
Forward Bending in Supine Test: Diagnostic Accuracy for Acute Vertebral Fragility Fracture

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
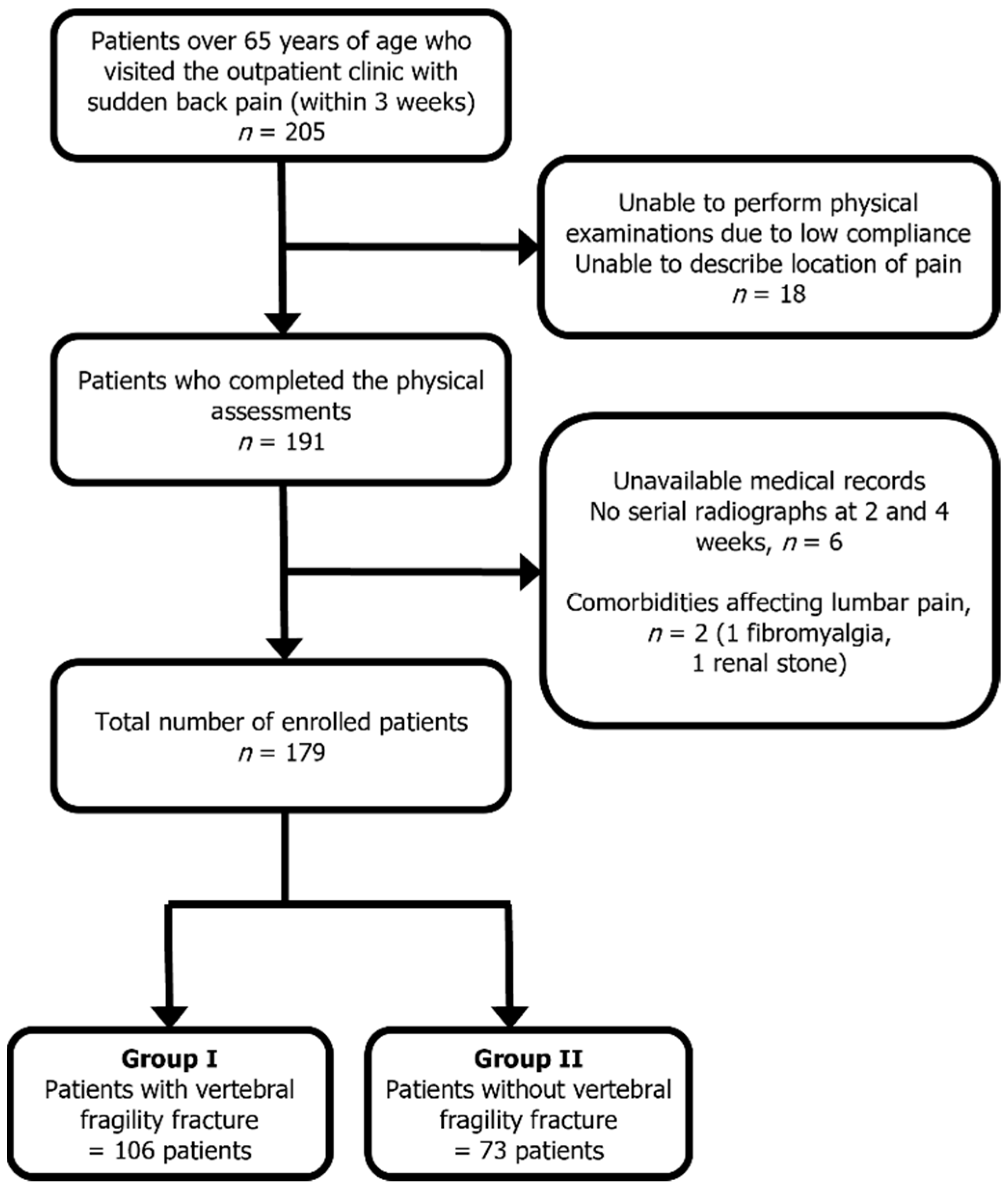
2.1. Study Participants
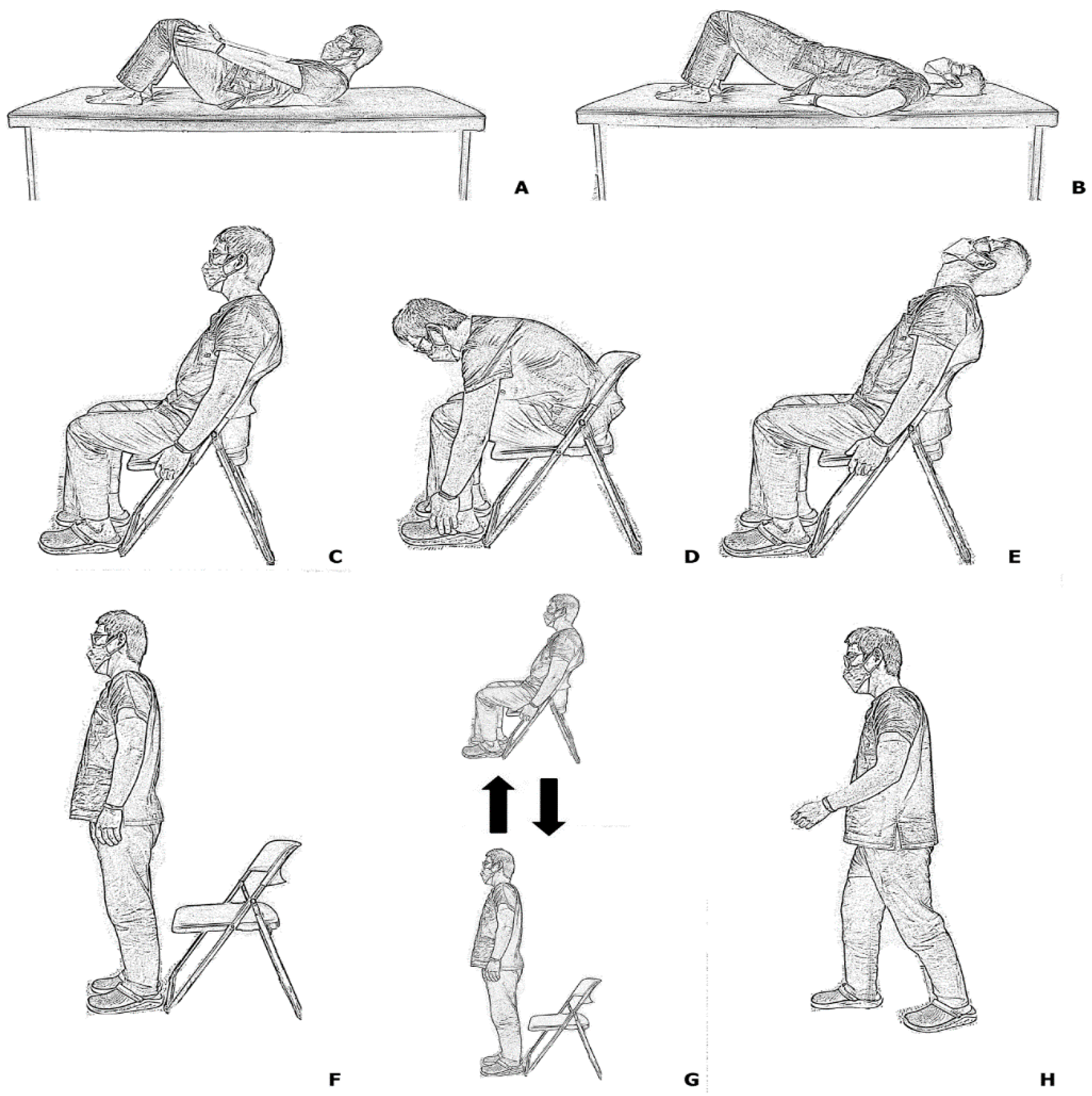
2.2. Physical Examinations
2.3. Evaluation of Plain Radiograph
2.4. Statistical Analysis
3. Results
3.1. Demographics
3.2. Diagnostic Values of Physical Examinations
3.3. Reliability of Plain Radiograph
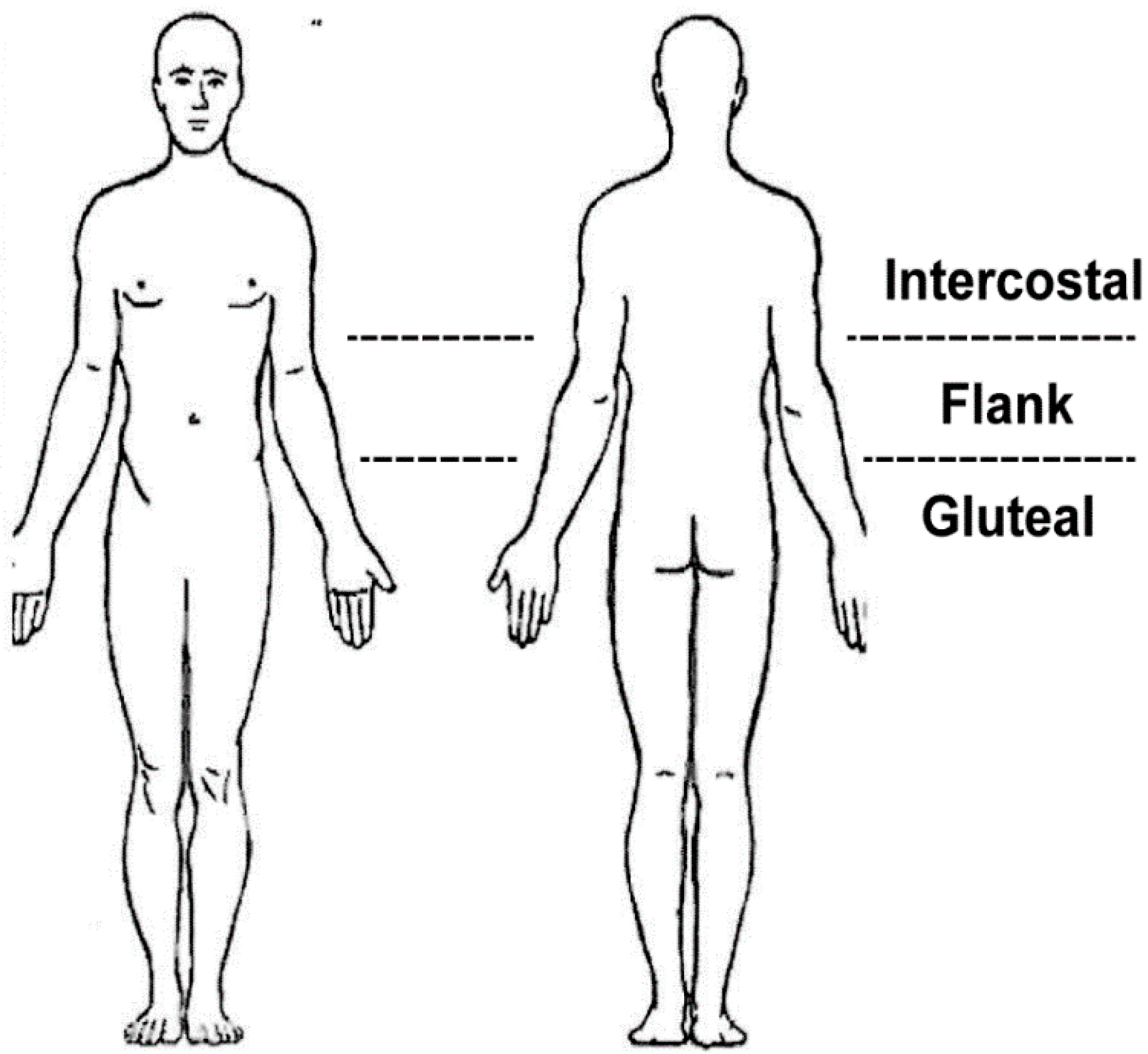
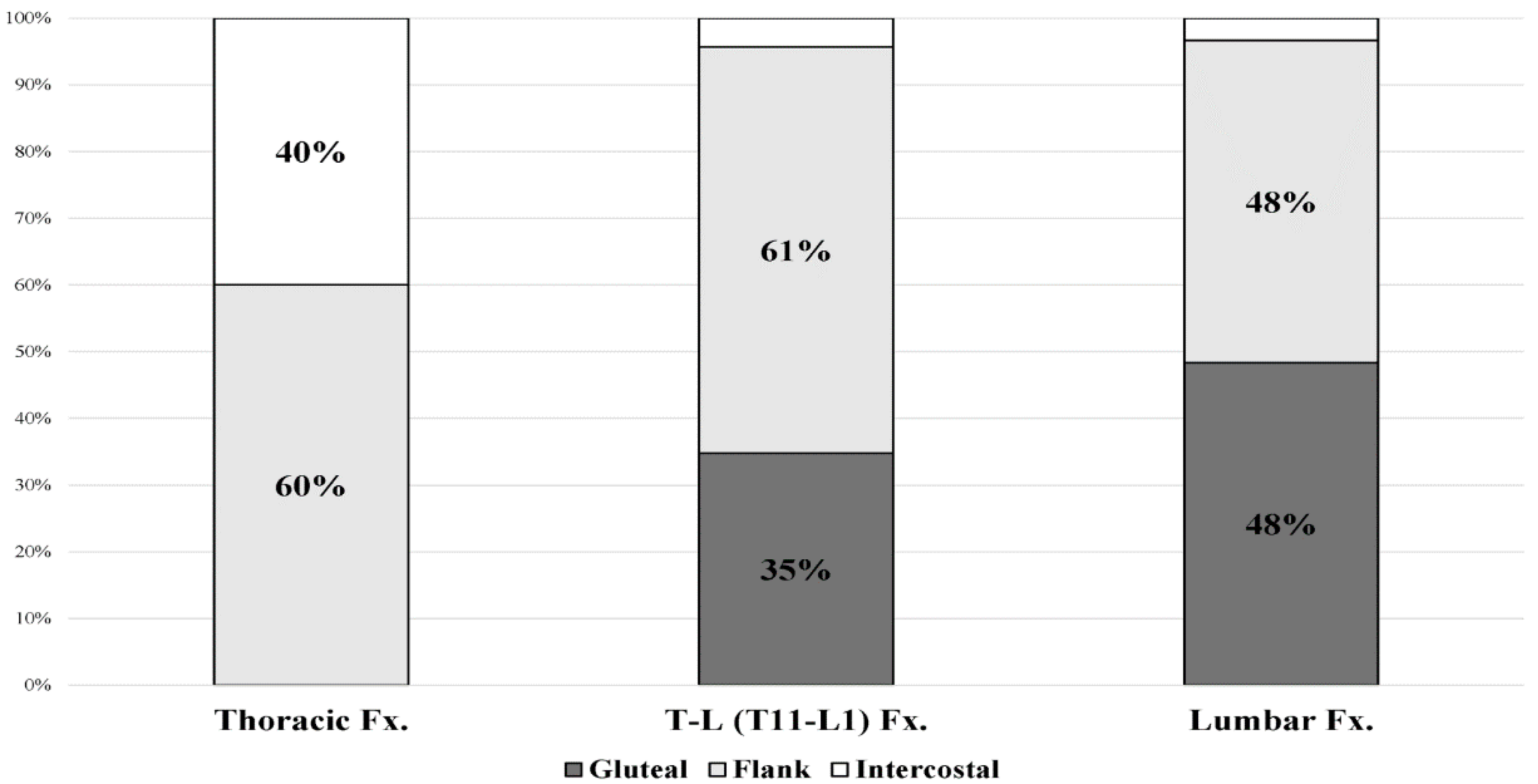
3.4. Location of Patient-Drawing Pain Based on Fracture Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Curtis, E.M.; Moon, R.J.; Harvey, N.C.; Cooper, C. Reprint of: The impact of fragility fracture and approaches to osteoporosis risk assessment worldwide. Int. J. Orthop. Trauma Nurs. 2017, 26, 7–17. [Google Scholar] [CrossRef] [Green Version]
- Ballane, G.; Cauley, J.A.; Luckey, M.M.; El-Hajj Fuleihan, G. Worldwide prevalence and incidence of osteoporotic vertebral fractures. Osteoporos. Int. 2017, 28, 1531–1542. [Google Scholar] [CrossRef] [PubMed]
- Kendler, D.L.; Bauer, D.C.; Davison, K.S.; Dian, L.; Hanley, D.A.; Harris, S.T.; McClung, M.R.; Miller, P.D.; Schousboe, J.T.; Yuen, C.K.; et al. Vertebral Fractures: Clinical Importance and Management. Am. J. Med. 2016, 129, 221.e1–221.e10. [Google Scholar] [CrossRef] [Green Version]
- El Maghraoui, A.; Rezqi, A.; Mounach, A.; Achemlal, L.; Bezza, A.; Ghozlani, I. Systematic vertebral fracture assessment in asymptomatic postmenopausal women. Bone 2013, 52, 176–180. [Google Scholar] [CrossRef]
- Suzuki, N.; Ogikubo, O.; Hansson, T. The course of the acute vertebral body fragility fracture: Its effect on pain, disability and quality of life during 12 months. Eur. Spine J. 2008, 17, 1380–1390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gehlbach, S.H.; Bigelow, C.; Heimisdottir, M.; May, S.; Walker, M.; Kirkwood, J.R. Recognition of vertebral fracture in a clinical setting. Osteoporos. Int. 2000, 11, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.W.; Jang, J.H.; Kim, J.J.; Lim, Y.S.; Hyun, S.Y.; Yang, H.J. The Value of X-ray Compared with Magnetic Resonance Imaging in the Diagnosis of Traumatic Vertebral Fractures. J. Trauma Inj. 2017, 30, 158–165. [Google Scholar] [CrossRef] [Green Version]
- Delmas, P.D.; van de Langerijt, L.; Watts, N.B.; Eastell, R.; Genant, H.; Grauer, A.; Cahall, D.L. Underdiagnosis of Vertebral Fractures Is a Worldwide Problem: The IMPACT Study. J. Bone Miner. Res. 2005, 20, 557–563. [Google Scholar] [CrossRef]
- Hirsch, J.A.; Beall, D.P.; Chambers, M.R.; Andreshak, T.G.; Brook, A.L.; Bruel, B.M.; Deen, H.G.; Gerszten, P.C.; Kreiner, D.S.; Sansur, C.A.; et al. Management of vertebral fragility fractures: A clinical care pathway developed by a multispecialty panel using the RAND/UCLA Appropriateness Method. Spine J. 2018, 18, 2152–2161. [Google Scholar] [CrossRef] [Green Version]
- Clark, E.M.; Cummings, S.R.; Schousboe, J.T. Spinal radiographs in those with back pain-when are they appropriate to diagnose vertebral fractures? Osteoporos. Int. 2017, 28, 2293–2297. [Google Scholar] [CrossRef] [Green Version]
- Longo, U.G.; Loppini, M.; Denaro, L.; Maffulli, N.; Denaro, V. Osteoporotic vertebral fractures: Current concepts of conservative care. Br. Med. Bull. 2011, 102, 171–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Compston, J.; Cooper, A.; Cooper, C.; Gittoes, N.; Gregson, C.; Harvey, N.; Hope, S.; Kanis, J.A.; McCloskey, E.V.; Poole, K.E.S.; et al. UK clinical guideline for the prevention and treatment of osteoporosis. Arch. Osteoporos. 2017, 12, 43. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Chang, G.; Kang, H.; Ham, D.-W.; Lee, J.-S.; Jung, H.S.; Song, K.-S. Impact of Bone Mineral Density on the Incidence of Age-Related Vertebral Fragility Fracture. J. Korean Med. Sci. 2020, 35, e116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langdon, J.; Way, A.; Heaton, S.; Bernard, J.; Molloy, S. Vertebral compression fractures—New clinical signs to aid diagnosis. Ann. R. Coll. Surg. Engl. 2010, 92, 163–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, Z.; Harada, A.; Matsui, Y.; Takemura, M.; Wakao, N.; Suzuki, T.; Nihashi, T.; Kawatsu, S.; Shimokata, H.; Ishiguro, N. Can you diagnose for vertebral fracture correctly by plain X-ray? Osteoporos. Int. 2006, 17, 1584–1591. [Google Scholar] [CrossRef]
- Cohen, J.F.; Korevaar, D.A.; Altman, D.G.; Bruns, D.E.; Gatsonis, C.A.; Hooft, L.; Irwig, L.; Levine, D.; Reitsma, J.B.; de Vet, H.C.W.; et al. STARD 2015 guidelines for reporting diagnostic accuracy studies: Explanation and elaboration. BMJ Open 2016, 6, e012799. [Google Scholar] [CrossRef]
- Lachenbruch, P.A. McNemar Test. In Wiley StatsRef: Statistics Reference Online; Balakrishnan, N., Colton, T., Everitt, B., Piegorsch, W., Ruggeri, F., Teugels, J.L., Eds.; Wiley: Hoboken, NJ, USA, 2014. [Google Scholar] [CrossRef]
- Fleiss, J.L.; Cohen, J. The Equivalence of Weighted Kappa and the Intraclass Correlation Coefficient as Measures of Reliability. Educ. Psychol. Meas. 1973, 33, 613–619. [Google Scholar] [CrossRef]
- Šimundić, A.-M. Measures of Diagnostic Accuracy: Basic Definitions. Electron. J. Int. Fed. Clin. Chem. Lab. Med. 2009, 19, 203–211. [Google Scholar]
- Herman, C.R.; Gill, H.K.; Eng, J.; Fajardo, L.L. Screening for Preclinical Disease: Test and Disease Characteristics. Am. J. Roentgenol. 2002, 179, 825–831. [Google Scholar] [CrossRef]
- Briggs, A.M.; Greig, A.M.; Bennell, K.L.; Hodges, P.W. Paraspinal muscle control in people with osteoporotic vertebral fracture. Eur. Spine J. 2007, 16, 1137–1144. [Google Scholar] [CrossRef] [Green Version]
- Postacchini, R.; Paolino, M.; Faraglia, S.; Cinotti, G.; Postacchini, F. Assessment of patient’s pain-related behavior at physical examination may allow diagnosis of recent osteoporotic vertebral fracture. Spine J. 2013, 13, 1126–1133. [Google Scholar] [CrossRef] [PubMed]
- Doo, T.-H.; Shin, D.; Kim, H.-I.; Shin, D.-G.; Kim, H.-J.; Chung, J.-H.; Lee, J.-O. Clinical Relevance of Pain Patterns in Osteoporotic Vertebral Compression Fractures. J. Korean Med. Sci. 2009, 23, 1005–1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischgrund, J.S.; Rhyne, A.; Macadaeg, K.; Moore, G.; Kamrava, E.; Yeung, C.; Truumees, E.; Schaufele, M.; Yuan, P.; De Palma, M.; et al. Long-term outcomes following intraosseous basivertebral nerve ablation for the treatment of chronic low back pain: 5-year treatment arm results from a prospective randomized double-blind sham-controlled multi-center study. Eur. Spine J. 2020, 29, 1925–1934. [Google Scholar] [CrossRef] [PubMed]
- D’Costa, H.; George, G.; Parry, M.; Pullinger, R.; Skinner, D.; Thomas, S.; Todd, B.; Wilson, M. Pitfalls in the clinical diagnosis of vertebral fractures: A case series in which posterior midline tenderness was absent. Emerg. Med. J. 2005, 22, 330. [Google Scholar] [CrossRef] [PubMed]
- Nolet, P.S.; Yu, H.; Côté, P.; Meyer, A.-L.; Kristman, V.L.; Sutton, D.; Murnaghan, K.; Lemeunier, N. Reliability and validity of manual palpation for the assessment of patients with low back pain: A systematic and critical review. Chiropr. Man. Ther. 2021, 29, 33. [Google Scholar] [CrossRef]
- Will, J.S.; Bury, D.C.; Miller, J.A. Mechanical Low Back Pain. Am. Fam. Phys. 2018, 98, 421–428. [Google Scholar]
- Choi, Y.-S. Pathophysiology of degenerative disc disease. Asian Spine J. 2009, 3, 39–44. [Google Scholar] [CrossRef]
- Old, J.L.; Calvert, M. Vertebral compression fractures in the elderly. Am. Fam. Phys. 2004, 69, 111–116. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Fracture (n = 106) | Non-Fracture (n = 73) | p-Value |
|---|---|---|---|
| Age | 74.84 (±7.45) | 72.68 (±7.44) | 0.065 |
| Height (cm) | 156.38 (±9.09) | 155.83 (±8.63) | 0.683 |
| Weight (kg) | 57.34 (±10.25) | 58.54 (±10.92) | 0.461 |
| BMI | 23.68 (±5.16) | 23.70 (±5.18) | 0.548 |
| Lumbar BMD (g/cm2) | 0.90 (±0.18) | 0.91 (±0.17) | 0.784 |
| Femur neck BMD (g/cm2) | 0.67 (±0.13) | 0.67 (±0.12) | 0.792 |
| Hip total BMD (g/cm2) | 0.71 (±0.14) | 0.72 (±0.72) | 0.591 |
| Diagnostic modality | |||
| Serial radiograph/CT/MRI | 23/14/69 | 51/9/13 | |
| Fracture location | |||
| Thoracic/Thoracolumbar/Lumbar | 10/33/63 |
| Diagnostic Test | Sensitivity (%) | Specificity (%) | Accuracy (%) | McNemar Test p-Value * | |
|---|---|---|---|---|---|
| Compared with Confirmatory Results | Compared with Radiographic Results of Rater 2 | ||||
| FB-SU | 90.6 | 71.2 | 82.7 | 0.072 | <0.001 |
| BB-SU | 22.6 | 93.2 | 51.4 | <0.001 | <0.001 |
| SIT | 14.2 | 100.0 | 49.2 | <0.001 | <0.001 |
| FB-SI | 37.7 | 91.8 | 59.7 | <0.001 | <0.001 |
| BB-SI | 17.0 | 98.6 | 50.3 | <0.001 | <0.001 |
| STAND | 16.0 | 98.6 | 49.7 | <0.001 | <0.001 |
| SIT-STAND | 34.0 | 87.7 | 55.9 | <0.001 | <0.001 |
| WALK | 17.9 | 95.9 | 49.7 | <0.001 | <0.001 |
| Tenderness | 45.3 | 75.3 | 57.5 | <0.001 | <0.001 |
| Radiographic interpretation (rater 1) | 68.4 | 71.9 | 69.8 | 0.016 | - |
| Radiographic interpretation (rater 2) | 69.3 | 71.9 | 70.4 | 0.026 | - |
| FB-SU | Fracture (+) | Fracture (−) | Total | BB-SU | Fracture (+) | Fracture (−) | Total |
| Finding (+) | 96 | 21 | 117 | Finding (+) | 24 | 5 | 29 |
| Finding (−) | 10 | 52 | 62 | Finding (−) | 82 | 68 | 150 |
| Total | 106 | 73 | 179 | Total | 106 | 73 | 179 |
| SIT | FB-SI | ||||||
| Finding (+) | 15 | 0 | 15 | Finding (+) | 40 | 6 | 46 |
| Finding (−) | 91 | 73 | 164 | Finding (−) | 66 | 67 | 133 |
| Total | 106 | 73 | 179 | Total | 106 | 73 | 179 |
| BB-SI | STAND | ||||||
| Finding (+) | 18 | 1 | 19 | Finding (+) | 17 | 1 | 18 |
| Finding (−) | 88 | 72 | 160 | Finding (−) | 89 | 72 | 161 |
| Total | 106 | 73 | 179 | Total | 106 | 73 | 179 |
| SIT-STAND | WALK | ||||||
| Finding (+) | 36 | 9 | 45 | Finding (+) | 19 | 3 | 22 |
| Finding (−) | 70 | 64 | 134 | Finding (−) | 87 | 70 | 157 |
| Total | 106 | 73 | 179 | Total | 106 | 73 | 179 |
| Tenderness | |||||||
| Finding (+) | 48 | 18 | 66 | ||||
| Finding (−) | 58 | 55 | 113 | ||||
| Total | 106 | 73 | 179 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, C.-W.; Lee, J.; Ham, D.-W.; Kang, H.; Chang, D.-G.; Kim, Y.B.; Ahn, Y.-J.; Shim, J.H.; Song, K.-S. Forward Bending in Supine Test: Diagnostic Accuracy for Acute Vertebral Fragility Fracture. Healthcare 2022, 10, 1215. https://doi.org/10.3390/healthcare10071215
Jung C-W, Lee J, Ham D-W, Kang H, Chang D-G, Kim YB, Ahn Y-J, Shim JH, Song K-S. Forward Bending in Supine Test: Diagnostic Accuracy for Acute Vertebral Fragility Fracture. Healthcare. 2022; 10(7):1215. https://doi.org/10.3390/healthcare10071215
Chicago/Turabian StyleJung, Chan-Woo, Jeongik Lee, Dae-Woong Ham, Hyun Kang, Dong-Gune Chang, Youngbae B. Kim, Young-Joon Ahn, Joo Hyun Shim, and Kwang-Sup Song. 2022. "Forward Bending in Supine Test: Diagnostic Accuracy for Acute Vertebral Fragility Fracture" Healthcare 10, no. 7: 1215. https://doi.org/10.3390/healthcare10071215