
Educational Videos as an Adjunct Learning Tool in Pre-Clinical Operative Dentistry—A Randomized Control Trial

 , ,
, ,
Abstract
:1. Introduction
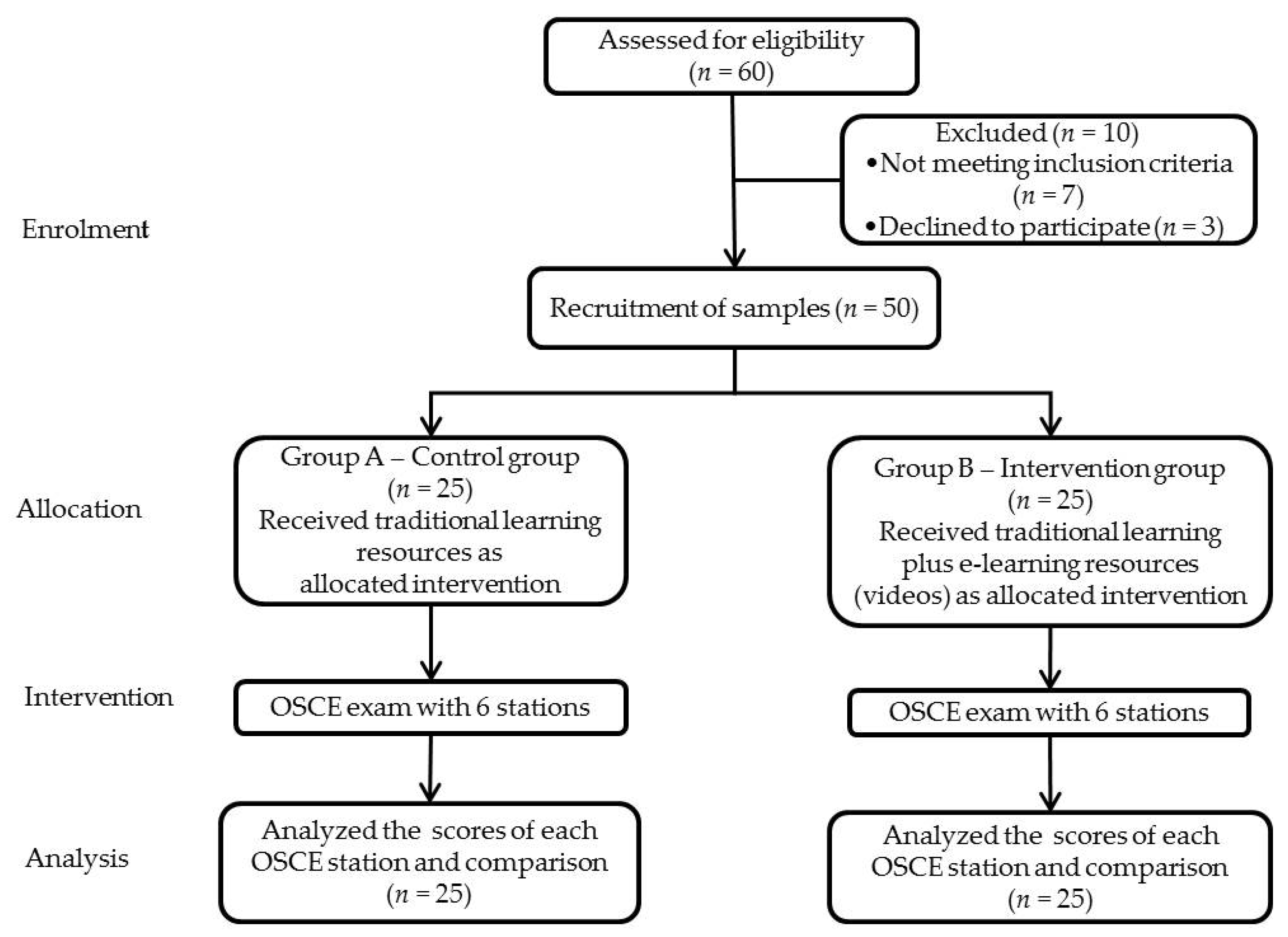
- Evaluating and comparing the effectiveness of e-learning resources as an additional teaching aid to traditional teaching methods in male and female students as well as based on the CGPA scores in a pre-clinical operative skill course.
- Correlating the effectiveness of e-learning resources with CGPA scores of dental students.
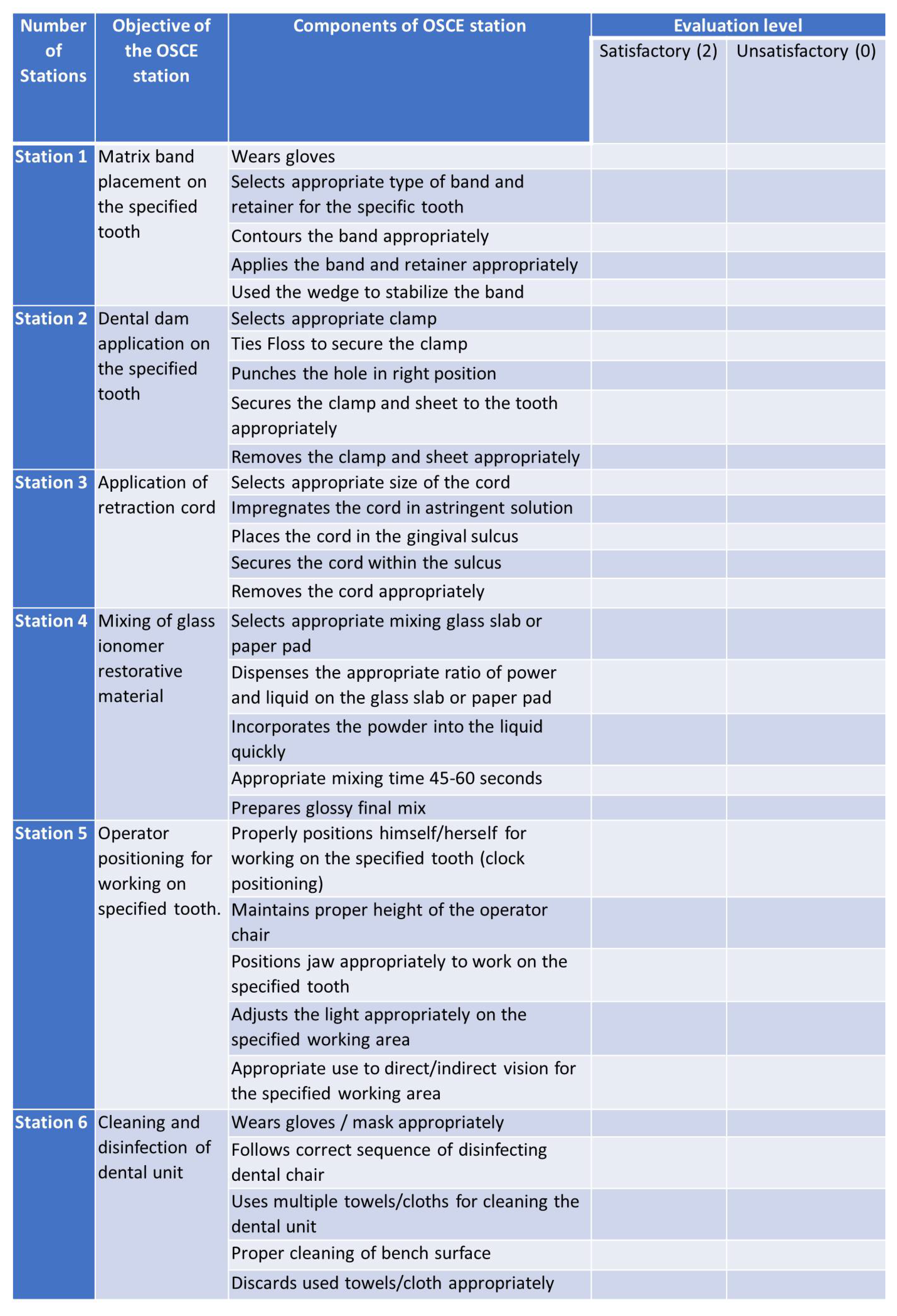
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ellaway, R.; Masters, K. AMEE Guide 32: E-Learning in medical education Part 1: Learning, teaching and assessment. Med. Teach. 2008, 30, 455–473. [Google Scholar] [CrossRef] [PubMed]
- Ganji, K.K. Evaluation of reliability in structured viva voce as a formative assessment of dental students. J. Dent. Educ. 2017, 81, 590–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Consorti, F. Didattica Professionalizzante nei Corsi di Laurea in Medicina; Edra: Milano, Italy, 2018. [Google Scholar]
- Turkyilmaz, I.; Hariri, N.H.; Jahangiri, L. Student’s perception of the impact of e-learning on dental education. J. Contemp. Dent. Pract. 2019, 20, 616–621. [Google Scholar] [CrossRef]
- Asiry, M.; Hashim, H. Tooth size ratios in Saudi subjects with Class II, Division 1 malocclusion. J. Int. Oral Health 2012, 4, 29. [Google Scholar]
- Al-Ansari, A.A.; El Tantawi, M.M. Predicting academic performance of dental students using perception of educational environment. J. Dent. Educ. 2015, 79, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Rudy, J.O.; Singleton, J.A.; Lewis, L.H.; Quick, R.N. Admissions criteria that influence dental hygiene students’ performance on board examinations. Am. Dent. Hyg. Assoc. 2017, 91, 24–29. [Google Scholar]
- Haq, I.; Higham, J.; Morris, R.; Dacre, J. Effect of ethnicity and gender on performance in undergraduate medical examinations. Med. Educ. 2005, 39, 1126–1128. [Google Scholar] [CrossRef] [PubMed]
- McDonough, C.; Horgan, A.; Codd, M.; Casey, P. Gender differences in the results of the final medical examination at University College Dublin. Med. Educ.-Oxf. 2000, 34, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Nuzhat, A.; Salem, R.O.; Al Hamdan, N.; Ashour, N. Gender differences in learning styles and academic performance of medical students in Saudi Arabia. Med. Teach. 2013, 35 (Suppl. S1), S78–S82. [Google Scholar] [CrossRef]
- Sawair, F.A.; Baqain, Z.H.; Al-Omari, I.K.; Wahab, F.K.; Rajab, L.D. Effect of gender on performance of undergraduate dental students at the University of Jordan, Amman. J. Dent. Educ. 2009, 73, 1313–1319. [Google Scholar] [CrossRef]
- Al-Elq, A.H. Simulation-based medical teaching and learning. J. Family Community Med. 2010, 17, 35. [Google Scholar] [CrossRef]
- Plakiotis, C. Objective structured clinical examination (OSCE) in psychiatry education: A review of its role in competency-based assessment. GeNeDis 2016 2017, 988, 159–180. [Google Scholar]
- Kemelova, G.; Tuleutaeva, S.; Aimbetova, D.; Garifullina, R. The objective structured clinical examination in dentistry: Strengths and weaknesses. Stomatologiia 2019, 98, 8–11. [Google Scholar] [CrossRef]
- Shigli, K.; Jyotsna, S.; Rajesh, G.; Wadgave, U.; Sankeshwari, B.; Nayak, S.S.; Vyas, R. Challenges in learning pre-clinical prosthodontics: A survey of perceptions of dental undergraduates and teaching faculty at an Indian dental school. J. Clin. Diagn. Res. JCDR 2017, 11, ZC01. [Google Scholar]
- Cervino, G.; Oteri, G. COVID-19 Pandemic and Telephone Triage before Attending Medical Office: Problem or Opportunity? Medicina 2020, 56, 250. [Google Scholar] [CrossRef]
- Bock, A.; Modabber, A.; Kniha, K.; Lemos, M.; Rafai, N.; Hölzle, F. Blended learning modules for lectures on oral and maxillofacial surgery. Br. J. Oral Maxillofac. Surg. 2018, 56, 956–961. [Google Scholar] [CrossRef]
- Qutieshat, A.S.; Abusamak, M.O.; Maragha, T.N. Impact of Blended Learning on Dental Students’ Performance and Satisfaction in Clinical Education. J. Dent. Educ. 2020, 84, 135–142. [Google Scholar] [CrossRef]
- Jang, H.W.; Kim, K.-J. Use of online clinical videos for clinical skills training for medical students: Benefits and challenges. BMC Med. Educ. 2014, 14, 56. [Google Scholar] [CrossRef] [Green Version]
- Reissmann, D.R.; Sierwald, I.; Berger, F.; Heydecke, G. A model of blended learning in a pre-clinical course in prosthetic dentistry. J. Dent. Educ. 2015, 79, 157–165. [Google Scholar] [CrossRef]
- Sladek, R.M.; Bond, M.J.; Frost, L.K.; Prior, K.N. Predicting success in medical school: A longitudinal study of common Australian student selection tools. BMC Med. Educ. 2016, 16, 187. [Google Scholar] [CrossRef] [Green Version]
- Albalawi, M. Does gender difference have an effect in the academic achievements of undergraduate students’ and later as interns? A single medical college experience, Taibah university, KSA. Allied J. Med. Res. 2019, 3, 20–25. [Google Scholar]



{kind=link}
{kind=link}
| Group | n | Mean | Std. Deviation | Std. Error Mean | F Value | p Value | |
|---|---|---|---|---|---|---|---|
| Station#1 | A | 25 | 6.480 | 1.045 | 0.209 | 0.763 | 0.067 * |
| B | 25 | 7.000 | 0.912 | 0.182 | |||
| Station#2 | A | 25 | 6.200 | 0.500 | 0.100 | 3.903 | 0.000 * |
| B | 25 | 7.000 | 0.866 | 0.173 | |||
| Station#3 | A | 25 | 6.240 | 0.925 | 0.185 | 0.480 | 0.002 * |
| B | 25 | 7.040 | 0.840 | 0.168 | |||
| Station#4 | A | 25 | 6.480 | 0.822 | 0.164 | 0.071 | 0.025 * |
| B | 25 | 7.040 | 0.888 | 0.177 | |||
| Station#5 | A | 25 | 6.280 | 0.791 | 0.158 | 1.186 | 0.000 * |
| B | 25 | 7.280 | 0.936 | 0.187 | |||
| Station#6 | A | 25 | 6.320 | 0.627 | 0.125 | 2.790 | 0.002 * |
| B | 25 | 7.080 | 0.996 | 0.199 | |||
| CGPA | A | 25 | 3.926 | 0.684 | 0.136 | 28.98 | 0.245 |
| B | 25 | 3.834 | 0.255 | 0.051 |
| Gender | n | Mean | Std. Deviation | Std. Error Mean | F Value | p Value | |
|---|---|---|---|---|---|---|---|
| Station#1 | Male | 33 | 6.424 | 0.902 | 0.157 | 0.763 | 0.001 * |
| Female | 17 | 7.352 | 0.931 | 0.225 | |||
| Station#2 | Male | 33 | 6.484 | 0.833 | 0.145 | 3.903 | 0.163 |
| Female | 17 | 6.823 | 0.727 | 0.176 | |||
| Station#3 | Male | 33 | 6.424 | 0.902 | 0.157 | 0.480 | 0.026 * |
| Female | 17 | 7.058 | 0.966 | 0.234 | |||
| Station#4 | Male | 33 | 6.666 | 0.924 | 0.160 | 0.071 | 0.308 |
| Female | 17 | 6.941 | 0.826 | 0.200 | |||
| Station#5 | Male | 33 | 6.515 | 0.972 | 0.169 | 1.186 | 0.007 * |
| Female | 17 | 7.294 | 0.848 | 0.205 | |||
| Station#6 | Male | 33 | 6.697 | 1.045 | 0.181 | 2.790 | 0.974 |
| Female | 17 | 6.705 | 0.587 | 0.142 |
| OSCE | CGPA Score | n | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | p Value | |
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||||
| Station#1 | Low | 5 | 5.400 | 0.547 | 0.244 | 4.719 | 6.080 | 0.000 |
| Average | 11 | 6.272 | 0.646 | 0.194 | 5.838 | 6.707 | ||
| High | 34 | 7.088 | 0.933 | 0.160 | 6.762 | 7.413 | ||
| Station#2 | Low | 5 | 5.800 | 0.447 | 0.200 | 5.244 | 6.355 | 0.002 |
| Average | 11 | 6.181 | 0.404 | 0.121 | 5.910 | 6.453 | ||
| High | 34 | 6.852 | 0.821 | 0.140 | 6.566 | 7.139 | ||
| Station#3 | Low | 5 | 5.200 | 0.447 | 0.200 | 4.644 | 5.755 | 0.000 |
| Average | 11 | 6.181 | 0.603 | 0.181 | 5.776 | 6.586 | ||
| High | 34 | 7.000 | 0.852 | 0.146 | 6.702 | 7.297 | ||
| Station#4 | Low | 5 | 5.800 | 1.095 | 0.489 | 4.439 | 7.160 | 0.006 |
| Average | 11 | 6.454 | 0.687 | 0.207 | 5.992 | 6.916 | ||
| High | 34 | 7.0000 | 0.816 | 0.140 | 6.715 | 7.284 | ||
| Station#5 | Low | 5 | 5.6000 | 0.547 | 0.244 | 4.919 | 6.280 | 0.000 |
| Average | 11 | 6.272 | 0.646 | 0.194 | 5.838 | 6.707 | ||
| High | 34 | 7.117 | 0.945 | 0.162 | 6.787 | 7.447 | ||
| Station#6 | Low | 5 | 5.800 | 0.447 | 0.200 | 5.244 | 6.355 | 0.004 |
| Average | 11 | 6.272 | 0.467 | 0.140 | 5.958 | 6.586 | ||
| High | 34 | 6.970 | 0.936 | 0.160 | 6.643 | 7.297 | ||
| Station#1 | Station#2 | Station#3 | Station#4 | Station#5 | Station#6 | CGPA | |
|---|---|---|---|---|---|---|---|
| Station#1 | 1 | ||||||
| Station#2 | 0.647 ** | 1 | |||||
| Station#3 | 0.722 ** | 0.493 ** | 1 | ||||
| Station#4 | 0.542 ** | 0.401 ** | 0.466 ** | 1 | |||
| Station#5 | 0.655 ** | 0.700 ** | 0.532 ** | 0.490 ** | 1 | ||
| Station#6 | 0.605 ** | 0.778 ** | 0.573 ** | 0.362 ** | 0.534 ** | 1 | |
| CGPA | 0.563 ** | 0.525 ** | 0.701 ** | 0.509 ** | 0.620 ** | 0.492 ** | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khattak, O.; Ganji, K.K.; Iqbal, A.; Alonazi, M.; Algarni, H.; Alsharari, T. Educational Videos as an Adjunct Learning Tool in Pre-Clinical Operative Dentistry—A Randomized Control Trial. Healthcare 2022, 10, 178. https://doi.org/10.3390/healthcare10020178
Khattak O, Ganji KK, Iqbal A, Alonazi M, Algarni H, Alsharari T. Educational Videos as an Adjunct Learning Tool in Pre-Clinical Operative Dentistry—A Randomized Control Trial. Healthcare. 2022; 10(2):178. https://doi.org/10.3390/healthcare10020178
Chicago/Turabian StyleKhattak, Osama, Kiran Kumar Ganji, Azhar Iqbal, Meshal Alonazi, Hmoud Algarni, and Thani Alsharari. 2022. "Educational Videos as an Adjunct Learning Tool in Pre-Clinical Operative Dentistry—A Randomized Control Trial" Healthcare 10, no. 2: 178. https://doi.org/10.3390/healthcare10020178