
Sex-Specific Association between Fasting Plasma Glucose and Serum Selenium Levels in Adults from Southern Mexico
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample and Ethical Approval
2.2. Anthropometric and Clinical Measurements
2.3. Serum Se Level Quantification by ICP-MS
2.4. Statistical Analysis
3. Results
3.1. Description of the General Characteristics of the Study Sample
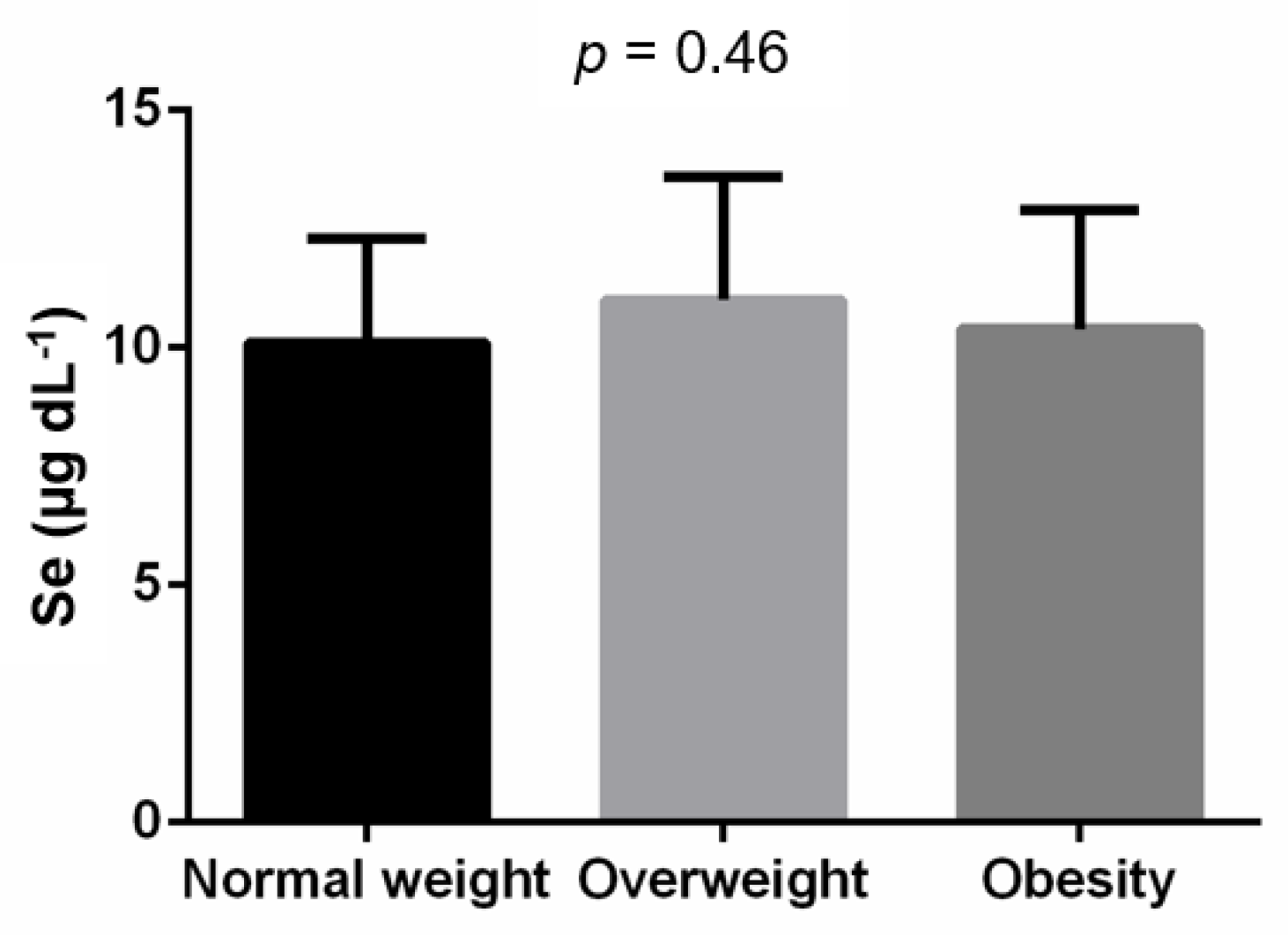
3.2. Association between BMI, Overweight, Obesity and Serum Se Level
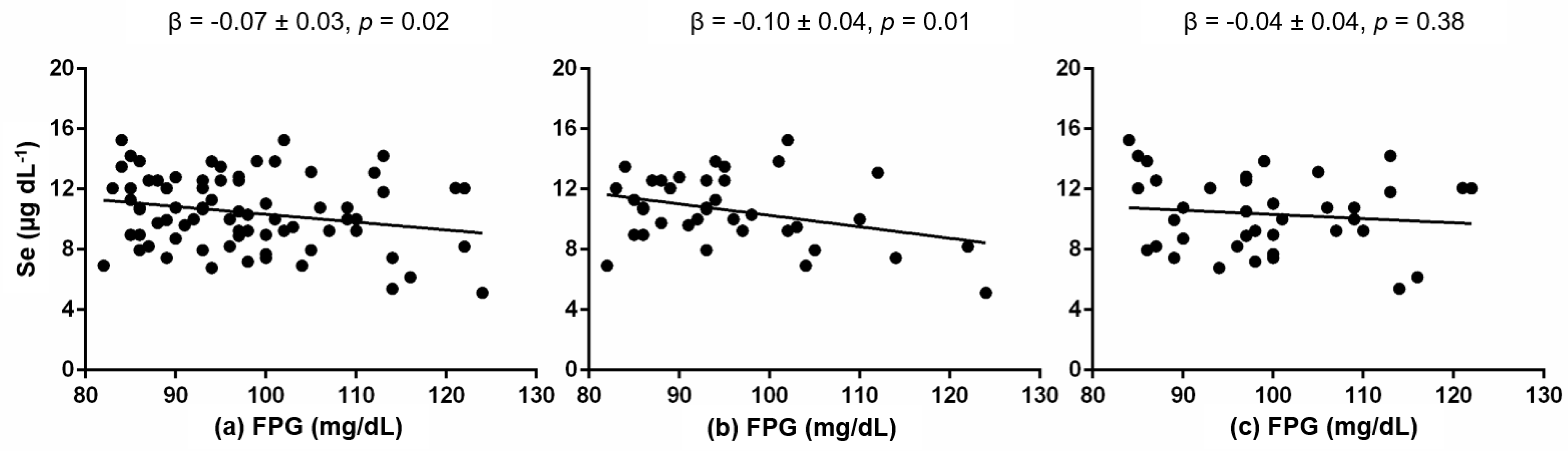
3.3. Association between Serum Se Level and Cardiometabolic Traits
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variable | Untransformed | Transformed |
|---|---|---|
| BMI (kg/m2) | 1.6 × 10−8 | 0.999 |
| SBP (mmHg) | 0.044 | 0.999 |
| DBP (mmHg) | 0.101 | - |
| TC (mg/dL) | 0.263 | - |
| HDL-C (mg/dL) | 0.051 | 0.995 |
| LDL-C (mg/dL) | 0.384 | - |
| TG (mg/dL) | 1.1 × 10−13 | 0.999 |
| FPG (mg/dL) | 0.004 | 0.995 |
| FPI (µU/mL) | 1.7 × 10−8 | 0.998 |
| HOMA-IR | 7.1 × 10−9 | 0.999 |
References
- Zimmet, P.Z. Diabetes and its drivers: The largest epidemic in human history? Clin. Diabetes Endocrinol. 2017, 3, 1. [Google Scholar] [CrossRef]
- Shamah-Levy, T.; Vielma-Orozco, E.; Heredia-Hernández, O.; Romero-Martínez, M.; Mojica-Cuevas, J.; Cuevas-Nasu, L.; Santaella-Castell, J.; Rivera-Dommarco, J. Encuesta Nacional de Salud y Nutrición 2018-19: Resultados Nacionales; Instituto Nacional de Salud Pública: Cuernavaca, Mexico, 2020. [Google Scholar]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef]
- Stumvoll, M.; Goldstein, B.J.; van Haeften, T.W. Type 2 diabetes: Principles of pathogenesis and therapy. Lancet 2005, 365, 1333–1346. [Google Scholar] [CrossRef]
- Chatterjee, S.; Khunti, K.; Davies, M.J. Type 2 diabetes. Lancet 2017, 389, 2239–2251. [Google Scholar] [CrossRef]
- Tinkov, A.A.; Ajsuvakova, O.P.; Filippini, T.; Zhou, J.-C.; Lei, X.G.; Gatiatulina, E.; Michalke, B.; Skalnaya, M.G.; Vinceti, M.; Aschner, M.; et al. Selenium and Selenoproteins in Adipose Tissue Physiology and Obesity. Biomolecules 2020, 10, 658. [Google Scholar] [CrossRef]
- Watanabe, L.; Navarro, A.; Seale, L. Intersection between Obesity, Dietary Selenium, and Statin Therapy in Brazil. Nutrients 2021, 13, 2027. [Google Scholar] [CrossRef]
- Méplan, C.; Hughes, D.J. The Role of Selenium in Health and Disease: Emerging and Recurring Trends. Nutrients 2020, 12, 1049. [Google Scholar] [CrossRef]
- Kohler, L.N.; Foote, J.; Kelley, C.P.; Florea, A.; Shelly, C.; Chow, H.-H.S.; Hsu, P.; Batai, K.; Ellis, N.; Saboda, K.; et al. Selenium and Type 2 Diabetes: Systematic Review. Nutrients 2018, 10, 1924. [Google Scholar] [CrossRef]
- Vinceti, M.; Filippini, T.; Rothman, K.J. Selenium exposure and the risk of type 2 diabetes: A systematic review and meta-analysis. Eur. J. Epidemiol. 2018, 33, 789–810. [Google Scholar] [CrossRef]
- Kohrle, J. Selenium in Endocrinology-Selenoprotein-Related Diseases, Population Studies, and Epidemiological Evidence. Endocrinology 2021, 162, bqaa228. [Google Scholar] [CrossRef]
- Misu, H.; Takamura, T.; Takayama, H.; Hayashi, H.; Matsuzawa-Nagata, N.; Kurita, S.; Ishikura, K.; Ando, H.; Takeshita, Y.; Ota, T.; et al. A Liver-Derived Secretory Protein, Selenoprotein P, Causes Insulin Resistance. Cell Metab. 2010, 12, 483–495. [Google Scholar] [CrossRef]
- Mita, Y.; Nakayama, K.; Toshinari, T.; Nishito, Y.; Yoshioka, Y.; Sakai, N.; Sotani, K.; Nagamura, T.; Kuzuhara, Y.; Inagaki, K.; et al. Selenoprotein P-neutralizing antibodies improve insulin secretion and glucose sensitivity in type 2 diabetes mouse models. Nat. Commun. 2017, 8, 1658. [Google Scholar] [CrossRef]
- Ojeda, M.L.; Nogales, F. Dietary Selenium and Its Antioxidant Properties Related to Growth, Lipid and Energy Metabolism. Antioxidants 2022, 11, 1402. [Google Scholar] [CrossRef]
- Zhong, Q.; Lin, R.; Nong, Q. Adiposity and Serum Selenium in U.S. Adults. Nutrients 2018, 10, 727. [Google Scholar] [CrossRef]
- Spina, A.; Guallar, E.; Rayman, M.P.; Tigbe, W.; Kandala, N.-B.; Stranges, S. Anthropometric indices and selenium status in British adults: The U.K. National Diet and Nutrition Survey. Free Radic. Biol. Med. 2013, 65, 1315–1321. [Google Scholar] [CrossRef]
- Othman, F.B.; Mohamed, H.J.B.J.; Sirajudeen, K.; Noh, M.F.B.; Rajab, N.F. The influence of selenium status on body composition, oxidative DNA damage and total antioxidant capacity in newly diagnosed type 2 diabetes mellitus: A case-control study. J. Trace Elem. Med. Biol. 2017, 43, 106–112. [Google Scholar] [CrossRef]
- Oo, S.M.; Misu, H.; Saito, Y.; Tanaka, M.; Kato, S.; Kita, Y.; Takayama, H.; Takeshita, Y.; Kanamori, T.; Nagano, T.; et al. Serum selenoprotein P, but not selenium, predicts future hyperglycemia in a general Japanese population. Sci. Rep. 2018, 8, 16727. [Google Scholar] [CrossRef]
- Galan, P.; Viteri, F.E.; Bertrais, S.; Czernichow, S.; Faure, H.; Arnaud, J.; Ruffieux, D.; Chenal, S.; Arnault, N.; Favier, A.; et al. Serum concentrations of β-carotene, vitamins C and E, zinc and selenium are influenced by sex, age, diet, smoking status, alcohol consumption and corpulence in a general French adult population. Eur. J. Clin. Nutr. 2005, 59, 1181–1190. [Google Scholar] [CrossRef]
- Letsiou, S.; Nomikos, T.; Panagiotakos, D.; Pergantis, S.; Fragopoulou, E.; Pitsavos, C.; Stefanadis, C.; Antonopoulou, S. Gender-specific distribution of selenium to serum selenoproteins: Associations with total selenium levels, age, smoking, body mass index, and physical activity. BioFactors 2014, 40, 524–535. [Google Scholar] [CrossRef]
- Tascilar, M.E.; Ozgen, I.T.; Abaci, A.; Serdar, M.; Aykut, O. Trace Elements in Obese Turkish Children. Biol. Trace Elem. Res. 2010, 143, 188–195. [Google Scholar] [CrossRef]
- Kljai, K.; Runje, R. Selenium and Glycogen Levels in Diabetic Patients. Biol. Trace Elem. Res. 2001, 83, 223–229. [Google Scholar] [CrossRef]
- Navarro-Alarcón, M.; de la Serrana, H.L.-G.; Pérez-Valero, V.; López-Martínez, C. Serum and urine selenium concentrations as indicators of body status in patients with diabetes mellitus. Sci. Total Environ. 1999, 228, 79–85. [Google Scholar] [CrossRef]
- Akbaraly, T.N.; Arnaud, J.; Rayman, M.P.; Hininger-Favier, I.; Roussel, A.-M.; Berr, C.; Fontbonne, A. Plasma selenium and risk of dysglycemia in an elderly French population: Results from the prospective Epidemiology of Vascular Ageing Study. Nutr. Metab. 2010, 7, 21. [Google Scholar] [CrossRef]
- Bleys, J.; Navas-Acien, A.; Guallar, E. Serum Selenium and Diabetes in U.S. Adults. Diabetes Care 2007, 30, 829–834. [Google Scholar] [CrossRef]
- Lippman, S.M.; Klein, E.A.; Goodman, P.J.; Lucia, M.S.; Thompson, I.M.; Ford, L.G.; Parnes, H.L.; Minasian, L.M.; Gaziano, J.M.; Hartline, J.A.; et al. Effect of selenium and vitamin E on risk of prostate cancer and other cancers: The Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA 2009, 301, 39–51. [Google Scholar] [CrossRef]
- Fang, C.; Wu, W.; Gu, X.; Dai, S.; Zhou, Q.; Deng, H.; Shen, F.; Chen, J. Association of serum copper, zinc and selenium levels with risk of metabolic syndrome: A nested case-control study of middle-aged and older Chinese adults. J. Trace Elem. Med. Biol. 2019, 52, 209–215. [Google Scholar] [CrossRef]
- Li, Z.; Li, X.; Ju, W.; Wu, G.; Yang, X.; Fu, X.; Gao, X. High serum selenium levels are associated with impaired fasting glucose and elevated fasting serum glucose in Linyi, China. J. Trace Elem. Med. Biol. 2018, 45, 64–69. [Google Scholar] [CrossRef]
- Lu, C.-W.; Chang, H.-H.; Yang, K.-C.; Chiang, C.-H.; Yao, C.-A.; Huang, K.-C. Gender Differences with Dose–Response Relationship between Serum Selenium Levels and Metabolic Syndrome—A Case-Control Study. Nutrients 2019, 11, 477. [Google Scholar] [CrossRef]
- Al-Mubarak, A.A.; Beverborg, N.G.; Suthahar, N.; Gansevoort, R.T.; Bakker, S.J.; Touw, D.J.; de Boer, R.A.; van der Meer, P.; Bomer, N. High selenium levels associate with reduced risk of mortality and new-onset heart failure: Data from PREVEND. Eur. J. Heart Fail. 2021, 24, 299–307. [Google Scholar] [CrossRef]
- WHO. Vitamin and Mineral Requirements in Human Nutrition; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Ge, X.; Yang, A.; Huang, S.; Luo, X.; Hou, Q.; Huang, L.; Zhou, Y.; Li, D.; Lv, Y.; Li, L.; et al. Sex-specific associations of plasma metals and metal mixtures with glucose metabolism: An occupational population-based study in China. Sci. Total Environ. 2020, 760, 143906. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Rios-Lugo, M.J.; Madrigal-Arellano, C.; Gaytán-Hernández, D.; Hernández-Mendoza, H.; Romero-Guzmán, E.T. Association of Serum Zinc Levels in Overweight and Obesity. Biol. Trace Elem. Res. 2020, 198, 51–57. [Google Scholar] [CrossRef]
- Vázquez-Moreno, M.; Locia-Morales, D.; Peralta-Romero, J.; Sharma, T.; Meyre, D.; Cruz, M.; Flores-Alfaro, E.; Valladares-Salgado, A. AGT rs4762 is associated with diastolic blood pressure in Mexicans with diabetic nephropathy. J. Diabetes Its Complicat. 2020, 35, 107826. [Google Scholar] [CrossRef]
- Vázquez-Moreno, M.; Locia-Morales, D.; Valladares-Salgado, A.; Sharma, T.; Wacher-Rodarte, N.; Cruz, M.; Meyre, D. Sex/Gender Modifies the Association Between the MC4R p.Ile269Asn Mutation and Type 2 Diabetes in the Mexican Population. J. Clin. Endocrinol. Metab. 2020, 106, e112–e117. [Google Scholar] [CrossRef]
- Ortega, M.; Rodriguez-Rodriguez, E.; Aparicio, A.; Jiménez-Ortega, I.; Palmeros, C.; Perea, M.; Navia, B.; López-Sobaler, A.M. Young Children with Excess of Weight Show an Impaired Selenium Status. Int. J. Vitam. Nutr. Res. 2012, 82, 121–129. [Google Scholar] [CrossRef]
- Błażewicz, A.; Klatka, M.; Astel, A.; Korona-Glowniak, I.; Dolliver, W.; Szwerc, W.; Kocjan, R. Serum and urinary selenium levels in obese children: A cross-sectional study. J. Trace Elem. Med. Biol. 2015, 29, 116–122. [Google Scholar] [CrossRef]
- Rayman, M.P. Selenium intake, status, and health: A complex relationship. Hormones 2019, 19, 9–14. [Google Scholar] [CrossRef]
- González-Torres, S.; González-Silva, N.; Pérez-Reyes, Á.; Anaya-Esparza, L.M.; Sánchez-Enríquez, S.; Vargas-Becerra, P.N.; Villagrán, Z.; García-García, M.R. Food Consumption and Metabolic Risks in Young University Students. Int. J. Environ. Res. Public Health 2021, 19, 449. [Google Scholar] [CrossRef]
- Wyatt, J.; Melendez, J.; Acufia, N.; Rascon, A. Selenium (Se) in foods in northern Mexico, their contribution to the daily Se intake and the relationship of Se plasma levels and glutathione peroxidase activity. Nutr. Res. 1996, 16, 949–960. [Google Scholar] [CrossRef]
- Tanvir, E.M.; Whitfield, K.M.; Ng, J.C.; Shaw, P.N. Development and Validation of an ICP-MS Method and Its Application to Determine Multiple Trace Elements in Small Volumes of Whole Blood and Plasma. J. Anal. Toxicol. 2020, 44, 1036–1046. [Google Scholar] [CrossRef]
- Laur, N.; Kinscherf, R.; Pomytkin, K.; Kaiser, L.; Knes, O.; Deigner, H.-P. ICP-MS trace element analysis in serum and whole blood. PLoS ONE 2020, 15, e0233357. [Google Scholar] [CrossRef] [PubMed]
- Longnecker, M.P.; Stram, D.O.; Taylor, P.R.; Levander, O.A.; Howe, M.; Veillon, C.; McAdam, P.A.; Patterson, K.Y.; Holden, J.M.; Morris, J.S.; et al. Use of Selenium Concentration in Whole Blood, Serum, Toenails, or Urine as a Surrogate Measure of Selenium Intake. Epidemiology 1996, 7, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Combs, G.F., Jr. Biomarkers of selenium status. Nutrients 2015, 7, 2209–2236. [Google Scholar] [CrossRef]
- Kornhauser, C.; Garcia-Ramirez, J.R.; Wrobel, K.; Pérez-Luque, E.-L.; Garay-Sevilla, M.-E.; Wrobel, K. Serum selenium and glutathione peroxidase concentrations in type 2 diabetes mellitus patients. Prim. Care Diabetes 2008, 2, 81–85. [Google Scholar] [CrossRef]
- Park, K.; Rimm, E.B.; Siscovick, D.S.; Spiegelman, D.; Manson, J.E.; Morris, J.S.; Hu, F.B.; Mozaffarian, D. Toenail Selenium and Incidence of Type 2 Diabetes in U.S. Men and Women. Diabetes Care 2012, 35, 1544–1551. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.; Heng, B.; He, W.; Shi, L.; Lai, C.; Xiao, L.; Ren, H.; Mo, S.; Su, Z. Chronic reactive oxygen species exposure inhibits glucose uptake and causes insulin resistance in C2C12 myotubes. Biochem. Biophys. Res. Commun. 2016, 478, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Salsman, S.J.; Hensley, K.; Floyd, R.A. Sensitivity of Protein Tyrosine Phosphatase Activity to the Redox Environment, Cytochrome c, and Microperoxidase. Antioxid. Redox Signal. 2005, 7, 1078–1088. [Google Scholar] [CrossRef]
- Mueller, A.S.; Klomann, S.D.; Wolf, N.M.; Schneider, S.; Schmidt, R.; Spielmann, J.; Stangl, G.; Eder, K.; Pallauf, J. Redox Regulation of Protein Tyrosine Phosphatase 1B by Manipulation of Dietary Selenium Affects the Triglyceride Concentration in Rat Liver. J. Nutr. 2008, 138, 2328–2336. [Google Scholar] [CrossRef]
- Fürnsinn, C.; Englisch, R.; Ebner, K.; Nowotny, P.; Vogl, C.; Waldhäusl, W. Insulin-like vs. non-insulin-like stimulation of glucose metabolism by vanadium, tungsten, and selenium compounds in rat muscle. Life Sci. 1996, 59, 1989–2000. [Google Scholar] [CrossRef]
- Siddiqi, S.M.; Sun, C.; Wu, X.; Shah, I.; Mehmood, A. The Correlation between Dietary Selenium Intake and Type 2 Diabetes: A Cross-Sectional Population-Based Study on North Chinese Adults. BioMed Res. Int. 2020, 2020, 8058463. [Google Scholar] [CrossRef]
- Goldstein, B.J.; Mahadev, K.; Wu, X. Redox paradox: Insulin action is facilitated by insulin-stimulated reactive oxygen species with multiple potential signaling targets. Diabetes 2005, 54, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Mahadev, K.; Zilbering, A.; Zhu, L.; Goldstein, B.J. Insulin-stimulated Hydrogen Peroxide Reversibly Inhibits Protein-tyrosine Phosphatase 1B in Vivo and Enhances the Early Insulin Action Cascade. J. Biol. Chem. 2001, 276, 21938–21942. [Google Scholar] [CrossRef] [PubMed]
- McClung, J.P.; Roneker, C.A.; Mu, W.; Lisk, D.J.; Langlais, P.; Liu, F.; Lei, X.G. Development of insulin resistance and obesity in mice overexpressing cellular glutathione peroxidase. Proc. Natl. Acad. Sci. USA 2004, 101, 8852–8857. [Google Scholar] [CrossRef] [PubMed]
- Waters, D.J.; Chiang, E.C.; Cooley, D.M.; Morris, J. Making sense of sex and supplements: Differences in the anticarcinogenic effects of selenium in men and women. Mutat. Res. Mol. Mech. Mutagen. 2004, 551, 91–107. [Google Scholar] [CrossRef]
- Cardoso, B.R.; Hare, D.J.; Macpherson, H. Sex-dependent association between selenium status and cognitive performance in older adults. Eur. J. Nutr. 2020, 60, 1153–1159. [Google Scholar] [CrossRef]
- Ma, X.; Jiang, S.; Yan, S.; Li, M.; Wang, C.; Pan, Y.; Sun, C.; Jin, L.; Yao, Y.; Li, B. Association Between Copper, Zinc, Iron, and Selenium Intakes and TC/HDL-C Ratio in US Adults. Biol. Trace Elem. Res. 2019, 197, 43–51. [Google Scholar] [CrossRef]
- Hu, H.; Bi, C.; Lin, T.; Liu, L.; Song, Y.; Wang, B.; Wang, P.; Zhou, Z.; Fang, C.; Ma, H.; et al. Sex difference in the association between plasma selenium and first stroke: A community-based nested case-control study. Biol. Sex Differ. 2021, 12, 39. [Google Scholar] [CrossRef]
- Liao, X.-L.; Wang, Z.-H.; Liang, X.-N.; Liang, J.; Wei, X.-B.; Wang, S.-H.; Guo, W.-X. The Association of Circulating Selenium Concentrations with Diabetes Mellitus. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 4755–4761. [Google Scholar] [CrossRef]
- Méplan, C.; Crosley, L.K.; Nicol, F.; Beckett, G.J.; Howie, A.F.; Hill, K.E.; Horgan, G.; Mathers, J.C.; Arthur, J.R.; Hesketh, J.E. Genetic polymorphisms in the human selenoprotein P gene determine the response of selenoprotein markers to selenium supplementation in a gender-specific manner (the SELGEN study). FASEB J. 2007, 21, 3063–3074. [Google Scholar] [CrossRef]
- Kim, M.J.; Rolland, Y.; Cepeda, O.; Gammack, J.K.; Morley, J.E. Diabetes mellitus in older men. Aging Male 2006, 9, 139–147. [Google Scholar] [CrossRef]
- Ren, J. Cardiac health and diabetes mellitus in women: Problems and prospects. Minerva Cardioangiol. 2006, 54, 289–309. [Google Scholar] [PubMed]
- Kelly, M.M.; Tyrka, A.R.; Anderson, G.M.; Price, L.H.; Carpenter, L.L. Sex differences in emotional and physiological responses to the Trier Social Stress Test. J. Behav. Ther. Exp. Psychiatry 2008, 39, 87–98. [Google Scholar] [CrossRef]
- Tomova, L.; von Dawans, B.; Heinrichs, M.; Silani, G.; Lamm, C. Is stress affecting our ability to tune into others? Evidence for gender differences in the effects of stress on self-other distinction. Psychoneuroendocrinology 2014, 43, 95–104. [Google Scholar] [CrossRef]
- Rannelli, L.A.; MacRae, J.; Mann, M.C.; Ramesh, S.; Hemmelgarn, B.R.; Rabi, D.; Sola, D.Y.; Ahmed, S.B. Sex differences in associations between insulin resistance, heart rate variability, and arterial stiffness in healthy women and men: A physiology study. Can. J. Physiol. Pharmacol. 2017, 95, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Mendoza, H.; Martínez-Navarro, I.; Hernández-Ochoa, E.; Espinoza-Ruiz, M.; Lugo-Trampe, A.; Trujillo-Murillo, K.D.C.; López-García, M.; Rios-Lugo, M.J.; Chang-Rueda, C. Serum zinc levels are associated with obesity and low-density lipoprotein cholesterol in Mexican adults. J. Trace Elem. Med. Biol. 2022, 73, 127002. [Google Scholar] [CrossRef] [PubMed]


| Variable | Women (n = 42) | Men (n = 54) | p-Value |
|---|---|---|---|
| Age (years) | 46.69 ± 11.62 | 50.51 ± 10.39 | 0.09 |
| BMI (kg/m2) | 28.35 ± 8.22 | 30.19 ± 6.51 | 0.22 |
| SBP (mmHg) | 109.47 ± 14.98 | 123.09 ± 13.97 | 1.0 × 10−5 |
| DBP (mmHg) | 71.79 ± 9.17 | 78.52 ± 9.23 | 4.7 × 10−4 |
| TC (mg/dL) | 191.70 ± 36.73 | 180.81 ± 36.65 | 0.18 |
| HDL-C (mg/dL) | 49.24 ± 12.39 | 39.81 ± 11.43 | 1.0 × 10−3 |
| LDL-C (mg/dL) | 116.09 ± 31.72 | 106.56 ± 32.46 | 0.19 |
| TG (mg/dL) | 129.70 ± 61.20 | 177.95 ± 101.28 | 0.01 |
| FPG (mg/dL) | 95.56 ± 10.26 | 99.31 ± 10.21 | 0.10 |
| FPI (µU/mL) | 8.48 ± 7.15 | 9.51 ± 6.16 | 0.45 |
| HOMA-IR | 2.01 ± 1.80 | 2.68 ± 2.70 | 0.21 |
| Se (µg dL−1) | 10.87 ± 3.11 | 9.84 ± 2.90 | 0.09 |
| Overweight n (%) | 8 (19.0) | 11 (20.4) | 0.32 |
| Obesity n (%) | 16 (38.1) | 27 (50.0) |
| Variable | Spearman Correlation Coefficients |
|---|---|
| BMI (kg/m2) | 0.09 (0.37) |
| SBP (mmHg) | −0.13 (0.18) |
| DBP (mmHg) | −0.14 (0.15) |
| TC (mg/dL) | 0.06 (0.59) |
| HDL-C (mg/dL) | 0.11 (0.30) |
| LDL-C (mg/dL) | 0.149 (0.18) |
| TG (mg/dL) | −0.02 (0.84) |
| FPG (mg/dL) | −0.24 (0.02) |
| FPI (µU/mL) | −0.15 (0.14) |
| HOMA-IR | −0.16 (0.15) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rios-Lugo, M.J.; Palos-Lucio, A.G.; Victoria-Campos, C.I.; Lugo-Trampe, A.; Trujillo-Murillo, K.D.C.; López-García, M.A.; Espinoza-Ruiz, M.; Romero-Guzmán, E.T.; Hernández-Mendoza, H.; Chang-Rueda, C. Sex-Specific Association between Fasting Plasma Glucose and Serum Selenium Levels in Adults from Southern Mexico. Healthcare 2022, 10, 1665. https://doi.org/10.3390/healthcare10091665
Rios-Lugo MJ, Palos-Lucio AG, Victoria-Campos CI, Lugo-Trampe A, Trujillo-Murillo KDC, López-García MA, Espinoza-Ruiz M, Romero-Guzmán ET, Hernández-Mendoza H, Chang-Rueda C. Sex-Specific Association between Fasting Plasma Glucose and Serum Selenium Levels in Adults from Southern Mexico. Healthcare. 2022; 10(9):1665. https://doi.org/10.3390/healthcare10091665
Chicago/Turabian StyleRios-Lugo, María Judith, Ana Gabriela Palos-Lucio, Claudia Inés Victoria-Campos, Angel Lugo-Trampe, Karina Del Carmen Trujillo-Murillo, Maximiliano Arahon López-García, Marisol Espinoza-Ruiz, Elizabeth Teresita Romero-Guzmán, Héctor Hernández-Mendoza, and Consuelo Chang-Rueda. 2022. "Sex-Specific Association between Fasting Plasma Glucose and Serum Selenium Levels in Adults from Southern Mexico" Healthcare 10, no. 9: 1665. https://doi.org/10.3390/healthcare10091665