
Subcutaneous Emphysema Related to Dental Treatment: A Case Series

 , ,
, ,
Abstract
:1. Introduction
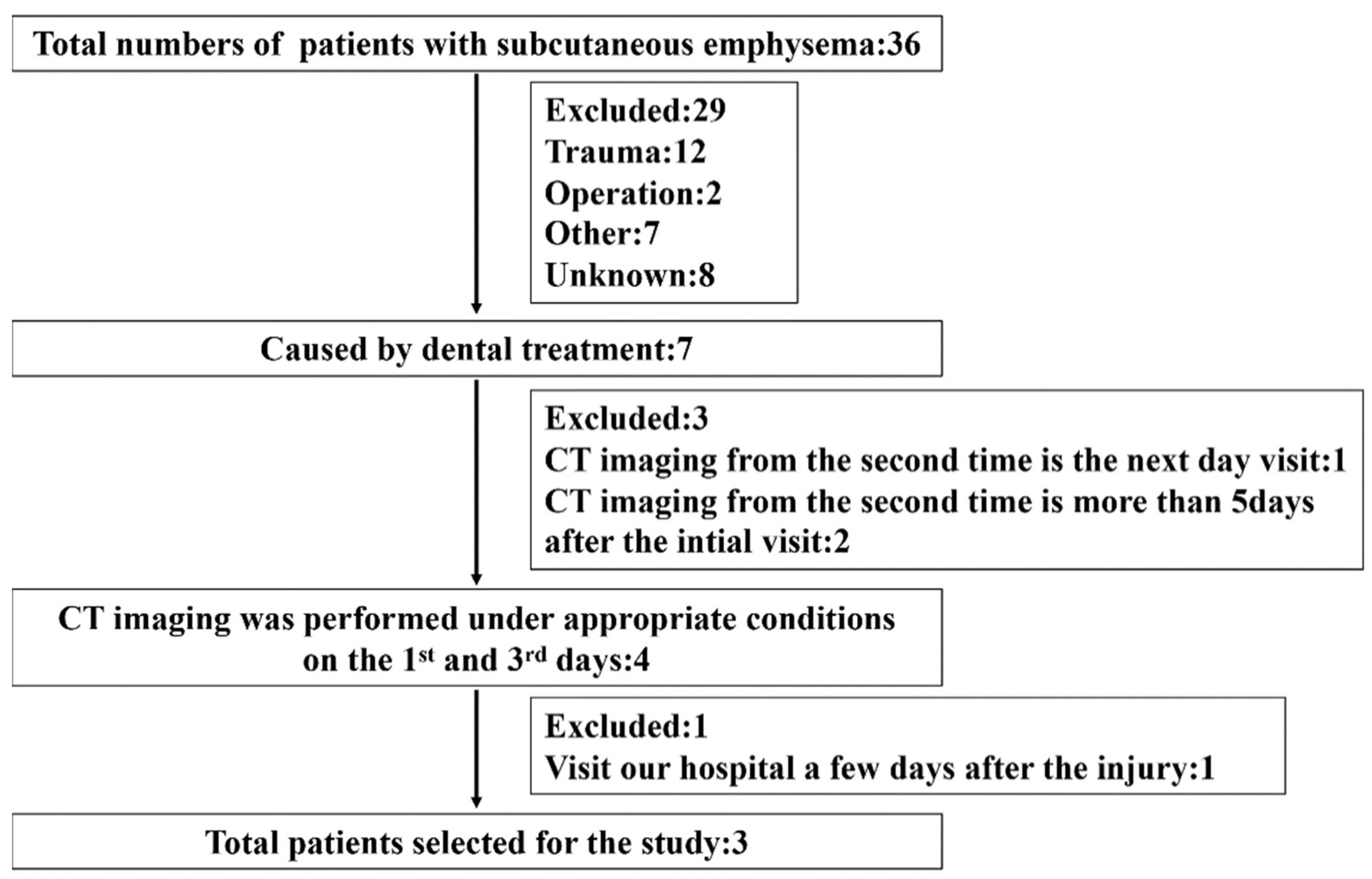
2. Case Series and Methods
- SE caused by dental treatment;
- SE spanning multiple areas;
- CT was performed under appropriate conditions on the 1st and 3rd days of onset;
- The CT requirements for this research protocol were as follows:
- Use of a non-enhanced multidetector CT scanner (Aquilion; Toshiba Medical Systems, Tokyo, Japan);
- The CT acquisition parameters at our department of matrix were as follows: tube voltage 120 kVp; tube current 100 mA; 512 × 512 pixels; 1 mm slice thickness; 1 mm speed per rotation; 1 mm reconstructed slice increment; and 0° reconstruction algorithm bone gantry tilt;
- Performing a multi-section reconstruction on an image processing workstation using each parameter;
- Measurements being made on a high-resolution monitor of bone mode images;
- Exclusion criteria:
- SE of unknown causes;
- SE due to trauma, operation, thotacolaparotomy, and thoracentesis;
- CT at the second visit was performed the next day or more than 5 days after the initial visit;
- Visiting our hospital a few days after the injury.
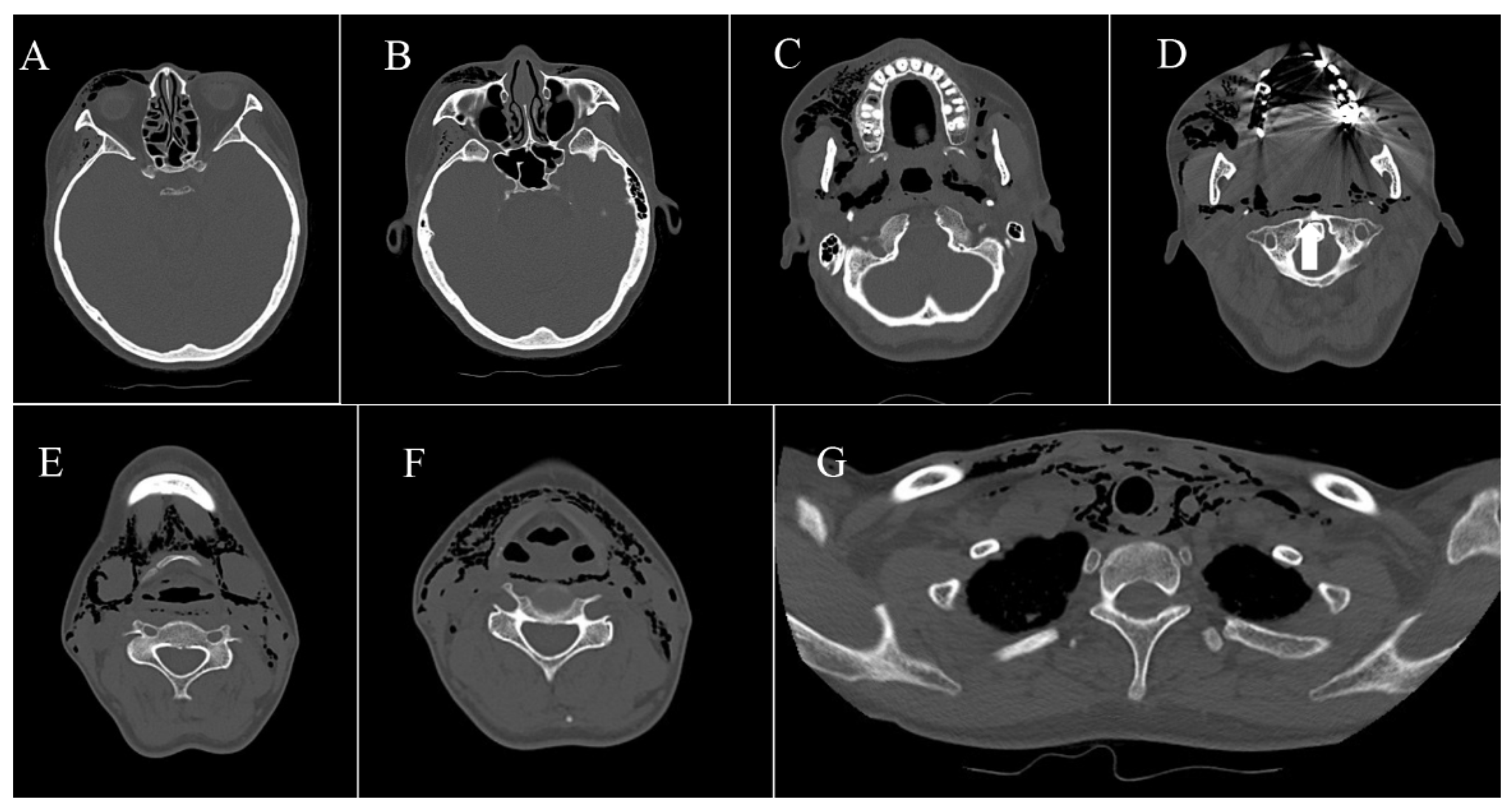
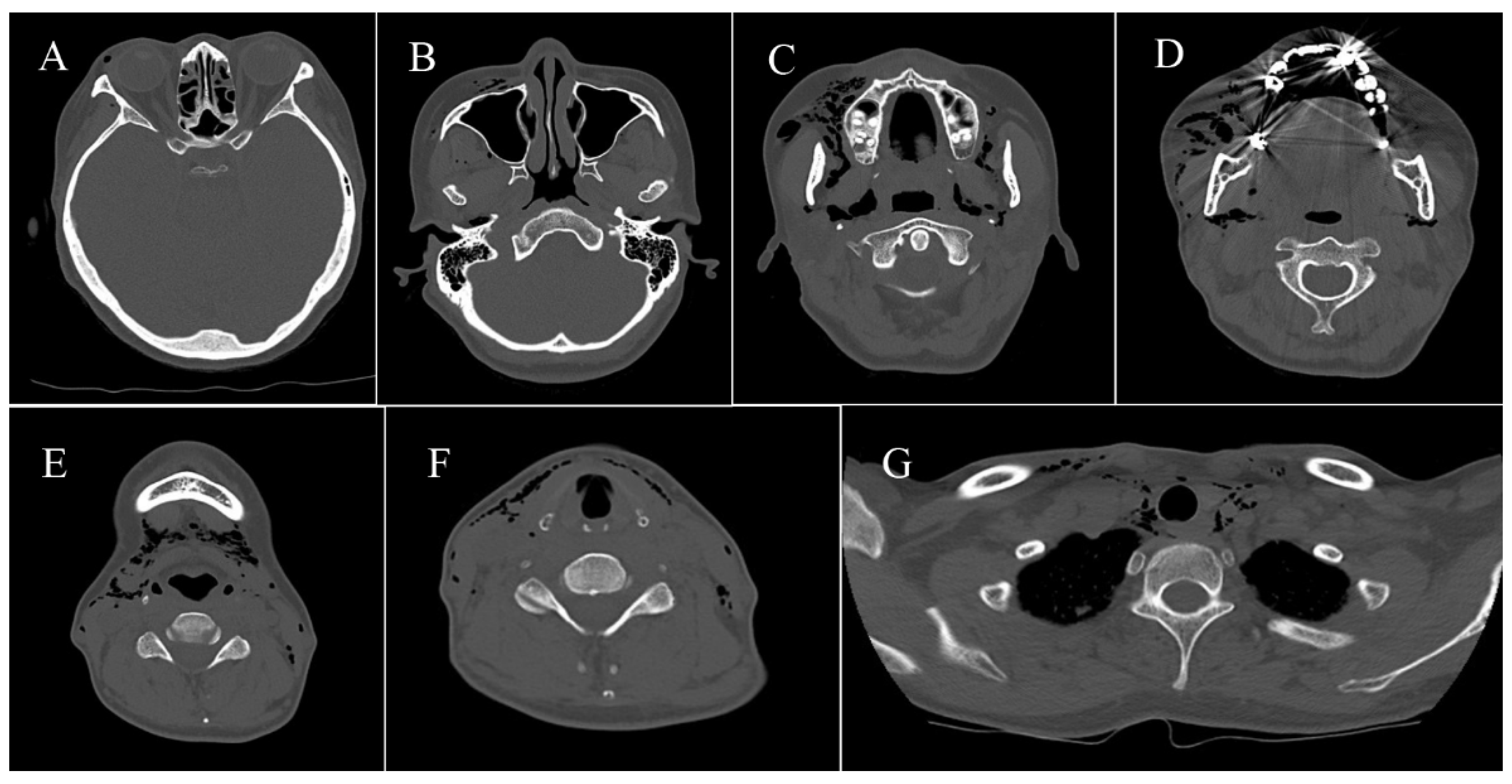
2.1. Range of Spread to Each Gap of SE
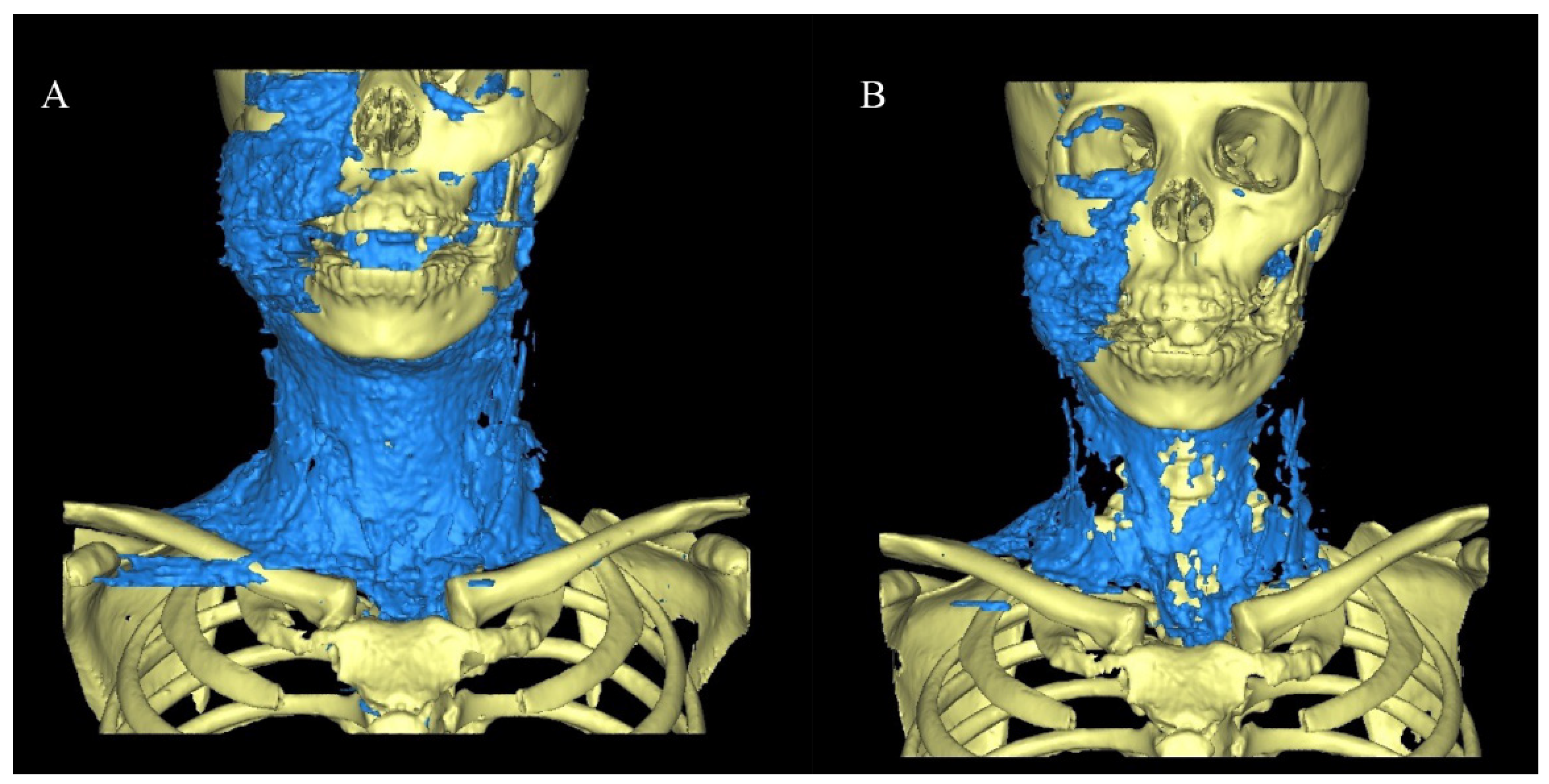
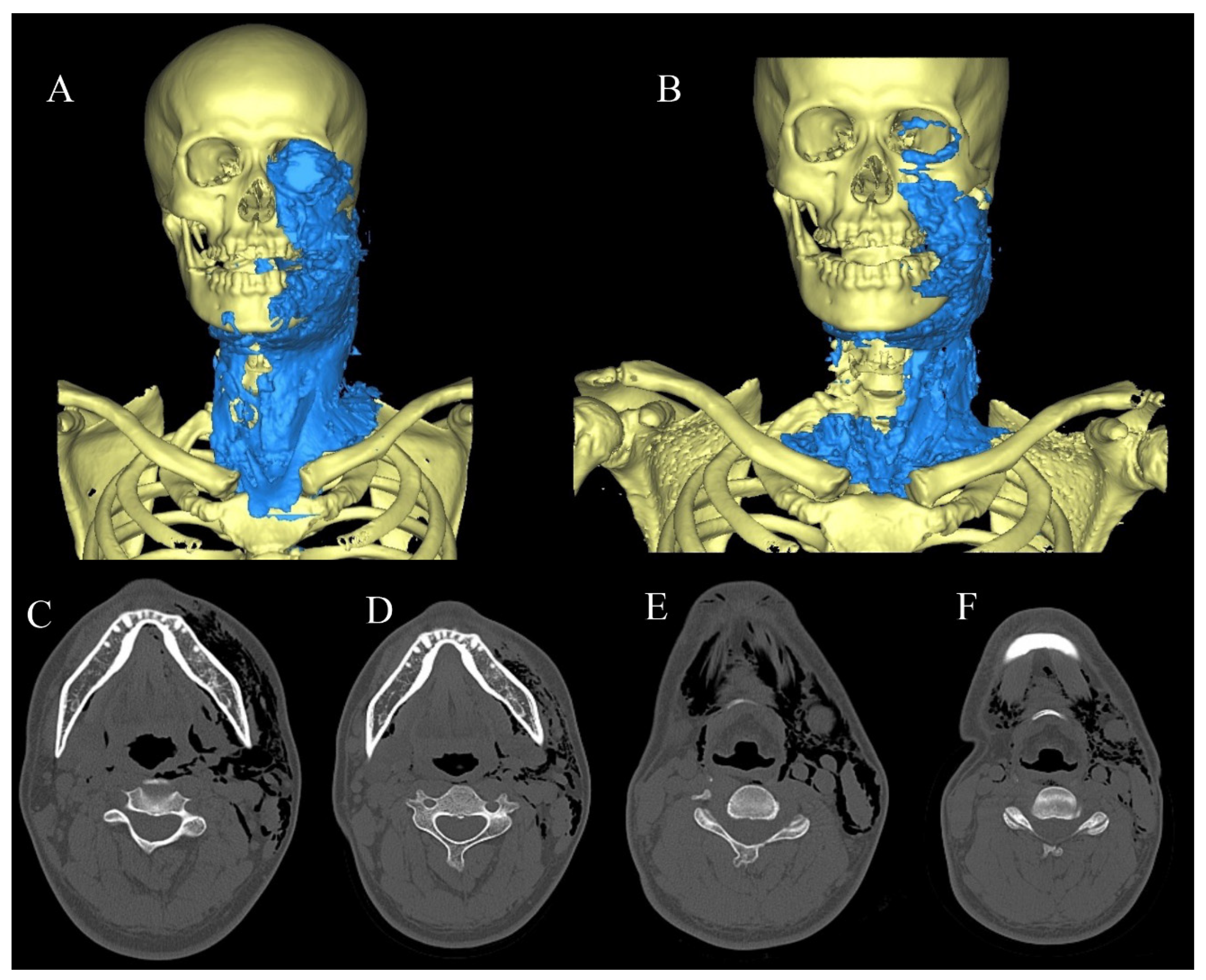
2.2. SE Volume Measurement Method
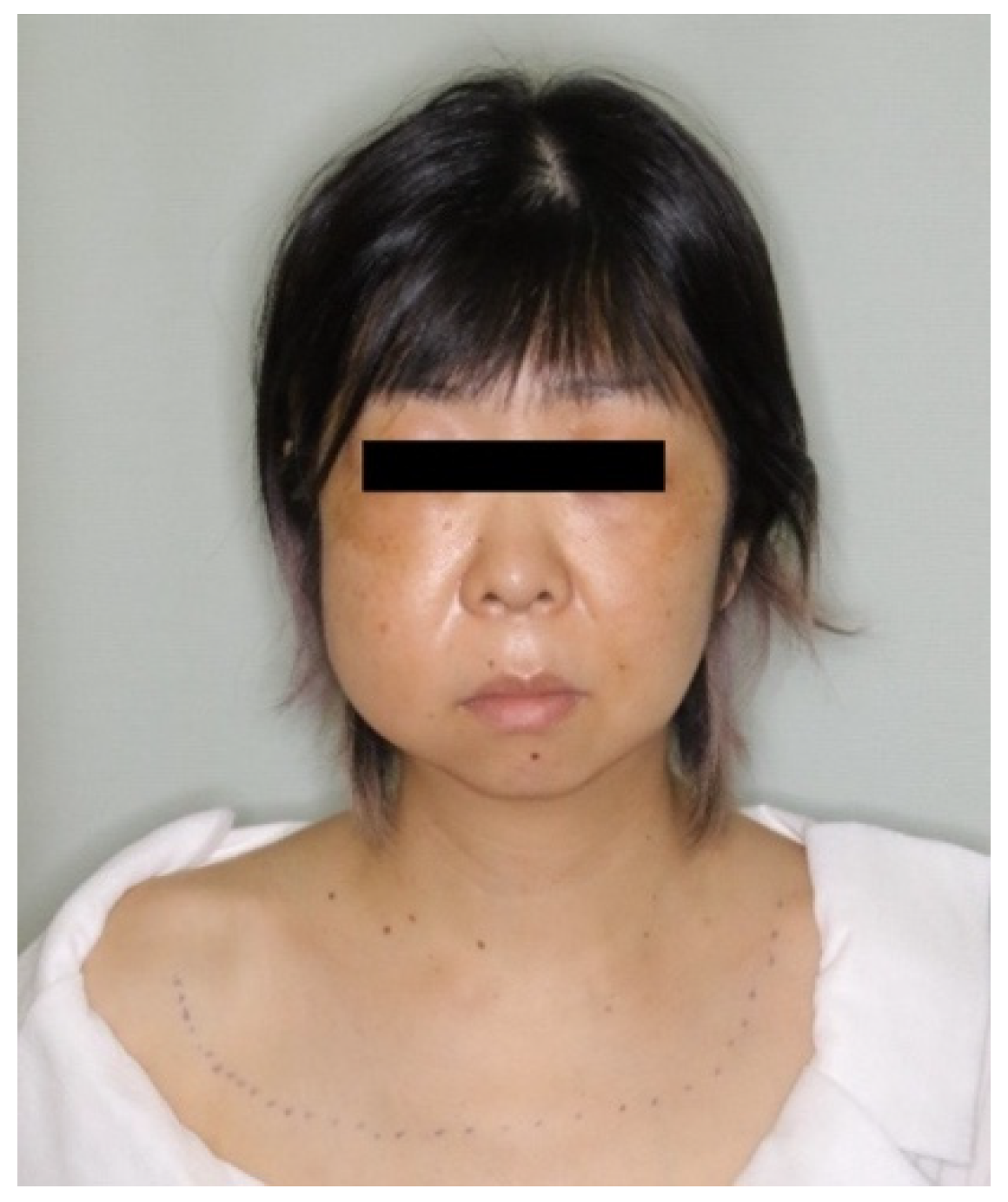
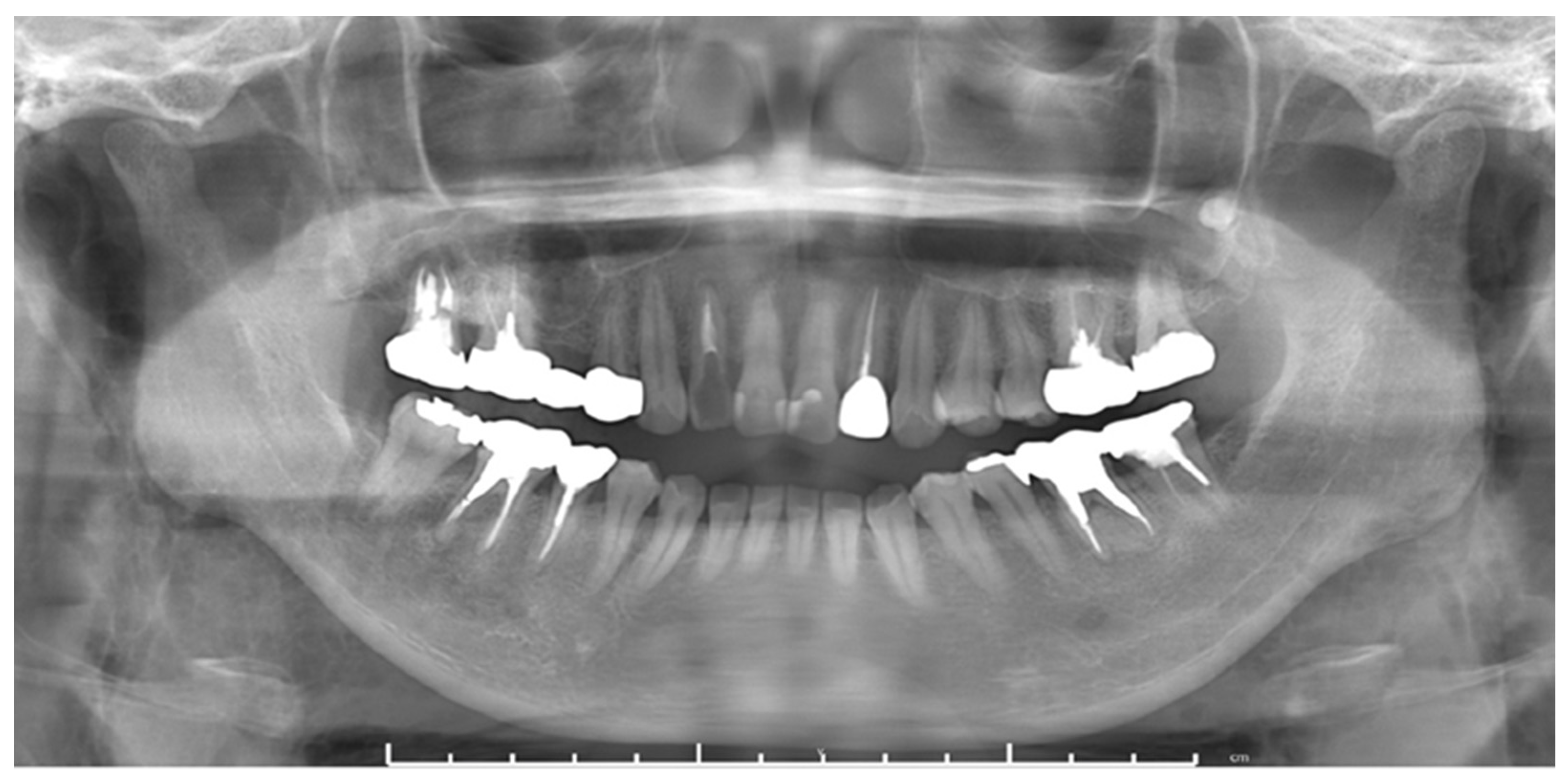
2.3. Case Series
2.3.1. Case 1
2.3.2. Case 2
2.3.3. Case 3
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chiou, B.J.; Chou, S.J.; Ho, D.C.; Fang, C.Y. Extraction with an electric motor-driven handpiece may still cause subcutaneous emphysema—A case report. J. Dent. Sci 2021, 16, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Rawlinson, R.D.; Negmadjanov, U.; Rubay, D.; Ohanisian, L.; Waxman, J. Pneumomediastinum After Dental Filling: A Rare Case Presentation. Cureus 2019, 11, e5593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, L.; Patnaik, S.; Patro, S.; Debnath, N.; Mishra, S. Iatrogenic subcutaneous emphysema of endodontic origin—Case report with literature review. J. Clin. Diagn. Res. 2014, 8, 279–281. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Lazow, S.K.; Berger, J. Cervicofacial subcutaneous emphysema: Case report and review of literature. J. Oral Maxillofac. Surg. 2010, 68, 1976–1982. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.; Stagnell, S.; Renton, T.; Aggarwal, V.R.; Moore, R. Causes of subcutaneous emphysema following dental procedures: A systematic review of cases 1993–2020. Br. Dent. J. 2021, 231, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Imhof, H.; Czerny, C. A Dirisamer. Head and neck imaging with MDCT. Eur. J. Radiol. 2003, 45, 23–31. [Google Scholar] [CrossRef]
- Sukegawa, S.; Masui, M.; Kanno, T.; Miki, M.; Nakamoto, H.; Furuki, Y. Evaluation of Open Reduction and Internal Fixation of Mandibular Condyle Fracture by Intraoperative Cone-Beam Computed Tomography in a Hybrid Operating Room. J. Craniofac. Surg. 2020, 31, 762–765. [Google Scholar] [CrossRef] [PubMed]
- Bocchialini, G.; Ambrosi, S.; Castellani, A. Massive Cervicothoracic Subcutaneous Emphysema and Pneumomediastinum Developing during a Dental Hygiene Procedure. Case Rep. Dent. 2017, 2017, 7016467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitsunaga, S.; Iwai, T.; Kitajima, H.; Yajima, Y.; Ohya, T.; Hirota, M.; Mitsudo, K.; Aoki, N.; Yamashita, Y.; Omura, S.; et al. Cervicofacial subcutaneous emphysema associated with dental laser treatment. Aust. Dent. J. 2013, 58, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Ong, W.C.; Lim, T.C.; Lim, J.; Sundar, G. Cervicofacial, Retropharyngeal and Mediastinal Emphysema: A Complication of Orbital Fracture. Asian J. Surg. 2005, 28, 305–308. [Google Scholar] [CrossRef] [Green Version]
- McKenzie, W.S.; Rosenberg, M. Iatrogenic subcutaneous emphysema of dental and surgical origin: A literature review. J. Oral Maxillofac. Surg. 2009, 67, 1265–1268. [Google Scholar] [CrossRef] [PubMed]
- Kuromatsu, Y.; Nakano, H.; Inoue, K.; Ogura, A.; Omori, M.; Nakajima, Y.; Ueno, T. A case of mediastinal emphysema caused by root canal treatment using Er: YAG laser. J. Oral Maxillofac. Surg. Med. Pathol. 2020, 32, 124–128. [Google Scholar] [CrossRef]
- La Monaca, G.; Pranno, N.; Annibali, S.; Vozza, I.; Cristalli, M.P. Subcutaneous Facial Emphysema Following Open-Flap Air-Powder Abrasive Debridement for Peri-Implantitis: A Case Report and an Overview. Int. J. Environ. Res. Public Health 2021, 18, 13286. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Ryu, J. Self-induced subcutaneous cervicofacial emphysema associated with a defect of external auditory. J. Oral Maxillofac. Surg. Med. Pathol 2020, 32, 454–457. [Google Scholar] [CrossRef]
- Lee, S.T.; Subu, M.G.; Kwon, T.G. Emphysema following air-powder abrasive treatment for peri-implantitis. Maxillofac. Plast. Reconstr. Surg. 2018, 40, 12. [Google Scholar] [CrossRef] [PubMed]
- Fasoulas, A.; Boutsioukis, C.; Lambrianidis, T. Subcutaneous emphysema in patients undergoing root canal treatment: A systematic review of the factors affecting its development and management. Int. Endod. J. 2019, 52, 1586–1604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, C.H.; Yoon, S.; Chung, S.W.; Kim, J.Y.; Park, K.H.; Huh, J.K. Subcutaneous emphysema related to dental procedures. J. Korean Assoc. Oral Maxillofac. Surg. 2018, 44, 212–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Facial | Neck | Mediastinum | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Orbital Soft Tissue | Buccal | Masticatory Muscle | Parotid Gland | Parapharyngeal | Posterior Pharyngeal | Sublingual | Submandibular | Anterior Cervical | Posterior Cervical | Posterior Pharyngeal | Carotid Artery Space | Anterior Mediastinum | ||
| Case1 | Day 1 | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● |
| Day 3 | ● | ● | ● | ● | ● | ● | ● | ● | ● | |||||
| Case 2 | Day 1 | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | ● | |
| Day 3 | ● | ● | ● | ● | ● | ● | ● | ● | ● | |||||
| Case 3 | Day 1 | ● | ● | ● | ● | ● | ● | ● | ● | ● | ||||
| Day 3 | ● | ● | ● | ● | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimizu, R.; Sukegawa, S.; Sukegawa, Y.; Hasegawa, K.; Ono, S.; Fujimura, A.; Yamamoto, I.; Ibaragi, S.; Sasaki, A.; Furuki, Y. Subcutaneous Emphysema Related to Dental Treatment: A Case Series. Healthcare 2022, 10, 290. https://doi.org/10.3390/healthcare10020290
Shimizu R, Sukegawa S, Sukegawa Y, Hasegawa K, Ono S, Fujimura A, Yamamoto I, Ibaragi S, Sasaki A, Furuki Y. Subcutaneous Emphysema Related to Dental Treatment: A Case Series. Healthcare. 2022; 10(2):290. https://doi.org/10.3390/healthcare10020290
Chicago/Turabian StyleShimizu, Rieko, Shintaro Sukegawa, Yuka Sukegawa, Kazuaki Hasegawa, Sawako Ono, Ai Fujimura, Izumi Yamamoto, Soichiro Ibaragi, Akira Sasaki, and Yoshihiko Furuki. 2022. "Subcutaneous Emphysema Related to Dental Treatment: A Case Series" Healthcare 10, no. 2: 290. https://doi.org/10.3390/healthcare10020290