
Changes in the Suicide Rate of Older Adults According to Gender, Age, and Region in South Korea from 2010 to 2017
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Variables
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.1.1. Analysis of Unconditional Model
3.1.2. Analysis of Conditional Model
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- OECD. Suicide Rates (Indicator); Organization for Economic Co-Operation and Development: Paris, France, 2022. [Google Scholar]
- KOSIS. Causes of Death Statistics in 2017; Statistics Korea: Daejeon, Republic of Korea, 2018.
- Arunkumar, P.; Maiese, A.; Bolino, G.; Gitto, L. Determined to Die! Ability to Act Following Multiple Self-inflicted Gunshot Wounds to the Head. The Cook County Office of Medical Examiner Experience (2005–2012) and Review of Literature. J. Forensic Sci. 2015, 60, 1373–1379. [Google Scholar] [CrossRef] [PubMed]
- Maiese, A.; Gitto, L.; dell’Aquila, M.; Bolino, G. A peculiar case of suicide enacted through the ancient Japanese ritual of Jigai. Am. J. Forensic Med. Pathol. 2014, 35, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Jung, H.; Won, D.; Shin, Y.; Noh, J.; Kang, T. Landscape of elderly suicide in South Korea: Its trend according to age, gender, and educational attainment. OMEGA J. Death Dying 2020, 82, 214–229. [Google Scholar] [CrossRef] [PubMed]
- Jia, C.-X.; Zhang, J. Confucian values, negative life events, and rural young suicide with major depression in China. OMEGA J. Death Dying 2017, 76, 3–14. [Google Scholar] [CrossRef]
- Kang, M.-Y.; Kim, H.-R. Association between voluntary/involuntary job loss and the development of stroke or cardiovascular disease: A prospective study of middle-aged to older workers in a rapidly developing Asian country. PLoS ONE 2014, 9, e113495. [Google Scholar] [CrossRef]
- Kim, H.; June, K.; Kim, Y. Gender differences in factors affecting suicidal ideation among the Korean elderly. J. Korean Gerontol. Soc. 2013, 33, 349–363. [Google Scholar]
- Koo, C.Y.; Kim, J.S.; Yu, J. A study on factors influencing elders’ suicidal ideation: Focused on comparison of gender differences. J. Korean Acad. Community Health Nurs. 2014, 25, 24–32. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.; Lee, M.-A. Age discrimination and suicidal ideation among Korean older adults. Am. J. Geriatr. Psychiatry 2020, 28, 748–754. [Google Scholar] [CrossRef]
- Kim, S.M.; Lee, G. Risk Factors of Suicide Ideation in Younger-Old and Older-Old Persons: Using Data from the Korea Health Panel Survey. J. Korean Gerontol. Nurs. 2020, 22, 281–290. [Google Scholar] [CrossRef]
- KFSP. White Paper on Suicide Prevention; Ministry of Health & Welfare Korea Suicide Prevention Center: Seoul, Republic of Korea, 2020.
- Yang, N.-Y.; Moon, S.-Y. The effects of suicidal thought on health status social support, and life satisfaction in elderly. J. Digit. Converg. 2012, 10, 515–524. [Google Scholar]
- Lee, S.-H.; Tsai, Y.-F.; Chen, C.-Y.; Huang, L.-B. Triggers of suicide ideation and protective factors of actually executing suicide among first onset cases in older psychiatric outpatients: A qualitative study. BMC Psychiatry 2014, 14, 269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, A.; Bhat, R.; Zarate-Escudero, S.; DeLeo, D.; Erlangsen, A. Suicide rates in five-year age-bands after the age of 60 years: The international landscape. Aging Ment. Health 2016, 20, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Innamorati, M.; Pompili, M.; Di Vittorio, C.; Baratta, S.; Masotti, V.; Badaracco, A.; Conwell, Y.; Girardi, P.; Amore, M. Suicide in the old elderly: Results from one Italian county. Am. J. Geriatr. Psychiatry 2014, 22, 1158–1167. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Ahn, J.S.; Kim, H.; Cha, Y.S.; Lee, J.; Kim, M.H.; Min, S. Sociodemographic and clinical characteristics of old-old suicide attempters compared with young-old and middle-aged attempters. Int. J. Geriatr. Psychiatry 2018, 33, 1717–1726. [Google Scholar] [CrossRef]
- Park, E.; Hyun, M.Y.; Lee, C.I.; Lee, E.J.; Hong, S.C. A Study on Regional Differentials in Death Caused by Suicide in South Korea. J. Korean Acad. Nurs. 2007, 37, 44–51. [Google Scholar] [CrossRef]
- Chan, C.H.; Caine, E.D.; You, S.; Yip, P.S.F. Changes in South Korean urbanicity and suicide rates, 1992 to 2012. BMJ Open 2015, 5, e009451. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-Y.; Yang, C.-T.; Cha, E.-S.; Sha, F.; Yip, P.S.F. Quantifying the contributions of age, sex, methods, and urbanicity to the changing suicide rate trends in South Korea, 2001–2016. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 55, 1121–1132. [Google Scholar] [CrossRef]
- Cheong, K.S.; Choi, M.H.; Cho, B.M.; Yoon, T.H.; Kim, C.H.; Kim, Y.M.; Hwang, I.K. Suicide rate differences by sex, age, and urbanicity, and related regional factors in Korea. J. Prev. Med. Public Health 2012, 45, 70–77. [Google Scholar] [CrossRef]
- Lee, J.-A.; Park, J.H.; Kim, M. Social and physical environments and self-rated health in urban and rural communities in Korea. Int. J. Environ. Res. Public Health 2015, 12, 14329–14341. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.-H.; Jung-Choi, K.; Jun, H.-J.; Kawachi, I. Socioeconomic inequalities in suicidal ideation, parasuicides, and completed suicides in South Korea. Soc. Sci. Med. 2010, 70, 1254–1261. [Google Scholar] [CrossRef]
- Oh, K.Y.; Van Dam, N.T.; Doucette, J.T.; Murrough, J.W. Effects of chronic physical disease and systemic inflammation on suicide risk in patients with depression: A hospital-based case–Control study. Psychol. Med. 2020, 50, 29–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarlow, K.R.; Johnson, T.A.; McCord, C.E. Rural status, suicide ideation, and telemental health: Risk assessment in a clinical sample. J. Rural Health 2019, 35, 247–252. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, J.F.; Blow, F.C.; Ignacio, R.V.; Ilgen, M.A.; Austin, K.L.; Valenstein, M. Suicide among patients in the Veterans Affairs Health System: Rural–Urban differences in rates, risks, and methods. Am. J. Public Health 2012, 102, S111–S117. [Google Scholar] [CrossRef] [PubMed]
- Park, E.; Lee, H.Y. Urban and rural differences in suicidal ideation and associated factors among older Koreans: Results from the Korean National Survey 2012–2013. Curr. Psychol. 2021, 1–10. [Google Scholar] [CrossRef]
- Ku, I.; Kim, C.-O. Decomposition analyses of the trend in poverty among older adults: The case of South Korea. J. Gerontol. Ser. B 2020, 75, 684–693. [Google Scholar] [CrossRef] [Green Version]
- OECD. Poverty Rate; Organisation for Economic Co-Operation and Development: Paris, France, 2022. [Google Scholar]
- WHO. World Health Statistics 2017: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2017.
- Lee, C.; Kang, S. Associated factors with the trajectory of local elderly suicide rate. Korean J. Gerontol. Soc. Welf. 2020, 75, 91–119. [Google Scholar]
- Jeong, K. A Study on the Typology of Local Governments by Variations in the Elderly Suicide Rates. Korean Assoc. Local Gov. Stud. 2019, 23, 111–134. [Google Scholar] [CrossRef]
- Okolie, C.; Dennis, M.; Thomas, E.S.; John, A. A systematic review of interventions to prevent suicidal behaviors and reduce suicidal ideation in older people. Int. Psychogeriatr. 2017, 29, 1801–1824. [Google Scholar] [CrossRef]
- RMJ. Status of National Action Plan for Suicide Prevention and Future Plan; Relevant Ministry Joint: Sejong-si, Republic of Korea, 2019. [Google Scholar]
- MoHW. 5 Years (2013~2017) National Suicide Death Analysis Results Report; MoHW: Sejong-si, Republic of Korea, 2021.
- Kaya, A.; Tasar, P.T.; Meral, O.; Sahın, S.; Balkay, M.; Aktas, E.O.; Akcıcek, F. The characteristics of older people suicides by sex and age subgroups. Leg. Med. 2020, 46, 101721. [Google Scholar] [CrossRef]
- Lee, H.-Y.; Hahm, M.-I.; Park, E.-C. Differential association of socio-economic status with gender-and age-defined suicidal ideation among adult and elderly individuals in South Korea. Psychiatry Res. 2013, 210, 323–328. [Google Scholar]
- Koh, E.H.; Song, S.M.; Huh, S.I.; Im, H.Y. The Effect of Economic Insecurity on Suicidal Thoughts in Middle-Aged and Older Adults with and without Disabilities. Health Soc. Welf. Rev. 2021, 41, 239–257. [Google Scholar] [CrossRef]
- Kwon, Y.; Byun, S. The Influence of the Participation in Elderly Job Project upon Job Satisfaction, Self-efficacy, Life Satisfaction. J. Humanit. Soc. Sci. 2022, 13, 689–704. [Google Scholar]
- Seoul Metropolitan City. ‘Seoul City’s Safety Income’ Government-Approved Project Design is Completed. Promotion in Cooperation with the City Council; press release; Seoul Metropolitan City: Seoul, Republic of Korea, 2019. [Google Scholar]
- Oh, C.-S. The effects of the elderly’s subjective health perceptions and quality of life on their depression and suicide ideation. Korean J. Health Serv. Manag. 2012, 6, 179–191. [Google Scholar] [CrossRef] [Green Version]
- Shon, C.; Seo, D.; Hwang, J. Factors influencing the community care satisfaction of the urban elderly focusing on the outreach community health service in Seoul. J. Korean Public Health Nurs. 2021, 35, 254–267. [Google Scholar]
- Jeong, K.; Ko, A. A study on the influencing factors of suicidal ideation of the young-old and old-old elderly in South Korea: Focusing on the individual, family, and community system factors. Korean J. Fam. Soc. Work 2016, 53, 45–78. [Google Scholar] [CrossRef]
- Kim, H.-S.; Kim, S.-H. Elderly’s Suicide Differentials and Their Factors: Focusing on 16 Metropolises and Provinces in Korea. J. Korea Contents Assoc. 2014, 14, 215–224. [Google Scholar] [CrossRef]
- Choi, S.M.; Hong, J.H. A Study on Factors Influencing the Elderly Suicide Rates in Urban and Rural Areas: Policy Design Focusing on the Difference Between Urban and Rural Areas. J. Gov. Stud. 2017, 23, 321–366. [Google Scholar] [CrossRef]
- Zimmerman, S.L. States’spending for public welfare and their suicide rates, 1960 to 1995: WHAT is the problem? J. Nerv. Ment. Dis. 2002, 190, 349–360. [Google Scholar] [CrossRef]
- Woo, H.J.; Lee, H.L. A Study on Operation Plan of Dementia Care Village in Nowon-gu; Nowon-gu District Office Research Team: Seoul, Republic of Korea, 2021. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Gender | Age | Region | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male (n = 252) | Female (n = 252) | Young–Old (n = 252) | Old–Old (n = 252) | Urban (n = 170) | Rural (n = 82) | |||||||
| M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | |
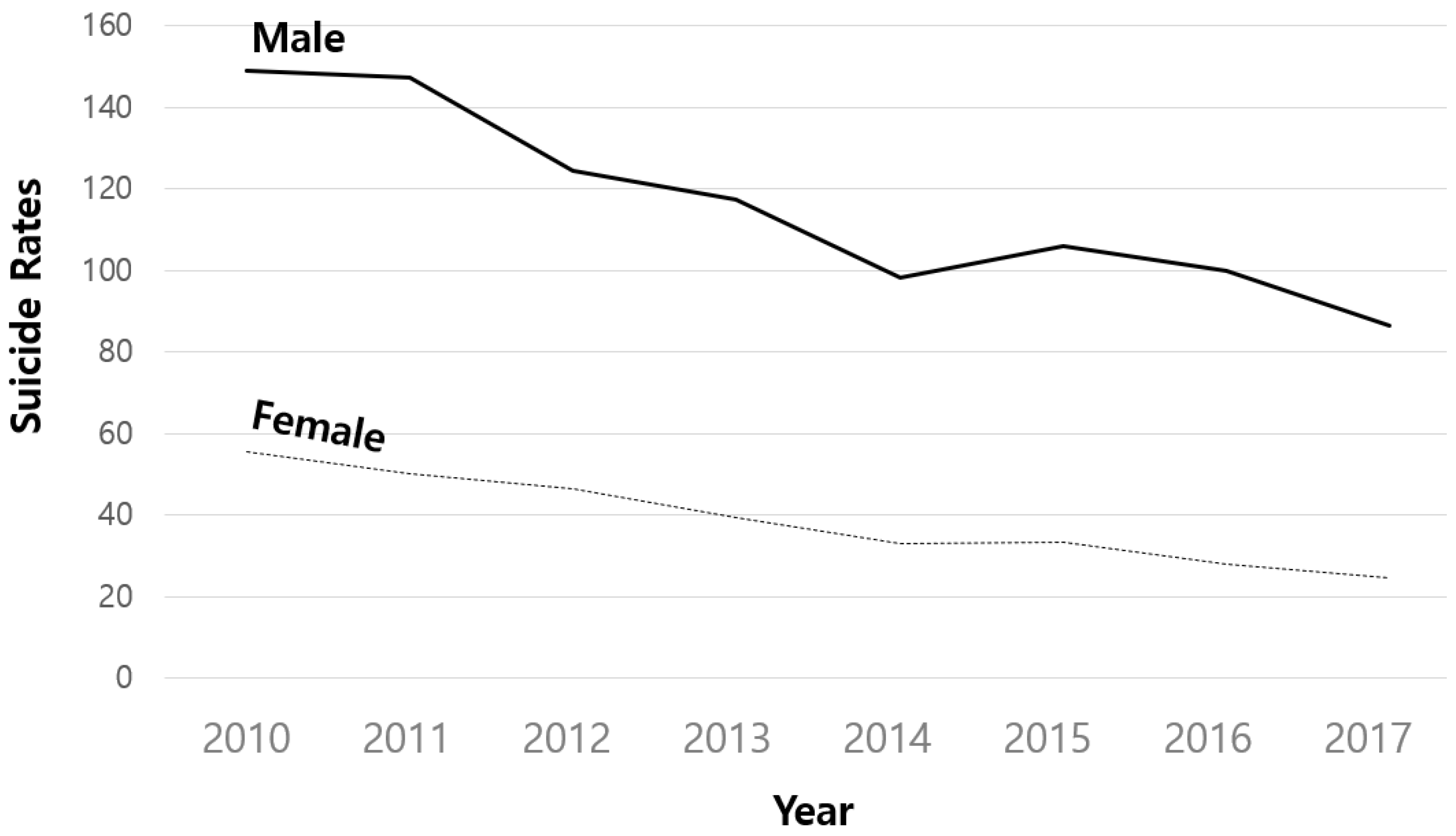
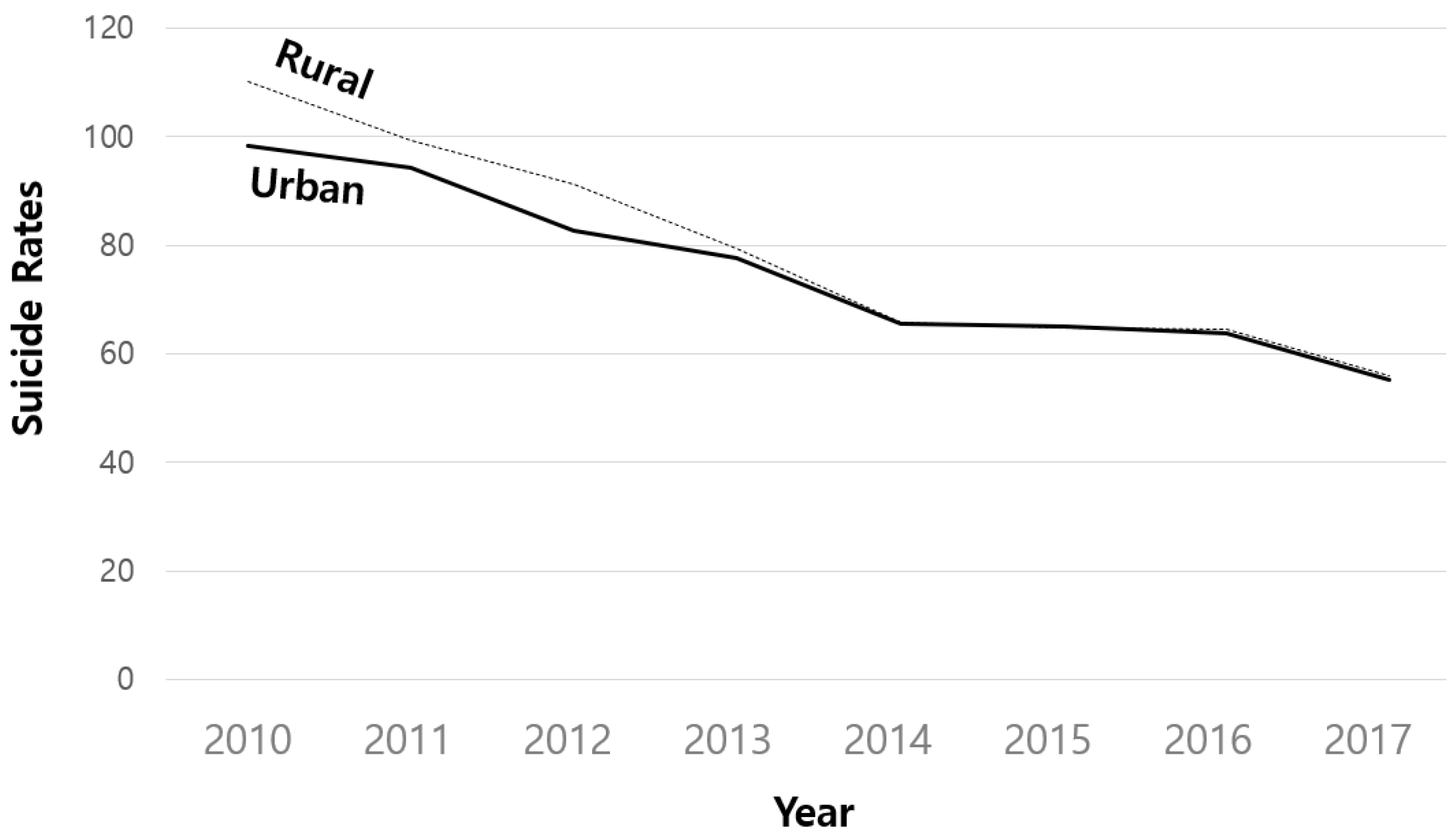
| 2010 | 148.99 | 99.90 | 55.38 | 46.79 | 73.81 | 62.94 | 130.56 | 104.81 | 98.32 | 78.99 | 110.17 | 111.35 |
| 2011 | 147.13 | 93.63 | 50.21 | 42.92 | 71.31 | 57.73 | 126.03 | 102.37 | 94.38 | 81.11 | 99.26 | 99.40 |
| 2012 | 124.49 | 84.33 | 46.45 | 38.86 | 61.49 | 50.70 | 109.45 | 89.16 | 82.68 | 67.17 | 91.23 | 92.30 |
| 2013 | 117.24 | 75.92 | 39.37 | 34.97 | 55.36 | 48.22 | 101.25 | 81.51 | 77.78 | 66.10 | 79.38 | 79.61 |
| 2014 | 98.11 | 65.15 | 33.12 | 29.55 | 47.49 | 41.63 | 83.74 | 69.58 | 65.48 | 56.49 | 65.89 | 67.09 |
| 2015 | 106.08 | 75.29 | 33.17 | 28.56 | 46.96 | 41.06 | 92.28 | 80.20 | 64.95 | 63.91 | 64.79 | 74.52 |
| 2016 | 99.94 | 68.60 | 28.08 | 24.05 | 43.37 | 38.50 | 84.65 | 74.40 | 63.71 | 57.61 | 64.64 | 72.22 |
| 2017 | 86.34 | 63.17 | 24.69 | 24.14 | 35.80 | 34.00 | 75.22 | 67.40 | 55.26 | 51.39 | 56.04 | 66.93 |
| Model | χ2 | df | CFI | TLI | RMSEA |
|---|---|---|---|---|---|
| No Growth Model | 824.012 *** | 34 | 0.763 | 0.805 | 0.152 |
| Linear Growth Model | 161.136 *** | 31 | 0.961 | 0.965 | 0.065 |
| Quadratic Growth Model | 123.947 *** | 27 | 0.971 | 0.970 | 0.060 |
| Variables | Mean | Variance | ||
|---|---|---|---|---|
| Estimate | S.E. | Estimate | S.E. | |
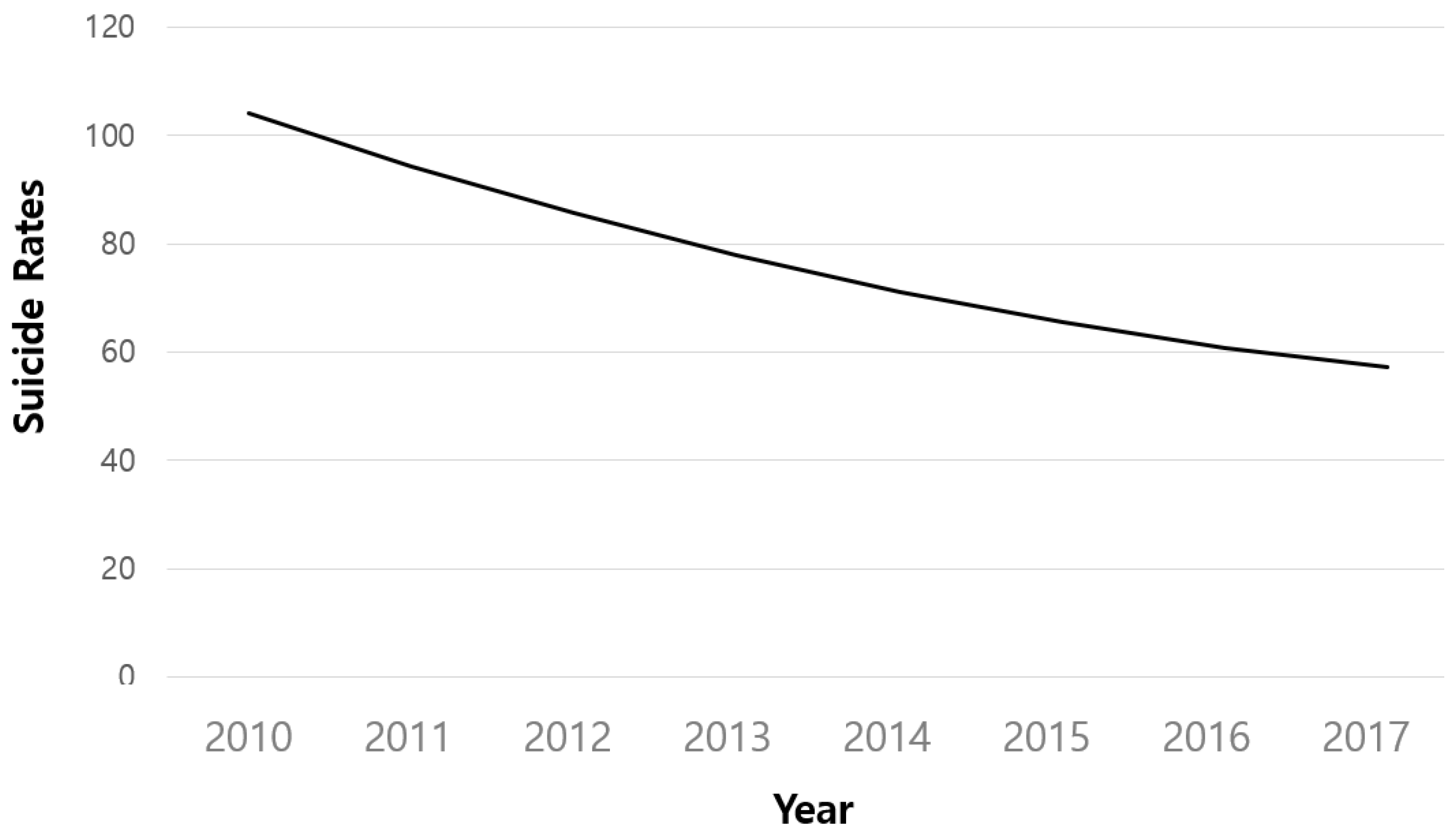
| Initial value | 104.232 *** | 2.667 | 4480.481 *** | 335.365 |
| Linear rate of change | −10.317 *** | 1.034 | 166.694 ** | 55.106 |
| Quadratic rate of change | 0.516 *** | 0.128 | 1.893 * | 0.855 |
| Path between Variables | Coef. | S.E. | ||
|---|---|---|---|---|
| Gender (ref. Male) | → | Initial value | −96.314 *** | 3.972 |
| Age (ref. Young old) | → | Initial value | 57.946 *** | 3.967 |
| Area (ref. Urban) | → | Initial value | 10.932 * | 4.231 |
| Gender (ref. Male) | → | Linear rate of change | 8.172 *** | 2.032 |
| Age (ref. Young old) | → | Linear rate of change | −6.002 ** | 2.029 |
| Area (ref. Urban) | → | Linear rate of change | −4.811 * | 2.162 |
| Gender (ref. Male) | → | Quadratic rate of change | −0.524 * | 0.254 |
| Age (ref. Young old) | → | Quadratic rate of change | 0.501 * | 0.253 |
| Area (ref. Urban) | → | Quadratic rate of change | 0.474 | 0.270 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, K.-H.; Yoon, J.-Y.; Lee, S.; Cho, S.; Woo, H.-J.; Kim, S. Changes in the Suicide Rate of Older Adults According to Gender, Age, and Region in South Korea from 2010 to 2017. Healthcare 2022, 10, 2333. https://doi.org/10.3390/healthcare10112333
Jeong K-H, Yoon J-Y, Lee S, Cho S, Woo H-J, Kim S. Changes in the Suicide Rate of Older Adults According to Gender, Age, and Region in South Korea from 2010 to 2017. Healthcare. 2022; 10(11):2333. https://doi.org/10.3390/healthcare10112333
Chicago/Turabian StyleJeong, Kyu-Hyoung, Ji-Yeon Yoon, Seoyoon Lee, Sunghwan Cho, Hyun-Jae Woo, and Sunghee Kim. 2022. "Changes in the Suicide Rate of Older Adults According to Gender, Age, and Region in South Korea from 2010 to 2017" Healthcare 10, no. 11: 2333. https://doi.org/10.3390/healthcare10112333