
Backward Walking Styles and Impact on Spatiotemporal Gait Characteristics

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Conditions of Walking
2.3. Experimental Procedure
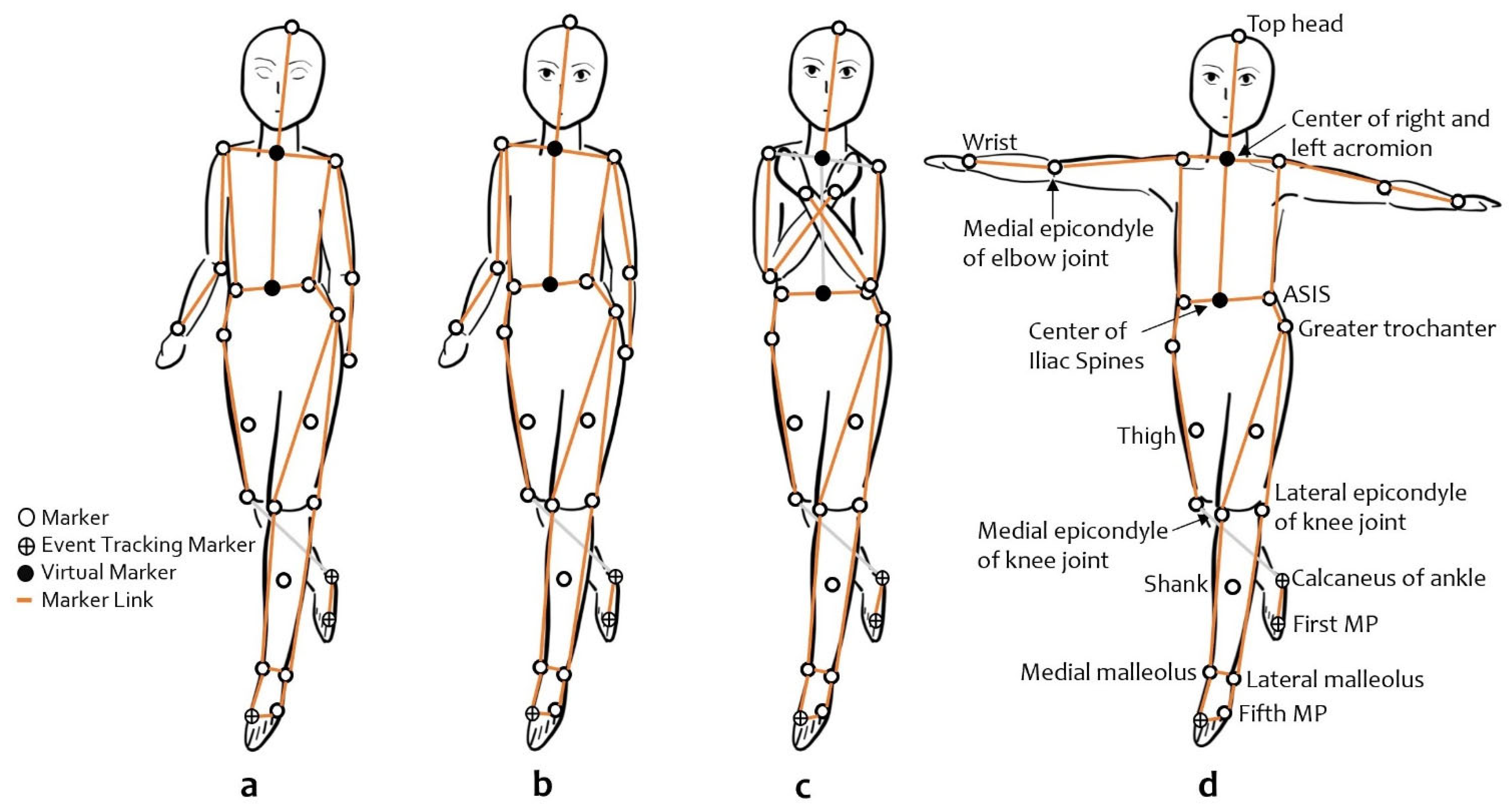
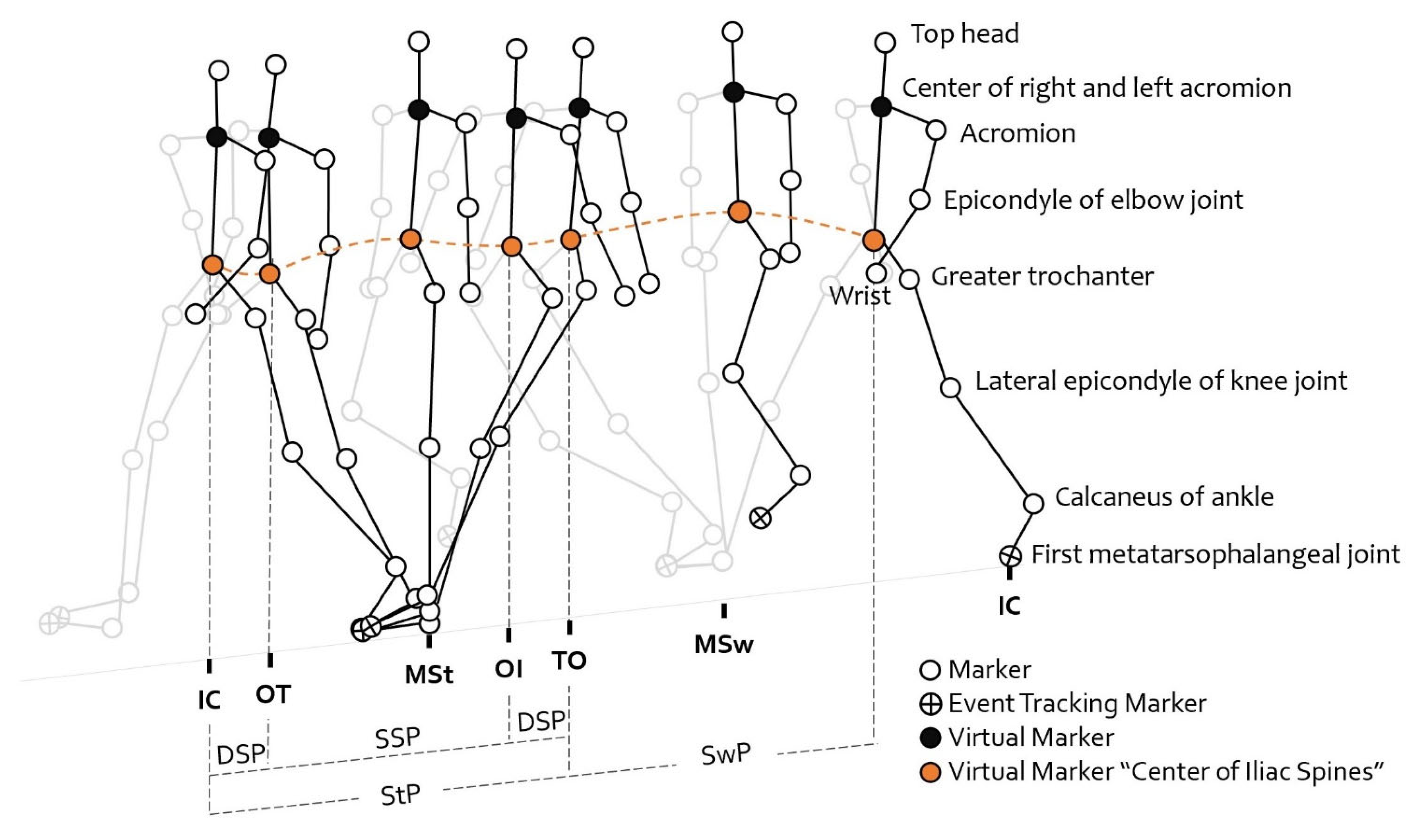
2.4. Measurement
2.5. Statistical Analysis
3. Results
3.1. The Effect of Walking Direction and Speed
3.2. The Effect of Arm Position
3.3. The Effect of Visual Feedback on Backward Walking
4. Discussion
4.1. The Effect of Direction and Speed on Backward and Forward Walking
4.2. The Effect of Arm Position on Backward Walking
4.3. The Effect of Visual Feedback on Backward Walking
4.4. Implications and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization Falls. Available online: https://www.who.int/news-room/fact-sheets/detail/falls (accessed on 11 May 2022).
- Brians, L.K.; Alexander, K.C.; Grota, P.A.; Chen, R.W.; Dumas, V. The Development of the RISK Tool for Fall Prevention. Rehabil. Nurs. J. 1991, 16, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Robinovitch, S.N.; Feldman, F.; Yang, Y.; Leung, P.; Health, F.; Sims-Gould, J.; Robinovitch, S.; Robinovitch, S.; Feldman, F.; Yang, Y.; et al. Video Capture of the Circumstances of Falls in Elderly People Residing in Long-Term Care: An Observational Study. Lancet 2013, 381, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Levine, D.; Richards, J.; Whittle, M. Whittle’s Gait Analysis, 5th ed.; Elsevier Health Sciences: Amsterdam, The Netherlands, 2012; ISBN 9780702042652. [Google Scholar]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age- and Gender-Related Test Performance in Community-Dwelling Elderly People: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and Gait Speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panella, L.; Tinelli, C.; Buizza, A.; Lombardi, R.; Gandolfi, R. Towards Objective Evaluation of Balance in the Elderly: Validity and Reliability of a Measurement Instrument Applied to the Tinetti Test. Int. J. Rehabil. Res. 2008, 31, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Pardasaney, P.K.; Latham, N.K.; Jette, A.M.; Wagenaar, R.C.; Ni, P.; Slavin, M.D.; Bean, J.F. Sensitivity to Change and Responsiveness of Four Balance Measures for Community-Dwelling Older Adults. Phys. Ther. 2012, 92, 388–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, G.W.; Abreu, E.L.; Cheng, A.-L.; Chertoff, K.K.; Brotto, L.; Kelly, P.J.; Brotto, M. A Multimodal Assessment of Balance in Elderly and Young Adults. Oncotarget 2016, 7, 13297–13306. [Google Scholar] [CrossRef] [Green Version]
- Carter, V.; Jain, T.; James, J.; Cornwall, M.; Aldrich, A.; de Heer, H.D. The 3-m Backwards Walk and Retrospective Falls: Diagnostic Accuracy of a Novel Clinical Measure. J. Geriatr. Phys. Ther. 2019, 42, 249–255. [Google Scholar] [CrossRef]
- Fritz, N.E.; Worstell, A.M.; Kloos, A.D.; Siles, A.B.; White, S.E.; Kegelmeyer, D.A. Backward Walking Measures Are Sensitive to Age-Related Changes in Mobility and Balance. Gait Posture 2013, 37, 593–597. [Google Scholar] [CrossRef]
- Taulbee, L.; Yada, T.; Graham, L.; O’Halloran, A.; Saracino, D.; Freund, J.; Vallabhajosula, S.; Balasubramanian, C.K. Use of Backward Walking Speed to Screen Dynamic Balance and Mobility Deficits in Older Adults Living Independently in the Community. J. Geriatr. Phys. Ther. 2021, 44, 189–197. [Google Scholar] [CrossRef]
- Kurz, M.J.; Wilson, T.W.; Arpin, D.J. Stride-Time Variability and Sensorimotor Cortical Activation during Walking. Neuroimage 2012, 59, 1602–1607. [Google Scholar] [CrossRef]
- Chang, K.-W.; Lin, C.-M.; Yen, C.-W.; Yang, C.-C.; Tanaka, T.; Guo, L.-Y. The Effect of Walking Backward on a Treadmill on Balance, Speed of Walking and Cardiopulmonary Fitness for Patients with Chronic Stroke: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 2376. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Yuan, W.; An, R. Effectiveness of Backward Walking Training on Spatial-Temporal Gait Characteristics: A Systematic Review and Meta-Analysis. Hum. Mov. Sci. 2018, 60, 57–71. [Google Scholar] [CrossRef]
- Lee, M.; Kim, J.; Son, J.; Kim, Y. Kinematic and Kinetic Analysis during Forward and Backward Walking. Gait Posture 2013, 38, 674–678. [Google Scholar] [CrossRef]
- Laufer, Y. Effect of Age on Characteristics of Forward and Backward Gait at Preferred and Accelerated Walking Speed. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2005, 60, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.; Shema, S.; Maidan, I.; Hausdorff, J.M. Chapter 7—Gait. In Handbook of Clinical Neurology; Day, B.L., Lord, S.R., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 159, pp. 119–134. ISBN 0072-9752. [Google Scholar]
- Weerdesteyn, V.; Hollands, K.L.; Hollands, M.A. Chapter 8—Gait Adaptability. In Handbook of Clinical Neurology; Day, B.L., Lord, S.R., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 159, pp. 135–146. ISBN 0072-9752. [Google Scholar]
- Bruijn, S.M.; Meijer, O.G.; van Dieën, J.H.; Kingma, I.; Lamoth, C.J.C. Coordination of Leg Swing, Thorax Rotations, and Pelvis Rotations during Gait: The Organisation of Total Body Angular Momentum. Gait Posture 2008, 27, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Bovonsunthonchai, S.; Hiengkaew, V.; Vachalathiti, R.; Vongsirinavarat, M.; Tretriluxana, J. Effect of Speed on the Upper and Contralateral Lower Limb Coordination during Gait in Individuals with Stroke. Kaohsiung J. Med. Sci. 2012, 28, 667–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ehara, Y.; Yamamoto, S. Introduction to Body-Dynamics—Analysis of Standing up Movement; Ishiyaku Publishers: Tokyo, Japan, 2001. [Google Scholar]
- Orendurff, M.; Segal, A.; Klute, G.; Berge, J.; Rohr, E.; Kadel, N. The Effect of Walking Speed on Center of Mass Displacement. J. Rehabil. Res. Dev. 2004, 41, 829–834. [Google Scholar] [CrossRef] [Green Version]
- Lu, H.-L.; Kuo, M.-Y.; Chang, C.-F.; Lu, T.-W.; Hong, S.-W. Effects of Gait Speed on the Body’s Center of Mass Motion Relative to the Center of Pressure during over-Ground Walking. Hum. Mov. Sci. 2017, 54, 354–362. [Google Scholar] [CrossRef]
- Tesio, L.; Rota, V. The Motion of Body Center of Mass During Walking: A Review Oriented to Clinical Applications. Front. Neurol. 2019, 10, 999. [Google Scholar] [CrossRef] [Green Version]
- Grasso, R.; Bianchi, L.; Lacquaniti, F. Motor Patterns for Human Gait: Backward Versus Forward Locomotion. J. Neurophysiol. 1998, 80, 1868–1885. [Google Scholar] [CrossRef]
- Laufer, Y. Age- and Gender-Related Changes in the Temporal-Spatial Characteristics of Forwards and Backwards Gaits. Physiother. Res. Int. 2003, 8, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Bogen, B.; Moe-Nilssen, R.; Ranhoff, A.H.; Aaslund, M.K. The Walk Ratio: Investigation of Invariance across Walking Conditions and Gender in Community-Dwelling Older People. Gait Posture 2018, 61, 479–482. [Google Scholar] [CrossRef] [PubMed]
- Thorstensson, A. How Is the Normal Locomotor Program Modified to Produce Backward Walking? Exp. Brain Res. 1986, 61, 664–668. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.W.; Mille, M.-L. Chapter 5—Balance Perturbations. In Handbook of Clinical Neurology; Day, B.L., Lord, S.R., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 159, pp. 85–105. ISBN 0072-9752. [Google Scholar]
- Rothwell, J. Control of Human Voluntary Movement, 2nd ed.; Chapman & Hall: London, UK, 1994. [Google Scholar]
- Rose, J.; Gamble, J.G. Human Walking, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, Pennsylvania, 2006; ISBN 1-4698-7998-0. [Google Scholar]
- Koo, H.-M.; Lee, S.-Y. Gait Analysis on the Condition of Arm Swing in Healthy Young Adults. Phys. Ther. Rehabil. Sci. 2016, 5, 149–154. [Google Scholar] [CrossRef] [Green Version]
- Ford, M.P.; Wagenaar, R.C.; Newell, K.M. Arm Constraint and Walking in Healthy Adults. Gait Posture 2007, 26, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Punt, M.; Bruijn, S.M.; Wittink, H.; van Dieën, J.H. Effect of Arm Swing Strategy on Local Dynamic Stability of Human Gait. Gait Posture 2015, 41, 504–509. [Google Scholar] [CrossRef] [Green Version]
- Bruijn, S.M.; Meijer, O.G.; Beek, P.J.; van Dieën, J.H. The Effects of Arm Swing on Human Gait Stability. J. Exp. Biol. 2010, 213, 3945–3952. [Google Scholar] [CrossRef] [Green Version]
- Eke-Okoro, S.T.; Gregoric, M.; Larsson, L.E. Alterations in Gait Resulting from Deliberate Changes of Arm-Swing Amplitude and Phase. Clin. Biomech. 1997, 12, 516–521. [Google Scholar] [CrossRef]
- Meyns, P.; Molenaers, G.; Desloovere, K.; Duysens, J. Interlimb Coordination during Forward Walking Is Largely Preserved in Backward Walking in Children with Cerebral Palsy. Clin. Neurophysiol. 2014, 125, 552–561. [Google Scholar] [CrossRef]
- Sanders, O.P.; Savin, D.N.; Creath, R.A.; Rogers, M.W. Protective Balance and Startle Responses to Sudden Freefall in Standing Humans. Neurosci. Lett. 2015, 586, 8–12. [Google Scholar] [CrossRef]
- McIlroy, W.E.; Maki, B.E. Early Activation of Arm Muscles Follows External Perturbation of Upright Stance. Neurosci. Lett. 1995, 184, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Udochkina, L.A.; Vorontsova, O.I.; Mazin, I.G.; Goncharova, L.A.; Akhmineeva, A.K. Kinematic Parameters of Movement at the Shoulder Joint in Normal Gait in Humans. Neurosci. Behav. Physiol. 2018, 48, 903–907. [Google Scholar] [CrossRef]
- Ortega, J.D.; Fehlman, L.A.; Farley, C.T. Effects of Aging and Arm Swing on the Metabolic Cost of Stability in Human Walking. J. Biomech. 2008, 41, 3303–3308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauby, C.E.; Kuo, A.D. Active Control of Lateral Balance in Human Walking. J. Biomech. 2000, 33, 1433–1440. [Google Scholar] [CrossRef]
- Wuehr, M.; Schniepp, R.; Pradhan, C.; Ilmberger, J.; Strupp, M.; Brandt, T.; Jahn, K. Differential Effects of Absent Visual Feedback Control on Gait Variability during Different Locomotion Speeds. Exp. Brain Res. 2013, 224, 287–294. [Google Scholar] [CrossRef]
- Dakin, C.J.; Rosenberg, A. Chapter 3—Gravity Estimation and Verticality Perception. In Handbook of Clinical Neurology; Day, B.L., Lord, S.R., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 159, pp. 43–59. ISBN 0072-9752. [Google Scholar]
- Goodale, M.A. Visuomotor Modules in the Vertebrate Brain. Can. J. Physiol. Pharmacol. 1996, 74, 390–400. [Google Scholar] [CrossRef]
- Reynolds, R.; Day, B. Visual Guidance of the Human Foot during a Step. J. Physiol. 2006, 569, 677–684. [Google Scholar] [CrossRef]
- Forbes, P.A.; Chen, A.; Blouin, J.-S. Chapter 4—Sensorimotor Control of Standing Balance. In Handbook of Clinical Neurology; Day, B.L., Lord, S.R., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 159, pp. 61–83. ISBN 0072-9752. [Google Scholar]
- Nashner, L.; Berthoz, A. Visual Contribution to Rapid Motor Responses during Postural Control. Brain Res. 1978, 150, 403–407. [Google Scholar] [CrossRef]
- Frost, R.; Skidmore, J.; Santello, M.; Artemiadis, P. Sensorimotor Control of Gait: A Novel Approach for the Study of the Interplay of Visual and Proprioceptive Feedback. Front. Hum. Neurosci. 2015, 9, 14. [Google Scholar] [CrossRef]
- Peterka, R.J. Chapter 2—Sensory Integration for Human Balance Control. In Handbook of Clinical Neurology; Day, B.L., Lord, S.R., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 159, pp. 27–42. ISBN 0072-9752. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics Data | Male (n = 11) | Female (n = 12) |
|---|---|---|
| Age (years) | 23.4 ± 1.3 | 22.8 ± 1.8 |
| Mass (kg) | 62.8 ± 6.9 | 54.8 ± 10.5 |
| Height (m) | 1.75 ± 0.1 | 1.62 ± 0.1 |
| BMI (kg/m2) | 20.4 ± 2.2 | 20.9 ± 3.5 |
| Normal Speed | Fast Speed | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Parameter | NFW | NBW | FFW | FBW | Speed | Direction | Interaction |
| Spatiotemporal parameter measures | |||||||
| Velocity (m/s) | 1.24 ± 0.18 | 0.99 ± 0.20 | 1.79 ± 0.26 | 1.45 ± 0.26 | <0.001 ⁑ | <0.001 ⁑ | 0.052 |
| Cadence (steps/min) | 113.7 ± 9.8 | 106.9 ± 15.2 | 138.9 ± 12.5 | 138.7 ± 18.5 | <0.001 ⁑ | 0.091 | 0.023 * |
| Step length (mm) | 651.9 ± 66.0 | 552.5 ± 68.9 | 775.4 ± 96.5 | 631.4 ± 89.6 | <0.001 ⁑ | <0.001 ⁑ | 0.002 * |
| Step width (mm) | 171.5 ± 23.9 | 200.4 ± 35.5 | 177.8 ± 26.9 | 217.4 ± 33.5 | 0.001 * | <0.001 ⁑ | 0.059 |
| Walk ratio (mm/steps/min) | 5.77 ± 6.7 | 5.26 ± 8.9 | 5.63 ± 8.9 | 4.64 ± 9.3 | 0.009 * | <0.001 ⁑ | 0.091 |
| Phases of gait cycle measures | |||||||
| Stance phase (s) | 0.62 ± 0.06 | 0.68 ± 0.12 | 0.48 ± 0.05 | 0.49 ± 0.7 | <0.001 ⁑ | 0.012 * | 0.019 * |
| Swing phase (s) | 0.44 ± 0.04 | 0.47 ± 0.06 | 0.40 ± 0.03 | 0.40 ± 0.05 | <0.001 ⁑ | 0.042 * | 0.008 * |
| DSP phase (s) | 0.09 ± 0.02 | 0.11 ± 0.03 | 0.04 ± 0.02 | 0.05 ± 0.02 | <0.001 ⁑ | 0.021 * | 0.140 |
| Stance phase (%) | 58.6 ± 1.4 | 59.3 ± 1.8 | 54.5 ±1.6 | 54.7 ± 2.2 | <0.001 ⁑ | 0.173 | 0.392 |
| Swing phase (%) | 41.4 ± 1.4 | 40.7 ± 1.8 | 45.5 ± 1.6 | 45.3 ± 2.2 | <0.001 ⁑ | 0.173 | 0.392 |
| DSP (%) | 8.5 ± 1.3 | 9.0 ± 1.8 | 4.5 ± 1.4 | 4.8 ± 2.1 | <0.001 ⁑ | 0.199 | 0.690 |
| COM displacement measures | |||||||
| ML COM (mm) | 34.2 ± 10.1 | 42.6 ± 16.6 | 35.0 ± 10.0 | 44.1 ± 18.2 | 0.633 | 0.009 * | 0.879 |
| VT COM (mm) | 32.1 ± 7.1 | 39.3 ± 10.8 | 38.8 ± 13.4 | 44.1 ±14.1 | <0.001 ⁑ | 0.003 * | 0.422 |
| Parameters | Backward Walking in Different Arm Positions | ||||
|---|---|---|---|---|---|
| NBW | CrossBW | AbBW | F | p-Value | |
| Spatiotemporal parameter measures | |||||
| Velocity (m/s) | 0.99 ± 0.2 | 0.94 ± 0.2 | 0.99 ± 0.2 | 0.556 | 0.576 |
| Cadence (steps/min) | 106.9 ± 15.2 | 105.8 ± 14.7 | 105.9 ± 16.4 | 0.034 | 0.967 |
| Step length (mm) | 552.5 ± 68.9 | 529.5 ± 80.5 | 564.3 ± 70.7 | 1.331 | 0.271 |
| Step width (mm) | 200.4 ± 35.5 | 207.2 ± 40.0 | 199.2 ± 35.5 | 0.311 | 0.733 |
| Walk ratio (mm/steps/min) | 5.26 ± 0.9 | 5.07 ± 0.9 | 5.43 ± 1.0 | 0.877 | 0.421 |
| Phases of gait cycle measures | |||||
| Stance phase (s) | 0.68 ± 0.12 | 0.69 ±0.12 | 0.68 ± 0.13 | 0.103 | 0.902 |
| Swing phase (s) | 0.47 ± 0.06 | 0.46 ± 0.54 | 0.48 ± 0.07 | 0.678 | 0.511 |
| DSP phase (s) | 0.11 ± 0.03 | 0.11 ± 0.03 | 0.10 ± 0.04 | 0.733 | 0.484 |
| Stance phase (%) | 59.3 ± 1.8 | 60.0 ± 2.1 | 58.5 ± 2.1 | 3.382 | 0.040 * |
| Swing phase (%) | 40.7 ± 1.8 | 40.0 ± 2.1 | 41.5 ± 2.1 | 3.381 | 0.040 * |
| DSP (%) | 9.0 ± 1.8 | 9.8 ± 1.8 | 8.2 ± 2.0 | 3.974 | 0.023 * |
| COM displacement measures | |||||
| ML COM (mm) | 42.6 ± 16.6 | 48.3 ± 20.0 | 47.8 ± 16.2 | 0.484 | 0.484 |
| VT COM (mm) | 39.3 ± 10.8 | 38.0 ± 11.6 | 36.8 ± 10.0 | 0.751 | 0.751 |
| BW in Different Visual Feedback Conditions | |||
|---|---|---|---|
| Parameters | NBW | ClosBW | p-Value |
| Spatiotemporal parameter measures | |||
| Velocity (m/s) | 0.99 ± 0.20 | 0.96 ± 0.2 | 0.626 |
| Cadence (steps/min) | 106.9 ± 15.2 | 108.1 ± 14.7 | 0.782 |
| Step length (mm) | 552.5 ± 68.9 | 527.2 ± 90.1 | 0.291 |
| Step width (mm) | 200.4 ± 35.5 | 211.3 ± 35.6 | 0.306 |
| Walk ratio (mm/steps/min) | 5.26 ± 8.9 | 4.93 ± 0.9 | 0.218 |
| Phases of gait cycle measures | |||
| Stance phase (s) | 0.68 ± 0.12 | 0.67 ±0.13 | 0.814 |
| Swing phase (s) | 0.47 ± 0.06 | 0.46 ± 0.05 | 0.573 |
| DSP phase (s) | 0.11 ± 0.03 | 0.10 ± 0.04 | 0.874 |
| Stance phase (%) | 59.3 ± 1.8 | 59.0 ± 2.0 | 0.573 |
| Swing phase (%) | 40.7 ± 1.8 | 41.0 ± 2.0 | 0.782 |
| DSP (%) | 9.0 ± 1.8 | 8.8 ± 2.0 | 0.703 |
| COM displacement measures | |||
| ML COM (mm) | 42.6 ± 16.6 | 84.2 ± 25.2 | <0.001 ⁑ |
| VT COM (mm) | 39.3 ± 10.8 | 36.6 ± 8.9 | 0.359 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luecha, T.; Takesue, S.; Yeoh, W.L.; Loh, P.Y.; Muraki, S. Backward Walking Styles and Impact on Spatiotemporal Gait Characteristics. Healthcare 2022, 10, 2487. https://doi.org/10.3390/healthcare10122487
Luecha T, Takesue S, Yeoh WL, Loh PY, Muraki S. Backward Walking Styles and Impact on Spatiotemporal Gait Characteristics. Healthcare. 2022; 10(12):2487. https://doi.org/10.3390/healthcare10122487
Chicago/Turabian StyleLuecha, Teerapapa, Shin Takesue, Wen Liang Yeoh, Ping Yeap Loh, and Satoshi Muraki. 2022. "Backward Walking Styles and Impact on Spatiotemporal Gait Characteristics" Healthcare 10, no. 12: 2487. https://doi.org/10.3390/healthcare10122487