
Qualitative Focus Groups with Professionals of Special Education and Parents of Young Females with Intellectual Disability Exploring Experiences with Menstrual Hygiene Management and the Trigger for the Non-Therapeutic Hysterectomy in Mexico
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Recruitment and Research Participants
2.3. Terminology
2.4. Sample and Sampling
2.5. Pre-Focus Group Activities
2.6. Procedure and Data Collection
2.7. Analysis
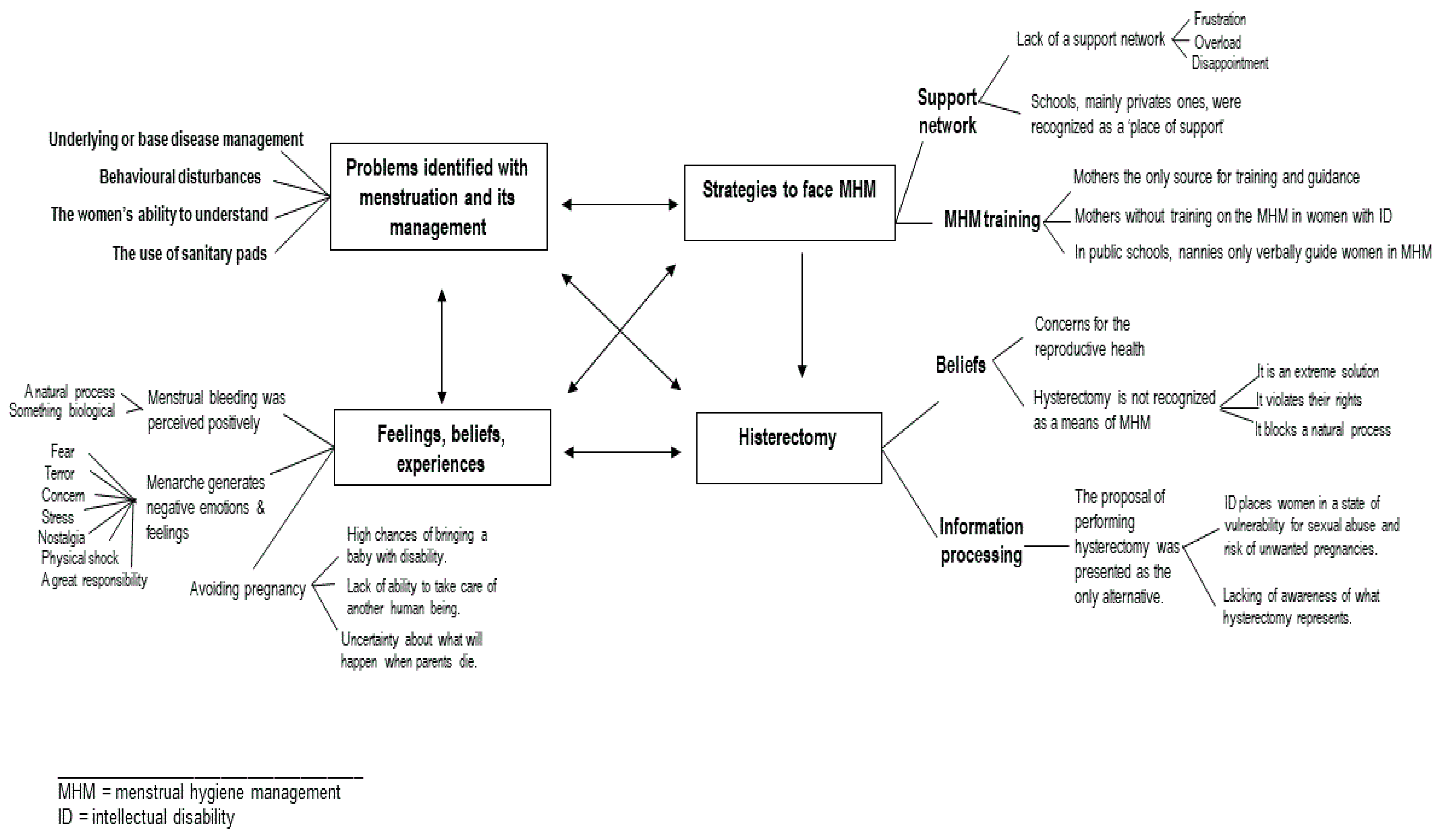
3. Results
3.1. Problems Identified with Menstruation and Its Management
3.1.1. The Underlying or Base Disease as a Problem
“Currently, I feel very happy, very satisfied with my daughter… obviously, in the beginning, it is like a struggle that one has to go through, until acceptance. When my daughter was seven years old, she entered the children’s psychiatric hospital, I could not talk to my daughter… I cried, cried and cried, so I received psychological therapy until I was able to accept my daughter, and when I succeeded, I said: well, that’s it!… And what did I do? Well, take care of her… Starting from there, I had to work for it” [P1, MG].
3.1.2. The Adolescent’s Ability to Understand
“It is hard to understand her… she tells us one thing, she specifies something, and for us, it is something like that on the air… very frustrating” [P1, PJ].
“She has not a properly developed language; then, making her understand that menstruation is coming and that it is completely natural is a problem; because there is no way to explain it to her directly, as you would do with someone who has a more extensive language” [P13, MK].
3.1.3. The Use of Sanitary Pads
“She did not like it, she made this [moves hands in the form of rejection] to take it away, she did not want it” [P6, M2].
“She comes home and takes off her pad… and says, with an annoyed expression: ‘This is getting on my nerves. And I insist: ‘Baby, you have to wear that’, and she says ‘No’” [P11, MS].
3.1.4. Behaviour Disturbances
“My daughter is tremendous… She is always hugging people, she hugs and kisses everyone, and she doesn’t care, even men… and that scares me a lot. I always talk to her and tell her: ‘No, daughter…’ It is very difficult for me to make her understand, that is my concern more than anything” [D15, MA].
3.1.5. School
“They do not bring them regularly, they leave them at home, precisely because the girls have not been helped with managing their cycle… that is why most choose not to send them [to school]. Parents only let us know: ‘They are in their menstrual cycle, and teacher, the truth is, I prefer not to bring her because I am the one who has to be cleaning her’. Parents who decide to take their daughters to school must sign [a document, at school] that they will be on the phone for when the girls have to go to the bathroom because they have to go change them themselves…” [P3, L].
3.2. Feelings, Beliefs, Experiences
“Menstruation is not something that important in our daughters, because, for the problems that one has, menstruation is the least of it… The fact that she menstruates, that she stains are the least of it” [P1, MG, MK, MJ].
“I did get scared, and the truth is, I then felt in my body that I couldn’t touch her. I didn’t have sisters, and well, we’re not ready, right? One only cries” [10, PZ].
“For me, it was a shock (…); yes, a responsibility, a great responsibility, for the care that we must have, not only in hygiene… Once the girl begins her menstrual period, she is subject to pregnancy…“ [10, ME].
“I’m not going to lie to you, I’m very scared, I don’t know what will happen, I think I start crying with her [she has an anguished expression] because literally, I’m alone [denotes that she wants to cry, but she contains herself]. I recently separated from my husband; so, the truth is, I am very scared; I have nightmares, I dream that my daughter is raped, that she becomes pregnant, that I see her give birth [she says it very quickly, she has an expression of anguish and terror]; I mean, literally (…), the truth is, I’m very scared” [11, M9].
“I feel that she is going to take it normally, but, well…, I’m afraid that moment will come, I imagine it will be very difficult…” [2, M1].
“But I am distressed, I have woken up with anxiety and panic attacks; yes, I have woken up like that… Because I think, what will happen when I die [he has an anguished expression]. Even though I think my son is going to treat her well, I am in a hurry to know whom she is going to stay with. This, too, was the most pressing issue for my wife when she died; furthermore, my wife made my sister swear that if no one would take care of her [she refers to her daughter with ID], she would take care of my daughter… [he has an expression of pain and sadness when he remembers this fact]; So yes, I do feel anguish, and a lot [you can see the tension in his face]…” [7].
3.3. Strategies to Face Menstrual Hygiene Management
3.3.1. Support Network
3.3.2. Menstrual Hygiene Management Training
“She knows what menstruation is… When changing the pad, I show it to her and say: ‘Look… does it go on like this?’ Likewise, when I take off the pad, I teach her what she should do… Also, in some way, I tell her: ‘Don’t say that [she refers to menstrual bleeding], you have to go to the bathroom and call me, but don’t tell people [she raises the volume of her voice]. No one should know that you have your period.’ But she has a cognitive level of a girl of three to four years, so, imagine that…” [7, M].
“Right now, it’s only three months [she refers to the menarche], I still have to be saying: ‘Look, this is a pad, we have to put it here…’. I have to be careful that she doesn’t get dirty, to take her to the bathroom… I know that she is going to learn it in time, and she is going to do it; but, well, it’s going to take a little while…” [14, MT].
3.4. Hysterectomy
3.4.1. Beliefs
3.4.2. Information Processing and Choice
“The pediatrician immediately told me: ‘You know what, why are you thinking about it? I mean, the only possibility you have with her is to remove the uterus. Medically, what is recommended for families is to operate them due to the situation that they are very vulnerable girls, they are very innocent girls…’ ‘The pediatrician also told me: ‘I understand that you take care of your daughter and you are always on the lookout for her; but… well, you never know…’
I thought they [surgeons] had to open it like a cesarean section or something like that, but she told me ‘no’, it’s through the navel… She even told me: ‘Look, you know that the uterus is only for having children, it does not help you to do anything other than having children, and the only thing you would do is help your daughter… in case of sexual abuse. And I have to tell you (she told me), I advise you to learn more about the operation, they are very vulnerable girls… Obviously, do it before it arrives’ [she refers to the menarche…]” [4, MY].
4. Discussion
4.1. The Underlying or Base Disease
4.2. Menstruation and Education
4.3. Pregnancy
4.4. Strengths and Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Definition: Intellectual Disability. Available online: http://www.euro.who.int/en/health-topics/noncommunicable-diseases/mental-health/news/news/2010/15/childrens-right-to-family-life/definition-intellectual-disability (accessed on 7 December 2021).
- WHO. ICD 11th Revision. Available online: https://icd.who.int/browse11/l-m/en (accessed on 7 December 2021).
- Maulik, P.K.; Mascarenhas, M.N.; Mathers, C.D.; Dua, T.; Saxena, S. Prevalence of intellectual disability: A meta-analysis of population-based studies. Res. Dev. Disabil. 2011, 32, 419–436. [Google Scholar] [CrossRef] [PubMed]
- Márquez-González, H.; Valdez-Martinez, E.; Bedolla, M. Hysterectomy for the management of menstrual hygiene in women with intellectual disability. A systematic review focusing on standards and ethical considerations for developing countries. Front. Public Health 2018, 6, 338. [Google Scholar] [CrossRef] [PubMed]
- Wilbur, J.; Torondel, B.; Hameed, S.; Mahon, T.; Kuper, H. Systematic review of menstrual hygiene management requirements, its barriers and strategies for disabled people. PLoS ONE 2019, 14, e0210974. [Google Scholar] [CrossRef]
- Márquez-González, H.; Valdez-Martínez, E.; Bedolla, M. Clinical, Epidemiologic and ethical aspects of hysterectomy in young females with intellectual disability: A multi-centre study of public hospitals in Mexico City. Front. Public Health 2021, 9, 746399. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Statistics and Geography (INEGI, Its Acronym in Spanish). National Diagnosis on the Situation of People with Impairment. May 2016. Available online: https://www.gob.mx/cms/uploads/attachment/file/126572/Diagn_stico_sobre_la_Situaci_n_de_las_Personas_Con_Discapacidad._Mayo_2016.pdf (accessed on 7 December 2021).
- Open Database: National Institute of Statistics and Geography (INEGI, Its Acronym in Spanish). Poverty in Mexico. Available online: https://www.coneval.org.mx/Medicion/Paginas/PobrezaInicio.aspx (accessed on 7 December 2021).
- Morgan, D.L. The Focus Group Guidebook. In The Focus Group Kit; Morgan, D.L., Krueger, R.A., Eds.; SAGE Publications Ltd.: London, UK, 1998. [Google Scholar]
- National Institute of Statistics and Geography (INEGI, Its Acronym in Spanish). Mexican National Directory of Associations of and for People with Disabilities. 2002. Available online: http://intranet.dif.df.gob.mx/transparencia/new/art_15/10/_anexos/07%20dir%20nal%20de%20asoc%20de%20y%20para%20personas%20con%20disca.pdf (accessed on 7 December 2021).
- Kuzel, A.J. Sampling in Qualitative Inquiry. In Doing Qualitative Research, 2nd ed.; Crabtree, B.G., Miller, W.L., Eds.; SAGE Publications Ltd.: London, UK, 1992; pp. 31–44. [Google Scholar]
- Sandelowski, M. Sample size in qualitative research. Res. Nurs. Health 1995, 18, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Can I use TA? Should I use TA? Should I not use TA? Comparing reflexive thematic analysis and other pattern-based qualitative analytic approaches. Couns. Psychother. Res. 2021, 21, 37–47. [Google Scholar] [CrossRef]
- Ambikile, J.S.; Outwater, A. Challenges of caring for children with mental disorders: Experiences and views of caregivers attending the outpatient clinic at Muhimbili national Hospital, Dar es Salaam, Tanzania. Child Adolesc. Psychiatry Ment. Health 2012, 6, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chandra Mouli, V.; Vipul-Patel, S. Mapping the knowledge and understanding of menarche, menstrual hygiene and menstrual health among adolescent girls in low- and middle-income countries. Reprod. Health 2017, 14, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Van Eijk, A.M.; Sivakami, M.; Thakkar, M.B.; Bauman, A.; Laserson, K.F.; Coates, S.; Phillips-Howard, P. Menstrual hygiene management among adolescent girls in India: A systematic review and meta-analysis. BMJ Open 2016, 6, e010290. [Google Scholar] [CrossRef] [PubMed]
- Amelik, Q.; Roozen, S.; Leistiknow, I.; Weenink, J.W. Sexual abuse of people with intellectual disabilities in residential stings: A 3-year analysis of incidents reported to the Dutch Halth anf Youth Care Inspectorate. BMJ Open 2021, 11, e053317. [Google Scholar] [CrossRef]
- Martin, B.K.; Ballan, M.; Darabi, F.; Karyany, A.K.; Soofi, M.; Soltani, S. Sexual health concerns in women with intellectual disabilities: A systematic review in qualitative studies. BMC Public Health 2021, 21, 1965. [Google Scholar] [CrossRef]
- Wissink, I.B.; van Vugt EMoonen, X.; Stams, G.J.J.M.; Hendriks, J. Sexual abuse involving children with an intellectual disability; a narrative review. Res. Dev. Disabil. 2015, 36, 20–35. [Google Scholar] [CrossRef] [PubMed]
- WHO; World Bank. World Report on Disability. 2011. Available online: https://www.who.int/teams/noncommunicable-diseases/sensory-functions-disability-and-rehabilitation/world-report-on-disability (accessed on 7 December 2021).
- Ahmad Odeh, B.; Khader AlTarawneh, R. Attitudes of the mothers toward hysterectomy for their daughters with intellectual disability in Sultanate of Oman, and motives for the hysterectomy. Eur. J. Soc. Sci. 2016, 53, 8090. [Google Scholar]
- Thapa, P.; Sivakami, M. Lost in transition: Menstrual experiences of intellectual disabled school-going adolescents in Delhi, India. Waterlines 2017, 36, 317–338. [Google Scholar] [CrossRef]
- Chou, Y.C.; Lu, Z.-Y.J. Caring for a daughter with intellectual disabilities in managing menstruation: A mother’s perspective. J. Intellect. Dev. Disabil. 2012, 37, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, J.; Dreyfus, D.; Cerreto, M.; Bokhour, B. “Sometimes I feel overwhelmed”: Educational needs of family physicians caring for people with intellectual disability. Intellect. Dev. Disabil. 2012, 50, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Agaronnik, N.; Campbell, E.G.; Ressalam, J.; Lezzoni, L.I. Exploring issues relating to disability cultural competence among practicing physicians. Disabil. Health J. 2019, 12, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Eddey, G.E.; Robey, K.L. Considering the culture of disability in cultural competence education. Acad. Med. 2005, 80, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Trollor, J.N.; Eagleson, C.; Turner, B.; Tracy, J.; Torr, J.J.; Durvasula SLacono, T.; Cvejic, R.C.; Lennox, N. Intellectual disability content within tertiary medical curriculum: How is it taught and by whom? BMC Med. Educ. 2018, 18, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beauchamp, T.L.; Childress, J.F. Principles of Biomedical Ethics, 5th ed.; Oxford University Press: New York, NY, USA, 2001. [Google Scholar]
- WHO. What Do We Know about Capacity Building? An Overview of Existing Knowledge and Good Practice. 2001. Available online: https://apps.who.int/iris/handle/10665/67394 (accessed on 16 August 2022).


{kind=link}
| a Parents n = 69 Number (%) | b Professionals of Special Education n = 11 Number (%) | |
|---|---|---|
| Carer’s age, mean (SD) | 44 (±10) | 38 (±7) |
| Carer’ gender | ||
| Female | 65 (94) | 9 |
| Male | 4 (6) | 2 |
| Carer’s marital status | ||
| Married | 37 (54) | |
| Single | 19 (28) | |
| Widow/widower | 7 (10) | |
| Living together | 3 (4) | |
| Without data | 3 (4) | 11 (100) |
| Carer’s relationship to women with ID | ||
| Mother | 61 (88) | |
| Parent | 4 (6) | |
| Grandmother | 3 (4) | |
| Aunt | 1 (1) | |
| Carer’ residence | ||
| Mexico City | 62 (90) | 7 (64) |
| State of Mexico | 7 (10) | 4 (36) |
| Carer’s highest education level c | ||
| Basic schooling | 22 (32) | |
| Medium superior level | 25 (36) | 1 (9) |
| Superior level | 22 (32) | 10 (99) |
| Carer’s employment status | ||
| Housewife | 38 (55) | |
| Employed (informal) | 15 (22) | |
| Employment (formal) | 13 (19) | d 11 (100) |
| Retired | 3 (4) |
| Number (%) | |
|---|---|
| Age, mean (SD) | 14 (±9) |
| Menstruation | |
| Premenarcheal | 36 (52) |
| Menstruating young women | a 32 (46) |
| Will not have menstruation | 1 (1) |
| Intellectual disability degree | |
| Superficial | 9 (13) |
| Mild | 17 (24) |
| Moderate | 15 (22) |
| Severe | 6 (9) |
| Carers ignored the ID degree | 22 (32) |
| Aetiology of the ID reported by the carers | |
| Multifactorial | 50 (72) |
| Genetic-primary | 19 (28) |
| Living situation | |
| With carer | 26 (38) |
| With family | 40 (58) |
| b Education level | |
| Basic schooling | 67 (97) |
| Medium superior level | 1 (1) |
| Superior level | 1 (1) |
| c Type of school | |
| Public | 53 (77) |
| Private | 16 (23) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flores-Medina, M.d.R.; Valdez-Martinez, E.; Márquez-González, H. Qualitative Focus Groups with Professionals of Special Education and Parents of Young Females with Intellectual Disability Exploring Experiences with Menstrual Hygiene Management and the Trigger for the Non-Therapeutic Hysterectomy in Mexico. Healthcare 2022, 10, 1690. https://doi.org/10.3390/healthcare10091690
Flores-Medina MdR, Valdez-Martinez E, Márquez-González H. Qualitative Focus Groups with Professionals of Special Education and Parents of Young Females with Intellectual Disability Exploring Experiences with Menstrual Hygiene Management and the Trigger for the Non-Therapeutic Hysterectomy in Mexico. Healthcare. 2022; 10(9):1690. https://doi.org/10.3390/healthcare10091690
Chicago/Turabian StyleFlores-Medina, Maria del Rosario, Edith Valdez-Martinez, and Horacio Márquez-González. 2022. "Qualitative Focus Groups with Professionals of Special Education and Parents of Young Females with Intellectual Disability Exploring Experiences with Menstrual Hygiene Management and the Trigger for the Non-Therapeutic Hysterectomy in Mexico" Healthcare 10, no. 9: 1690. https://doi.org/10.3390/healthcare10091690