
The Importance of Behavioral and Native Factors on COVID-19 Infection and Severity: Insights from a Preliminary Cross-Sectional Study

 , , ,
, , ,  ,
,  , and
, and
Abstract
:1. Introduction
1.1. Background
1.2. Literature Review on the Main Risk Factors
1.2.1. Physical Activity
1.2.2. Age
1.2.3. Resistance (Immunity)
1.2.4. The Continent of Residence
1.2.5. Ethnicity
1.2.6. Blood Group
1.2.7. Observance of Protective Measures
1.2.8. Educational Attainment
1.2.9. Tobacco
1.2.10. Alcohol
1.2.11. Gender
1.3. Aims and Importance of Research
2. Materials and Methods
2.1. Overview
2.2. Development of the Questionnaire
2.3. Statistical Analysis
- The dependence of having been affected before or not by COVID-19 on the potential risk factors investigated was analyzed using logistic regression, a statistical method modeling a binary event as the probability of its occurrence.
- The dependence of the severity of infection on potential risk factors investigated was also analyzed using logistic regression after eliminating healthy subjects from the analysis and turning the “Severity” variable into a binary one, which indicates if the patient needs treatment or intensive care.
3. Results
3.1. Descriptive Statistics
3.2. Data Analysis
4. Discussion
4.1. Significance of the Results and Health Recommendations
4.2. Importance of the Study
4.3. Methodological Limitations
- (i).
- Integrating vaccination as a protective measure rather than as a factor in its own right when carrying out this sampling was not a limiting factor; time has shown that this is the case now; it was impossible at the time of developing the study, given the non-democratization of vaccinations at this time. For example, vaccination started in France on 27 December 2020 [155], on 29 December 2020 in Argentina [156], on 19 January 2021 in India [157], and on 10 February, Algeria [158].
- (ii).
- There could also be biases among social media users. For example, only 36% of Facebook users are over 35 years old [159].
- (iii).
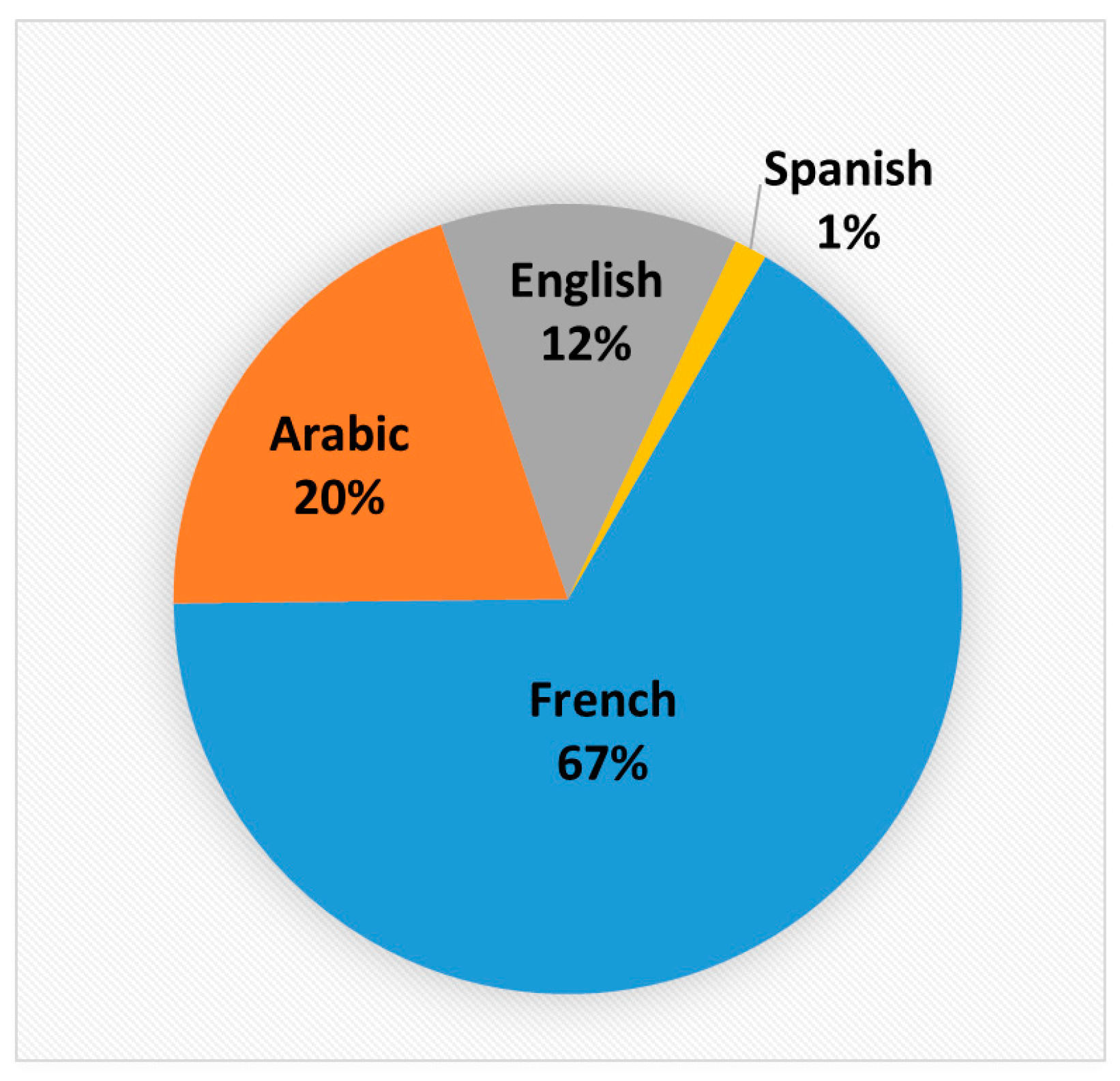
- The same remark is valid regarding the languages. More than 60% of our sample answered the study in French, which could suggest that they are mainly located in the MENA region and French-speaking Europe or the possible presence of migrants.
4.4. Perspectives for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cui, J.; Li, F.; Shi, Z.-L. Origin and evolution of pathogenic coronaviruses. Nat. Rev. Microbiol. 2019, 17, 181–192. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.; Sirajuddin, A.; Zhang, X.; Liu, G.; Teng, Z.; Zhao, S.; Lu, M. The role of imaging in 2019 novel coronavirus pneumonia (COVID-19). Eur. Radiol. 2020, 30, 4874–4882. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Feng, Z.; Li, P.; Yu, Q. Relationship between ABO blood group distribution and clinical characteristics in patients with COVID-19. Clin. Chim. Acta 2020, 509, 220–223. [Google Scholar] [CrossRef]
- Yasuhara, J.; Kuno, T.; Takagi, H.; Sumitomo, N. Clinical characteristics of COVID-19 in children: A systematic review. Pediatr. Pulmonol. 2020, 55, 2565–2575. [Google Scholar] [CrossRef]
- Deng, S.-Q.; Peng, H.-J. Characteristics of and Public Health Responses to the Coronavirus Disease 2019 Outbreak in China. J. Clin. Med. 2020, 9, 575. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Novel Coronavirus (2019-nCoV) Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 7 July 2022).
- Van Damme, W.; Dahake, R.; Delamou, A.; Ingelbeen, B.; Wouters, E.; Vanham, G.; Van De Pas, R.; Dossou, J.-P.; Ir, P.; Abimbola, S.; et al. The COVID-19 pandemic: Diverse contexts; different epidemics—how and why? BMJ Glob. Health 2020, 5, e003098. [Google Scholar] [CrossRef]
- Wong, J.; Goh, Q.Y.; Tan, Z.; Lie, S.A.; Tay, Y.C.; Ng, S.Y.; Soh, C.R. Preparing for a COVID-19 pandemic: A review of operating room outbreak response measures in a large tertiary hospital in Singapore. Can. J. Anaesth. 2020, 67, 732–745. [Google Scholar] [CrossRef] [Green Version]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Balanzá-Martínez, V.; Kapczinski, F.; Cardoso, T.D.A.; Atienza-Carbonell, B.; Rosa, A.R.; Mota, J.C.; De Boni, R.B. The assessment of lifestyle changes during the COVID-19 pandemic using a multidimensional scale. Rev. Psiquiatr. Y Salud Ment. 2020, 14, 16–26. [Google Scholar] [CrossRef]
- Garre-Olmo, J.; Turró-Garriga, O.; Martí-Lluch, R.; Zacarías-Pons, L.; Alves-Cabratosa, L.; Serrano-Sarbosa, D.; Vilalta-Franch, J.; Ramos, R.; Manté, X.A.; Casedevall, J.B.; et al. Changes in lifestyle resulting from confinement due to COVID-19 and depressive symptomatology: A cross-sectional a population-based study. Compr. Psychiatry 2020, 104, 152214. [Google Scholar] [CrossRef]
- Geldsetzer, P. Knowledge and Perceptions of COVID-19 Among the General Public in the United States and the United Kingdom: A Cross-sectional Online Survey. Ann. Intern. Med. 2020, 173, 157–160. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, A.; Ranjan, P.; Rohilla, P.; Saikaustubh, Y.; Sahu, A.; Dwivedi, S.N.; Baitha, U.; Kumar, A. Development and validation of a questionnaire to assess preventive practices against COVID-19 pandemic in the general population. Prev. Med. Rep. 2021, 22, 101339. [Google Scholar] [CrossRef]
- Pan, K.-Y.; Kok, A.A.L.; Eikelenboom, M.; Horsfall, M.; Jörg, F.; Luteijn, R.A.; Rhebergen, D.; van Oppen, P.; Giltay, E.J.; Penninx, B.W.J.H. The mental health impact of the COVID-19 pandemic on people with and without depressive, anxiety, or obsessive-compulsive disorders: A longitudinal study of three Dutch case-control cohorts. Lancet Psychiatry 2021, 8, 121–129. [Google Scholar] [CrossRef]
- Chopra, S.; Ranjan, P.; Malhotra, A.; Sahu, A.; Dwivedi, S.; Baitha, U.; Goel, A.; Kumar, A. Development and validation of a questionnaire to evaluate the impact of COVID-19 on lifestyle-related behaviours: Eating habits, activity and sleep behaviour. Public Health Nutr. 2020, 24, 1275–1290. [Google Scholar] [CrossRef]
- Yan, S.; Xu, R.; Stratton, T.D.; Kavcic, V.; Luo, D.; Hou, F.; Bi, F.; Jiao, R.; Song, K.; Jiang, Y. Sex differences and psychological stress: Responses to the COVID-19 pandemic in China. BMC Public Health 2021, 21, 79. [Google Scholar] [CrossRef]
- Kobayashi, L.C.; O’Shea, B.Q.; Kler, J.S.; Nishimura, R.; Palavicino-Maggio, C.B.; Eastman, M.R.; Vinson, Y.R.; Finlay, J.M. Cohort profile: The COVID-19 Coping Study, a longitudinal mixed-methods study of middle-aged and older adults’ mental health and well-being during the COVID-19 pandemic in the USA. BMJ Open 2021, 11, e044965. [Google Scholar] [CrossRef]
- Moulin, F.; El-Aarbaoui, T.; Bustamante, J.J.H.; Héron, M.; Mary-Krause, M.; Rouquette, A.; Galéra, C.; Melchior, M. Risk and protective factors related to children’s symptoms of emotional difficulties and hyperactivity/inattention during the COVID-19-related lockdown in France: Results from a community sample. Eur. Child Adolesc. Psychiatry 2021, 1–12. [Google Scholar] [CrossRef]
- Zhou, F.; You, C.; Zhang, X.; Qian, K.; Hou, Y.; Gao, Y.; Zhou, X.-H. Epidemiological Characteristics and Factors Associated with Critical Time Intervals of COVID-19 in Eighteen Provinces, China: A Retrospective Study. Int. J. Infect. Dis. 2020, 102, 123–131. [Google Scholar] [CrossRef]
- Wolff, D.; Nee, S.; Hickey, N.S.; Marschollek, M. Risk factors for Covid-19 severity and fatality: A structured literature review. Infection 2020, 49, 15–28. [Google Scholar] [CrossRef]
- Wong, C.-M.; Lai, H.-K.; Ou, C.-Q.; Ho, D.S.Y.; Chan, K.-P.; Thach, T.Q.; Yang, L.; Chau, Y.-K.; Lam, T.H.; Hedley, A.J.; et al. Is Exercise Protective Against Influenza-Associated Mortality? PLoS ONE 2008, 3, e2108. [Google Scholar] [CrossRef] [Green Version]
- Lowder, T.; Padgett, D.A.; Woods, J.A. Moderate exercise protects mice from death due to influenza virus. Brain Behav. Immun. 2005, 19, 377–380. [Google Scholar] [CrossRef]
- Zimmer, P.; Schenk, A.; Kieven, M.; Holthaus, M.; Lehmann, J.; Lövenich, L.; Bloch, W. Exercise induced alterations in NK-cell cytotoxicity-methodological issues and future perspectives. Exerc. Immunol. Rev. 2017, 23, 66–81. [Google Scholar]
- Wackerhage, H.; Everett, R.; Krüger, K.; Murgia, M.; Simon, P.; Gehlert, S.; Neuberger, E.; Baumert, P.; Schönfelder, M. Sport, exercise and COVID-19, the disease caused by the SARS-CoV-2 coronavirus. Dtsch Z Sportmed 2020, 71, E1–E12. [Google Scholar] [CrossRef]
- Narici, M.; De Vito, G.; Franchi, M.; Paoli, A.; Moro, T.; Marcolin, G.; Grassi, B.; Baldassarre, G.; Zuccarelli, L.; Biolo, G.; et al. Impact of sedentarism due to the COVID-19 home confinement on neuromuscular, cardiovascular and metabolic health: Physiological and pathophysiological implications and recommendations for physical and nutritional countermeasures. Eur. J. Sport Sci. 2021, 21, 614–635. [Google Scholar] [CrossRef]
- Hammami, A.; Harrabi, B.; Mohr, M.; Krustrup, P. Physical activity and coronavirus disease 2019 (COVID-19): Specific recommendations for home-based physical training. Manag. Sport Leis. 2020, 27, 26–31. [Google Scholar] [CrossRef]
- Polero, P.; Rebollo-Seco, C.; Adsuar, J.C.; Pérez-Gómez, J.; Rojo-Ramos, J.; Manzano-Redondo, F.; Garcia-Gordillo, M.; Carlos-Vivas, J. Physical Activity Recommendations during COVID-19: Narrative Review. Int. J. Environ. Res. Public Health 2020, 18, 65. [Google Scholar] [CrossRef]
- Wang, Y.; Pang, S.-C.; Yang, Y. A potential association between immunosenescence and high COVID-19 related mortality among elderly patients with cardiovascular diseases. Immun. Ageing 2021, 18, 25. [Google Scholar] [CrossRef]
- Porcheddu, R.; Serra, C.; Kelvin, D.; Kelvin, N.; Rubino, S. Similarity in Case Fatality Rates (CFR) of COVID-19/SARS-COV-2 in Italy and China. J. Infect. Dev. Ctries 2020, 14, 125–128. [Google Scholar] [CrossRef]
- Bonanad, C.; García-Blas, S.; Tarazona-Santabalbina, F.; Sanchis, J.; Bertomeu-González, V.; Fácila, L.; Ariza, A.; Núñez, J.; Cordero, A. The Effect of Age on Mortality in Patients With COVID-19: A Meta-Analysis With 611,583 Subjects. J. Am. Med. Dir. Assoc. 2020, 21, 915–918. [Google Scholar] [CrossRef]
- Aouissi, H.; Belhaouchet, I. What about rheumatic diseases and COVID-19? New Microbes New Infect. 2021, 41, 100846. [Google Scholar] [CrossRef]
- Cox, L.S.; Bellantuono, I.; Lord, J.M.; Sapey, E.; Mannick, J.B.; Partridge, L.; Gordon, A.L.; Steves, C.J.; Witham, M.D. Tackling immunosenescence to improve COVID-19 outcomes and vaccine response in older adults. Lancet Health Longev. 2020, 1, e55–e57. [Google Scholar] [CrossRef]
- Genebat, M.; Tarancón-Díez, L.; de Pablo-Bernal, R.; Calderón, A.; Muñoz-Fernández, M.; Leal, M. Coronavirus Disease (COVID-19): A Perspective from Immunosenescence. Aging Dis. 2021, 12, 3–6. [Google Scholar] [CrossRef]
- Pietrobon, A.J.; Teixeira, F.M.E.; Sato, M.N. I mmunosenescence and Inflammaging: Risk Factors of Severe COVID-19 in Older People. Front. Immunol. 2020, 11, 579220. [Google Scholar] [CrossRef]
- Sasson, I. Age and COVID-19 mortality: A comparison of Gompertz doubling time across countries and causes of death. Demogr. Res. 2021, 44, 379–396. [Google Scholar] [CrossRef]
- Lim, M.Q.; Kumaran, E.; Tan, H.C.; Lye, D.; Leo, Y.S.; Ooi, E.E.; Macary, P.A.; Bertoletti, A.; Rivino, L. Cross-Reactivity and Anti-viral Function of Dengue Capsid and NS3-Specific Memory T Cells toward Zika Virus. Front. Immunol. 2018, 9, 2225. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Bastard, P.; Liu, Z.; Le Pen, J.; Moncada-Velez, M.; Chen, J.; Ogishi, M.; Sabli, I.K.D.; Hodeib, S.; Korol, C.; et al. Inborn errors of type I IFN immunity in patients with life-threatening COVID-19. Science 2020, 370, eabd4570. [Google Scholar] [CrossRef]
- Bastard, P.; Rosen, L.B.; Zhang, Q.; Michailidis, E.; Hoffmann, H.-H.; Zhang, Y.; Dorgham, K.; Philippot, Q.; Rosain, J.; Béziat, V.; et al. Auto-antibodies against type I IFNs in patients with life-threatening COVID-19. Science 2020, 370, eabd4585. [Google Scholar] [CrossRef]
- Le Bert, N.; Tan, A.T.; Kunasegaran, K.; Tham, C.Y.L.; Hafezi, M.; Chia, A.; Chng, M.H.Y.; Lin, M.; Tan, N.; Linster, M.; et al. SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Nature 2020, 584, 457–462. [Google Scholar] [CrossRef]
- Van Damme, W.; Dahake, R.; van de Pas, R.; Vanham, G.; Assefa, Y. COVID-19: Does the infectious inoculum dose-response relationship contribute to understanding heterogeneity in disease severity and transmission dynamics? Med. Hypotheses 2020, 146, 110431. [Google Scholar] [CrossRef]
- Fakhroo, A.D.; Al Thani, A.A.; Yassine, H.M. Markers Associated with COVID-19 Susceptibility, Resistance, and Severity. Viruses 2020, 13, 45. [Google Scholar] [CrossRef]
- Aouissi, H.A.; Ababsa, M.; Gaagai, A. Review of a controversial treatment method in the fight against COVID-19 with the example of Algeria. Bull. Natl. Res. Cent. 2021, 45, 94. [Google Scholar] [CrossRef]
- An, B.Y.; Tang, S.-Y. Lessons From COVID-19 Responses in East Asia: Institutional Infrastructure and Enduring Policy Instruments. Am. Rev. Public Adm. 2020, 50, 790–800. [Google Scholar] [CrossRef]
- Xu, T. Media, Trust in Government, and Risk Perception of COVID-19 in the Early Stage of Epidemic: An Analysis Based on Moderating Effect. Healthcare 2021, 9, 1597. [Google Scholar] [CrossRef]
- Ababsa, M.; Aouissi, H.A. Current State of the Coronavirus (Covid-19) in Algeria. J. Community Med. Health Care 2020, 5, 1036. [Google Scholar] [CrossRef]
- McKenzie, G.; Adams, B. A country comparison of place-based activity response to COVID-19 policies. Appl. Geogr. 2020, 125, 102363. [Google Scholar] [CrossRef]
- Bhopal, R.S. Migration, Ethnicity, Race, and Health in Multicultural Societies; Oxford University Press: Oxford, UK, 2014. [Google Scholar]
- Yancy, C.W. COVID-19 and African Americans. JAMA 2020, 323, 1891. [Google Scholar] [CrossRef] [Green Version]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Katikireddi, S.V.; Lal, S.; Carrol, E.D.; Niedzwiedz, C.L.; Khunti, K.; Dundas, R.; Diderichsen, F.; Barr, B. Unequal impact of the COVID-19 crisis on minority ethnic groups: A framework for understanding and addressing inequalities. J. Epidemiol. Community Health 2021, 75, 970–974. [Google Scholar] [CrossRef]
- Sze, S.; Pan, D.; Nevill, C.R.; Gray, L.J.; Martin, C.A.; Nazareth, J.; Minhas, J.S.; Divall, P.; Khunti, K.; Abrams, K.R.; et al. Ethnicity and clinical outcomes in COVID-19: A systematic review and meta-analysis. EClinicalMedicine 2020, 29, 100630. [Google Scholar] [CrossRef]
- Vist, G.E.; Arentz-Hansen, E.H.; Vedøy, T.F.; Spilker, R.A.C.S.; Hafstad, E.V.; Giske, L. Incidence and Severe Outcomes from COVID-19 among Immigrant and Minority Ethnic Groups and among Groups of Different Socio-Economic Status: A Systematic Review. Available online: https://hdl.handle.net/11250/2754026 (accessed on 7 July 2022).
- Nacher, M.; Rousseau, C.; Succo, T.; Andrieu, A.; Gaillet, M.; Michaud, C.; Servas, V.; Douine, M.; Schaub, R.; Adenis, A.; et al. The Epidemiology of COVID 19 in the Amazon and the Guianas: Similarities, Differences, and International Comparisons. Front. Public Health 2021, 9, 586299. [Google Scholar] [CrossRef]
- Li, J.; Wang, X.; Chen, J.; Cai, Y.; Deng, A.; Yang, M. Association between ABO blood groups and risk of SARS-CoV-2 pneumonia. Br. J. Haematol. 2020, 190, 24–27. [Google Scholar] [CrossRef]
- Anderson, J.L.; May, H.T.; Knight, S.; Bair, T.L.; Muhlestein, J.B.; Knowlton, K.U.; Horne, B.D. Association of Sociodemographic Factors and Blood Group Type With Risk of COVID-19 in a US Population. JAMA Netw. Open 2021, 4, e217429. [Google Scholar] [CrossRef]
- Goel, R.; Bloch, E.M.; Pirenne, F.; Al-Riyami, A.Z.; Crowe, E.; Dau, L.; Land, K.; Townsend, M.; Jecko, T.; Rahimi-Levene, N.; et al. ABO blood group and COVID-19: A review on behalf of the ISBT COVID-19 Working Group. Vox Sang. 2021, 116, 849–861. [Google Scholar] [CrossRef]
- Miotto, M.; Di Rienzo, L.; Gosti, G.; Milanetti, E.; Ruocco, G. Does blood type affect the COVID-19 infection pattern? PLoS ONE 2021, 16, e0251535. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Protect Yourself: Coronavirus Disease (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html (accessed on 4 February 2021).
- Oshio, T.; Kan, M. Educational level as a predictor of the incidences of non-communicable diseases among middle-aged Japanese: A hazards-model analysis. BMC Public Health 2019, 19, 852. [Google Scholar] [CrossRef]
- Concepción-Zavaleta, M.J.; Coronado-Arroyo, J.C.; Zavaleta-Gutiérrez, F.E.; Concepción-Urteaga, L.A. Does level of education influence mortality of SARS-CoV-2 in a developing country? Int. J. Epidemiol. 2020, 49, 2091–2093. [Google Scholar] [CrossRef]
- Priyadarsini, S.L.; Suresh, M. Factors influencing the epidemiological characteristics of pandemic COVID 19: A TISM approach. Int. J. Health Manag. 2020, 13, 89–98. [Google Scholar] [CrossRef] [Green Version]
- Millett, G.A.; Jones, A.T.; Benkeser, D.; Baral, S.; Mercer, L.; Beyrer, C.; Honermann, B.; Lankiewicz, E.; Mena, L.; Crowley, J.S.; et al. Assessing differential impacts of COVID-19 on black communities. Ann. Epidemiol. 2020, 47, 37–44. [Google Scholar] [CrossRef]
- Margolis, R. Educational Differences in Healthy Behavior Changes and Adherence among Middle-aged Americans. J. Health Soc. Behav. 2013, 54, 353–368. [Google Scholar] [CrossRef] [Green Version]
- Friis, K.; Lasgaard, M.; Rowlands, G.; Osborne, R.; Maindal, H.T. Health Literacy Mediates the Relationship Between Educational Attainment and Health Behavior: A Danish Population-Based Study. J. Health Commun. 2016, 21 (Suppl. S2), 54–60. [Google Scholar] [CrossRef]
- Upshaw, T.L.; Brown, C.; Smith, R.; Perri, M.; Ziegler, C.; Pinto, A.D. Social determinants of COVID-19 incidence and outcomes: A rapid review. PLoS ONE 2021, 16, e0248336. [Google Scholar] [CrossRef]
- Lee, J.; Lim, H.; Allen, J.; Choi, G. Effects of Learning Attitudes and COVID-19 Risk Perception on Poor Academic Performance among Middle School Students. Sustainability 2021, 13, 5541. [Google Scholar] [CrossRef]
- Islam, F.M.A.; Walton, A. Tobacco Smoking and Use of Smokeless Tobacco and Their Association with Psychological Distress and Other Factors in a Rural District in Bangladesh: A Cross-Sectional Study. J. Environ. Public Health 2019, 2019, 1424592. [Google Scholar] [CrossRef]
- Yingst, J.M.; Krebs, N.M.; Bordner, C.R.; Hobkirk, A.L.; Allen, S.I.; Foulds, J. Tobacco Use Changes and Perceived Health Risks among Current Tobacco Users during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 1795. [Google Scholar] [CrossRef]
- Kim, L.; Garg, S.; O’Halloran, A.; Whitaker, M.; Pham, H.; Anderson, E.J.; Armistead, I.; Bennett, N.M.; Billing, L.; Como-Sabetti, K.; et al. Risk Factors for Intensive Care Unit Admission and In-hospital Mortality Among Hospitalized Adults Identified through the US Coronavirus Disease 2019 (COVID-19)-Associated Hospitalization Surveillance Network (COVID-NET). Clin. Infect. Dis. 2020, 72, e206–e214. [Google Scholar] [CrossRef]
- Ko, J.Y.; Danielson, M.L.; Town, M.; Derado, G.; Greenlund, K.J.; Kirley, P.D.; Alden, N.B.; Yousey-Hindes, K.; Anderson, E.J.; A Ryan, P.; et al. Risk Factors for Coronavirus Disease 2019 (COVID-19)–Associated Hospitalization: COVID-19–Associated Hospitalization Surveillance Network and Behavioral Risk Factor Surveillance System. Clin. Infect. Dis. 2020, 72, e695–e703. [Google Scholar] [CrossRef]
- Berlin, I.; Thomas, D.; Le Faou, A.-L.; Cornuz, J. COVID-19 and Smoking. Nicotine Tob. Res. 2020, 22, 1650–1652. [Google Scholar] [CrossRef] [Green Version]
- Mistry, S.K.; Ali, A.M.; Rahman, A.; Yadav, U.N.; Gupta, B.; Rahman, M.A.; Huque, R. Changes in Tobacco Use Patterns During COVID-19 and Their Correlates among Older Adults in Bangladesh. Int. J. Environ. Res. Public Health 2021, 18, 1779. [Google Scholar] [CrossRef]
- Simou, E.; Britton, J.; Leonardi-Bee, J. Alcohol and the risk of pneumonia: A systematic review and meta-analysis. BMJ Open 2018, 8, e022344. [Google Scholar] [CrossRef] [Green Version]
- Abuga, K.; Nyamweya, N. Alcohol-Based Hand Sanitizers in COVID-19 Prevention: A Multidimensional Perspective. Pharmacy 2021, 9, 64. [Google Scholar] [CrossRef]
- Da, B.L.; Im, G.Y.; Schiano, T.D. Coronavirus Disease 2019 Hangover: A Rising Tide of Alcohol Use Disorder and Alcohol-Associated Liver Disease. Hepatology 2020, 72, 1102–1108. [Google Scholar] [CrossRef]
- Testino, G. Are Patients With Alcohol Use Disorders at Increased Risk for Covid-19 Infection? Alcohol Alcohol. 2020, 55, 344–346. [Google Scholar] [CrossRef]
- Heidari, M.; Sayfouri, N. COVID-19 and Alcohol Poisoning: A Fatal Competition. Disaster Med. Public Health Prep. 2021, 1–3. [Google Scholar] [CrossRef]
- Hassanian-Moghaddam, H.; Pajoumand, A.; Dadgar, S.; Shadnia, S. Prognostic factors in methanol poisoning. Hum. Exp. Toxicol. 2007, 26, 583–586. [Google Scholar] [CrossRef]
- Lassen, M.C.H.; Skaarup, K.G.; Sengeløv, M.; Iversen, K.; Ulrik, C.S.; Jensen, J.U.S.; Biering-Sørensen, T. Alcohol Consumption and the Risk of Acute Respiratory Distress Syndrome in COVID-19. Ann. Am. Thorac. Soc. 2021, 18, 1074–1076. [Google Scholar] [CrossRef]
- Dehingia, N.; Raj, A. Sex differences in COVID-19 case fatality: Do we know enough? Lancet Glob. Health 2020, 9, e14–e15. [Google Scholar] [CrossRef]
- Judah, G.; Aunger, R.; Schmidt, W.P.; Michie, S.; Granger, S.; Curtis, V. Experimental pretesting of hand-washing interventions in a natural setting. Am. J. Public Health 2009, 99, S405–S411. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef]
- Raimondi, F.; Novelli, L.; Ghirardi, A.; Russo, F.M.; Pellegrini, D.; Biza, R.; Trapasso, R.; Giuliani, L.; Anelli, M.; Amoroso, M.; et al. Covid-19 and gender: Lower rate but same mortality of severe disease in women—An observational study. BMC Pulm. Med. 2021, 21, 96. [Google Scholar] [CrossRef]
- Joe, W.; Kumar, A.; Rajpal, S.; Mishra, U.; Subramanian, S. Equal risk, unequal burden? Gender differentials in COVID-19 mortality in India. J. Glob. Health Sci. 2020, 2, e17. [Google Scholar] [CrossRef]
- Bhopal, S.S.; Bhopal, R. Sex differential in COVID-19 mortality varies markedly by age. Lancet 2020, 396, 532–533. [Google Scholar] [CrossRef]
- Combessie, J.C. La méthode de Sociologie, Chapter 4. Sondages, échantillons. In Reperes; La découverte: Paris, France, 2007; Volume 5, pp. 45–54. [Google Scholar]
- Arora, C. Development and Validation of Health Education Tools and Evaluation Questionnaires for Improving Patient Care in Lifestyle Related Diseases. J. Clin. Diagn. Res. 2017, 11, JE06–JE09. [Google Scholar] [CrossRef]
- Ranjan, P.; Reethesh, S.; Arora, C.; Kaloiya, G.; Vikram, N.K.; Dwivedi, S.N.; Jyotsna, V.P.; Soneja, M. Development and validation of a questionnaire assessing knowledge, attitude, and practices about obesity among obese individuals. Indian J. Endocrinol. Metab. 2019, 23, 102–110. [Google Scholar] [CrossRef]
- Pereltsvaig, A. Languages of the World: An Introduction, 2nd ed.; Cambridge University Press: Cambridge, UK, 2017. [Google Scholar] [CrossRef]
- Sawik, B.; Płonka, J. Project and Prototype of Mobile Application for Monitoring the Global COVID-19 Epidemiological Situation. Int. J. Environ. Res. Public Health 2022, 19, 1416. [Google Scholar] [CrossRef]
- Kong, Y.; Jiang, H.; Liu, Z.; Guo, Y.; Hu, D. The Uptake and Vaccination Willingness of COVID-19 Vaccine among Chinese Residents: Web-Based Online Cross-Sectional Study. Vaccines 2022, 10, 90. [Google Scholar] [CrossRef]
- Thornton, L.; Batterham, P.J.; Fassnacht, D.B.; Kay-Lambkin, F.; Calear, A.L.; Hunt, S. Recruiting for health, medical or psychosocial research using Facebook: Systematic review. Internet Interv. 2016, 4, 72–81. [Google Scholar] [CrossRef] [Green Version]
- Schneider, D.; Harknett, K. What’s to Like? Facebook as a Tool for Survey Data Collection. Sociol. Methods Res. 2019, 51, 108–140. [Google Scholar] [CrossRef] [Green Version]
- Shaver, L.G.; Khawer, A.; Yi, Y.; Aubrey-Bassler, K.; Etchegary, H.; Roebothan, B.; Asghari, S.; Wang, P.P. Using Facebook Advertising to Recruit Representative Samples: Feasibility Assessment of a Cross-Sectional Survey. J. Med. Internet Res. 2019, 21, e14021. [Google Scholar] [CrossRef] [Green Version]
- Koinig, I. Picturing Mental Health on Instagram: Insights from a Quantitative Study Using Different Content Formats. Int. J. Environ. Res. Public Health 2022, 19, 1608. [Google Scholar] [CrossRef]
- Tricas-Vidal, H.J.; Vidal-Peracho, M.C.; Lucha-López, M.O.; Hidalgo-García, C.; Lucha-López, A.C.; Monti-Ballano, S.; Toro, J.C.-D.; Márquez-Gonzalvo, S.; Tricás-Moreno, J.M. Nutrition-Related Content on Instagram in the United States of America: Analytical Cross-Sectional Study. Foods 2022, 11, 239. [Google Scholar] [CrossRef]
- Liu, J.C.J.; Tong, E.M.W. The Relation Between Official WhatsApp-Distributed COVID-19 News Exposure and Psychological Symptoms: Cross-Sectional Survey Study. J. Med. Internet Res. 2020, 22, e22142. [Google Scholar] [CrossRef]
- Manji, K.; Hanefeld, J.; Vearey, J.; Walls, H.; de Gruchy, T. Using WhatsApp messenger for health systems research: A scoping review of available literature. Health Policy Plan. 2021, 36, 774–789. [Google Scholar] [CrossRef]
- Kühne, S.; Zindel, Z. Using Facebook and Instagram to Recruit Web Survey Participants: A Step-by-Step Guide and Application. Survey Methods: Insights from the Field (SMIF) Special Issue: ‘Advancements in Online and Mobile Survey Methods’ 2020. Available online: https://surveyinsights.org/?p=13558 (accessed on 7 July 2022).
- Hoffman, J.I.E. Logistic regression. In Basic Biostatistics for Medical and Biomedical Practitioners; Hoffman, J.I.E., Ed.; Academic Press: San Diego, CA, USA, 2019; pp. 581–589. [Google Scholar]
- Collett, D. Modelling Binary Data, 2nd ed.; Chapman & Hall/CRC: London, UK, 2003; p. 93. [Google Scholar] [CrossRef]
- Kebaili, F.K.; Baziz-Berkani, A.; Aouissi, H.A.; Mihai, F.-C.; Houda, M.; Ababsa, M.; Azab, M.; Petrisor, A.-I.; Fürst, C. Characterization and Planning of Household Waste Management: A Case Study from the MENA Region. Sustainability 2022, 14, 5461. [Google Scholar] [CrossRef]
- Subedi, D.; Pantha, S.; Subedi, S.; Gautam, A.; Gaire, A.; Sapkota, D.; Sapkota, S.; Kandel, M.; Parajuli, A.; Ghimire, H.; et al. Perceptions towards COVID-19 Vaccines and Willingness to Vaccinate in Nepal. Vaccines 2021, 9, 1448. [Google Scholar] [CrossRef]
- Carmagnola, D.; Toma, M.; Henin, D.; Perrotta, M.; Pellegrini, G.; Dellavia, C. Personal Protection Equipment and Infection Control Procedures among Health Workers during the COVID-19 Pandemic. Healthcare 2022, 10, 944. [Google Scholar] [CrossRef]
- Lipsitch, M.; Kahn, R. Interpreting vaccine efficacy trial results for infection and transmission. MedRxiv 2021. [Google Scholar] [CrossRef]
- Lounis, M.; Rais, M.A.; Bencherit, D.; Aouissi, H.A.; Oudjedi, A.; Klugarová, J.; Pokorná, A.; Klugar, M.; Riad, A. Side Effects of COVID-19 Inactivated Virus vs. Adenoviral Vector Vaccines: Experience of Algerian Healthcare Workers. Front. Public Health 2022, 10, 896343. [Google Scholar] [CrossRef]
- Abdulateef, D.S.; Rahman, H.S.; Salih, J.M.; Osman, S.M.; Mahmood, T.A.; Omer, S.H.S.; Ahmed, R.A. COVID-19 severity in relation to sociodemographics and vitamin D use. Open Med. 2021, 16, 591–609. [Google Scholar] [CrossRef]
- Sohn, M.; Koo, B.K.; Yoon, H.I.; Song, K.-H.; Kim, E.S.; Bin Kim, H.; Lim, S. Impact of COVID-19 and Associated Preventive Measures on Cardiometabolic Risk Factors in South Korea. J. Obes. Metab. Syndr. 2021, 30, 248–260. [Google Scholar] [CrossRef]
- Rana, M.S.; Usman, M.; Alam, M.M.; Ikram, A.; Salman, M.; Zaidi, S.S.Z.; Umair, M.; Qadir, M. Impact of COVID-19 preventive measures on other infectious and non-infectious respiratory diseases in Pakistan. J. Infect. 2021, 82, e31–e32. [Google Scholar] [CrossRef]
- Sugimura, M.; Chimed-Ochir, O.; Yumiya, Y.; Ohge, H.; Shime, N.; Sakaguchi, T.; Tanaka, J.; Takafuta, T.; Mimori, M.; Kuwabara, M.; et al. The Association between Wearing a Mask and COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 9131. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2020, 396, 1979–1993. [Google Scholar] [CrossRef]
- O’Driscoll, M.; Dos Santos, G.R.; Wang, L.; Cummings, D.A.T.; Azman, A.S.; Paireau, J.; Fontanet, A.; Cauchemez, S.; Salje, H. Age-specific mortality and immunity patterns of SARS-CoV-2. Nature 2021, 590, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Liao, X.; Zhou, Y.; Wang, L.; Yang, H.; Zhang, W.; Zhang, Z.; Kang, Y. Comparison of Associations Between Glucocorticoids Treatment and Mortality in COVID-19 Patients and SARS Patients: A Systematic Review and Meta-Analysis. Shock 2021, 56, 215–228. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.-D.; Ding, M.; Dong, X.; Zhang, J.-J.; Azkur, A.K.; Azkur, D.; Gan, H.; Sun, Y.-L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- McClain, C.; Vatsalya, V.; Cave, M. Role of Zinc in the Development/Progression of Alcoholic Liver Disease. Curr. Treat. Options Gastroenterol. 2017, 15, 285–295. [Google Scholar] [CrossRef]
- Hikida, S.; Morioka, S.; Fujii, N.; Tajima, T.; Terayama, Y.; Sugiura, Y.; Ishikane, M.; Takasaki, J.; Hojo, M.; Ohmagari, N. A single-center descriptive study of untraced sources of infection among new cases of coronavirus disease in Tokyo, Japan. Glob. Health Med. 2021, 3, 236–239. [Google Scholar] [CrossRef]
- González-Reimers, E.; Santolaria-Fernández, F.; Martín-González, M.C.; Fernández-Rodríguez, C.M.; Quintero-Platt, G. Alcoholism: A systemic proinflammatory condition. World J. Gastroenterol. 2014, 20, 14660–14671. [Google Scholar] [CrossRef]
- Dai, M.; Tao, L.; Chen, Z.; Tian, Z.; Guo, X.; Allen-Gipson, D.S.; Tan, R.; Li, R.; Chai, L.; Ai, F.; et al. Influence of Cigarettes and Alcohol on the Severity and Death of COVID-19: A Multicenter Retrospective Study in Wuhan, China. Front. Physiol. 2020, 11, 588553. [Google Scholar] [CrossRef]
- Murthy, P.; Narasimha, V.L. Effects of the COVID-19 pandemic and lockdown on alcohol use disorders and complications. Curr. Opin. Psychiatry 2021, 34, 376–385. [Google Scholar] [CrossRef]
- Saengow, U.; Assanangkornchai, S.; Casswell, S. Alcohol: A probable risk factor of COVID-19 severity. Addiction 2020, 116, 204–205. [Google Scholar] [CrossRef] [PubMed]
- Calina, D.; Hartung, T.; Mardare, I.; Mitroi, M.; Poulas, K.; Tsatsakis, A.; Rogoveanu, I.; Docea, A.O. COVID-19 pandemic and alcohol consumption: Impacts and interconnections. Toxicol. Rep. 2021, 8, 529–535. [Google Scholar] [CrossRef]
- Reddy, R.K.; Charles, W.N.; Sklavounos, A.; Dutt, A.; Seed, P.T.; Khajuria, A. The effect of smoking on COVID-19 severity: A systematic review and meta-analysis. J. Med. Virol. 2020, 93, 1045–1056. [Google Scholar] [CrossRef] [PubMed]
- Izcovich, A.; Ragusa, M.A.; Tortosa, F.; Marzio, M.A.L.; Agnoletti, C.; Bengolea, A.; Ceirano, A.; Espinosa, F.; Saavedra, E.; Sanguine, V.; et al. Prognostic factors for severity and mortality in patients infected with COVID-19: A systematic review. PLoS ONE 2020, 15, e0241955. [Google Scholar] [CrossRef] [PubMed]
- Simons, D.; Shahab, L.; Brown, J.; Perski, O. The association of smoking status with SARS-CoV-2 infection, hospitalization and mortality from COVID-19: A living rapid evidence review with Bayesian meta-analyses (version 7). Addiction 2021, 116, 1319–1368. [Google Scholar] [CrossRef] [PubMed]
- Rozhnova, G.; van Dorp, C.H.; Bruijning-Verhagen, P.; Bootsma, M.C.J.; van de Wijgert, J.H.H.M.; Bonten, M.J.M.; Kretzschmar, M.E. Model-based evaluation of school- and non-school-related measures to control the COVID-19 pandemic. Nat. Commun. 2021, 12, 1614. [Google Scholar] [CrossRef]
- Krishnaratne, S.; Pfadenhauer, L.M.; Coenen, M.; Geffert, K.; Jung-Sievers, C.; Klinger, C.; Kratzer, S.; Littlecott, H.; Movsisyan, A.; E Rabe, J.; et al. Measures implemented in the school setting to contain the COVID-19 pandemic: A rapid scoping review. Cochrane Database Syst. Rev. 2020, 2020, CD013812. [Google Scholar] [CrossRef]
- Zhao, Y.; Liang, W.; Luo, Y.; Chen, Y.; Liang, P.; Zhong, R.; Chen, A.; He, J. Personal protective equipment protecting healthcare workers in the Chinese epicentre of COVID-19. Clin. Microbiol. Infect. 2020, 26, 1716–1718. [Google Scholar] [CrossRef]
- Canet-Vélez, O.; Botigué, T.; Santamaría, A.L.; Masot, O.; Cemeli, T.; Roca, J. The perception of training and professional development according to nursing students as health workers during COVID-19: A qualitative study. Nurse Educ. Pract. 2021, 53, 103072. [Google Scholar] [CrossRef]
- Thomson, S. Achievement at school and socioeconomic background—An educational perspective. NPJ Sci. Learn. 2018, 3, 5. [Google Scholar] [CrossRef]
- Destin, M.; Hanselman, P.; Buontempo, J.; Tipton, E.; Yeager, D.S. Do Student Mindsets Differ by Socioeconomic Status and Explain Disparities in Academic Achievement in the United States? AERA Open 2019, 5, 2332858419857706. [Google Scholar] [CrossRef] [PubMed]
- Schultze, J.L.; Aschenbrenner, A.C. COVID-19 and the human innate immune system. Cell 2021, 184, 1671–1692. [Google Scholar] [CrossRef] [PubMed]
- Chumakov, K.; Avidan, M.S.; Benn, C.S.; Bertozzi, S.M.; Blatt, L.; Chang, A.Y.; Jamison, D.T.; Khader, S.A.; Kottilil, S.; Netea, M.G.; et al. Old vaccines for new infections: Exploiting innate immunity to control COVID-19 and prevent future pandemics. Proc. Natl. Acad. Sci. USA 2021, 118, e2101718118. [Google Scholar] [CrossRef] [PubMed]
- Kasuga, Y.; Zhu, B.; Jang, K.-J.; Yoo, J.-S. Innate immune sensing of coronavirus and viral evasion strategies. Exp. Mol. Med. 2021, 53, 723–736. [Google Scholar] [CrossRef] [PubMed]
- Franza, L.; Cianci, R. Pollution, Inflammation, and Vaccines: A Complex Crosstalk. Int. J. Environ. Res. Public Health 2021, 18, 6330. [Google Scholar] [CrossRef]
- Annweiler, C.; Sacco, G.; Salles, N.; Aquino, J.-P.; Gautier, J.; Berrut, G.; Guérin, O.; Gavazzi, G. National French Survey of Coronavirus Disease (COVID-19) Symptoms in People Aged 70 and Over. Clin. Infect. Dis. 2020, 72, 490–494. [Google Scholar] [CrossRef] [PubMed]
- Montagni, I.; Roussel, N.; Thiébaut, R.; Tzourio, C. Health Care Students’ Knowledge of and Attitudes, Beliefs, and Practices Toward the French COVID-19 App: Cross-sectional Questionnaire Study. J. Med. Internet Res. 2021, 23, e26399. [Google Scholar] [CrossRef]
- Nieto, R.; Pardo, R.; Sora, B.; Feliu-Soler, A.; Luciano, J. Impact of COVID-19 Lockdown Measures on Spanish People with Chronic Pain: An Online Study Survey. J. Clin. Med. 2020, 9, 3558. [Google Scholar] [CrossRef]
- Abdou, M.S.; Kheirallah, K.A.; Aly, M.O.; Ramadan, A.; Elhadi, Y.A.M.; Elbarazi, I.; Deghidy, E.A.; El Saeh, H.M.; Salem, K.M.; Ghazy, R.M. The coronavirus disease 2019 (COVID-19) vaccination psychological antecedent assessment using the Arabic 5c validated tool: An online survey in 13 Arab countries. PLoS ONE 2021, 16, e0260321. [Google Scholar] [CrossRef]
- Grover, S.; Sahoo, S.; Mehra, A.; Avasthi, A.; Tripathi, A.; Subramanyan, A.; Pattojoshi, A.; Rao, G.P.; Saha, G.; Mishra, K.; et al. Psychological impact of COVID-19 lockdown: An online survey from India. Indian J. Psychiatry 2020, 62, 354–362. [Google Scholar] [CrossRef]
- Ingram, C.; Chen, Y.; Buggy, C.; Downey, V.; Archibald, M.; Rachwal, N.; Roe, M.; Drummond, A.; Perrotta, C. Development and validation of a multi-lingual online questionnaire for surveying the COVID-19 prevention and control measures used in global workplaces. BMC Public Health 2022, 22, 74. [Google Scholar] [CrossRef] [PubMed]
- Cagetti, M.G.; Cairoli, J.L.; Senna, A. Guglielmo Campus COVID-19 Outbreak in North Italy: An Overview on Dentistry. A Questionnaire Survey. Int. J. Environ. Res. Public Health 2020, 17, 3835. [Google Scholar] [CrossRef] [PubMed]
- Algahtani, F.D.; Hassan, S.-u.-N.; Alsaif, B.; Zrieq, R. Assessment of the Quality of Life during COVID-19 Pandemic: A Cross-Sectional Survey from the Kingdom of Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 847. [Google Scholar] [CrossRef] [PubMed]
- Boutebal, S.E.; Madani, A.; Bryant, C.R. COVID-19 pandemic: Rapid survey on social and mobility impact in Algerian cities. J. Public Health 2021. [Google Scholar] [CrossRef] [PubMed]
- Medrano, M.; Cadenas-Sanchez, C.; Oses, M.; Arenaza, L.; Amasene, M.; Labayen, I. Changes in lifestyle behaviours during the COVID -19 confinement in Spanish children: A longitudinal analysis from the MUGI project. Pediatr. Obes. 2020, 16, e12731. [Google Scholar] [CrossRef]
- He, M.; Xian, Y.; Lv, X.; He, J.; Ren, Y. Changes in Body Weight, Physical Activity, and Lifestyle During the Semi-lockdown Period After the Outbreak of COVID-19 in China: An Online Survey. Disaster Med. Public Health Prep. 2020, 15, e23–e28. [Google Scholar] [CrossRef]
- Aldhuwayhi, S.; Mallineni, S.K.; Sakhamuri, S.; Thakare, A.A.; Mallineni, S.; Sajja, R.; Sethi, M.; Nettam, V.; Mohammad, A.M. Covid-19 Knowledge and Perceptions Among Dental Specialists: A Cross-Sectional Online Questionnaire Survey. Risk Manag. Health Policy 2021, 14, 2851–2861. [Google Scholar] [CrossRef]
- Swann, J. The Pharmaceutical Industries. In The Modern Biological and Earth Sciences; Pickstone, J.V., Bowler, P.J., Eds.; The Cambridge History of Science; Cambridge University Press: Cambridge, UK, 2009; Volume 6, pp. 126–140. ISBN 978-0-521-57201-9. [Google Scholar]
- Komal, A.; Noreen, M.; Akhtar, J.; Imran, M.; Jamal, M.; Atif, M.; Khan, J.; Roman, M.; Haq, F.U.; Aftab, U.; et al. Analyses of ABO blood groups with susceptibility and symptomatic variations of COVID-19 infection, a questionnaire-based survey. APMIS Acta Pathol. Microbiol. Immunol. Scand. 2021, 129, 579–586. [Google Scholar] [CrossRef]
- Coccia, M. Factors determining the diffusion of COVID-19 and suggested strategy to prevent future accelerated viral infectivity similar to COVID. Sci. Total Environ. 2020, 729, 138474. [Google Scholar] [CrossRef]
- Lim, Y.K.; Kweon, O.J.; Kim, H.R.; Kim, T.-H.; Lee, M.-K. The impact of environmental variables on the spread of COVID-19 in the Republic of Korea. Sci. Rep. 2021, 11, 5977. [Google Scholar] [CrossRef]
- Leveau, C.M.; Aouissi, H.A.; Kebaili, F.K. Spatial diffusion of COVID-19 in Algeria during the third wave. GeoJournal 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Jimenez, J.; Prather, K.A.; Tufekci, Z.; Fisman, D.; Schooley, R. Ten scientific reasons in support of airborne transmission of SARS-CoV-2. Lancet 2021, 397, 1603–1605. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Patel, M.; Chaubey, A.K.; Pittman, C.U.; Mlsna, T.; Mohan, D. Coronavirus (SARS-CoV-2) in the environment: Occurrence, persistence, analysis in aquatic systems and possible management. Sci. Total Environ. 2020, 765, 142698. [Google Scholar] [CrossRef] [PubMed]
- Pageaud, S.; Pothier, C.; Rigotti, C.; Eyraud-Loisel, A.; Bertoglio, J.-P.; Bienvenüe, A.; Leboisne, N.; Ponthus, N.; Gauchon, R.; Gueyffier, F.; et al. Expected Evolution of COVID-19 Epidemic in France for Several Combinations of Vaccination Strategies and Barrier Measures. Vaccines 2021, 9, 1462. [Google Scholar] [CrossRef]
- Urrunaga-Pastor, D.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Toro-Huamanchumo, C.J.; Rodriguez-Morales, A.J.; Hernandez, A.V.; Benites-Zapata, V.A.; Bendezu-Quispe, G. Prevalence and Factors Associated with Parents’ Non-Intention to Vaccinate Their Children and Adolescents against COVID-19 in Latin America and the Caribbean. Vaccines 2021, 9, 1303. [Google Scholar] [CrossRef]
- Umakanthan, S.; Patil, S.; Subramaniam, N.; Sharma, R. COVID-19 Vaccine Hesitancy and Resistance in India Explored through a Population-Based Longitudinal Survey. Vaccines 2021, 9, 1064. [Google Scholar] [CrossRef]
- Aouissi, H.A. Algeria’s preparedness for Omicron variant and for the fourth wave of COVID-19. Glob. Health Med. 2021, 3, 413–414. [Google Scholar] [CrossRef]
- Pang, P.; Cai, Q.; Jiang, W.; Chan, K. Engagement of Government Social Media on Facebook during the COVID-19 Pandemic in Macao. Int. J. Environ. Res. Public Health 2021, 18, 3508. [Google Scholar] [CrossRef]
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodés-Guirao, L. A global database of COVID-19 vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Answers | Sample | Percentage % |
|---|---|---|---|
| Continent of residence | Africa | 963 | 85.6% |
| Europe | 83 | 7.4% | |
| North America | 19 | 1.7% | |
| South America | 10 | 0.9% | |
| Asia | 48 | 4.3% | |
| Oceania | 2 | 0.2% | |
| Ethnic origin | Not precise | 13 | 1.2% |
| Other | 98 | 8.7% | |
| African/Afro-American | 126 | 11.2% | |
| Caucasian | 61 | 5.4% | |
| Arabic | 794 | 70.6% | |
| Asian | 22 | 2.0% | |
| Latino | 11 | 1.0% | |
| Gender | not precise | 7 | 0.6% |
| Male | 394 | 35.0% | |
| Female | 721 | 64.1% | |
| Other | 3 | 0.3% | |
| Age | 18–30 years | 727 | 64.6% |
| 31–45 | 315 | 28.0% | |
| 46–59 | 60 | 5.3% | |
| 60 | 23 | 2.0% | |
| Blood group | not precise | 13 | 1.2% |
| A+ | 344 | 30.6% | |
| A− | 21 | 1.9% | |
| B+ | 163 | 14.5% | |
| B− | 17 | 1.5% | |
| AB+ | 56 | 5.0% | |
| AB− | 8 | 0.7% | |
| O+ | 471 | 41.9% | |
| O− | 32 | 2.8% | |
| Educational attainment | Not precise | 0 | 0.0% |
| No study or primary | 67 | 6.0% | |
| Middle or secondary | 236 | 21.0% | |
| University or post-university | 820 | 73.0% | |
| Little or no activity | 557 | 49.6% | |
| Sports activity | Moderate | 451 | 40.2% |
| Very active | 114 | 10.2% | |
| Resistant (little or no flu/colds…) | 730 | 65.3% | |
| Health status | Moderately sensitive (regularly subject to flu/colds…) | 331 | 29.6% |
| Very sensitive (suffering from chronic disease(s) or others) | 57 | 5.1% | |
| No | 962 | 85.7% | |
| Tobacco use | Occasionally | 83 | 7.4% |
| Frequently | 78 | 6.9% | |
| No | 1025 | 91.4% | |
| Alcohol Consumption | Occasionally | 81 | 7.2% |
| Frequently | 16 | 1.4% | |
| Not at all | 65 | 5.8% | |
| Observance of protective measures | Medium application | 649 | 57.7% |
| Strict application | 411 | 36.5% | |
| Infection with COVID-19 | No | 790 | 70.4% |
| Yes | 332 | 29.6% | |
| Healthy (no infection) | 802 | 71.3% | |
| Infection state | Low (no special care) | 179 | 15.9% |
| Treatment and /or care | 130 | 11.6% | |
| Intensive care | 14 | 1.2% |
| Influence (Model) | Dependent Variable | |||||
|---|---|---|---|---|---|---|
| Infection | Severity | |||||
| Univariate | Full Model | Selected Model | Univariate | Full Model | Selected Model | |
| Continent | 0.3949 | 0.0891 | 0.2074 | 0.0888 | ||
| Ethnicity | 0.3217 | 0.1553 | 0.9307 | 0.6429 | ||
| Gender | 0.1654 | 0.7951 | 0.1088 | 0.7922 | ||
| Age | 0.0027 | 0.0185 | 0.0019 | 0.4958 | 0.6296 | |
| Blood | 0.0667 | 0.1869 | 0.4963 | 0.4590 | ||
| Education | 0.2661 | 0.5919 | 0.6485 | 0.6156 | ||
| Sports | 0.0009 | 0.0010 | 0.0005 | 0.1478 | 0.2808 | |
| Health | 0.0032 | 0.0919 | 0.0118 | 0.0723 | 0.1300 | |
| Tobacco | 0.0934 | 0.6743 | 0.0164 | 0.3364 | 0.0370 | |
| Alcohol | 0.1483 | 0.7615 | 0.1589 | 0.3068 | ||
| Protection | 0.4519 | 0.4083 | 0.0004 | 0.0042 | 0.0015 | |
| Variable | DF | Wald Chi-Square | p-Value | Level | OR Estimate | 95% Lower Wald Confidence Limit | 95% Upper Wald Confidence Limit |
|---|---|---|---|---|---|---|---|
| Continent | 3 | 6.5147 | 0.0891 | Africa vs. North America | 0.355 | 0.013 | 9.687 |
| Asia vs. North America | 0.691 | 0.014 | 34.708 | ||||
| Europe vs. North America | 2.781 | 0.083 | 92.650 | ||||
| Ethnicity | 4 | 6.6549 | 0.1553 | Other vs. Asian | 2.790 | 0.222 | 35.031 |
| African/Afro-American vs. Other | 2.198 | 0.154 | 31.419 | ||||
| Caucasian vs. Asian | 9.962 | 0.571 | 173.918 | ||||
| Arabic vs. Asian | 4.956 | 0.369 | 66.604 | ||||
| Gender | 1 | 0.0674 | 0.7951 | Male vs. Female | 1.089 | 0.571 | 2.076 |
| Age | 3 | 10.0082 | 0.0185 | 18–30 vs. 60+ | 13.133 | 1.238 | 139.335 |
| 31–45 vs. 60+ | 4.112 | 0.413 | 40.952 | ||||
| 46–59 vs. 60+ | 3.485 | 0.293 | 41.460 | ||||
| Blood | 7 | 10.0299 | 0.1869 | A+ vs. O− | 3.081 | 0.638 | 14.887 |
| A− vs. O− | <0.001 * | <0.001 * | >999.999 * | ||||
| B+ vs. O− | 1.192 | 0.224 | 6.338 | ||||
| B− vs. O− | 4.288 | 0.125 | 147.175 | ||||
| AB+ vs. O− | 9.939 | 1.106 | 89.323 | ||||
| AB− vs. O− | 0.474 | 0.010 | 22.533 | ||||
| O+ vs. O− | 2.720 | 0.569 | 12.987 | ||||
| Education | 2 | 1.0488 | 0.5919 | No study or primary vs. University/post-university | 1.401 | 0.514 | 3.820 |
| Middle/secondary vs. University/post-university | 1.535 | 0.597 | 3.947 | ||||
| Sports | 2 | 13.7657 | 0.0010 | Little or no activity vs. Very active | 2.729 | 0.978 | 7.620 |
| Moderate vs. Very active | 0.941 | 0.346 | 2.559 | ||||
| Health | 2 | 4.7731 | 0.0919 | Resistant vs. Very sensitive | 4.078 | 1.069 | 15.559 |
| Moderately sensitive vs. Very sensitive | 3.007 | 0.769 | 11.763 | ||||
| Tobacco | 2 | 0.7881 | 0.6743 | No vs. Frequently | 0.647 | 0.191 | 2.189 |
| Occasionally vs. Frequently | 0.531 | 0.131 | 2.155 | ||||
| Alcohol | 2 | 0.5448 | 0.7615 | No vs. Frequently | 0.683 | 0.077 | 6.035 |
| Occasionally vs. Frequently | 0.460 | 0.041 | 5.129 | ||||
| Protection | 2 | 1.7915 | 0.4083 | Not at all vs. Strict application | 1.629 | 0.546 | 4.859 |
| Medium application vs. Strict application | 1.462 | 0.815 | 2.622 |
| Variable | DF | Wald Chi-Square | p-Value | Level | OR Estimate | 95% Lower Wald Confidence Limit | 95% Upper Wald Confidence Limit |
|---|---|---|---|---|---|---|---|
| Age | 3 | 14.8694 | 0.0019 | 18–30 vs. 60+ | 10.841 | 1.247 | 94.234 |
| 31–45 vs. 60+ | 4.707 | 0.531 | 41.732 | ||||
| 46–59 vs. 60+ | 3.940 | 0.377 | 41.199 | ||||
| Sports | 2 | 15.3573 | 0.0005 | Little or no activity vs. Very active | 2.820 | 1.192 | 6.668 |
| Moderate vs. Very active | 1.037 | 0.448 | 2.400 | ||||
| Health | 3 | 8.8880 | 0.0118 | Resistant vs. Very sensitive | 5.158 | 1.587 | 16.763 |
| Moderately sensitive vs. Very sensitive | 3.384 | 1.010 | 11.337 |
| Variable | DF | Wald Chi-Square | p-Value | Level | OR Estimate | 95% Lower Wald Confidence Limit | 95% Upper Wald Confidence Limit |
|---|---|---|---|---|---|---|---|
| Continent | 3 | 6.5229 | 0.0888 | Africa vs. North America | 0.531 | 0.156 | 1.803 |
| Asia vs. North America | 1.339 | 0.303 | 5.916 | ||||
| Europe vs. North America | 0.966 | 0.255 | 3.654 | ||||
| Ethnicity | 4 | 2.5095 | 0.6429 | Other vs. Asian | 1.873 | 0.593 | 5.916 |
| African/Afro-American vs. Other | 1.568 | 0.497 | 4.953 | ||||
| Caucasian vs. Asian | 1.167 | 0.336 | 4.050 | ||||
| Arabic vs. Asian | 1.756 | 0.582 | 5.299 | ||||
| Gender | 1 | 0.0694 | 0.7922 | Male vs. Female | 0.957 | 0.690 | 1.327 |
| Age | 3 | 1.7330 | 0.6296 | 18–30 vs. 60+ | 1.450 | 0.539 | 3.899 |
| 31–45 vs. 60+ | 1.199 | 0.455 | 3.162 | ||||
| 46–59 vs. 60+ | 0.986 | 0.330 | 2.949 | ||||
| Blood | 7 | 6.7163 | 0.4590 | A+ vs. O− | 1.465 | 0.643 | 3.341 |
| A− vs. O− | 5.754 | 1.067 | 31.035 | ||||
| B+ vs. O− | 1.655 | 0.695 | 3.944 | ||||
| B− vs. O− | 3.469 | 0.624 | 19.265 | ||||
| AB+ vs. O− | 2.032 | 0.734 | 5.626 | ||||
| AB− vs. O− | 1.575 | 0.241 | 10.299 | ||||
| O+ vs. O− | 1.422 | 0.630 | 3.209 | ||||
| Education | 2 | 0.9703 | 0.6156 | No study or primary vs. University/post-university | 0.946 | 0.538 | 1.664 |
| Middle/secondary vs. University/post-university | 1.250 | 0.767 | 2.035 | ||||
| Sports | 2 | 2.5403 | 0.2808 | Little or no activity vs. Very active | 0.968 | 0.585 | 1.603 |
| Moderate vs. Very active | 0.777 | 0.470 | 1.283 | ||||
| Health | 2 | 4.0803 | 0.1300 | Resistant vs. Very sensitive | 1.273 | 0.691 | 2.345 |
| Moderately sensitive vs. Very sensitive | 0.943 | 0.502 | 1.772 | ||||
| Tobacco | 2 | 2.1788 | 0.3364 | No vs. Frequently | 0.985 | 0.550 | 1.765 |
| Occasionally vs. Frequently | 0.673 | 0.331 | 1.368 | ||||
| Alcohol | 2 | 2.3629 | 0.3068 | No vs. Frequently | 1.864 | 0.550 | 6.324 |
| Occasionally vs. Frequently | 1.243 | 0.334 | 4.631 | ||||
| Protection | 2 | 10.9263 | 0.0042 | Not at all vs. Strict application | 0.387 | 0.210 | 0.715 |
| Medium application vs. Strict application | 0.700 | 0.517 | 0.947 |
| Variable | DF | Wald Chi-Square | p-Value | Level | OR Estimate | 95% Lower Wald Confidence Limit | 95% Upper Wald Confidence Limit |
|---|---|---|---|---|---|---|---|
| Tobacco | 2 | 6.5963 | 0.0370 | No vs. Frequently | 0.983 | 0.589 | 1.641 |
| Occasionally vs. Frequently | 0.539 | 0.280 | 1.040 | ||||
| Protection | 2 | 13.0085 | 0.0015 | Not at all vs. Strict application | 0.382 | 0.220 | 0.663 |
| Medium application vs. Strict application | 0.725 | 0.547 | 0.961 |
| Significance Test | Infection | Severity | ||
|---|---|---|---|---|
| Full Model | Selected Model | Full Model | Selected Model | |
| Likelihood Ratio | <0.0001 | <0.0001 | 0.0446 | <0.0001 |
| Score | 0.0007 | <0.0001 | 0.0605 | 0.0291 |
| Wald | 0.0263 | <0.0001 | 0.1078 | 0.0180 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aouissi, H.A.; Kechebar, M.S.A.; Ababsa, M.; Roufayel, R.; Neji, B.; Petrisor, A.-I.; Hamimes, A.; Epelboin, L.; Ohmagari, N. The Importance of Behavioral and Native Factors on COVID-19 Infection and Severity: Insights from a Preliminary Cross-Sectional Study. Healthcare 2022, 10, 1341. https://doi.org/10.3390/healthcare10071341
Aouissi HA, Kechebar MSA, Ababsa M, Roufayel R, Neji B, Petrisor A-I, Hamimes A, Epelboin L, Ohmagari N. The Importance of Behavioral and Native Factors on COVID-19 Infection and Severity: Insights from a Preliminary Cross-Sectional Study. Healthcare. 2022; 10(7):1341. https://doi.org/10.3390/healthcare10071341
Chicago/Turabian StyleAouissi, Hani Amir, Mohamed Seif Allah Kechebar, Mostefa Ababsa, Rabih Roufayel, Bilel Neji, Alexandru-Ionut Petrisor, Ahmed Hamimes, Loïc Epelboin, and Norio Ohmagari. 2022. "The Importance of Behavioral and Native Factors on COVID-19 Infection and Severity: Insights from a Preliminary Cross-Sectional Study" Healthcare 10, no. 7: 1341. https://doi.org/10.3390/healthcare10071341