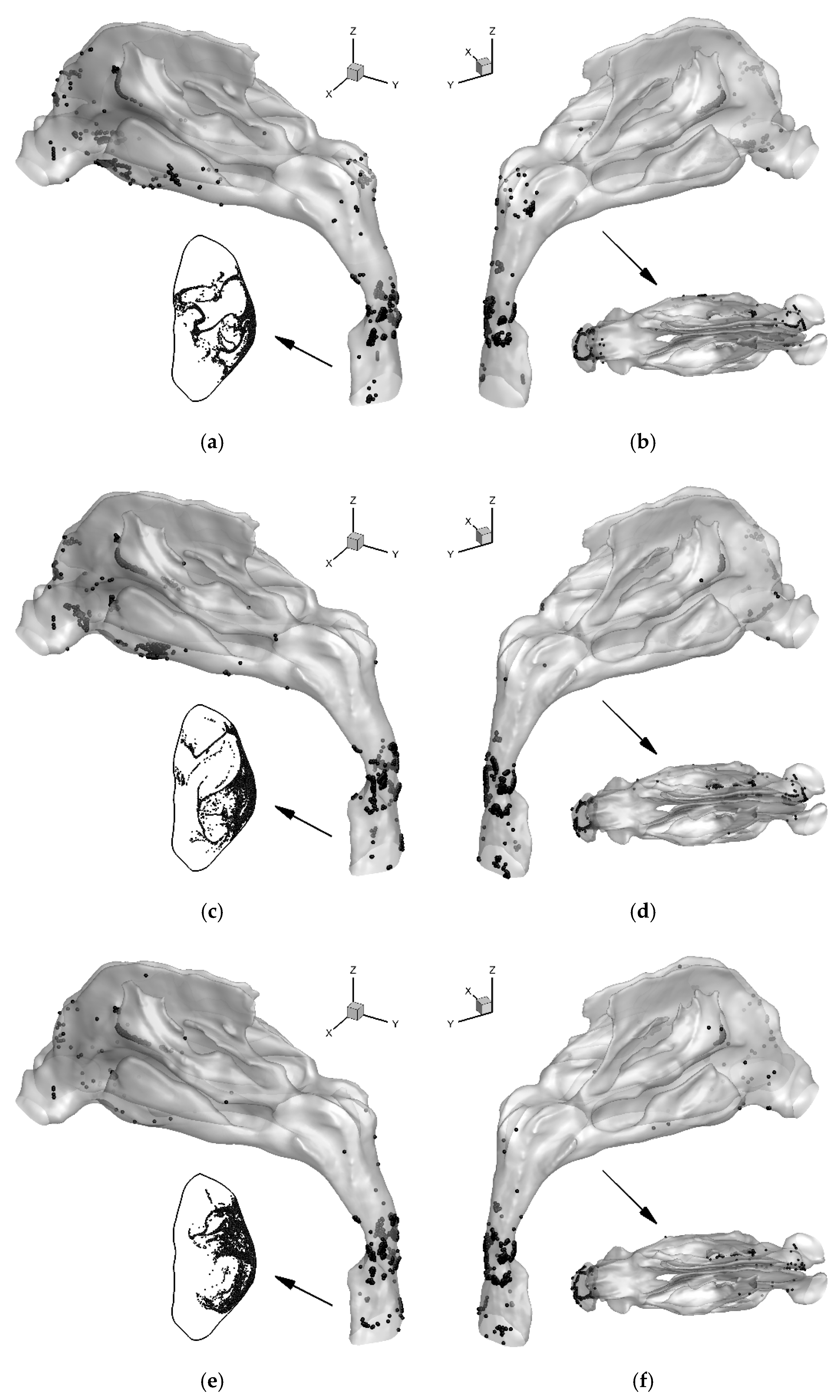
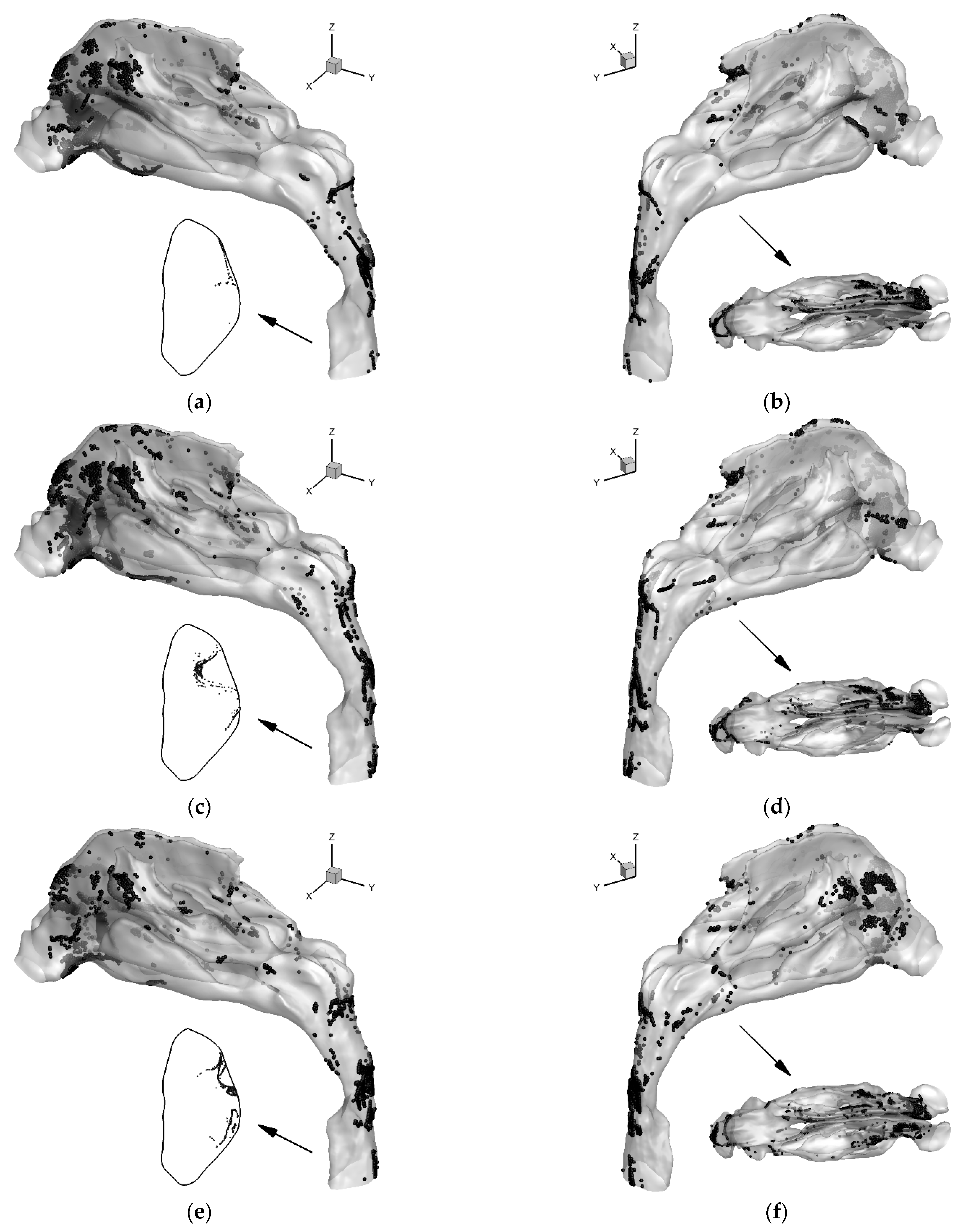
3.3. Localized Deposition Patterns
4. Conclusions
- The CFD simulation combined with virtual surgery can help to evaluate the surgical plans for septum deviation and predict the airflow allocation between the two sides of the nasal cavity.
- Corrections of the obstruction in the nasal vestibule and caudal nasal septal deviation are important, beyond the correction of deviated deep areas of septal cartilage and bone. They can enhance the ratio of the inhalation flow rate of one side by up to 17%.
- The better virtual surgical plan for the septum deviation, i.e., the VS2 model in this study, not only improves the airflow distribution, but also significantly reduces particle deposition in the nasal cavity.
- For the septum deviation, the better virtual surgical plan reduces the particle deposition on the convex side, but slightly increases the deposition on the concave side. This may reduce the possibility of nasal diseases.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Nomenclature
| drag force coefficient for aerosol | |
| cross-diffusion term | |
| modified term for destruction of turbulence kinetic energy | |
| dissipation of ω | |
| particle diameter | |
| gravitational acceleration | |
| k | turbulence kinetic energy |
| mp | mass of the particle |
| production of turbulence kinetic energy | |
| , | transition source terms |
| , | transition destruction terms |
| modified term of with intermittency | |
| source term for transition momentum thickness Reynolds number | |
| air pressure | |
| transport scalar for momentum thickness Reynolds number | |
| time | |
| fluid velocity | |
| velocity vector of the particle | |
| Greek | |
| intermittency | |
| dynamic viscosity of the fluid | |
| turbulent viscosity | |
| kinematic viscosity of the fluid | |
| turbulent eddy viscosity | |
| ρ | fluid density |
| turbulent Prandtl number for k | |
| turbulent Prandtl number for ω | |
| constant | |
| ω | specific dissipation rate |
References
- Stewart, M.G.; Witsell, D.L.; Smith, T.L.; Weaver, E.M.; Yueh, B.; Hannley, M.T. Development and validation of the Nasal Obstruction Symptom Evaluation (NOSE) scale. Otolaryngol.—Head Neck Surg. 2004, 130, 157–163. [Google Scholar] [CrossRef]
- Schaitkin, B.; Strauss, M.; Houck, J.R. Epistaxis: Medical versus surgical therapy: A comparison of efficacy, complications, and economic considerations. Laryngoscope 1987, 97, 1392–1396. [Google Scholar] [CrossRef] [PubMed]
- Tosun, F.; Gerek, M.; Özkaptan, Y. Nasal surgery for contact point headaches. Headache J. Head Face Pain 2000, 40, 237–240. [Google Scholar] [CrossRef]
- Liu, T.; Han, D.; Wang, J.; Tan, J.; Zang, H.; Wang, T.; Li, Y.; Cui, S. Effects of septal deviation on the airflow characteristics: Using computational fluid dynamics models. Acta Oto-Laryngol. 2012, 132, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Dawson, W.W. Chemical stimulation of the peripheral trigeminal nerve. Nature 1962, 196, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Abu-Bakra, M.; Jones, N. Prevalence of nasal mucosal contact points in patients with facial pain compared with patients without facial pain. J. Laryngol. Otol. 2001, 115, 629–632. [Google Scholar] [CrossRef] [PubMed]
- Huizing, E.H.; de Groot, J.A.M. Functional Reconstructive Nasal Surgery; Thieme: New York, NY, USA, 2003; Available online: https://books.google.com/books?id=q0DtCGQINq8C (accessed on 8 May 2022).
- Tomkinson, A.; Eccles, R. Comparison of the relative abilities of acoustic rhinometry, rhinomanometry, and the visual analogue scale in detecting change in the nasal cavity in a healthy adult population. Am. J. Rhinol. 1996, 10, 161–166. [Google Scholar] [CrossRef]
- Hilberg, O.; Jackson, A.; Swift, D.; Pedersen, O. Acoustic rhinometry: Evaluation of nasal cavity geometry by acoustic reflection. J. Appl. Physiol. 1989, 66, 295–303. [Google Scholar] [CrossRef]
- Doty, R.L.; Deems, D.A.; Frye, R.E.; Pelberg, R.; Shapiro, A. Olfactory sensitivity, nasal resistance, and autonomic function in patients with multiple chemical sensitivities. Arch. Otolaryngol.–Head Neck Surg. 1988, 114, 1422–1427. [Google Scholar] [CrossRef]
- Ho, W.; Yuen, A.P.; Tang, K.; Wei, W.I.; Lam, P.K. Time course in the relief of nasal blockage after septal and turbinate surgery: A prospective study. Arch. Otolaryngol.–Head Neck Surg. 2004, 130, 324–328. [Google Scholar] [CrossRef] [Green Version]
- Roblin, D.; Eccles, R. What, if any, is the value of septal surgery? Clin. Otolaryngol. Allied Sci. 2002, 27, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, R.; Miyazaki, S.; Karaki, M.; Kobayashi, E.; Karaki, R.; Akiyama, K.; Matsubara, A.; Mori, N. Measurement of nasal resistance by rhinomanometry in 892 Japanese elementary school children. Auris Nasus Larynx 2011, 38, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, W. The Handicapped Nose Breathing, 1st ed.; ATMOS MedizinTechnik GmbH & Co. KG: Bengaluru, India, 2000. [Google Scholar]
- Rhee, J.S.; Pawar, S.S.; Garcia, G.J.; Kimbell, J.S. Toward personalized nasal surgery using computational fluid dynamics. Arch. Facial Plast. Surg. 2011, 13, 305–310. [Google Scholar] [CrossRef]
- Zhao, K.; Malhotra, P.; Rosen, D.; Dalton, P.; Pribitkin, E.A. Computational fluid dynamics as surgical planning tool: A pilot study on middle turbinate resection. Anat. Rec. 2014, 297, 2187–2195. [Google Scholar] [CrossRef] [PubMed]
- Hariri, B.M.; Rhee, J.S.; Garcia, G.J. Identifying patients who may benefit from inferior turbinate reduction using computer simulations. Laryngoscope 2015, 125, 2635–2641. [Google Scholar] [CrossRef] [PubMed]
- Vanhille, D.L.; Garcia, G.J.; Asan, O.; Borojeni, A.A.; Frank-Ito, D.O.; Kimbell, J.S.; Pawar, S.S.; Rhee, J.S. Virtual surgery for the nasal airway: A preliminary report on decision support and technology acceptance. JAMA Facial Plast. Surg. 2018, 20, 63–69. [Google Scholar] [CrossRef]
- Kelly, J.T.; Asgharian, B.; Kimbell, J.S.; Wong, B.A. Particle deposition in human nasal airway replicas manufactured by different methods. Part I: Inertial regime particles. Aerosol Sci. Technol. 2004, 38, 1063–1071. [Google Scholar] [CrossRef]
- Schroeter, J.D.; Garcia, G.J.; Kimbell, J.S. Effects of surface smoothness on inertial particle deposition in human nasal models. J. Aerosol Sci. 2011, 42, 52–63. [Google Scholar] [CrossRef]
- Storey-Bishoff, J.; Noga, M.; Finlay, W. Deposition of micrometer-sized aerosol particles in infant nasal airway replicas. J. Aerosol Sci. 2008, 39, 1055–1065. [Google Scholar] [CrossRef]
- Golshahi, L.; Finlay, W.; Olfert, J.; Thompson, R.; Noga, M. Deposition of inhaled ultrafine aerosols in replicas of nasal airways of infants. Aerosol Sci. Technol. 2010, 44, 741–752. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Matida, E.A.; Johnson, M.R. Experimental measurements and computational modeling of aerosol deposition in the Carleton-Civic standardized human nasal cavity. J. Aerosol Sci. 2010, 41, 569–586. [Google Scholar] [CrossRef]
- Farkas, D.; Hindle, M.; Longest, P.W. Application of an inline dry powder inhaler to deliver high dose pharmaceutical aerosols during low flow nasal cannula therapy. Int. J. Pharm. 2018, 546, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Golshahi, L.; Walenga, R.L.; Longest, P.W.; Hindle, M. Development of a transient flow aerosol mixer-heater system for lung delivery of nasally administered aerosols using a nasal cannula. Aerosol Sci. Technol. 2014, 48, 1009–1021. [Google Scholar] [CrossRef]
- Longest, P.W.; Tian, G.; Hindle, M. Improving the lung delivery of nasally administered aerosols during noninvasive ventilation—an application of enhanced condensational growth (ECG). J. Aerosol Med. Pulm. Drug Deliv. 2011, 24, 103–118. [Google Scholar] [CrossRef] [PubMed]
- Su, W.-C.; Wu, J.; Marijnissen, J.C.; Cheng, Y.S. Deposition of man-made fibers in a human nasal airway. Aerosol Sci. Technol. 2008, 42, 173–181. [Google Scholar] [CrossRef]
- Tavakol, M.; Ghahramani, E.; Abouali, O.; Yaghoubi, M.; Ahmadi, G. Deposition fraction of ellipsoidal fibers in a model of human nasal cavity for laminar and turbulent flows. J. Aerosol Sci. 2017, 113, 52–70. [Google Scholar] [CrossRef]
- Wang, Z.; Hopke, P.K.; Ahmadi, G.; Cheng, Y.-S.; Baron, P.A. Fibrous particle deposition in human nasal passage: The influence of particle length, flow rate, and geometry of nasal airway. J. Aerosol Sci. 2008, 39, 1040–1054. [Google Scholar] [CrossRef]
- Pope, C.A., III; Dockery, D.W. Epidemiology of particle effects. In Air Pollution and Health, 1st ed.; Holgate, S.T., Samet, J.M., Koren, H.S., Maynard, R.L., Eds.; Academic Press: Cambridge, MA, USA, 1999; pp. 673–705. [Google Scholar]
- Uduma, A.; Jimoh, W. High incidence of asthma, bronchitis, pneumonia and sinusitis in Kano state, North West Nigeria during Saharan Dust Events. Am. J. Environ. Energy Power Res. 2013, 18, 174–185. Available online: https://www.semanticscholar.org/paper/High-Incidence-of-Asthma-%2C-Bronchitis-%2C-Pneumonia-%2C-Uduma/8fd72fd302e09a6fe97a533664567004174f62a1 (accessed on 8 May 2022).
- Chu, H.; Xin, J.; Yuan, Q.; Wang, M.; Cheng, L.; Zhang, Z.; Lu, M. The effects of particulate matters on allergic rhinitis in Nanjing, China. Environ. Sci. Pollut. Res. 2019, 26, 11452–11457. [Google Scholar] [CrossRef]
- Calhoun, K.H.; Waggenspack, G.A.; Simpson, C.B.; Hokanson, J.A.; Bailey, B.J. CT evaluation of the paranasal sinuses in symptomatic and asymptomatic populations. Otolaryngol.—Head Neck Surg. 1991, 104, 480–483. [Google Scholar] [CrossRef]
- Kucybała, I.; Janik, K.A.; Ciuk, S.; Storman, D.; Urbanik, A. Nasal Septal Deviation and Concha Bullosa–Do They Have an Impact on Maxillary Sinus Volumes and Prevalence of Maxillary Sinusitis? Pol. J. Radiol. 2017, 82, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yousem, D.M.; Kennedy, D.; Rosenberg, S. Ostiomeatal complex risk factors for sinusitis: CT evaluation. J. Otolaryngol. 1991, 20, 419. [Google Scholar] [PubMed]
- Inthavong, K. A unifying correlation for laminar particle deposition in 90-degree pipe bends. Powder Technol. 2019, 345, 99–110. [Google Scholar] [CrossRef]
- Park, W.B.; Kim, Y.J.; Kang, K.L.; Lim, H.C.; Han, J.Y. Long-term outcomes of the implants accidentally protruding into nasal cavity extended to posterior maxilla due to inferior meatus pneumatization. Clin. Implant. Dent. Relat. Res. 2020, 22, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Matida, E.A.; Gu, J.; Johnson, M.R. Numerical simulation of aerosol deposition in a 3-D human nasal cavity using RANS, RANS/EIM, and LES. J. Aerosol Sci. 2007, 38, 683–700. [Google Scholar] [CrossRef]
- Menter, F.R.; Langtry, R.; Likki, S.; Suzen, Y.; Huang, P.; Völker, S. A correlation-based transition model using local variables—Part I: Model formulation. J. Turbomach. 2006, 128, 413–422. [Google Scholar] [CrossRef]
- Menter, F.R.; Langtry, R.; Völker, S. Transition modelling for general purpose CFD codes. Flow Turbul. Combust. 2006, 77, 277–303. [Google Scholar] [CrossRef]
- Heenan, A.; Matida, E.; Pollard, A.; Finlay, W. Experimental measurements and computational modeling of the flow field in an idealized human oropharynx. Exp. Fluids 2003, 35, 70–84. [Google Scholar] [CrossRef]
- Chen, X.; Feng, Y.; Zhong, W.; Kleinstreuer, C. Numerical investigation of the interaction, transport and deposition of multicomponent droplets in a simple mouth-throat model. J. Aerosol Sci. 2017, 105, 108–127. [Google Scholar] [CrossRef]
- Chen, X.; Zhong, W.; Sun, B.; Jin, B.; Zhou, X. Study on gas/solid flow in an obstructed pulmonary airway with transient flow based on CFD–DPM approach. Powder Technol. 2012, 217, 252–260. [Google Scholar] [CrossRef]
- Chen, X.; Kleinstreuer, C.; Zhong, W.; Feng, Y.; Zhou, X. Effects of thermal airflow and mucus-layer interaction on hygroscopic droplet deposition in a simple mouth–throat model. Aerosol Sci. Technol. 2018, 52, 900–912. [Google Scholar] [CrossRef]
- Zhang, Z.; Kleinstreuer, C. Laminar-to-turbulent fluid–nanoparticle dynamics simulations: Model comparisons and nanoparticle-deposition applications. Int. J. Numer. Methods Biomed. Eng. 2011, 27, 1930–1950. [Google Scholar] [CrossRef]
- Calmet, H.; Kleinstreuer, C.; Houzeaux, G.; Kolanjiyil, A.; Lehmkuhl, O.; Olivares, E.; Vázquez, M. Subject-variability effects on micron particle deposition in human nasal cavities. J. Aerosol Sci. 2018, 115, 12–28. [Google Scholar] [CrossRef]
- Swift, D. Inspiratory inertial deposition of aerosols in human nasal airway replicate casts: Implication for the proposed NCRP lung model. Radiat. Prot. Dosim. 1991, 38, 29–34. [Google Scholar] [CrossRef]
- Guilmette, R.; Cheng, Y.; Yeh, H.; Swift, D. Deposition of 0.005–12 μm monodisperse particles in a computer-milled, MRI-based nasal airway replica. Inhal. Toxicol. 1994, 6, 395–399. [Google Scholar]
- Baraniuk, J.N. Pathogenesis of allergic rhinitis. J. Allergy Clin. Immunol. 1997, 99, S763–S772. [Google Scholar] [CrossRef]
- Hong, Z.; Guo, Z.; Zhang, R.; Xu, J.; Dong, W.; Zhuang, G.; Deng, C. Airborne fine particulate matter induces oxidative stress and inflammation in human nasal epithelial cells. Tohoku J. Exp. Med. 2016, 239, 117–125. [Google Scholar] [CrossRef]
- Meng, Y.; Wang, C.; Zhang, L. Recent developments and highlights in allergic rhinitis. Allergy 2019, 74, 2320–2328. [Google Scholar] [CrossRef]
- Heusinkveld, H.J.; Wahle, T.; Campbell, A.; Westerink, R.H.; Tran, L.; Johnston, H.; Stone, V.; Cassee, F.R.; Schins, R.P. Neurodegenerative and neurological disorders by small inhaled particles. Neurotoxicology 2016, 56, 94–106. [Google Scholar] [CrossRef]
- Ghalati, P.F.; Keshavarzian, E.; Abouali, O.; Faramarzi, A.; Tu, J.; Shakibafard, A. Numerical analysis of micro- and nano-particle deposition in a realistic human upper airway. Comput. Biol. Med. 2012, 42, 39–49. [Google Scholar] [CrossRef]
- Polat, C.; Dostbil, Z. Evaluation of the nasal mucociliary transport rate by rhinoscintigraphy before and after surgery in patients with deviated nasal septum. Eur. Arch. Oto-Rhino-Laryngol. 2010, 267, 529–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nose-to-Throat Airway | Flow Rate (L/min) | Airflow Allocation (%) | Pressure Drop (Pa) | |||
|---|---|---|---|---|---|---|
| Total | Left | Right | Left | Right | ||
| Original model | 15.0 | 12.6 | 2.4 | 84.0 | 16.0 | 31.6 |
| 60.0 | 50.0 | 10.0 | 83.3 | 16.7 | 425.8 | |
| VS1 model | 15.0 | 11.4 | 3.6 | 76.0 | 24.0 | 31.3 |
| 60.0 | 46.3 | 13.7 | 77.2 | 22.8 | 416.2 | |
| VS2 model | 15.0 | 10.0 | 5.0 | 66.7 | 33.3 | 30.9 |
| 60.0 | 39.1 | 20.9 | 65.2 | 34.8 | 415.5 | |
| Flow Rate | Model | Regional Deposition Fraction (%) | Total Deposition Fraction (%) | ||
|---|---|---|---|---|---|
| Nasal Cavity | Nasopharynx | Laryngopharynx and Throat | |||
| 15 L/min | Original | 6.39 | 0.44 | 14.00 | 20.83 |
| VS1 | 9.67 | 0.06 | 10.98 | 20.71 | |
| VS2 | 3.24 | 0.05 | 9.29 | 12.58 | |
| 60 L/min | Original | 89.78 | 2.50 | 6.59 | 98.87 |
| VS1 | 88.88 | 3.36 | 5.66 | 97.90 | |
| VS2 | 62.53 | 7.11 | 19.28 | 88.92 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tao, F.; Feng, Y.; Sun, B.; Wang, J.; Chen, X.; Gong, J. Septoplasty Effect on the Enhancement of Airflow Distribution and Particle Deposition in Nasal Cavity: A Numerical Study. Healthcare 2022, 10, 1702. https://doi.org/10.3390/healthcare10091702
Tao F, Feng Y, Sun B, Wang J, Chen X, Gong J. Septoplasty Effect on the Enhancement of Airflow Distribution and Particle Deposition in Nasal Cavity: A Numerical Study. Healthcare. 2022; 10(9):1702. https://doi.org/10.3390/healthcare10091702
Chicago/Turabian StyleTao, Feng, Yu Feng, Baobin Sun, Jianwei Wang, Xiaole Chen, and Jiarui Gong. 2022. "Septoplasty Effect on the Enhancement of Airflow Distribution and Particle Deposition in Nasal Cavity: A Numerical Study" Healthcare 10, no. 9: 1702. https://doi.org/10.3390/healthcare10091702