
Fractional CO2 Laser versus Fractional Radiofrequency for Skin Striae Treatment: Study Protocol for a Randomized Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
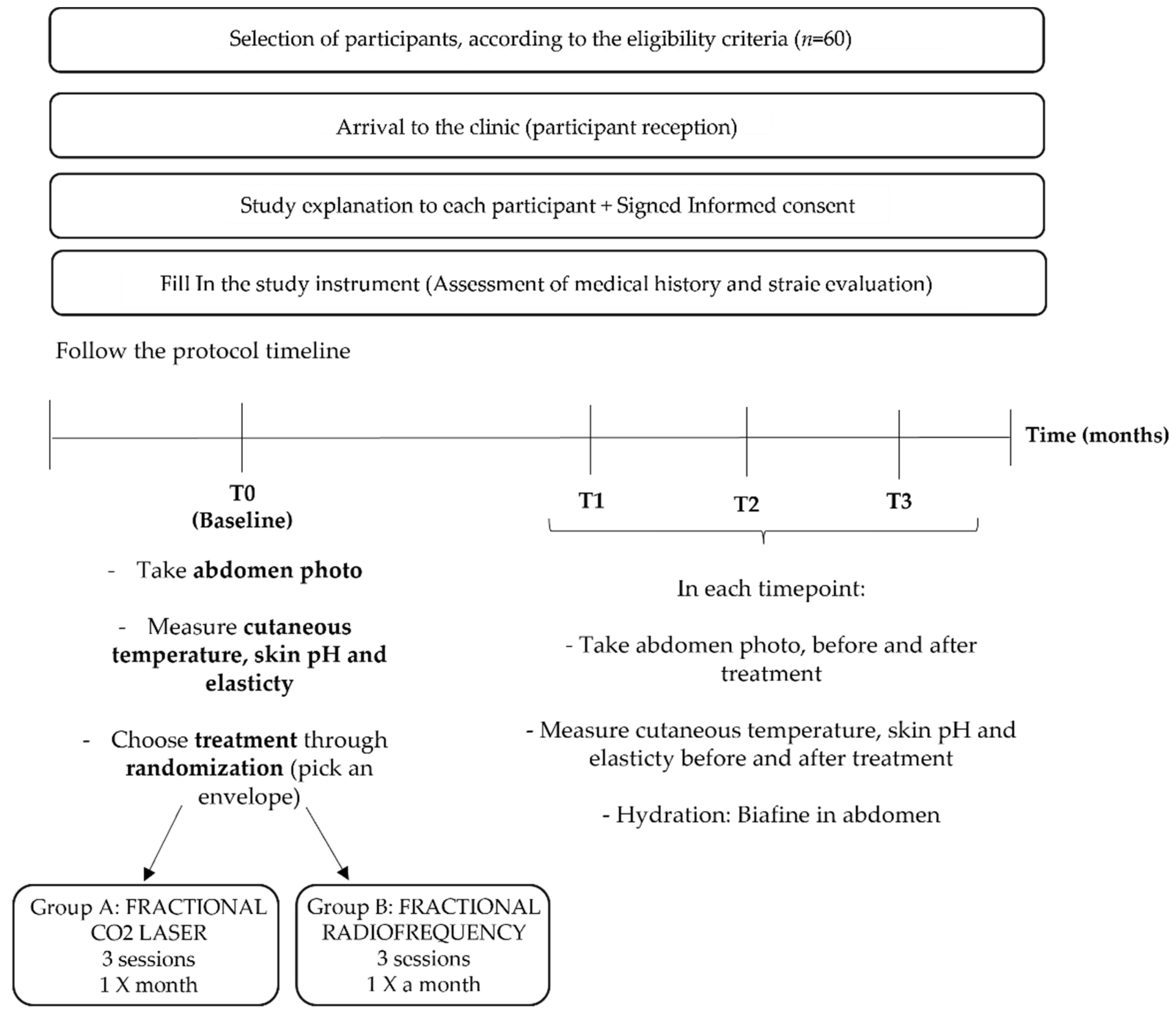
2.1. Study Design
2.2. Recruitment and Participants
2.3. Eligibility Criteria
2.4. Allocation
2.5. Intervention
3. Results
3.1. Primary Outcome
3.2. Secondary Outcome
3.3. Participant Timeline
3.4. Adverse Events
3.5. Data Collection and Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rogalski, C.; Haustein, U.-F.; Glander, H.-J.; Paasch, U. Extensive Striae Distensae as a Result of Topica Corticosteroid Therapy in Psoriasis Vulgaris. Acta Dermato Venereol. 2002, 83, 54–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kravvas, G.; Veitch, D.; Al-Niaimi, F. The Use of Energy Devices in the Treatment of Striae: A Systematic Literature Review. J. Dermatol. Treat. 2019, 3, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Dover, J.S.; Rothaus, K.; Gold, M.H. Evaluation of Safety and Patient Subjective Efficacy of Using Radiofrequency and Pulsed Magnetic Fields for the Treatment of Striae (Stretch Marks). J.Clin. Aesthet. Dermatol. 2014, 7, 30–33. [Google Scholar] [PubMed]
- Elsaie, M.L.; Baumann, L.S.; Elsaaiee, L.T. Striae distensae (stretch marks) and different modalities of therapy: An update. Dermatol. Surg. 2009, 35, 563–573. [Google Scholar] [CrossRef]
- Viviano, M.T.; Provini, A.; Mazzanti, C.; Nisticò, S.P.; Patruno, C.; Cannarozzo, G.; Bennardo, S.; Fusco, I.; Bennardo, L. Clinical Evaluation on the Performance and Safety of a Non-Ablative Fractional 1340 nm Laser for the Treatment of Stretch Marks in Adolescents and Young Adults: A Case Series. Bioengineering 2022, 9, 139. [Google Scholar] [CrossRef]
- Oakley, A.M.; Patel, B.C. Stretch Marks; StatPearls: Treasure Island, FL, USA, 2022; pp. 1–9. [Google Scholar]
- Piérard-Franchimont, C.; Hermanns, J.F.; Hermanns-Lê, T.; Piérard, G.E. Striae distensae in darker skin types: The influence of melanocyte mechanobiology. J. Cosmet. Dermatol. 2005, 4, 174–178. [Google Scholar] [CrossRef]
- de Angelis, F.; Kolesnikova, L.; Renato, F.; Liguori, G. Fractional nonablative 1540-nm laser treatment of striae distensae in Fitzpatrick skin types II to IV: Clinical and histological results. Aesthet. Surg. J. 2011, 31, 411–419. [Google Scholar] [CrossRef] [Green Version]
- Tabaie, S.M.; Nasr, E.; Naderi, M.S.; Rezvan, M. Treatment of striae distensae using fractional ablative CO2 laser in skin types II-IV: A retrospective case series study. J. Cosmet. Laser. Ther. 2018, 20, 330–334. [Google Scholar] [CrossRef]
- Wollina, U.; Goldman, A. Management of stretch marks (with a focus on striae rubrae). J. Cutan. Aesthet. Surg. 2017, 10, 124–129. [Google Scholar] [CrossRef]
- Shin, J.U.; Roh, M.R.; Rah, D.K.; Ae, N.K.; Suh, H.; Chung, K.Y. The effect of succinylated atelocollagen and ablative fractional resurfacing laser on striae distensae. J. Dermatolog. Treat. 2011, 22, 113–121. [Google Scholar] [CrossRef]
- Sardana, K. Lasers for Treating Striae: An Emergent Need for Better Evidence. Indian J. Dermatol. Venereol. Leprol. 2014, 80, 392–394. [Google Scholar] [CrossRef] [PubMed]
- Forbat, E.; Al-Niaimi, F. Treatment of Striae Distensae: An Evidence-Based Approach. J. Cosmet. Laser Ther. 2019, 21, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Xu, L.; Wu, T.; Mu, Y.-Z. New Progress in Therapeutic Modalities of Striae Distensae. Clin. Cosmet. Investig. Dermatol. 2022, 15, 2101–2115. [Google Scholar] [CrossRef] [PubMed]
- Sobhi, R.M.; Mohamed, I.S.; el Sharkawy, D.A.; el Wahab, M.A.E.F.A. Comparative Study between the Efficacy of Fractional Micro-Needle Radiofrequency and Fractional CO2 Laser in the Treatment of Striae Distensae. Lasers Med. Sci. 2019, 34, 1295–1304. [Google Scholar] [CrossRef]
- Atwa, E.M.E.; Assaf, M.I.E.E.K.; Ghonemy, S.; Besheer, R.M.B.M.E. A Comparative Study Between the Fractional Co2 Laser and Carboxytherapy in Treatment of Striae Distensae: A Clinical and Histopathological Study. Zagazig Univ. Med. J. 2022, 28, 791–804. [Google Scholar]
- Savas, J.A.; Ledon, J.A.; Franca, K.; Nouri, K. Lasers and lights for the treatment of striae distensae. Lasers Med. Sci. 2014, 29, 1735–1743. [Google Scholar] [CrossRef]
- Nouri, K.; Romagosa, R.; Chartier, T.; Bowes, L.; Spencer, J.M. Comparison of the 585 nm pulse dye laser and the short pulsed CO2 laser in the treatment of striae distensae in skin types IV and VI. Dermatol. Surg. 1999, 25, 368–370. [Google Scholar] [CrossRef]
- Aldahan, A.S.; Shah, V.; Mlacker, S.; Samarkandy, S.; Alsaidan, M.; Nouri, K. Laser and Light Treatments for Striae Distensae: A Comprehensive Review of the Literature. Am. J. Clin. Dermatol. 2016, 17, 239–256. [Google Scholar] [CrossRef]
- Naein, F.F.; Soghrati, M. Fractional CO2 Laser as an Effective Modality in Treatment of Striae Alba in Skin Types III and IV. J. Res. Med. Sci. 2012, 17, 928–933. [Google Scholar]
- Lee, S.E.; Kim, J.H.; Lee, S.J.; Lee, J.E.; Kang, J.M.; Kim, Y.K.; Bang, D.; Cho, S.B. Treatment of Striae Distensae Using an Ablative 10,600-Nm Carbon Dioxide Fractional Laser: A Retrospective Review of 27 Participants. Dermatol. Surg. 2010, 36, 1683–1690. [Google Scholar] [CrossRef]
- Alexiades-Armenakas, M.; Sarnoff, D.; Gotkin, R.; Sadick, N. Multi-Center Clinical Study and Review of Fractional Ablative CO2 Laser Resurfacing for the Treatment of Rhytides, Photoaging, Scars and Striae. J. Drugs Dermatol. 2011, 10, 352–362. [Google Scholar] [PubMed]
- Halachmi, S.; Onder, M.; Fritz, K. Fractional Radiofrequency. Aesthet. Dermatol. 2015, 2, 50–61. [Google Scholar]
- Kim, I.S.; Park, K.Y.; Kim, B.J.; Kim, M.N.; Kim, C.W.; Kim, S.E. Efficacy of intradermal radiofrequency combined with autologous platelet-rich plasma in striae distensae: A pilot study. Int. J. Dermatol. 2012, 51, 1253–1258. [Google Scholar] [CrossRef] [PubMed]
- Manuskiatti, W.; Boonthaweeyuwat, E.; Varothai, S. Treatment of Striae Distensae with a TriPollar Radiofrequency Device: A Pilot Study. J. Dermatol. Treat. 2009, 20, 359–364. [Google Scholar] [CrossRef]
- Sany, I.; Sobhi, R.M.; Badawi, A.; Mostafa, P.I.N.; Elmaadawi, Z.M. Comparative Study Between the Efficacy of Fractional CO2 Laser/Radiofrequency, PRP and a Combination of Both in the Treatment of Striae Distensae: A Pilot Study. Clin. Cosmet. Investig. Dermatol. 2022, 15, 1687–1694. [Google Scholar] [CrossRef]
- Harmelin, Y.; Boineau, D.; Cardot-Leccia, N.; Fontas, E.; Bahadoran, P.; Becker, A.; Montaudié, H.; Castela, E.; Perrin, C.; Lacour, J.; et al. Fractionated Bipolar Radiofrequency and Bipolar Radiofrequency Potentiated by Infrared Light for Treating Striae: A Prospective Randomized, Comparative Trial with Objective Evaluation. Lasers. Surg. Med. 2016, 48, 245–253. [Google Scholar] [CrossRef]
- Gemert, M.J.; Jacques, S.L.; Sterenborg, H.J.C.M.; Star, W.M. Skin Optics. IEEE Trans. Biomed. Eng. 1989, 36, 1146–1154. [Google Scholar] [CrossRef]
- Alhallak, K.; Omran, D.; Tomi, S.; Abdulhafid, A. Skin, Light and Their Interactions, an In-Depth Review for Modern Light-Based Skin Therapies. 2021. Available online: https://www.heraldopenaccess.us/article_pdf/22/skin-light-and-their-interactions-an-in-depth-review-for-modern-light-based-skin-therapies.pdf (accessed on 25 June 2020).
- Li, S.; Ardabilian, M.; Zine, A. Fast Determination of Melanin based on Skin Hyperspectral Reflectance. In Proceedings of the 25th International Conference on Pattern Recognition (ICPR), Milan, Italy, 10–15 January 2021; Available online: https://ieeexplore.ieee.org/document/9412919 (accessed on 25 June 2020).
- Chan, A.W.; Tetzlaff, J.M.; Gøtzsche, P.C.; Altman, D.G.; Mann, H.; Berlin, J.A.; Dickersin, K.; Hróbjartsson, A.; Schulz, K.F.; Parulekar, W.R.; et al. SPIRIT 2013 Explanation and Elaboration: Guidance for Protocols of Clinical Trials. BMJ 2013, 346, 7586. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Period | ||||||
|---|---|---|---|---|---|---|
| Screening | Baseline 0-Month | 1-Month | 2-Month | 3-Month | ||
| Patient | Eligibility Informed consent Clinical data Physical examination Randomization | X | X X X X | |||
| Intervention | Fractional CO2 laser: Group A | 1 session per month for 3 months | ||||
| Fractional radiofrequency: Group B | 1 session per month for 3 months | |||||
| Outcomes | Digital photo collection | X | X | X | X | |
| Cutaneous temperature | X | X | X | X | ||
| Skin pH | X | X | X | X | ||
| Skin elasticity | X | X | X | X | ||
| Participant Safety | Adverse effects | X | X | X | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendes, N.; Alves, P.J.; Barros, M.; Machado, J. Fractional CO2 Laser versus Fractional Radiofrequency for Skin Striae Treatment: Study Protocol for a Randomized Controlled Trial. Healthcare 2022, 10, 2372. https://doi.org/10.3390/healthcare10122372
Mendes N, Alves PJ, Barros M, Machado J. Fractional CO2 Laser versus Fractional Radiofrequency for Skin Striae Treatment: Study Protocol for a Randomized Controlled Trial. Healthcare. 2022; 10(12):2372. https://doi.org/10.3390/healthcare10122372
Chicago/Turabian StyleMendes, Nuno, Paulo Jorge Alves, Mafalda Barros, and Jorge Machado. 2022. "Fractional CO2 Laser versus Fractional Radiofrequency for Skin Striae Treatment: Study Protocol for a Randomized Controlled Trial" Healthcare 10, no. 12: 2372. https://doi.org/10.3390/healthcare10122372