
Cross Sectional Study on the Association between Dental Caries and Life Habits in School Age Italian Children


Abstract
:
1. Keynotes
2. Introduction
3. Materials and Methods
- Breastfeeding
- Bottle feeding
- Night-time feeding
- Child allergies
- Child mucolytics or cough suppressants
- Child mouth breathing
- Child systemic fluoride
- Child daily number of brushings
- Fluoride toothpaste
- Child dental flossing
- Pacifier
- Bacterial Colonization
- Honey
- Night-time bottle
- Child sex
- Single mother
- Mother No. of children
- Smoking mother
- Mother caries
- Mother annual dental visits
- Mother daily brushing
- Mother systemic fluoride during pregnancy
- Smoking father
- Father annual dental visits
- Father caries
- Sex
- Age
- Presence/absence of caries
- Number of decayed teeth
4. Statistical Analysis
5. Results
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health National Guidelines for the Promotion of Oral Health and Disease Prevention. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2073_allegato.pdf (accessed on 5 January 2022).
- Ministry of Health General Secretariat Clinical Recommendations in Odontostomatology. 2017. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2637_allegato.pdf (accessed on 5 January 2022).
- Italian Society of Children’s Dentistry Guidelines for the Prevention of Caries in Children. 2013. Available online: https://www.sioi.it/wp-content/uploads/2013/03/linee_guida_SIOI.pdf (accessed on 5 January 2022).
- Buldur, B. Pathways between Parental and Individual Determinants of Dental Caries and Dental Visit Behaviours among Children: Validation of a New Conceptual Model. Community Dent. Oral Epidemiol. 2020, 48, 280–287. [Google Scholar] [CrossRef]
- Štefanová, E.; Baška, T.; Holubčíková, J.; Timková, S.; Tatarková, M.; Sovičová, M.; Hudečková, H. Selected Behavioural Factors Affecting Oral Health in Schoolchildren: Results from the Health Behaviour in School-Aged Children (HBSC) Slovak Study. Int. J. Environ. Res. Public Health 2020, 17, 7516. [Google Scholar] [CrossRef]
- Chen, L.; Hong, J.; Xiong, D.; Zhang, L.; Li, Y.; Huang, S.; Hua, F. Are Parents’ Education Levels Associated with Either Their Oral Health Knowledge or Their Children’s Oral Health Behaviors? A Survey of 8446 Families in Wuhan. BMC Oral Health 2020, 20, 203. [Google Scholar] [CrossRef] [PubMed]
- Colombo, S.; Gallus, S.; Beretta, M.; Lugo, A.; Scaglioni, S.; Colombo, P.; Paglia, M.; Gatto, R.; Marzo, G.; Caruso, S.; et al. Prevalence and Determinants of Early Childhood Caries in Italy. Eur. J. Paediatr. Dent. 2019, 20, 267–273. [Google Scholar] [CrossRef]
- Guedes, R.S.; Piovesan, C.; Ardenghi, T.M.; Emmanuelli, B.; Braga, M.M.; Mendes, F.M. Presence of Initial Caries Lesions as a Risk Factor for Caries in Preschool Children: A Cohort Study. CRE 2018, 52, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-J.; Kim, J.-B.; Jin, B.-H.; Paik, D.-I.; Bae, K.-H. Risk Factors for Dental Caries in Childhood: A Five-Year Survival Analysis. Community Dent. Oral Epidemiol. 2015, 43, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Howenstein, J.; Kumar, A.; Casamassimo, P.S.; McTigue, D.; Coury, D.; Yin, H. Correlating Parenting Styles with Child Behavior and Caries. Pediatr. Dent. 2015, 37, 59–64. [Google Scholar]
- World Health Organization. Oral Health Surveys: Basic Methods, 4th ed.; World Health Organization: Geneva, Switzerland; Available online: https://apps.who.int/iris/handle/10665/41905 (accessed on 5 January 2022).
- World Health Organization. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Mathur, V.P.; Dhillon, J.K. Dental Caries: A Disease Which Needs Attention. Indian J. Pediatr. 2018, 85, 202–206. [Google Scholar] [CrossRef]
- Valaitis, R.; Hesch, R.; Passarelli, C.; Sheehan, D.; Sinton, J. A Systematic Review of the Relationship between Breastfeeding and Early Childhood Caries. Can. J. Public Health 2000, 91, 411–417. [Google Scholar] [CrossRef]
- Tham, R.; Bowatte, G.; Dharmage, S.C.; Tan, D.J.; Lau, M.X.Z.; Dai, X.; Allen, K.J.; Lodge, C.J. Breastfeeding and the Risk of Dental Caries: A Systematic Review and Meta-Analysis. Acta Paediatr. 2015, 104, 62–84. [Google Scholar] [CrossRef] [Green Version]
- Ferraro, M.; Vieira, A.R. Explaining Gender Differences in Caries: A Multifactorial Approach to a Multifactorial Disease. Int. J. Dent. 2010, 2010, 649643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadaki, S.; Douglas, G.V.A.; HaniBani, A.; Kang, J. Gender Differences in Caries and Periodontal Status in UK Children. medRxiv 2021. [Google Scholar] [CrossRef]
- Jacobis, I.T.D.; de Gennaro, F.; Ceglie, G.; Villani, A. Gender medicine and paediatrics: Present and future perspectives. Ital. J. Gend. Specif. Med. 2017, 3, 71–80. [Google Scholar]
- Chuang, C.Y.; Sun, H.L.; Ku, M.S. Allergic Rhinitis, Rather than Asthma, Is a Risk Factor for Dental Caries. Clin. Otolaryngol. 2018, 43, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Nava, F.; Vázquez, R.E.M.; Saldivar, G.A.H.; Beltrán, G.F.J.; Almeida, A.V.M.; Vázquez, R.C.F. Allergic Rhinitis, Feeding and Oral Habits, Toothbrushing and Socioeconomic Status. Effects on Development of Dental Caries in Primary Dentition. Caries Res. 2008, 42, 141–147. [Google Scholar] [CrossRef]
- Thie, N.M.R.; Kato, T.; Bader, G.; Montplaisir, J.Y.; Lavigne, G.J. The Significance of Saliva during Sleep and the Relevance of Oromotor Movements. Sleep Med. Rev. 2002, 6, 213–227. [Google Scholar] [CrossRef]
- Oksenberg, A.; Froom, P.; Melamed, S. Dry Mouth upon Awakening in Obstructive Sleep Apnea. J. Sleep Res. 2006, 15, 317–320. [Google Scholar] [CrossRef]
- Jacobson, L. Mouthbreathing and Gingivitis. 1. Gingival Conditions in Children with Epipharyngeal Adenoids. J. Periodontal. Res. 1973, 8, 269–277. [Google Scholar] [CrossRef]
- Johansson, A.-K.; Lingström, P.; Birkhed, D. Comparison of Factors Potentially Related to the Occurrence of Dental Erosion in High- and Low-Erosion Groups. Eur. J. Oral Sci. 2002, 110, 204–211. [Google Scholar] [CrossRef]
- Stensson, M.; Wendt, L.-K.; Koch, G.; Oldaeus, G.; Birkhed, D. Oral Health in Preschool Children with Asthma. Int. J. Paediatr. Dent. 2008, 18, 243–250. [Google Scholar] [CrossRef] [Green Version]
- Patil, S.; Iyengar, A.R.; Nagesh, K.S.; Ramneek. Oral Health in Individuals with Asthma. J. Asthma Allergy Educ. 2012, 3, 250–254. [Google Scholar] [CrossRef]
- Stensson, M.; Wendt, L.-K.; Koch, G.; Oldaeus, G.; Lingström, P.; Birkhed, D. Caries Prevalence, Caries-Related Factors and Plaque PH in Adolescents with Long-Term Asthma. Caries Res. 2010, 44, 540–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stensson, M.; Wendt, L.-K.; Koch, G.; Oldaeus, G.; Ramberg, P.; Birkhed, D. Oral Health in Young Adults with Long-Term, Controlled Asthma. Acta Odontol. Scand. 2011, 69, 158–164. [Google Scholar] [CrossRef]
- Weiler, R.M.E.; Fisberg, M.; Barroso, A.S.; Nicolau, J.; Simi, R.; Siqueira, W.L. A Study of the Influence of Mouth-Breathing in Some Parameters of Unstimulated and Stimulated Whole Saliva of Adolescents. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Dawes, C. Circadian Rhythms in Human Salivary Flow Rate and Composition. J. Physiol. 1972, 220, 529–545. [Google Scholar] [CrossRef] [PubMed]
- Pevernagie, D.A.; De Meyer, M.M.; Claeys, S. Sleep, Breathing and the Nose. Sleep Med. Rev. 2005, 9, 437–451. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.S.; Parolia, A.; Kundabala, M.; Vikram, M. Asthma and Oral Health: A Review. Aust. Dent. J. 2010, 55, 128–133. [Google Scholar] [CrossRef]
- Samec, T.; Amaechi, B.T.; Battelino, T.; Krivec, U.; Jan, J. Influence of Anti-Asthmatic Medications on Dental Caries in Children in Slovenia. Int. J. Paediatr. Dent. 2013, 23, 188–196. [Google Scholar] [CrossRef]
- Ho, S.-W.; Lue, K.-H.; Ku, M.-S. Allergic Rhinitis, Rather than Asthma, Might Be Associated with Dental Caries, Periodontitis, and Other Oral Diseases in Adults. PeerJ 2019, 7, e7643. [Google Scholar] [CrossRef]
- Dean, H. The Investigation of Physiological Effects by the Epidemiological Method. In Fluorine and Dental Health; Moulton, F.R., Ed.; American Association for the Advancement of Science: Washington, DC, USA, 1942; pp. 23–31. [Google Scholar]
- Mckay, F.S. An Appraisal of the Water-Borne Fluoride-Dental Caries Relationship. Am. J. Public Health Nations Health 1953, 43 Pt 1, 700–703. [Google Scholar] [CrossRef] [Green Version]
- Glenn, F.B.; Glenn, W.D.; Duncan, R.C. Fluoride Tablet Supplementation during Pregnancy for Caries Immunity: A Study of the Offspring Produced. Am. J. Obs. Gynecol. 1982, 143, 560–564. [Google Scholar] [CrossRef]
- Bibby, B.G.; Wilkins, E.; Witol, E. A Preliminary Study of the Effects of Fluoride Lozenges and Pills on Dental Caries. Oral Surg. Oral Med. Oral Pathol. 1955, 8, 213–216. [Google Scholar] [CrossRef]
- LeGeros, R.Z.; Glenn, F.B.; Lee, D.D.; Glenn, W.D. Some Physico-Chemical Properties of Deciduous Enamel of Children with and without Pre-Natal Fluoride Supplementation (PNF). J. Dent. Res. 1985, 64, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Kariesbefall von Kindern Nach Unterschiedlich Langer Applikation von Fluoridtabletten. Available online: https://www.online-dzz.de/archiv/ausgabe/artikel/dzz-4-1992/3319-kariesbefall-von-kindern-nach-unterschiedlich-langer-applikation-von-fluoridtabletten/ (accessed on 15 February 2022).
- Leverett, D.H.; Adair, S.M.; Vaughan, B.W.; Proskin, H.M.; Moss, M.E. Randomized Clinical Trial of the Effect of Prenatal Fluoride Supplements in Preventing Dental Caries. Caries Res. 1997, 31, 174–179. [Google Scholar] [CrossRef]
- Künzel, W.; Fischer, T. Rise and Fall of Caries Prevalence in German Towns with Different F Concentrations in Drinking Water. Caries Res. 1997, 31, 166–173. [Google Scholar] [CrossRef]
- Limeback, H. A Re-Examination of the Pre-Eruptive and Post-Eruptive Mechanism of the Anti-Caries Effects of Fluoride: Is There Any Anti-Caries Benefit from Swallowing Fluoride? Community Dent. Oral Epidemiol. 1999, 27, 62–71. [Google Scholar] [CrossRef]
- König, K. Aktuelle Empfehlungen Zum Fluoridgehalt in Kinderzahnpasten - Konsequenzen Für Die Systemische Fluoridierung. Gesundheitswesen 2002, 64, 33–38. [Google Scholar] [CrossRef]
- Thylstrup, A.; Fejerskov, O.; Bruun, C.; Kann, J. Enamel Changes and Dental Caries in 7-Year-Old Children given Fluoride Tablets from Shortly after Birth. Caries Res. 1979, 13, 265–276. [Google Scholar] [CrossRef]
- Riordan, P.J. Fluoride Supplements for Young Children: An Analysis of the Literature Focusing on Benefits and Risks. Community Dent. Oral Epidemiol. 1999, 27, 72–83. [Google Scholar] [CrossRef]
- Riordan, P.J. Fluoride Supplements in Caries Prevention: A Literature Review and Proposal for a New Dosage Schedule. J. Public Health Dent. 1993, 53, 174–189. [Google Scholar] [CrossRef]
- Oganessian, E.; Lencová, E.; Broukal, Z. Is Systemic Fluoride Supplementation for Dental Caries Prevention in Children Still Justifiable? Prague Med. Rep. 2007, 108, 306–314. [Google Scholar] [PubMed]
- Connett, P. 50 Reasons to Oppose Fluoridation. Available online: https://fluoridealert.org/articles/50-reasons/ (accessed on 15 February 2022).
- Aoun, A.; Darwiche, F.; Al Hayek, S.; Doumit, J. The Fluoride Debate: The Pros and Cons of Fluoridation. Prev. Nutr. Food Sci. 2018, 23, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Avila, W.M.; Pordeus, I.A.; Paiva, S.M.; Martins, C.C. Breast and Bottle Feeding as Risk Factors for Dental Caries: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0142922. [Google Scholar] [CrossRef] [PubMed]
- Olak, J.; Nguyen, M.S.; Nguyen, T.T.; Nguyen, B.B.T.; Saag, M. The Influence of Mothers’ Oral Health Behaviour and Perception Thereof on the Dental Health of Their Children. EPMA J. 2018, 9, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Azimi, S.; Taheri, J.B.; Tennant, M.; Kruger, E.; Molaei, H.; Ghorbani, Z. Relationship Between Mothers’ Knowledge and Attitude Towards the Importance of Oral Health and Dental Status of Their Young Children. Oral Health Prev. Dent. 2018, 16, 265–270. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Caries | p | ||
|---|---|---|---|---|
| NO | YES | |||
| Breastfeeding | NO | 20 (55.6%) | 16 (44.4%) | 0.551 |
| YES | 164 (60.7%) | 106 (39.3%) | ||
| Bottle feeding | NO | 72 (54.5%) | 60 (45.5%) | 0.106 |
| YES | 109 (63.7%) | 62 (36.3%) | ||
| Night-time feeding | NO | 119 (57.8%) | 87 (42.2%) | 0.179 |
| YES | 62 (66%) | 32 (34%) | ||
| Child allergies | NO | 154 (60.9%) | 99 (39.1%) | 0.365 |
| YES | 27 (54%) | 23 (46%) | ||
| Child mucolytics or cough suppressants | NO | 124 (59.3%) | 85 (40.7%) | 0.994 |
| YES | 57 (59.4%) | 39 (40.6%) | ||
| Child mouth breathing | NO | 143 (58.6%) | 101 (41.4%) | 0.448 |
| YES | 39 (63.9%) | 22 (36.1%) | ||
| Child systemic fluoride | NO | 156 (61.7%) | 97 (38.3%) | 0.138 |
| YES | 23 (50.5%) | 23 (50%) | ||
| Child daily number of brushing | 0 | 0 (0%) | 1 (100%) | 0.276 |
| 1 | 28 (65.1%) | 15 (34.9%) | ||
| 2 | 133 (58.1%) | 96 (41.9%) | ||
| 3 | 23 (69.7%) | 10 (30.3%) | ||
| 4 | 0 (0%) | 1 (100%) | ||
| Fluoride toothpaste | NO | 38 (52.1%) | 35 (47.9%) | 0.119 |
| YES | 147 (62.3%) | 89 (37.7%) | ||
| Child dental flossing | NO | 178 (60.8%) | 115 (39.2%) | 0.177 |
| YES | 7 (43.8%) | 9 (56.3%) | ||
| Pacifier | NO | 73 (56.6%) | 56 (43.4%) | 0.29 |
| YES | 112 (62.6%) | 67 (37.4%) | ||
| Bacterial colonization | NO | 124 (61.4%) | 78 (38.6%) | 0.489 |
| YES | 59 (57.3%) | 44 (42.7%) | ||
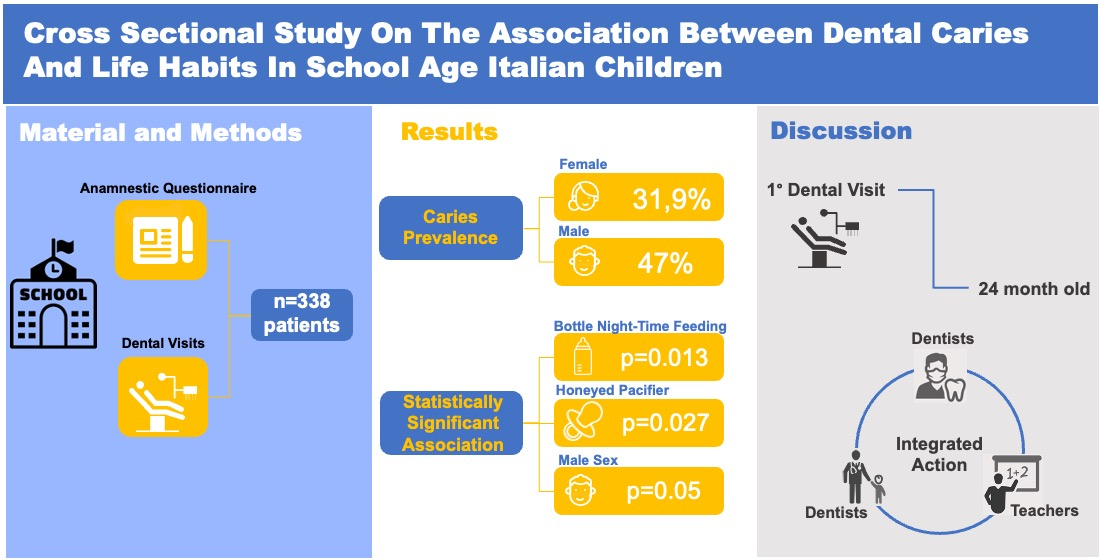
| Honey | NO | 176 (60.7%) | 114 (39.3%) | 0.027 * |
| YES | 3 (27.3%) | 8 (72.7%) | ||
| Night-time bottle | NO | 147 (56.8%) | 112 (43.2%) | 0.013 * |
| YES | 31 (77.5%) | 9 (22.5%) | ||
| Child sex | F | 109 (68.1%) | 51 (31.9%) | 0.005 * |
| M | 88 (53%) | 78 (47%) | ||
| Single mother | NO | 181 (60.5%) | 118 (39.5%) | 0.878 |
| YES | 7 (58.3%) | 5 (41.7%) | ||
| Mother No. of children | 1 | 49 (58.3%) | 35 (41.7%) | 0.199 |
| 2 | 94 (64.8%) | 51 (35.2%) | ||
| 3 | 34 (56.7%) | 26 (43.3%) | ||
| 4 | 2 (28.6%) | 5 (71.4%) | ||
| Smoking mother | NO | 134 (61.5%) | 84 (38.5%) | 0.648 |
| YES | 54 (58.7%) | 38 (41.3%) | ||
| Mother caries | NO | 36 (70.6%) | 15 (29.4%) | 0.107 |
| YES | 151 (58.5%) | 107 (41.5%) | ||
| Mother annual dental visits | 0 | 9 (56.3%) | 7 (43.8%) | 0.966 |
| 1 | 77 (59.7%) | 52 (40.3%) | ||
| 2 | 99 (61.5%) | 62 (38.5%) | ||
| 3 | 2 (66.7%) | 1 (33.3%) | ||
| Mother daily brushing | 1 | 7 (70%) | 3 (30%) | 0.825 |
| 2 | 112 (60.2%) | 74 (39.8%) | ||
| 3 | 67 60.4%) | 44 (39.6%) | ||
| Mother systemic fluoride during pregnancy | 0 | 154 (61.1%) | 98 (38.9%) | 0.613 |
| 1 | 31 (57.4%) | 23 (42.6%) | ||
| Smoking father | NO | 115 (60.8%) | 74 (39.2%) | 0.645 |
| YES | 61 (58.1%) | 44 (41.9%) | ||
| Father annual dental visits | 0 | 22 (66.7%) | 11 (33.3%) | 0.39 |
| 1 | 76 (62.8%) | 45 (37.2%) | ||
| 2 | 78 (56.1%) | 61 (43.9%) | ||
| Father caries | NO | 40 (56.3%) | 31 (43.7%) | 0.486 |
| YES | 136 (61%) | 87 (39%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciribè, M.; Galeotti, A.; Dolci, C.; Gargiullo, L.; Mammone, M.; Cirillo, E.; Festa, P.; La Torre, G. Cross Sectional Study on the Association between Dental Caries and Life Habits in School Age Italian Children. Healthcare 2022, 10, 607. https://doi.org/10.3390/healthcare10040607
Ciribè M, Galeotti A, Dolci C, Gargiullo L, Mammone M, Cirillo E, Festa P, La Torre G. Cross Sectional Study on the Association between Dental Caries and Life Habits in School Age Italian Children. Healthcare. 2022; 10(4):607. https://doi.org/10.3390/healthcare10040607
Chicago/Turabian StyleCiribè, Massimiliano, Angela Galeotti, Chiara Dolci, Livia Gargiullo, Martina Mammone, Erika Cirillo, Paola Festa, and Giuseppe La Torre. 2022. "Cross Sectional Study on the Association between Dental Caries and Life Habits in School Age Italian Children" Healthcare 10, no. 4: 607. https://doi.org/10.3390/healthcare10040607