
Effectiveness of Three Agents in Pulpotomy Treatment of Permanent Molars with Incomplete Root Development: A Randomized Controlled Trial


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
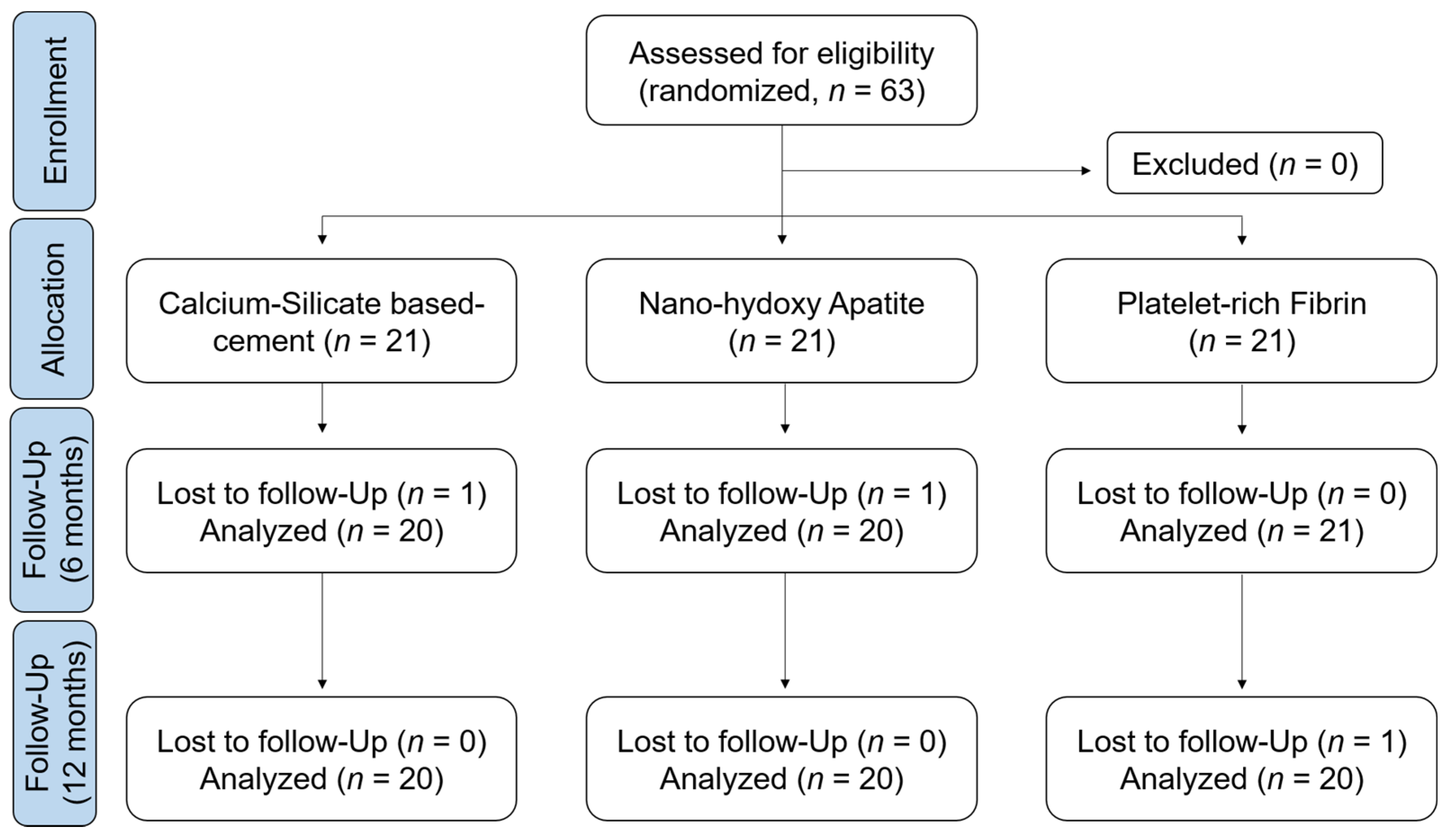
2.1. Study Design
2.2. Study Participants
- -
- Children aged between 6 and 12 years;
- -
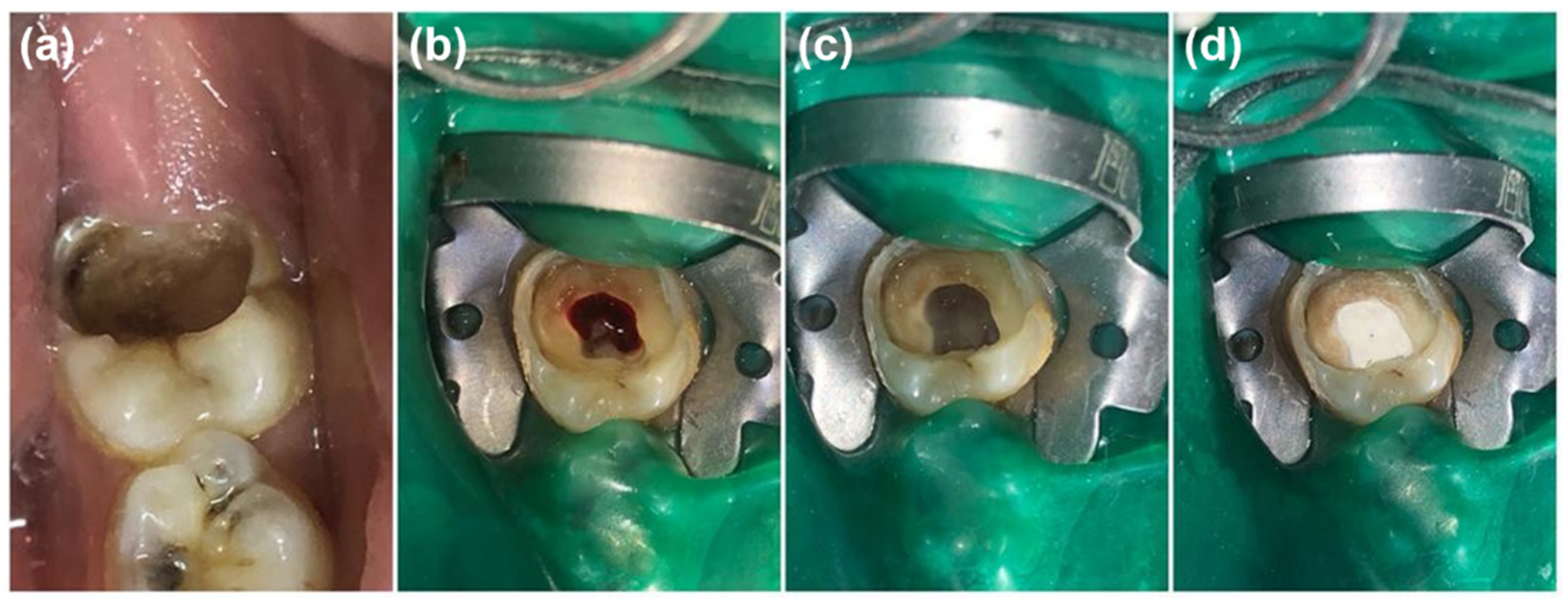
- Symptomatic/Asymptomatic vital permanent molars with deep caries lesion close to the pulp chamber roof or with clinical carious exposure of the pulp after spoon excavation or with pulp exposure after trauma (within 48 h) and the existence of bleeding upon exposure;
- -
- Incomplete root development visible in the radiograph;
- -
- Intraoperative bleeding time of radicular pulp not exceeding 5 min;
- -
- Physiological mobility;
- -
- Restorable crown.
- -
- History of systemic disease or allergic reaction;
- -
- History of spontaneous pain;
- -
- Presence of external or internal resorption;
- -
- Apical or inter-radicular lesion.
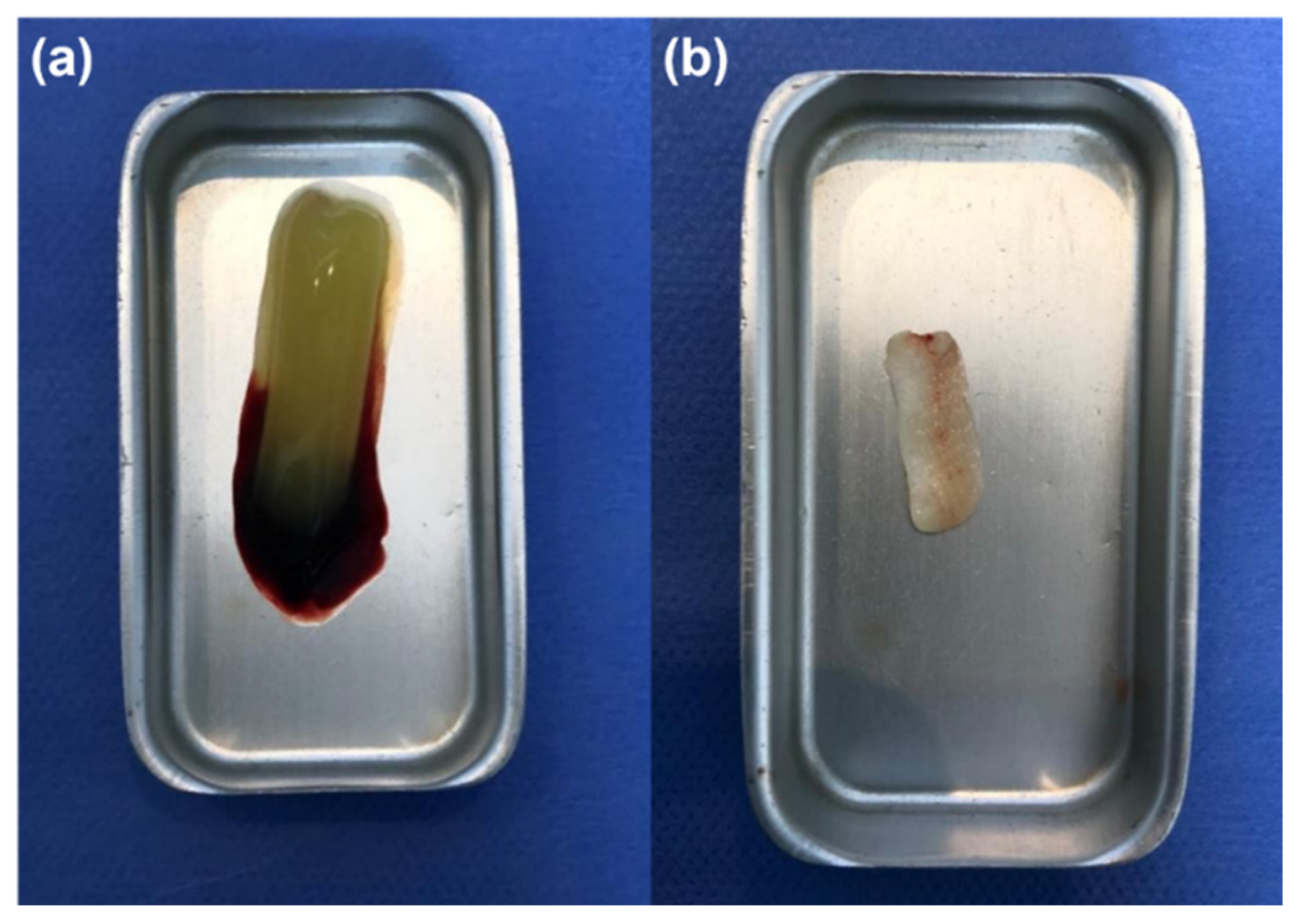
2.3. Study Intervention
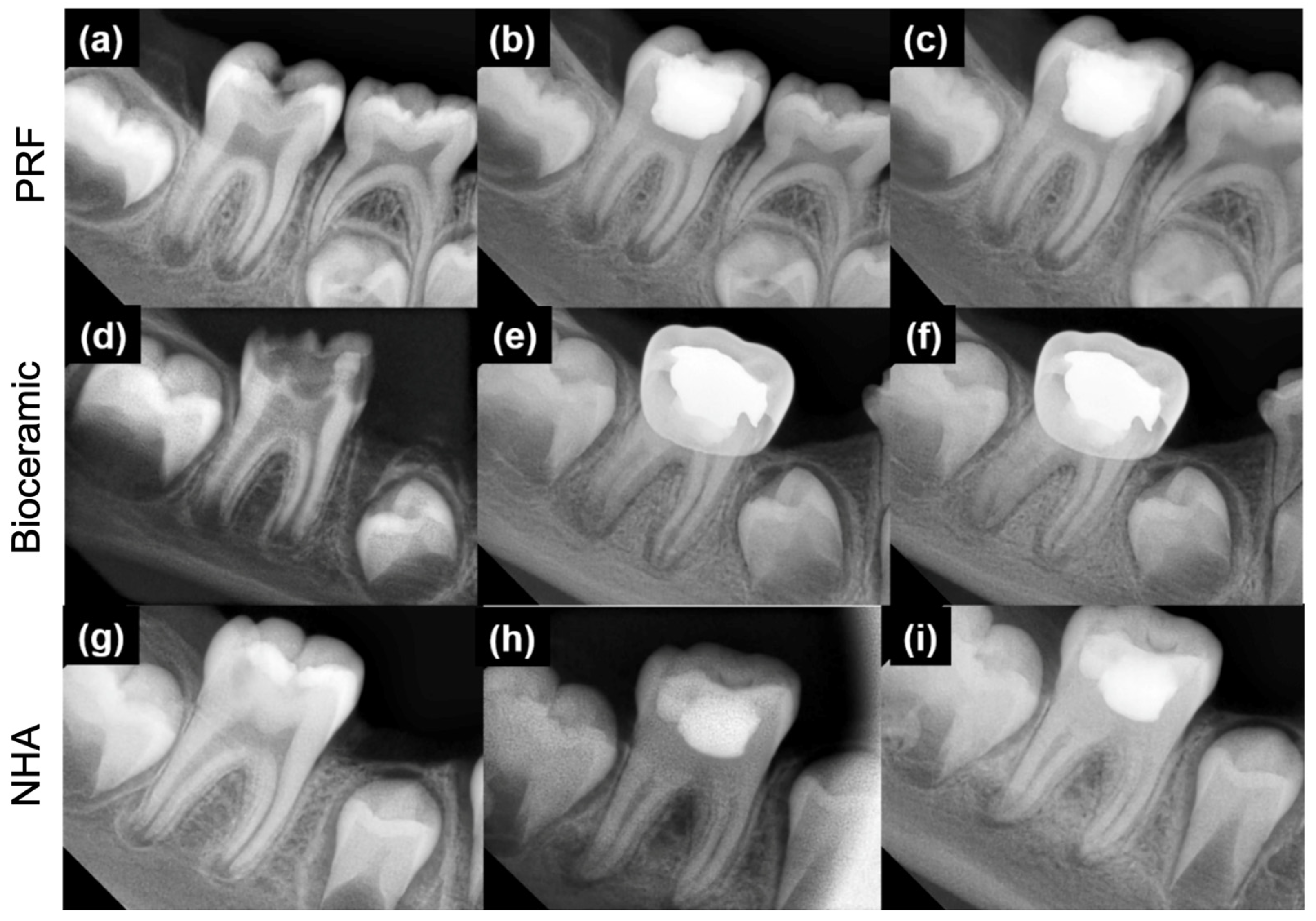
2.4. Study Follow-Up and Evaluation
2.5. Statistical Analysis
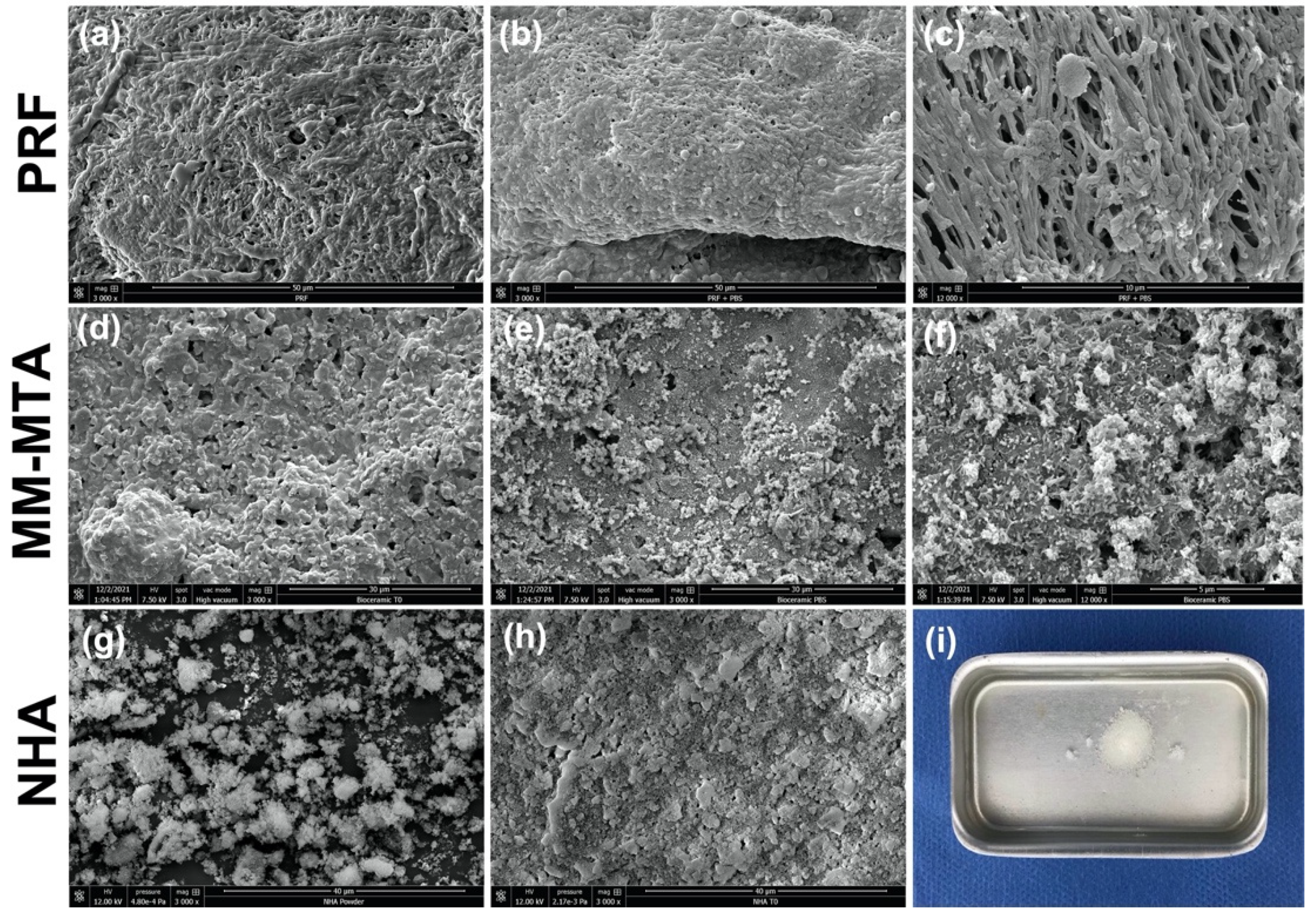
2.6. Scanning Electron Microscopy Analysis (SEM)
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W.; GBD 2015 Oral Health Collaborators. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Heng, C. Tooth Decay Is the Most Prevalent Disease. Fed. Pract. 2016, 33, 31–33. [Google Scholar] [PubMed]
- Emmanuelli, B.; Knorst, J.K.; Menegazzo, G.R.; Mendes, F.M.; Ardenghi, T.M. The Impact of Early Childhood Factors on Dental Caries Incidence in First Permanent Molars: A 7-Year Follow-Up Study. Caries Res. 2021, 55, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Satcher, D.; Nottingham, J.H. Revisiting Oral Health in America: A Report of the Surgeon General. Am. J. Public Health 2017, 107, S32–S33. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Chen, Y.; Yu, Y.; Xie, Y.; Zhu, H.; Wang, H. Caries prevalence of the first permanent molars in 6–8 years old children. PLoS ONE 2021, 16, e0245345. [Google Scholar] [CrossRef]
- Bhardwaj, V.K. Dental caries prevalence in individual tooth in primary and permanent dentition among 6–12-year-old school children in Shimla, Himachal Pradesh. Int. J. Health Appl. Sci. 2014, 3, 125. [Google Scholar] [CrossRef] [Green Version]
- Kaklamanos, E.G.; Lazaridou, D.; Tsiantou, D.; Kotsanos, N.; Athanasiou, A.E. Dental arch spatial changes after premature loss of first primary molars: A systematic review of controlled studies. Odontology 2017, 105, 364–374. [Google Scholar] [CrossRef]
- Noor Mohamed, R.; Basha, S.; Al-Thomali, Y. Efficacy of platelet concentrates in pulpotomy—A systematic review. Platelets 2018, 29, 440–445. [Google Scholar] [CrossRef]
- American Academy of Pediatric Dentistry. Clinical guidelines on pulp therapy for primary and young permanent teeth: Reference manual 2011–2012. Pediatr. Dent. 2011, 33, 212–219. [Google Scholar]
- Kumar, V.; Juneja, R.; Duhan, J.; Sangwan, P.; Tewari, S. Comparative evaluation of platelet-rich fibrin, mineral trioxide aggregate, and calcium hydroxide as pulpotomy agents in permanent molars with irreversible pulpitis: A randomized controlled trial. Contemp. Clin. Dent. 2016, 7, 512–518. [Google Scholar]
- Keswani, D.; Pandey, R.K.; Ansari, A.; Gupta, S. Comparative evaluation of platelet-rich fibrin and mineral trioxide aggregate as pulpotomy agents in permanent teeth with incomplete root development: A randomized controlled trial. J. Endod. 2014, 40, 599–605. [Google Scholar] [CrossRef]
- American Association of Neurological Surgeons (AANS); American Society of Neuroradiology (ASNR); Cardiovascular and Interventional Radiology Society of Europe (CIRSE); Canadian Interventional Radiology Association (CIRA); Congress of Neurological Surgeons (CNS); European Society of Minimally Invasive Neurological Therapy (ESMINT); European Society of Neuroradiology (ESNR); European Stroke Organization (ESO); Society for Cardiovascular Angiography and Interventions (SCAI); Society of Interventional Radiology (SIR); et al. Multisociety Consensus Quality Improvement Revised Consensus Statement for Endovascular Therapy of Acute Ischemic Stroke. Int. J. Stroke 2018, 13, 612–632. [Google Scholar]
- Mohammad, N.S.; Nazli, R.; Zafar, H.; Fatima, S. Effects of lipid based Multiple Micronutrients Supplement on the birth outcome of underweight pre-eclamptic women: A randomized clinical trial. Pak. J. Med. Sci. 2022, 38, 219–226. [Google Scholar] [PubMed]
- Cushley, S.; Duncan, H.F.; Lappin, M.J.; Tomson, P.L.; Lundy, F.T.; Cooper, P.; Clarke, M.; El Karim, I.A. Pulpotomy for mature carious teeth with symptoms of irreversible pulpitis: A systematic review. J. Dent. 2019, 88, 103158. [Google Scholar] [CrossRef] [PubMed]
- Aminabadi, N.A.; Parto, M.; Emamverdizadeh, P.; Jamali, Z.; Shirazi, S. Pulp bleeding color is an indicator of clinical and histohematologic status of primary teeth. Clin. Oral Investig. 2017, 21, 1831–1841. [Google Scholar] [CrossRef]
- Rechenberg, D.K.; Galicia, J.C.; Peters, O.A. Biological Markers for Pulpal Inflammation: A Systematic Review. PLoS ONE 2016, 11, e0167289. [Google Scholar] [CrossRef] [Green Version]
- European Society of Endodontology (ESE); Duncan, H.F.; Galler, K.M.; Tomson, P.L.; Simon, S.; El-Karim, I.; Kundzina, R.; Krastl, G.; Dammaschke, T.; Fransson, H.; et al. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. Int. Endod. J. 2019, 52, 923–934. [Google Scholar]
- American Association of Endodontists. Available online: https://www.aae.org/specialty/clinical-resources/guidelines-position-statements/ (accessed on 20 February 2022).
- Taha, N.A.; Khazali, M.A. Partial Pulpotomy in Mature Permanent Teeth with Clinical Signs Indicative of Irreversible Pulpitis: A Randomized Clinical Trial. J. Endod. 2017, 43, 1417–1421. [Google Scholar] [CrossRef]
- Hilton, T.J.; Ferracane, J.L.; Mancl, L. Northwest Practice-based Research Collaborative in Evidence-based Dentistry (NWP). Comparison of CaOH with MTA for direct pulp capping: A PBRN randomized clinical trial. J. Dent. Res. 2013, 92, 16S–22S. [Google Scholar] [CrossRef] [Green Version]
- Aeinehchi, M.; Eslami, B.; Ghanbariha, M.; Saffar, A.S. Mineral trioxide aggregate (MTA) and calcium hydroxide as pulp-capping agents in human teeth: A preliminary report. Int. Endod. J. 2003, 36, 225–231. [Google Scholar] [CrossRef]
- Parirokh, M.; Torabinejad, M.; Dummer, P.M.H. Mineral trioxide aggregate and other bioactive endodontic cements: An updated overview—Part I: Vital pulp therapy. Int. Endod. J. 2018, 51, 177–205. [Google Scholar] [CrossRef] [PubMed]
- Wongwatanasanti, N.; Jantarat, J.; Sritanaudomchai, H.; Hargreaves, K.M. Effect of Bioceramic Materials on Proliferation and Odontoblast Differentiation of Human Stem Cells from the Apical Papilla. J. Endod. 2018, 44, 1270–1275. [Google Scholar] [CrossRef] [PubMed]
- MacInnes, A. What is the most effective endodontic medicament for pulpotomies in immature permanent teeth? Evid. Based Dent. 2020, 21, 108–109. [Google Scholar] [CrossRef] [PubMed]
- Choukroun, J.; Adda, F.; Schoeffler, C.; Vervelle, A.P. Une opportunité en paro-implantologie: Le PRF. Implantodontie 2001, 42, e62. [Google Scholar]
- Fan, B.; Yi, M.; Yang, G.; Yang, L.; Shang, W.; Liu, Y.; Zhong, X.; Zhu, L.; Wang, D. Expanded validation of the effect and quality of a pathogen inactivation system based on riboflavin photochemistry on platelet bacterial contamination. Ann. Transl. Med. 2021, 9, 1736. [Google Scholar] [CrossRef]
- Geeta, I.B.; Galagali, G.; Kulkarni, S.; Suran, P.; Noushin, F. A natural meliorate: Revolutionary tissue engineering in endodontics. J. Clin. Diagn. Res. 2013, 7, 2644–2646. [Google Scholar]
- Mohamed, D.A.; Abdelfattah, M.I.; Aboulezz, E.H.A. The Effect of Three Different Biomaterials on Proliferation and Viability of Human Dental Pulp Stem Cells (In-vitro Study). Open Access Maced. J. Med. Sci. 2017, 5, 657–663. [Google Scholar] [CrossRef] [Green Version]
- Saini, N.; Mathur, S.; Saini, V.; Kapoor, A.; Vijay, S.; Gurjar, S. Effect of commercially available nano-hydroxy apatite containing desensitizing mouthwash on dentinal tubular occlusion: An in vitro FESEM analysis. Med. Pharm. Rep. 2020, 93, 396–404. [Google Scholar] [CrossRef]
- Turkez, H.; Yousef, M.I.; Sönmez, E.; Togar, B.; Bakan, F.; Sozio, P.; Stefano, A.D. Evaluation of cytotoxic, oxidative stress and genotoxic responses of hydroxyapatite nanoparticles on human blood cells. J. Appl. Toxicol. 2014, 34, 373–379. [Google Scholar] [CrossRef]
- Haghgoo, R.; Asgary, S.; Mashhadi Abbas, F.; Montazeri Hedeshi, R. Nano-hydroxyapatite and calcium-enriched mixture for pulp capping of sound primary teeth: A randomized clinical trial. Iran. Endod. J. 2015, 10, 107–111. [Google Scholar]
- Swarup, S.J.; Rao, A.; Boaz, K.; Srikant, N.; Shenoy, R. Pulpal response to nano hydroxyapatite, mineral trioxide aggregate and calcium hydroxide when used as a direct pulp capping agent: An in vivo study. J. Clin. Pediatr. Dent. 2014, 38, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Shayegan, A.; Atash, R.; Petein, M.; Abbeele, A.V. Nanohydroxyapatite used as a pulpotomy and direct pulp capping agent in primary pig teeth. J. Dent. Child. 2010, 77, 77–83. [Google Scholar]
- Ricucci, D.; Loghin, S.; Lin, L.M.; Spångberg, L.S.; Tay, F.R. Is hard tissue formation in the dental pulp after the death of the primary odontoblasts a regenerative or a reparative process? J. Dent. 2014, 42, 1156–1170. [Google Scholar] [CrossRef] [PubMed]
- Pednekar, A.; Ataide, I.; Fernandes, M.; Lambor, R.; Soares, R. Spectrophotometric Analysis of Coronal Discolouration Induced by ProRoot MTA, Biodentine and MTA Repair HP Used for Pulpotomy Procedures. Eur. Endod. J. 2021, 6, 189–196. [Google Scholar]
- Uyar, D.S.; Alacam, A. Evaluation of partial pulpotomy treatment in cariously exposed immature permanent molars: Randomized controlled trial. Niger. J. Clin. Pract. 2021, 24, 1511–1519. [Google Scholar] [CrossRef]
- Poggio, C.; Trovati, F.; Ceci, M.; Colombo, M.; Pietrocola, G. Antibacterial activity of different root canal sealers against Enterococcus faecalis. J. Clin. Exp. Dent. 2017, 9, e743–e748. [Google Scholar] [CrossRef] [Green Version]
- Kharouf, N.; Hemmerlé, J.; Haikel, Y.; Mancino, D. Technical Quality of Root Canal Filling in Preclinical Training at Strasbourg University Using Two Teaching Protocols. Eur. J. Dent. 2019, 13, 521–526. [Google Scholar] [CrossRef] [Green Version]
- Abuelniel, G.M.; Duggal, M.S.; Kabel, N. A comparison of MTA and Biodentine as medicaments for pulpotomy in traumatized anterior immature permanent teeth: A randomized clinical trial. Dent. Traumatol. 2020, 36, 400–410. [Google Scholar] [CrossRef]
- Lima, S.P.R.; Santos, G.L.D.; Ferelle, A.; Ramos, S.P.; Pessan, J.P.; Dezan-Garbelini, C.C. Clinical and radiographic evaluation of a new stain-free tricalcium silicate cement in pulpotomies. Braz. Oral Res. 2020, 34, e102. [Google Scholar] [CrossRef]
- Kharouf, N.; Zghal, J.; Addiego, F.; Gabelout, M.; Jmal, H.; Haikel, Y.; Bahlouli, N.; Ball, V. Tannic acid speeds up the setting of mineral trioxide aggregate cements and improves its surface and bulk properties. J. Colloid Interface Sci. 2021, 589, 318–326. [Google Scholar] [CrossRef]
- Debelian, G.; Trope, M. The use of premixed bioceramic materials in endodontics. G. Ital. Di Endod. 2016, 30, 70–80. [Google Scholar] [CrossRef] [Green Version]
- Kharouf, N.; Arntz, Y.; Eid, A.; Zghal, J.; Sauro, S.; Haikel, Y.; Mancino, D. Physicochemical and Antibacterial Properties of Novel, Premixed Calcium Silicate-Based Sealer Compared to Powder–Liquid Bioceramic Sealer. J. Clin. Med. 2020, 9, 3096. [Google Scholar] [CrossRef] [PubMed]
- Khalil, I.T.; Sarkis, T.; Naaman, A. MM-MTA for direct pulp capping: A histologic comparison with ProRoot MTA in rat molars. J. Contemp. Dent. Pract. 2013, 14, 1019–1023. [Google Scholar] [PubMed]
- American Academy of Pediatric Dentistry. Guideline on pulp therapy for primary and immature permanent teeth. Pediatr. Dent. 2016, 38, 280–288. [Google Scholar]
- Mielke, C.H., Jr.; Kaneshiro, M.M.; Maher, I.A.; Weiner, J.M.; Rapaport, S.I. The standardized normal Ivy bleeding time and its prolongation by aspirin. Blood 1969, 34, 204–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Academy of Pediatric Dentistry. Pulp Therapy for Primary and Immature Permanent Teeth. The Reference Manual of Pediatric Dentistry; American Academy of Pediatric Dentistry: Elk Grove Village, IL, USA, 2021; pp. 399–407. [Google Scholar]
- Kharouf, N.; Mancino, D.; Zghal, J.; Helle, S.; Jmal, H.; Lenertz, M.; Viart, N.; Bahlouli, N.; Meyer, F.; Haikel, Y.; et al. Dual role of tannic acid and pyrogallol incorporated in plaster of Paris: Morphology modification and release for antimicrobial properties. Mater. Sci. Eng. C Mater. Biol. Appl. 2021, 127, 112209. [Google Scholar] [CrossRef]
- Vu, T.T.; Nguyen, M.T.; Sangvanich, P.; Nguyen, Q.N.; Thunyakitpisal, P. Acemannan Used as an Implantable Biomaterial for Vital Pulp Therapy of Immature Permanent Teeth Induced Continued Root Formation. Pharmaceutics 2020, 12, 644. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part II: Platelet-related biologic features. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e45–e50. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part III: Leucocyte activation: A new feature for platelet concentrates? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e51–e55. [Google Scholar] [CrossRef]
- Toffler, M.; Toscano, N.; Holtzclaw, D.; Corso, M.D.; Ehrenfest, D.D. Introducing Choukroun’s Platelet Rich Fibrin (PRF) to the Reconstructive Surgery Milieu. J. Implant. Adv. Clin. Dent. 2009, 1, 21–32. [Google Scholar]
- Choukroun, J.; Diss, A.; Simonpieri, A.; Girard, M.O.; Schoeffler, C.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Dohan, D.M. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part IV: Clinical effects on tissue healing. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e56–e60. [Google Scholar] [CrossRef] [PubMed]
- Hiremath, H.; Saikalyan, S.; Kulkarni, S.S.; Hiremath, V. Second-generation platelet concentrate (PRF) as a pulpotomy medicament in a permanent molar with pulpitis: A case report. Int. Endod. J. 2012, 45, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Camps, J.; Jeanneau, C.; El Ayachi, I.; Laurent, P.; About, I. Bioactivity of a Calcium Silicate-based Endodontic Cement (BioRoot RCS): Interactions with Human Periodontal Ligament Cells In Vitro. J. Endod. 2015, 41, 1469–1473. [Google Scholar] [CrossRef] [PubMed]
- Landi, E.; Celotti, G.; Logroscino, G.; Tampieri, A. Carbonated hydroxyapatite as bone substitute. J. Eur. Ceram. Soc. 2003, 23, 2931–2937. [Google Scholar] [CrossRef]
- Nasrallah, H.; El Noueiri, B.; Pilipili, C.; Ayoub, F. Clinical and Radiographic Evaluations of Biodentine™ Pulpotomies in Mature Primary Molars (Stage 2). Int. J. Clin. Pediatr. Dent. 2018, 11, 496–504. [Google Scholar]
- Rajasekharan, S.; Martens, L.C.; Vandenbulcke, J.; Jacquet, W.; Bottenberg, P.; Cauwels, R.G. Efficacy of three different pulpotomy agents in primary molars: A randomized control trial. Int. Endod. J. 2017, 50, 215–228. [Google Scholar] [CrossRef] [PubMed]
- Patidar, S.; Kalra, N.; Khatri, A.; Tyagi, R. Clinical and radiographic comparison of platelet-rich fibrin and mineral trioxide aggregate as pulpotomy agents in primary molars. J. Indian Soc. Pedod. Prev. Dent. 2017, 35, 367–373. [Google Scholar] [PubMed]
- Grossman, L.I. Endodontic Practice; Lea & Febiger: Philadelphia, PA, USA, 1978. [Google Scholar]
- Duarte, M.A.H.; Marciano, M.A.; Vivan, R.R.; Tanomaru Filho, M.; Tanomaru, J.M.G.; Camilleri, J. Tricalcium silicate-based cements: Properties and modifications. Braz. Oral Res. 2018, 32, e70. [Google Scholar] [CrossRef] [Green Version]
- Kwon, S.-Y.; Seo, M.-S. Comparative evaluation of volumetric changes of three different retrograde calcium silicate materials placed under different pH condititions. BMC Oral Health 2020, 20, 330. [Google Scholar] [CrossRef]
- Camilleri, J. Characterization and hydration kinetics of tricalcium silicate cement for use as a dental biomaterial. Dent. Mater. 2011, 27, 836–844. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria/Group | MM-MTA (G1) | Nano-Hydroxyapatite (G2) | PRF (G3) | Statistical Analysis |
|---|---|---|---|---|
| Age (years) | 8.6 ± 2.0 | 8.8 ± 1.8 | 8.8 ± 2.1 | p = 0.911 |
| Sex females (%) | 11 (55) | 10 (50) | 9 (45) | p = 0.819 |
| Apical closure complete (6 months) (%) | 5 (25) | 3 (15) | 4 (19.04) | p = 0.726 |
| Apical closure complete (12 months) (%) | 10 (50) | 11 (55) | 12 (60) | p = 0.817 |
| Canal obliteration (6 months) (%) | 3 (15) | 4 (20) | 0 (0) | p = 0.111 |
| Canal obliteration (12 months) (%) | 7 (35) | 9 (45) | 1 (5) | p = 0.014 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eid, A.; Mancino, D.; Rekab, M.S.; Haikel, Y.; Kharouf, N. Effectiveness of Three Agents in Pulpotomy Treatment of Permanent Molars with Incomplete Root Development: A Randomized Controlled Trial. Healthcare 2022, 10, 431. https://doi.org/10.3390/healthcare10030431
Eid A, Mancino D, Rekab MS, Haikel Y, Kharouf N. Effectiveness of Three Agents in Pulpotomy Treatment of Permanent Molars with Incomplete Root Development: A Randomized Controlled Trial. Healthcare. 2022; 10(3):431. https://doi.org/10.3390/healthcare10030431
Chicago/Turabian StyleEid, Ammar, Davide Mancino, Mohammad Salem Rekab, Youssef Haikel, and Naji Kharouf. 2022. "Effectiveness of Three Agents in Pulpotomy Treatment of Permanent Molars with Incomplete Root Development: A Randomized Controlled Trial" Healthcare 10, no. 3: 431. https://doi.org/10.3390/healthcare10030431