
Effectiveness of Acupuncture in Parkinson’s Disease Symptoms—A Systematic Review
 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Methods for Study Identification and Screening Literature Search
2.2. Inclusion and Exclusion Criteria
2.2.1. Types of Studies
2.2.2. Participants
2.2.3. Types of Interventions
2.2.4. Types of Outcome Measures
2.3. Data Collection, Analysis and Management
3. Results
3.1. Participants
3.1.1. Groups
3.1.2. Number of Participants
3.1.3. Including and Excluding Criteria
3.2. Randomisation
3.3. Treatment Characteristics
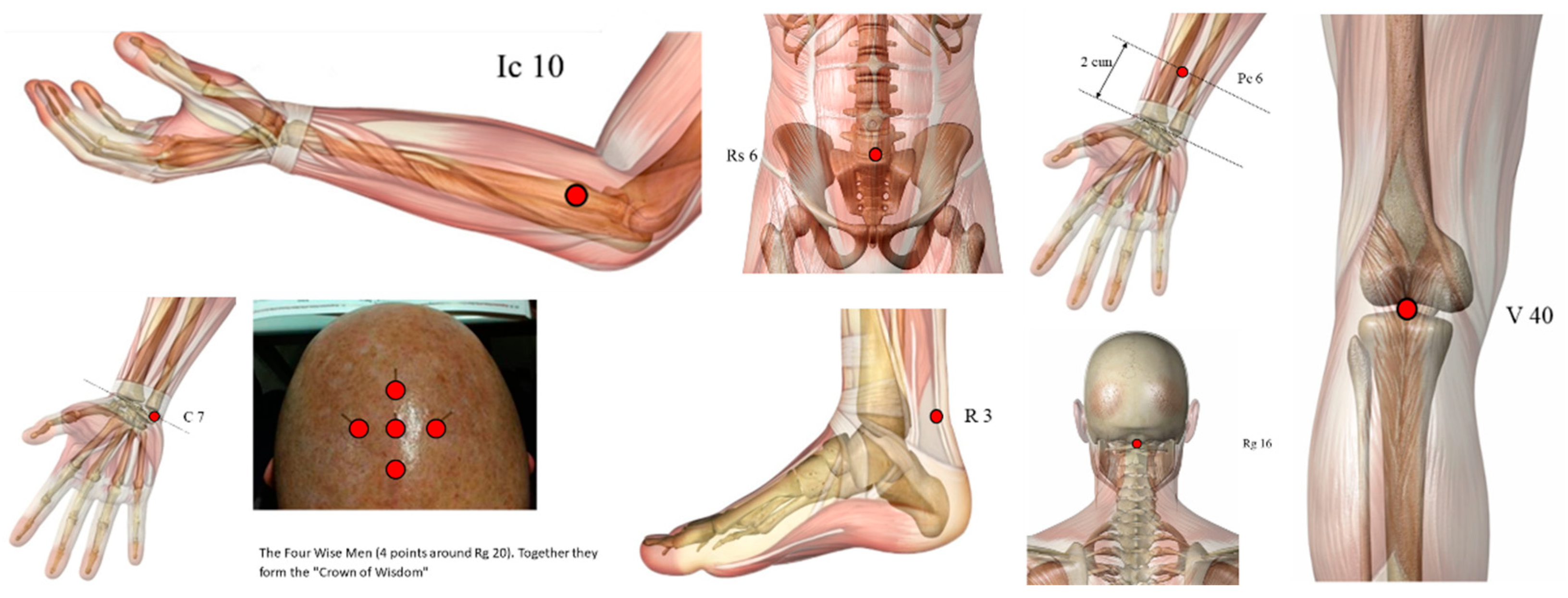
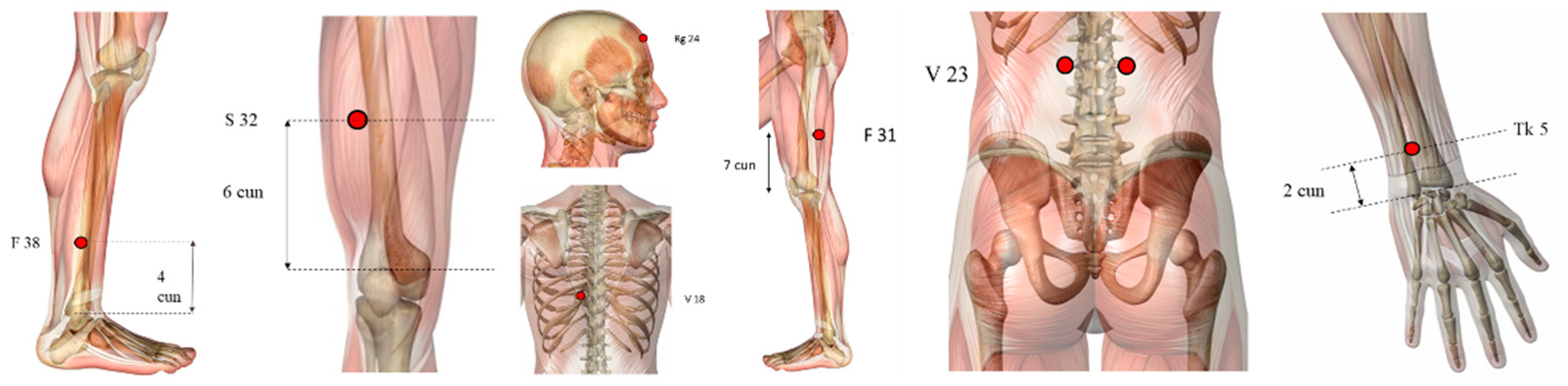
3.3.1. Points
3.3.2. Recurrence Rate
3.3.3. Efficacy Rate
3.4. Outcome Measure
3.5. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gai, C.; Qiang, T.; Zhang, Y.; Chai, Y.; Feng, W.; Sun, H. Electroacupuncture in treatment of Parkinson disease: A protocol for meta-analysis and systematic review. Medicine 2021, 100, e23010. [Google Scholar] [CrossRef]
- Lee, S.H.; Lim, S. Clinical effectiveness of acupuncture on Parkinson disease: A PRISMA-compliant systematic review and meta-analysis. Medicine 2017, 96, e5836. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, Z.; Qin, S.; Fan, W.; Li, W.; Liu, J.; Wang, S.; Xu, Z.; Zhao, M. Acupuncture for Parkinson’s Disease: Efficacy Evaluation and Mechanisms in the Dopaminergic Neural Circuit. Neural Plast. 2021, 2021, 9926445. [Google Scholar] [CrossRef]
- Zeng, B.Y.; Salvage, S.; Jenner, P. Current development of acupuncture research in Parkinson’s disease. Int. Rev. Neurobiol. 2013, 111, 141–158. [Google Scholar] [CrossRef]
- Kalia, L.V.; Lang, A.E. Parkinson disease in 2015: Evolving basic, pathological and clinical concepts in PD. Nat. Rev. Neurol. 2016, 12, 65–66. [Google Scholar] [CrossRef]
- Afentou, N.; Jarl, J.; Gerdtham, U.G.; Saha, S. Economic Evaluation of Interventions in Parkinson’s Disease: A Systematic Literature Review. Mov. Disord. Clin. Pract. 2019, 6, 282–290. [Google Scholar] [CrossRef] [Green Version]
- Findley, L. The economic impact of Parkinson’s disease. Park. Relat. Disord. 2007, 13, S8–S12. [Google Scholar] [CrossRef]
- Zeng, B.Y.; Zhao, K. Effect of Acupuncture on the Motor and Nonmotor Symptoms in Parkinson’s Disease-A Review of Clinical Studies. CNS-Neurosci. Ther. 2016, 22, 333–341. [Google Scholar] [CrossRef] [Green Version]
- Fukuda, S.; Egawa, M. Effect of acupuncture on gait in Parkinson’s disease: A case report. Acupunct. Med. 2015, 33, 325–328. [Google Scholar] [CrossRef]
- Kwon, S.; Seo, B.K.; Kim, S. Acupuncture points for treating Parkinson’s disease based on animal studies. Chin. J. Integr. Med. 2016, 22, 723–727. [Google Scholar] [CrossRef]
- Li, Z.; Hu, Y.Y.; Zheng, C.Y.; Su, Q.Z.; An, C.; Luo, X.D.; Liu, M.C. Rules of meridians and acupoints selection in treatment of Parkinson’s disease based on data mining techniques. Chin. J. Integr. Med. 2015, 26, 624–628. [Google Scholar] [CrossRef]
- Deuel, L.M.; Seeberger, L.C. Complementary Therapies in Parkinson Disease: A Review of Acupuncture, Tai Chi, Qi Gong, Yoga, and Cannabis. Neurotherapeutics 2020, 17, 1434–1455. [Google Scholar] [CrossRef]
- Danqing, X. Acupuncture for Parkinson’s Disease: A review of clinical, animal, and functional Magnetic Resonance Imaging studies. J. Tradit. Chin. Med. 2015, 35, 709–717. [Google Scholar] [CrossRef] [Green Version]
- Kabra, A.; Sharma, R.; Kabra, R.; Baghel, U.S. Emerging and Alternative Therapies For Parkinson Disease: An Updated Review. Curr. Pharm. Des. 2018, 24, 2573–2582. [Google Scholar] [CrossRef]
- de Amorim Aroxa, F.H.; de Oliveira Gondim, I.T.G.; Santos, E.L.W.; de Sales, M.D.G.W.; Asano, A.G.C.; Asano, N.M.J. Acupuncture as Adjuvant Therapy for Sleep Disorders in Parkinson’s Disease. J. Acupunct. Meridian Stud. 2017, 10, 33–38. [Google Scholar] [CrossRef]
- Hayes, M.; Fung, V.; Kimber, T.; O’Sullivan, J. Current concepts in the management of Parkinson disease. Med. J. Aust. 2020, 192, 144–149. [Google Scholar] [CrossRef]
- Huang, J.; Qin, X.; Cai, X.; Huang, Y. Effectiveness of Acupuncture in the Treatment of Parkinson’s Disease: An Overview of Systematic Reviews. Front. Neurol. 2020, 11, 917. [Google Scholar] [CrossRef]
- Jiang, F.; Yang, T.; Yin, H.; Guo, Y.; Namba, H.; Sun, Z.; Asakawa, T. Evidence for the Use of Acupuncture in Treating Disease: Update of Information From the Past 5 Years, a Mini Review of the Literature. Front. Neurol. 2018, 9, 596. [Google Scholar] [CrossRef]
- Lee, H.S.; Park, H.L.; Lee, S.J.; Shin, B.C.; Choi, J.Y.; Lee, M.S. Scalp acupuncture for Parkinson’s disease: A systematic review of randomized controlled trials. Chin. J. Integr. Med. 2013, 19, 297–306. [Google Scholar] [CrossRef]
- Lee, M.S.; Shin, B.-C.; Kong, J.C.; Ernst, E. Effectiveness of acupuncture for Parkinson’s disease: A systematic review. Mov. Disord. Off. J. Mov. Disord. Soc. 2008, 23, 1505–1515. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.-P.; Chang, C.-M.; Shiu, J.-H.; Chiu, J.-H.; Wu, T.-P.; Yang, J.-L.; Kung, Y.-Y.; Chen, F.-J.; Chern, C.-M.; Hwang, S.-J. A clinical study of integrating acupuncture and Western medicine in treating patients with Parkinson’s disease. Am. J. Chin. Med. 2015, 43, 407–423. [Google Scholar] [CrossRef] [PubMed]
- Lei, H.; Toosizadeh, N.; Schwenk, M.; Sherman, S.; Karp, S.; Sternberg, E.; Najafi, B. A Pilot Clinical Trial to Objectively Assess the Efficacy of Electroacupuncture on Gait in Patients with Parkinson’s Disease Using Body Worn Sensors. PLoS ONE 2016, 11, e0155613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Y.; Cai, X.; Qu, S.; Zhang, J.; Zhang, Z.; Yao, Z.; Huang, Y.; Zhong, Z. Madopar combined with acupuncture improves motor and non-motor symptoms in Parkinson’s disease patients: A multicenter randomized controlled trial. Eur. J. Integr. Med. 2020, 34, 101049. [Google Scholar] [CrossRef]
- Leem, J. Acupuncture for motor symptom improvement in Parkinson’s disease and the potential identification of responders to acupuncture treatment. Integr. Med. Res. 2016, 5, 332–335. [Google Scholar] [CrossRef] [Green Version]
- Kong, K.H.; Ng, H.L.; Li, W.; Ng, D.W.; Tan, S.I.; Tay, K.Y.; Au, W.L.; Tan, L.C.S. Acupuncture in the treatment of fatigue in Parkinson’s disease: A pilot, randomized, controlled, study. Brain Behav. 2018, 8, e00897. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Chen, J.; Cheng, J.; Huang, S.; Hu, Y.; Wu, Y.; Li, G.; Liu, B.; Liu, X.; Guo, W.; et al. Acupuncture Modulates the Cerebello-Thalamo-Cortical Circuit and Cognitive Brain Regions in Patients of Parkinson’s Disease with Tremor. Front. Aging Neurosci. 2018, 10, 206. [Google Scholar] [CrossRef] [Green Version]
- Yeo, S.; Choe, I.-H.; van den Noort, M.; Bosch, P.; Jahng, G.-H.; Rosen, B.; Kim, S.-H.; Lim, S. Acupuncture on GB34 activates the precentral gyrus and prefrontal cortex in Parkinson’s disease. BMC Complement. Altern. Med. 2014, 14, 336. [Google Scholar] [CrossRef] [Green Version]
- Toosizadeh, N.; Lei, H.; Schwenk, M.; Sherman, S.J.; Sternberg, E.; Mohler, J.; Najafi, B. Does integrative medicine enhance balance in aging adults? Proof of concept for the benefit of electroacupuncture therapy in Parkinson’s disease. Gerontology 2015, 61, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Sun, L.; Zhang, X.-Z.; Jia, J.; Liu, Z.; Huang, X.-Y.; Yu, S.-Y.; Zuo, L.-J.; Cao, C.-J.; Wang, X.-M.; et al. Effect and Potential Mechanism of Electroacupuncture Add-On Treatment in Patients with Parkinson’s Disease. Evid.-Based Complement. Altern. Med. 2015, 2015, 692795. [Google Scholar] [CrossRef]
- Cho, S.-Y.; Shim, S.-R.; Rhee, H.Y.; Park, H.-J.; Jung, W.-S.; Moon, S.-K.; Park, J.-M.; Ko, C.-N.; Cho, K.-H.; Park, S.-U. Effectiveness of acupuncture and bee venom acupuncture in idiopathic Parkinson’s disease. Park. Relat. Disord. 2012, 18, 948–952. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; An, S.J.; Kim, S.W.; Lee, Y. Effects of Acupuncture & Qigong Meditation on Nonmotor Symptoms of Parkinson’s Disease. J. Acupunct. Res. 2020, 7, 247–253. [Google Scholar] [CrossRef]
- Cho, S.-Y.; Lee, Y.-E.; Doo, K.-H.; Lee, J.-H.; Jung, W.-S.; Moon, S.-K.; Park, J.-M.; Ko, C.-N.; Kim, H.; Rhee, H.Y.; et al. Efficacy of Combined Treatment with Acupuncture and Bee Venom Acupuncture as an Adjunctive Treatment for Parkinson’s Disease. Altern. Complement. Med. 2018, 24, 25–32. [Google Scholar] [CrossRef]
- Werth, U.; Muñoz-Gaona, A. Comparative study of the efficacy of the usual therapy for Parkinson’s disease plus auricular acupuncture and the usual therapy without acupuncture. Rev. Int. Acupunt. 2018, 12, 5–14. [Google Scholar] [CrossRef]
- Guo, L.; Zhang, C.; Wang, J.; Teng, J.; Feng, G.; Mengyan, L. Evaluation of Rehabilitation and MRI Results of the Combined Therapy of Bushenzhichan Formula and Needle Embedding for Parkinson’s Disease. Indian J. Pharm. Sci. 2020, 82, 51–54. [Google Scholar] [CrossRef]
- Jag, J.-H.; Park, S.; An, J.; Choi, J.-D.; Seol, J.-D.; Seol, I.C.; Park, G.; Lee, S.H.; Moon, Y.; Kang, W.; et al. Gait Disturbance Improvement and Cerebral Cortex Rearrangement by Acupuncture in Parkinson’s Disease: A Pilot Assessor-Blinded, Randomized, Controlled, Parallel-Group Trial. Neurorehabilit. Neural Repair 2020, 34, 1111–1123. [Google Scholar] [CrossRef]
- Kluger, B.; Robowski, D.; Christian, M.; Cedar, D.; Wang, B.; Crawford, J.; Uveges, K.; Berk, J.; Abaca, E.; Corbin, L.; et al. Randomized, Controlled Trial of Acupuncture for Fatigue in Parkinson’s Disease. Mov. Disord. 2016, 31, 1027–1032. [Google Scholar] [CrossRef] [PubMed]
- Gelb, D.J.; Oliver, E.; Gilman, S. Diagnostic Criteria for Parkinson Disease. Arch. Neurol. 1999, 56, 33–39. [Google Scholar] [CrossRef]
- Wen, X.; Li, K.; Wen, H.; Wang, Q.; Wu, Z.; Yao, X.; Jiao, B.; Sun, P.; Ge, S.; Wen, C.; et al. Acupuncture-Related Therapies for Parkinson’s Disease: A Meta-Analysis and Qualitative Review. Front. Aging. Neurosci. 2021, 13, 676827. [Google Scholar] [CrossRef]
- Noh, H.; Kwon, S.; Cho, S.Y.; Jung, W.S.; Moon, S.K.; Park, J.M.; Ko, C.N.; Park, S.U. Effectiveness and safety of acupuncture in the treatment of Parkinson’s disease: A systematic review and meta-analysis of randomized controlled trials. Complement. Ther. Med. 2017, 34, 86–103. [Google Scholar] [CrossRef]
- Lam, Y.C.; Kum, W.F.; Durairajan, S.S.; Lu, J.H.; Man, S.C.; Xu, M.; Zhang, X.F.; Huang, X.Z.; Li, M. Efficacy and safety of acupuncture for idiopathic Parkinson´s disease: A systematic review. J. Altern. Complement. Med. 2008, 14, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Chen, L.; Zhang, Z.; Geng, G.; Chen, W.; Dong, H.; Chen, L.; Zhan, S.; Li, T. Effectiveness and safety of acupuncture combined with Madopar for Parkinson’s disease: A systematic review with meta-analysis. Acupunct. Med. 2017, 35, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Kwon, M.; Cheong, M.J.; Leem, J.; Kim, T.H. Effect of Acupuncture on Movement Function in Patients with Parkinson’s Disease: Network Meta-Analysis of Randomized Controlled Trials. Healthcare 2021, 9, 1502. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Qin, X.; Cai, X.; Huang, Y. The effectiveness of acupuncture for Parkinson’s disease: An overview of systematic reviews. Complement. Ther. Med. 2020, 50, 102383. [Google Scholar] [CrossRef]
- Chae, Y.; Lee, H.; Kim, H.; Kim, C.H.; Chang, D.I.; Kim, K.M.; Park, H.J. Parsing brain activity associated with acupuncture treatment in Parkinson’s diseases. Mov. Disord. 2009, 24, 1794–1802. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Details | Participants | Study Design | Control Group | Interventions (GE) | Outcomes Measures | Results/Conclusions | Side Effect |
|---|---|---|---|---|---|---|---|
| A Clinical Study of Integrating Acupuncture and Western Medicine in Treating Patients with Parkinson’s Disease The American Journal of Chinese Medicine [22] | Inclusion Criteria: Diagnosed with PD for over 6 months (criteria of the Core Assessment Program for Intracerebral Transplantation (CAPIT). Exclusion Criteria: Severe diseases of the heart, brain, liver, kidneys, endocrine, or hematopoietic system, psychosis, or dementia and who did not agree to participate in the study. Dropout: NA Randomisation: Non-random sample | Effects of acupuncture treatment in PD patients N = 40 | Drug Therapy Levodopa N = 20 | Acupuncture Treatment + Drug Therapy 19 points: DU20 (unilateral), GB20, LI11, LI10, LI4, GB31, ST32, GB34, GB38 (bilateral) Frequency: 2×/week - short-term (18 weeks—36 sessions) n = 20 - long-term (36 weeks—72 sessions) n = 13 Depth of insertion: 5–30 mm Needle stimulation: manual (“De-Qi”: soreness, numbness, distention and pain) Time: 15 min Needle type: 0.27 mm × 25/40 mm | 3 Assessment Moments:before, in the middle and at the end of the study. - Unified Parkinson’s Disease Rating Scale (UPDRS) - Beck Anxiety Inventory (BAI) - Beck Depression Inventory-Version 2 (BDI-II) - WHO quality of life (WHOQOL) | Acupuncture treatment: -reduces symptoms and signs of mind, behaviour, mood, depression - complications of therapy - reduce UPDRS scores - improve the quality of life | NO |
| A Pilot Clinical Trial to Objectively Assess the Efficacy of Electroacupuncture on Gait in Patients with Parkinson’s Disease Using Body Worn Sensors PLoS ONE [23] | Inclusion Criteria: (1) Community-dwelling aged 55 years or older with a diagnosis of PD; (2) patients who can walk 20 m without walking assistance; and (3) patients who are stable without anti-PD medication(s) change for at least 1 month. Exclusion Criteria: Patients who (1) have received previous acupuncture; (2) DBS; (3) with any clinically significant medical condition, psychiatric condition, drug or alcohol abuse, or laboratory abnormality that would, in the judgment of the investigators, interfere with the ability to participate in the study; and (4) with non-PD related gait disorders Dropout: zero dropout rate Randomisation: drawing pieces of paper from a bag | Efficacy of EA for gait disorders using body-worn sensor technology in patients with PD N = 15 | Sham Acupuncture Insertion less than 4 mm, under the skin at non-acupuncture points, without needle manipulation N = 5 | EA Treatment 11 points: in Foot Motor Sensory Area, Balance Area, GV20, GV14, LI4, ST36, GB34, BL40, SP6, KI3, LR3 Frequency: 3×/week Depth of insertion: 0.25 × 40–50 mm—Transversely in GV20, Balance Area, Foot Motor Sensory Area and Perpendicularly in the rest Needle stimulation: from 4 to 100 Hz. The pulse was an asymmetric biphasic square wave with a pulse width of 100 microseconds (μS). “De-qi” was achieved with needle manipulation. Three pocket portable electric stimulators (ITO ES-130, Japan) were used for EA stimulation. Time: 30-min sessions Needle type: Sterile disposable, surgical stainless steel acupuncture needles (Seirin, L type, Japan) N = 10 | 2 Assessment Moments: At baseline and after completion of treatments. - Unified Parkinson’s Disease Rating Scale (UPDRS) - SF-12 health survey - Short Falls Efficacy Scale-International (FES-I) - Visual analogue scale (VAS) - Steady-state gait speed (stride length, cadence, double support, and midswing angular velocity) | All gait parameters were improved in the experimental group in response to EA treatment. | YES |
| Acupuncture as Adjuvant Therapy for Sleep Disorders in Parkinson’s Disease Journal of Acupuncture and Meridian Studies [15] | Inclusion criteria: (1) patients with idiopathic PD according to the UK Parkinson’s Disease Society Brain Bank criteria (2) Stage I e III PD, according to the Hoehn e Yahr scale (3) age 35 e 80 years; (4) minimum score of 18 on the Mini-Mental State Examination for a low academic level or a minimum score of 26 for high academic level and (5) a stable dose of antiparkinsonian medication for 2 months. Exclusion criteria: another neurological condition or who had received physiotherapy Dropout: NA Randomisation: The patients were enumerated and allocated to experimental or control groups according to a simple raffle. | Effects of acupuncture on sleep disturbances N = 11 | No Intervention N = 11 | Acupuncture Treatment 8 points: LR3, SP6, LI4, TE5, HT7, PC6, LI11, GB20. Frequency: 1×/week for 8 weeks Time: 30 min N = 11 | 2 Assessment Moments:Prior to the start of the study and after. - MMSE - HY scale - PDSS (Parkinson’s Disease Sleep Scale) | A therapeutic benefit of acupuncture in sleep disorders in patients with PD. | NO |
| Madopar combined with acupuncture improves motor and non-motor symptoms in Parkinson’s disease patients: A multicentre randomised controlled trial. European Journal of Integrative Medicine [24] | Inclusion: (1) met the diagnostic criteria; (2) aged between 40–75 years; (3) patients with the revised Hoehn–Yahr stage 1–4; (4) Madopar dosage could be maintained for ≥3 months with a stable medical condition or first-consult patients who had not been treated for Parkinson’s disease in the past; (5) inpatients or outpatients who were able to follow up; (6) conscious with normal communication; and (7) signed informed consent form. Exclusion: Patients with (1) Hoehn–Yahr stage 4–5; (2) Parkinson’s syndrome (3) merged with other serious diseases, such as diseases of the heart, liver, kidney, endocrine and hematopoietic system; (4) mental illness or dementia; (6) allergic patients; or (7) non-first-consult patients. | Effect of integrated therapy on improving motor and nonmotor symptoms in PD patients. N = 76 | Drug Therapy Madopar only | Acupuncture Treatment + Drug Therapy (Madopar) Jin’s three-needle therapy: GV17, GB19A, Sishenzhen and temporal three-needle midpoint of the posterior hairline, the depression above the protuberantia occipitalis externa. Frequency: 4 days per week; 12 weeks—2×/week (four-week follow-up) Time: 30 min per day | 3 Assessment Moments: In Week 0. within (Week 4), and after (Week 8) - Unified Parkinson’s Disease Rating Scale (UPDRS) - Modified Webster Scale - Parkinson’s Disease Sleep Scale (PDSS) - Self-rating Depression Scale (SDS) | Integrated therapy showed a greater advantage, with earlier non-motor symptom improvement. Acupuncture had a certain long-term effect. | NO |
| Acupuncture for motor symptom improvement in Parkinson’s disease and the potential identification of responders to acupuncture treatment Integrative Medicine Research [25] | Inclusion: a stable dosage of anti-PD medication for at least two months without adverse effects and diagnosed by a neurologist according to the UK Parkinson’s Disease Society Brain Bank criteria Exclusion: Parkinson-plus syndrome or secondary Parkinson’s syndrome | Effectiveness of EA and explore its mechanisms in PD patients when used as adjunctive therapy to conventional drugs. N = 50 | Drug Therapy | EA + drug 4 points: GB20 + LI4 and central GV16 + GV14 Frequency: 8 weeks—20 session sessions that occur every 3 days Needle stimulation: 9 V, 1 A, 9 W, and 100 Hz Time: 30 min | Assessment Moments: 12 h after the latest intake of medication. - Unified Parkinson’s Disease Rating Scale (UPDRS) III and IV - Hoehn–Yahr (H-Y) stage -Nonmotor Symptoms Quest (NMSQ) -Parkinson’s Disease Quality of Life Questionnaire (PDQ) 39 items - Hamilton Depression Scale (HAMD) - Pittsburgh Sleep Quality Index (PSQI) - Hamilton Anxiety Scale (HAMA) - Neuroinflammatory factors: nitric oxide, tumour necrosis factor, interleukin-1, and prostaglandin –Neurotransmitters: dopamine, acetylcholine, norepinephrine, and 5-hydroxytryptamine. | Acupuncture improves motor symptoms and quality of sleep | NO |
| Acupuncture in the treatment of fatigue in Parkinson’s disease: A pilot, randomised, controlled, study. Brain and Behaviour [26] | Inclusion: (1) diagnosis of PD based on criteria developed by Gelb, Oliver, and Gilman (1999) which is adopted by the National Institute of Neurological Disorders and Stroke, US National Institute of Health, (2) age 21–85 years old, (3) presence of moderately severe fatigue as defined by a score of ≥10 on the General Fatigue Domain of the Multidimensional Fatigue Inventory (Smets, Grasen, Bonke, and De Haes, 1995), and (4) no acupuncture treatment in the past 6 months. Exclusion: (1) significant cognitive, language or psychiatric illnesses which prevent the subject from understanding instructions and participating in the study, (2) needle phobia, (3) comorbidity with a bleeding disorder, (4) known anaemia with haemoglobin level < 10 g/dl, (5) known congestive cardiac failure and/or end-stage renal disease, (6) female subjects of childbearing age, and (7) presence of symptomatic postural hypotension. | Efficacy of acupuncture in patients with PD-related fatigue N = 40 | Sham Acupuncture Needles developed by Jongbae Park (Park Sham Device, PSD)—When pressed onto the skin, it telescopes into the handle and the blunt tip stay on the skin instead of penetrating it. The plastic tube with adhesive foot-plate is placed on the skin to hold it in place | Real Acupuncture 11 acupoints: right PC 6, left PC 6, right LI 4, left LI4, right ST 36, left ST 36, right SP 6, left SP 6, right KI 3, left KI 3, and CV 6. Frequency: 10 sessions—5 weeks—2×/week Time: 20 min | 3 Assessment Moments: at baseline, 5 and 9 weeks. - General Fatigue Score of the Multidimensional Fatigue Inventory (MFI-GF) - MFI-Total Score - Unified Parkinson’s Disease Rating Scale Motor score (UPDRS Motor) - Parkinson’s Disease Questionnaire-39 (PDQ 39) - Geriatrics Depression Scale (GDS) - Epworth Sleepiness Scale ESS) | Both real and sham acupuncture are equally effective in improving PD-related fatigue, and this is likely due to nonspecific or placebo effects this improvement was maintained up to 4 weeks after completion of treatment. | YES—3 |
| Acupuncture Modulates the Cerebello-Thalamo-Cortical Circuit and Cognitive Brain Regions in Patients of Parkinson’s Disease with Tremor Frontiers Aging Neuroscience [27] | Inclusion: diagnosed based on the UK PD Society Brain Bank clinical diagnostic criteria, and tremor at rest in at least one upper or lower extremity on either side was assessed by item 20 of the Unified Parkinson’s Disease Rating Scale Exclusion: secondary Parkinsonism, atypical parkinsonian disease, advanced PD stage (H-Y ≥ 4), age less than 45 or greater than 80 years, history of other neurological disorders or head trauma, left-handedness, cognitive impairment (Mini-Mental State Examination (MMSE) score < 24), depression tendency (Beck Depression Inventory (BDI) score > 4), and any contraindications for fMRI. | Effect of acupuncture on PD patients with tremor and its potential neural mechanism by fMRI N = 41 | Sham Acupuncture (0.2 cm deep and 0.5cun next to the points) + Waiting Group (True acupuncture was performed after final evaluation) | True acupuncture group DU20, GB20, and the Chorea-Tremor Controlled Zone Needle stimulation: The reinforcing-reducing method conducted by twirling was performed every 10 min Time: 30 min needle retention time | 2 Assessment Moments:Before and after the treatment course. - fMRI scans of the patients’ brains - UPDRS II and III subscales | Acupuncture reduces tremor | NO |
| Acupuncture on GB34 activates the precentral gyrus and prefrontal cortex in Parkinson’s disease BMC Complementary and Alternative Medicine [28] | Inclusion: Diagnosed with clinically definite idiopathic PD by a neurologist from the Kyung Hee Medical Hospital. Exclusion: Atypical parkinsonian disorder, other neurological or major medical conditions (head injury, stroke) or current psychiatric problems. | Evaluate the influence of GB 34 in brain areas And compare brain activity between PD patients and healthy participants N = 24 | Healthy Participants N = 12 | PD Patients 1 Point: Right GB 34 (frequently used acupoint for motor function treatment in the oriental medical field needle) Depth of insertion: 1.0 cm Needle type: 0.25 × 40 mm N = 12 | Assessment Moments - fMRI experiment - Edinburg Handedness Inventory - Hoen and Yahr stage - Korean Mini-Mental State Examination - Beck Depression Inventory | GB 34 seems to be a suitable acupoint | NO |
| Does Integrative Medicine Enhance Balance in Aging Adults?—Proof of Concept for Benefit of Electro-acupuncture Therapy in Parkinson’s Disease Gerontology [29] | Inclusion: Aging adults aged 55 years or older with idiopathic PD diagnosed by movement disorder specialists based on the UK Brain Bank criteria. Exclusion: Any type of neurological disorder other than PD or if they have prior experience with EA therapy. | Assess EA improvement in postural balance in PD patients N = 56 | Sham Acupuncture (With the insertion of needles just under the skin at non-acupuncture points) stimulation with minimal intensity compared to real EA (just turning on the light of the stimulator) Healthy Participants | EA treatment 20 points: GV20, GV14 on the midline and bilateral Foot Motor Sensory Area, Balance Area, bilateral ST36, LI4, GB34, LR3, KI3, SP6, BL40. Frequency: 1×/week—3 weeks Needle stimulation: Electrical stimulation frequency: 4 Hz or 100 Hz with intensity just below the level that induces visible muscle contraction. Time: 30 min N = 15 | 2 Assessment Moments: At baseline and after the final therapy. In the “off medication stage” (>12 h after their last PD medication dose). - Balance assessment (Medial-lateral centre of gravity sway to anterior-posterior sway and ankle-to-hip sway during eyes-open, eyes-closed, and eyes-open dual-tasks trials) - Unified Parkinson’s Disease Rating Scale (UPDRS) - Visual analogue scale (VAS) - SF-12 health survey - Short Falls Efficacy Scale-International (SHORT FES-I) - Mini-Mental State Examination (MMSE) - Hoehn and Yahr staging | Improvement in rigidity and balance following EA | NO |
| Effect and Potential Mechanism of Electroacupuncture Add-On Treatment in Patients with Parkinson’s Disease Evidence-Based Complementary and Alternative Medicine [30] | Inclusion: a stable dose of anti-Parkinsonian medication for at least 2 months and did not report adverse events. Patients were diagnosed with PD according to UK Parkinson’s Disease Society Brain Bank criteria. Exclusion: secondary Parkinson’s syndromes, Parkinson-plus syndromes, infectious disease in central and peripheral systems, dysarthria, severe psychiatric diseases affecting expression, malignant tumour, disability, and other serious somatic diseases. | Effectiveness and mechanisms of EA add-on treatment in PD patients N = 50 | Drug Therapy | Drug + EA 6 points: bilateral GB20 and LI4 and central Du14 and Du16 Frequency: 20 sessions every 3 days and lasted 2 months Depth of insertion: 2.0–2.5 cm Needle stimulation: inserted obliquely electrical pulses of 9 V, 1 A, 9 W, and 100 Hz Time: 30 min Needle type: 0.25 mm × 40 mm | 2 Assessment Moments Before and after. GC was reevaluated on the first day after 2 months of drug treatment. Evaluated 12 h after Parkinsonian drugs. - Unified Parkinson’s Disease Rating Scale (UPDRS) III - Hamilton Depression Rating Scale (HAMD-) - Pittsburgh Sleep Quality Index - Anxiety Scale- (HAMA-) - Nonmotor Symptoms Quest (NMSQ) - Montreal Cognitive Assessment - Mini-Mental State Examination | EA dramatically reduces motor symptoms of PD patients and nonmotor symptoms, especially sleep quality and depression | NO |
| Effectiveness of acupuncture and bee venom acupuncture in idiopathic Parkinson’s disease Parkinsonism and Related Disorders [31] | Inclusion: adults with idiopathic Parkinson’s disease who had been on a stable dose of antiparkinsonian medication for at least 1 month. The study neurologist diagnosed each patient with IPD based on symptoms, medications, and brain imaging. Exclusion: patients with severe previous or current psychiatric or organic brain disorders other than PD (including secondary Parkinsonism), atypical Parkinsonism, somatic diseases, alcohol abuse, or narcotic abuse. | Effectiveness of both acupuncture and bee venom acupuncture as adjuvant therapies for idiopathic Parkinson’s disease N = 35 | No Intervention N = 9 | 1. Acupuncture Treatment 2. Bee Venom Acupuncture Treatment 10 points: GB 20, LI11, GB34, ST36, LR3 bilateral Frequency: 16 total sessions—twice a week for 8 weeks Depth of insertion: 1.0 × 101.5 cm Needle stimulation: rotated at 2 Hz for 10 s to achieve Deqi Time: 20 min. Needle type: 0.25mm × 0.30 mm N = 13 each | 2 Assessment Moments Before and after the treatment. - Unified Parkinson’s Disease Rating Scale - Parkinson’s Disease Quality of Life Questionnaire - Beck Depression Inventory - Berg Balance Scale - Time and number of steps required to walk 30 m | Both acupuncture and bee venom acupuncture showed promising results as adjuvant therapies for Parkinson’s disease | NO |
| Effects of Acupuncture and Qigong Meditation on Nonmotor Symptoms of Parkinson’s Disease Journal of Acupuncture Research [32] | Inclusion: idiopathic PD (based on UK Parkinson’s Disease Society Brain Bank criteria), who were taking an anti- Parkinson’s medication Exclusion: NA | Whether Qigong and acupuncture affect nonmotor symptoms of PD N = 21 | Qigong Meditation Only | Acupuncture and Qigong Meditation 6 points: bilateral GB20, LI4 and central Du14 and Du16 + Healing breathing, Kwanjeong Meditation, and Qigong healing—repeated 12 times Frequency: 12 treatments—5 min until De qi was achieved Depth of insertion: 2.0–2.5 cm obliquely Time: 50 min Needle type: 0.25 × 40 mm | 2 Assessment Moments Before and after 12 treatments at baseline and 1 month after 12 treatments. - Unified Parkinson’s Disease Rating Scales (UPDRS 1) - Test of Smell Identification (TSI) | The combination of Qigong and acupuncture and Qigong alone was shown to improve the nonmotor symptoms and olfactory function of PD. | NA |
| Efficacy of Combined Treatment with Acupuncture and Bee Venom Acupuncture as an Adjunctive Treatment for Parkinson’s Disease The Journal of Alternative and Complementary Medicine [33] | Inclusion: Stable dose of antiparkinsonian medication for at least 1 month; Hoehn and Yahr scale I–IV; More than 1 point in two or more items in the UPDRS part III; Mini-Mental State Examination-Korean version score greater than 24 points (out of 30); Consent to the study after full description. Exclusion: Severe psychiatric or organic brain disorders other than PD, previous or current; Secondary parkinsonism due to medication, cerebrovascular disease, tumour, infection, etc; Atypical Parkinsonism or Parkinson-plus syndrome; Somatic disease; Alcohol or narcotic abuse; Expecting a baby; Determined to be inappropriate for participation by the investigator. Dropout: Skipped more than 8 of the total 24 treatment sessions in the study or control group; Not able to continue the study because of serious adverse events or aggravation of the condition; Withdrawal of the consent; Impossible to complete the scheduled study as planned by the judgment of the principal investigator. Randomisation: Double-blind | Efficacy of acupuncture and bee venom acupuncture for idiopathic Parkinson’s disease. Duration of the effects by follow-up assessments at the end of the treatment N = 63 | Drug Therapy Antiparkinsonian drugs without additional intervention Sham Acupuncture received a normal saline injection (shallow minimal acupuncture stimulation was performed at the same points using the same acupuncture needles for 15 min without de qi) | Acupuncture Treatment 10 points: GB20, LI11, GB34, ST36, and LR3 bilateral Frequency: twice a week for 12 weeks Depth of insertion: 1.0–1.5 cm Needle stimulation: rotated at 2 Hz for 10 s to achieve de qi Time: 15 min Needle type: 0.25 × 30 mm | 4 Assessment Moments At baseline and at 12, 16, and 20 weeks. Performed in the medication “on” - Unified Parkinson’s Disease Rating Scale (UPDRS) part II and part III score - Postural instability—posturography using the Balance Master System - Gait disturbance (PIGD) score - Gait speed and number - Parkinson’s Disease Quality of Life Questionnaire - Beck Depression Inventory | Combined treatment of acupuncture and BVA might be a safe and useful adjunctive treatment | NO |
| Comparative study of the efficacy of the usual therapy for Parkinson’s disease plus auricular acupuncture and the usual therapy without acupuncture Revista Internacional de Acupuntura [34] | Inclusion: Diagnosis of idiopathic PE confirmed by a neurologist. Symptomatic PE with a duration of between 1 and 15 years before entering the study. Age between 30 and 75 years at the time of diagnosis. Exclusion: Major motor disabilities (only a la EP). Psychiatric illnesses such as: Clinically diagnosed depression (severe depression will be considered to have 30 points or more on the Beck scale), generalised anxiety, social phobia, etc.—Cortical dementia with synamnesia, aphasia, or any other typical Alzheimer’s symptom.—Parkinsonism (parkinsonian syndromes), isolated phenomena, cerebellar syndrome. | Efficacy of the routine treatment in Parkinson’s disease (PD) plus permanent auricular acupuncture versus routine treatment without acupuncture N = 32 | Sham Acupuncture | 100–120 needles Depth of insertion: 2 mm Needle type: titanium needles | 2 Assessment Moments Before and 12 weeks after. - Unified Parkinson’s Disease Rating Scale | The efficacy of the Forever Needles, compared to those of the group without permanent insertion for the treatment of PD, could not be established in this study. | NA |
| Evaluation of Rehabilitation and MRI Results of the Combined Therapy of Bushenzhichan Formula and Needle Embedding for Parkinson’s Disease Indian Journal of Pharmaceutical Sciences [35] | Inclusion: Diagnostic criteria of the Motor Disorder and (PD) Group of the Chinese Medical Association Neurology Chapter Exclusion: NA | Evaluate Parkinson’s disease patients using combined therapy of Bushenzhichan formula and needle embedding and analysing the Magnetic resonance imaging test results N = 180 | Drug Therapy Madopar Only (100/1500 mg, 3–4 times a day) N = 90 | Madopar as well as combined therapy of Bushenzhichan formula and needle embedding. The constituents of Bushenzhichan formula are as follow up 9 g deer antler glue, 9 g Zhigancao, 20 g raw tortoise plastron, 20 g fructus cannabis, 20 g codonopsis, 20 g raw turtle shell, 12 g gelatin, 12 g gastrodiaelata, 12 g pulp of cornus, 30 g Fructus Lycii, 30 g Radix Paeoniae alba, 30 g dries Radix Rehmanniae, 30 g cistanche, 30 g uncaria, 15 g Radix Ophiopogonis, 10 g polygonatum. It is considered a single Chinese herb free from decoction, which could be dissolved in 400 mL of boiled water, once a day, and used as a tea after lunch and dinner while warm Points: Baihui (GV 20), Sishencong (EX-HN 1), Fengchi (GV 20), Taichong (LR 3), Yanglingquan (GB 34), Sanyinjiao (BP6), Hegu (LI4), Ganshu (BL18), Shenshu (BL23) and the chorea-trembling controlled area. N = 90 | Assessment Moments - MRI test results - UPDRS | The combined therapy of Bushenzhichan formula and needle embedding could significantly improve the therapeutic efficacy and promote recovery in Parkinson’s disease patients | NA |
| Gait Disturbance Improvement and Cerebral Cortex Rearrangement by Acupuncture in Parkinson’s Disease: A Pilot Assessor-Blinded, Randomised, Controlled, Parallel-Group Trial Neurorehabilitation and Neural Repair [36] | Inclusion: WI Exclusion: WI Randomisation: Not blinding | Effects of acupuncture on gait disturbance N = 26 | Drug Therapy | Acupuncture Treatment + Drug Therapy 8 treatments—2×/week for 4 weeks Points: WI | Assessment Moments Assessments in the “on” state intervention phase (4 weeks) and a follow-up phase (4 weeks). - Gait parameters—GAITRite system and hemodynamic responses in the cerebral cortices using functional near-infrared spectroscopy - Unified Parkinson’s Disease Rating Scale (UPDRS) scores - Neurotransmitter levels | Acupuncture tended to improve hypometric gait and rearranged activation of the cerebral cortex | NA |
| Randomised, Controlled Trial of Acupuncture for Fatigue in Parkinson’s Disease Movements Disorders [37] | Inclusion: UK Brain Bank criteria for probable PD10; age 40 to 99 years; fluent in English; stable medication uses for 30 days; and self-reported moderate or severe fatigue using the International Parkinson’s and Movement Disorder Society UPDRS fatigue item. Exclusion: dementia or a score below 24 on the Montreal Cognitive Assessment (MoCA) presence of another medical condition expected to produce fatigue; active depression or Hospital Anxiety and Depression Scale (HADS) depression subscale score greater than 10; the presence of an untreated sleep disorder; or exposure to acupuncture within the past 6 months. | Determine whether a 6-week course of acupuncture could improve PD-related fatigue N = 94 | Sham Acupuncture (non-acupuncture points, located 0.5 in lateral to the real) | Acupuncture Treatment 11 points: GV20, GV24, CV6, unilateral, LI 10, HT 7, ST36, SP 6 bilateral Frequency: 2/week during 6 weeks = 12 Treatments Depth of insertion: 0.5 to 1 cm Needle stimulation: The needle was twisted three times to the right Time: 30 min | Assessment Moments: - Modified Fatigue Impact Scale at 6 weeks - Sleep, mood, quality of life, and maintenance of benefits at 12 weeks - Parkinson’s Disease Sleep Scale (PDSS) - Epworth Sleepiness Scale (ESS) - Apathy Evaluation Scale (AES). - Quality of life (QOL) - Parkinson’s Disease Questionnaire (PDQ-39) | Acupuncture may improve PD-related fatigue, but real acupuncture offers no greater benefit than sham treatments. | YES—constipation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, C.R.; Machado, J.; Rodrigues, J.; de Oliveira, N.M.; Criado, M.B.; Greten, H.J. Effectiveness of Acupuncture in Parkinson’s Disease Symptoms—A Systematic Review. Healthcare 2022, 10, 2334. https://doi.org/10.3390/healthcare10112334
Pereira CR, Machado J, Rodrigues J, de Oliveira NM, Criado MB, Greten HJ. Effectiveness of Acupuncture in Parkinson’s Disease Symptoms—A Systematic Review. Healthcare. 2022; 10(11):2334. https://doi.org/10.3390/healthcare10112334
Chicago/Turabian StylePereira, Catarina Ramos, Jorge Machado, Jorge Rodrigues, Natália M. de Oliveira, Maria Begoña Criado, and Henri J. Greten. 2022. "Effectiveness of Acupuncture in Parkinson’s Disease Symptoms—A Systematic Review" Healthcare 10, no. 11: 2334. https://doi.org/10.3390/healthcare10112334