
Chronic Encapsulated Intracerebral Hematoma as an Occasional Finding in Sudden Cardiac Death

 ,
,  , , ,
, , ,  and
and 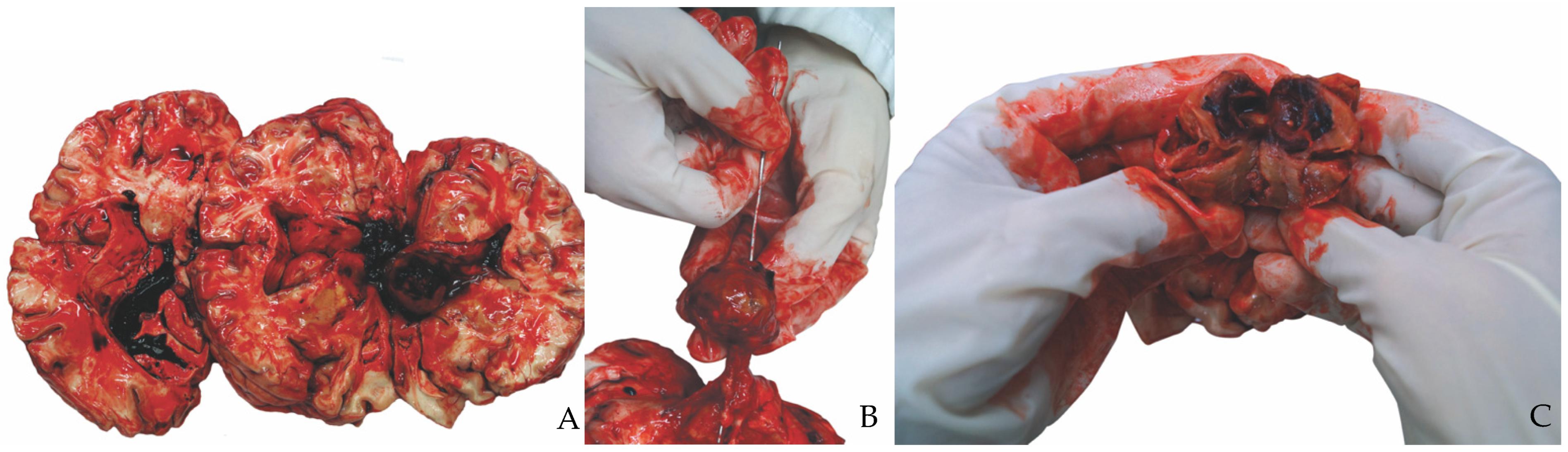{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
2.1. Autopsy Finding—Macroscopic Findings
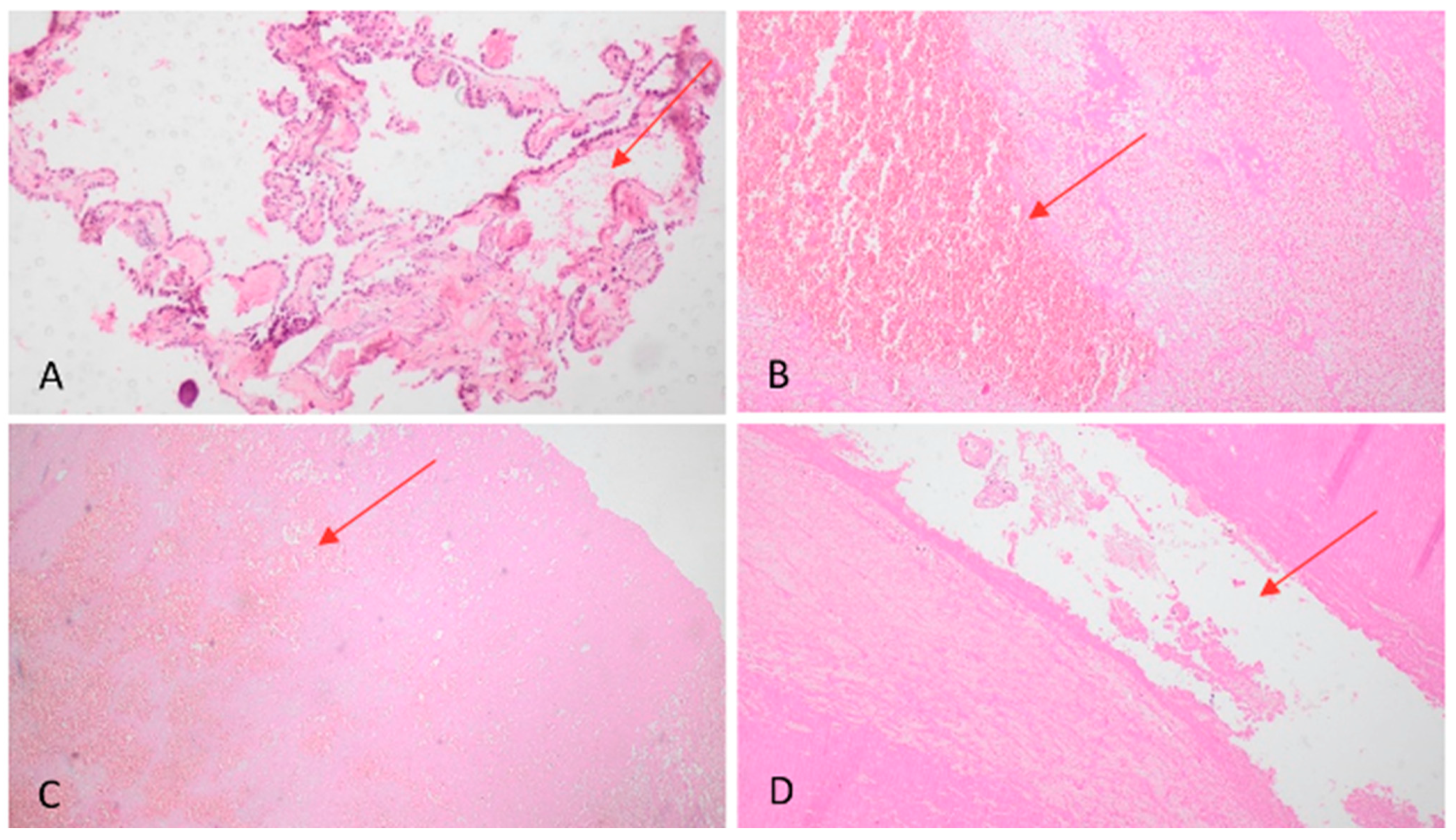
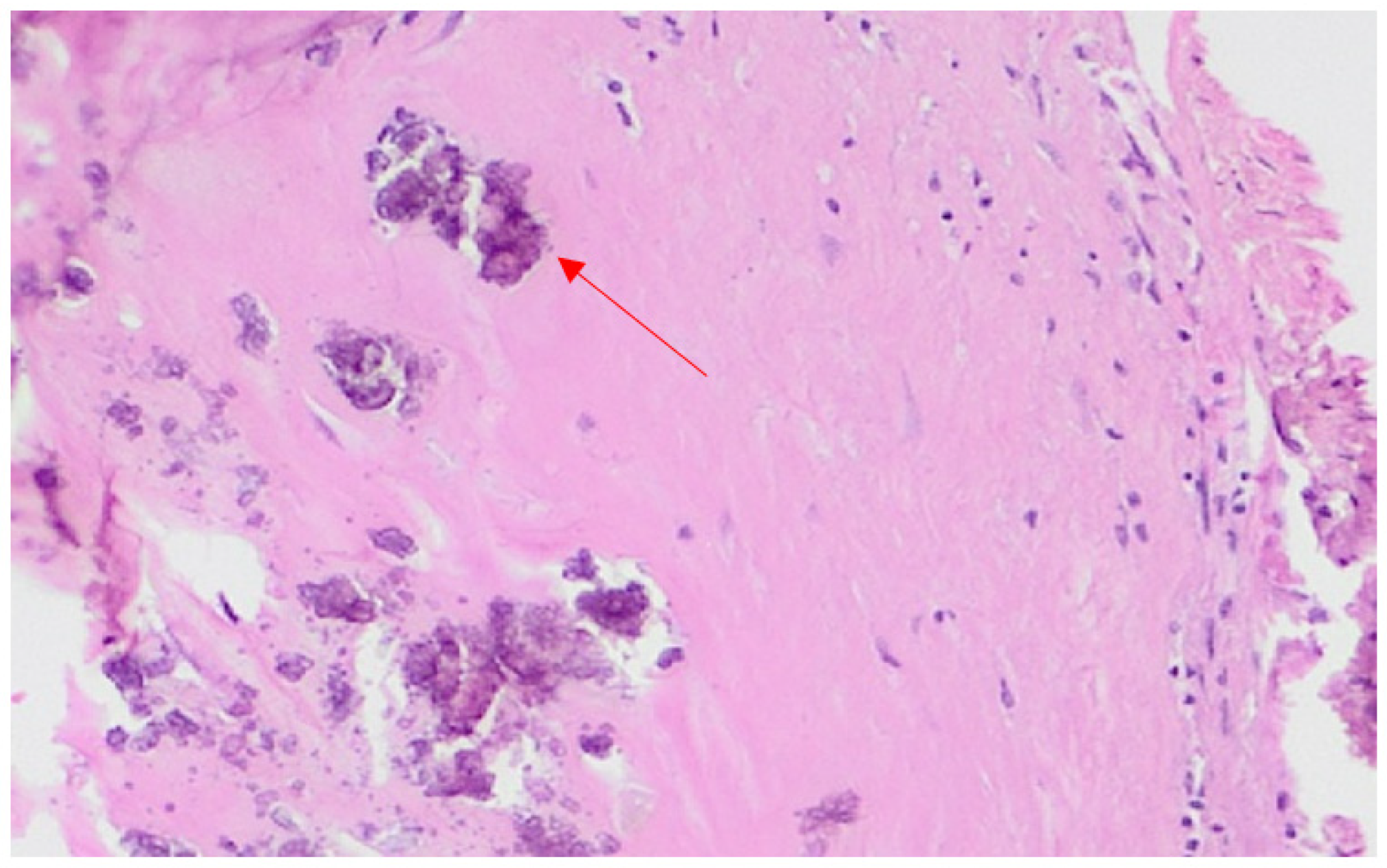
2.2. Microscopic Findings—Histology
2.3. Toxicological Analysis
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nishiyama, A.; Toi, H.; Takai, H. Chronic encapsulated intracerebral hematoma: Three case reports and a literature review. Surg. Neurol. Int. 2014, 5, 88. [Google Scholar]
- Sakaida, H.; Sakakura, M.; Tochio, H.; Nakao, K.; Taniguchi, A.; Yabana, T. Chronic encapsulated intracerebral hematoma associated with angiographically occult arteriovenous malformation—Case report. Neurol. Med. Chir. 1993, 33, 638–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finitsis, S.; Bernier, V.; Buccheit, I.; Klein, O.; Bracard, S.; Zhu, F.; Gauchotte, G.; Anxionnat, R. Late complications of radiosurgery for cerebral arteriovenous malformations: Report of 5 cases of chronic encapsulated intracerebral hematomas and review of the literature. Radiat. Oncol. 2020, 15, 177. [Google Scholar] [CrossRef]
- Takeuchi, S.; Takasato, Y.; Masaoka, H.; Hayakawa, T.; Otani, N.; Yoshino, Y.; Yatsushige, H.; Sugawara, T. Development of chronic encapsulated intracerebral hematoma after radiosurgery for a cerebral arteriovenous malformation. Acta Neurochir. 2009, 151, 1513–1515. [Google Scholar] [CrossRef]
- Takei, J.; Tanaka, T.; Yamamoto, Y.; Teshigawara, A.; Tochigi, S.; Hasegawa, Y.; Murayama, Y. Chronic Encapsulated Expanding Thalamic Hematoma Associated with Obstructive Hydrocephalus following Radiosurgery for a Cerebral Arteriovenous Malformation: A Case Report and Literature Review. Case Rep. Neurol. Med. 2016, 2016, 5130820. [Google Scholar] [CrossRef] [Green Version]
- Marutani, A.; Nagata, K.; Deguchi, J.; Nikaido, Y.; Kazuki, S. A Case of Recurrent Hemorrhages due to a Chronic Expanding Encapsulated Intracranial Hematoma. Case Rep. Neurol. 2015, 7, 173–180. [Google Scholar] [CrossRef]
- Roberti, F.; Bell, J. Septum Pellucidum Chronic Encapsulated Hematoma with Osseous Metaplasia Mimicking Recurrent Astrocytoma and Shunt-Related Foreign Body Granuloma. Cureus 2020, 12, e9839. [Google Scholar] [CrossRef]
- Kamide, T.; Seki, S.; Suzuki, K. A chronic encapsulated intracerebral hematoma mimicking a brain tumor: Findings on arterial spin labeling of MRI. Neuroradiol. J. 2016, 29, 273–276. [Google Scholar] [CrossRef] [PubMed]
- Cai, S.; Zhou, B.; Liao, H.; Tan, C. Imaging Diagnosis of Chronic Encapsulated Intracerebral Hematoma, a Comparison of Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) characteristics. Pol. J. Radiol. 2017, 82, 578–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, E.J.; Jasinski, J.M.; Tong, D.; Kado, K.; Richards, B.; Mccabe, R.W. Encapsulated Intracerebral Hematoma Presenting as Cerebral Abscess. Cureus 2021, 13, e15198. [Google Scholar] [CrossRef] [PubMed]
- Shibao, S.; Akiyama, T.; Yoshida, K.; Akiyama, T. Chronic Encapsulated Intracerebral Hematoma: Endoscopic Removal as Minimally Invasive Surgery for a Patient with Alcoholic Cirrhosis. NMC Case Rep. J. 2017, 4, 51–53. [Google Scholar] [CrossRef] [PubMed]
- Basso, C.; Aguilera, B.; Banner, J.; Cohle, S.; d’Amati, G.; de Gouveia, R.H.; di Gioia, C.; Fabre, A.; Gallagher, P.J.; Leone, O.; et al. Association for European Cardiovascular Pathology. Guidelines for autopsy investigation of sudden cardiac death: 2017 update from the Association for European Cardiovascular Pathology. Virchows Arch. 2017, 471, 691–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scalia, G.; Umana, G.E.; Crea, A.; Vats, A.; Chaurasia, B.; Graziano, F.; Marrone, S.; Furnari, M.; Ponzo, G.; Giuffrida, M.; et al. Chronic encapsulated intracerebral hematomas: A systematic review. Br. J. Neurosurg. 2022, 1–6. [Google Scholar] [CrossRef]
- Pozzati, E.; Giuliani, G.; Gaist, G.; Piazza, G.; Vergoni, G. Chronic expanding intracerebral hematoma. J. Neurosurg. 1986, 65, 611–614. [Google Scholar] [CrossRef]
- Hirsh, L.F.; Spector, H.B.; Bogdanoff, B.M. Chronic encapsulated intracerebral hematoma. Neurosurgery 1981, 9, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Park, J.C.; Ahn, J.S.; Kwon, D.H.; Kwun, B.D. Growing Organized Hematomas Following Gamma Knife Radiosurgery for Cerebral Arteriovenous Malformation: Five Cases of Surgical Excision. J. Korean Neurosurg. Soc. 2015, 58, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Roda, J.M.; Carceller, F.; Pérez-Higueras, A.; Morales, C. Encapsulated intracerebral hematomas: A defined entity. Case report. J. Neurosurg. 1993, 78, 829–833. [Google Scholar] [CrossRef] [PubMed]
- Dey, M.; Turner, M.S.; Pytel, P.; Awad, I.A. A “pseudo-cavernoma”—An encapsulated hematoma of the choroid plexus. J. Clin. Neurosci. 2011, 18, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Tomioka, A.; Takahashi, S.; Imai, R.; Nogawa, H.; Okita, H.; Ueno, A.; Toda, M. A Case of Bilateral Cerebellar Chronic Encapsulated Intracerebral Hematoma with Rapidly Progressive Symptoms. NMC Case Rep. J. 2022, 9, 111–116. [Google Scholar] [CrossRef]
- Wetzel, J.; Bray, D.; Wrubel, D. Chronic encapsulated intraventricular hematoma in a pediatric patient: Case report. J. Neurosurg. Pediatr. 2018, 22, 68–73. [Google Scholar] [CrossRef]
- Avol, M.; Vogel, P.J. Circumscribed intraventricular hematoma simulating an encapsulated neoplasm. Bull. Los Angel. Neurol. Soc. 1955, 20, 25–29. [Google Scholar]
- Lin, S.Z.; Shih, C.J.; Wang, Y.C.; Tsai, S.H. Intracerebral hematoma simulating a new growth. Surg. Neurol. 1984, 21, 459–464. [Google Scholar] [CrossRef]
- Ooba, H.; Kamida, T.; Isono, M.; Kobayashi, H.; Karashima, A.; Yamashita, M. Chronic intraventricular encapsulated hematoma presenting unique radiological features: A case report. Surg. Neurol. 2003, 59, 23–27. [Google Scholar] [CrossRef]
- Kechagias, E.; Ioakimidou, C.; Georgakoulias, N.; Seretis, A.; Kontogeorgos, G. Chronic Intraventricular Encapsulated Hematoma in an Adult: A Case Report. Case Rep. Neurol. 2010, 2, 118–121. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.C.; Pan, D.H.; Ho, D.M.; Wu, H.M.; Chung, W.Y.; Liu, K.D.; Guo, W.Y.; Shih, Y.H. Chronic encapsulated expanding hematoma after gamma knife stereotactic radiosurgery for cerebral arteriovenous malformation. Clin. Neurol. Neurosurg. 2011, 113, 668–671. [Google Scholar] [CrossRef] [PubMed]
- Nakamizo, A.; Suzuki, S.O.; Saito, N.; Shono, T.; Matsumoto, K.; Onaka, S.; Mizoguchi, M.; Sasaki, T. Clinicopathological study on chronic encapsulated expanding hematoma associated with incompletely obliterated AVM after stereotactic radiosurgery. Acta Neurochir. 2011, 153, 883–893. [Google Scholar] [CrossRef]
- Feola, A.; Ciamarra, P.; De Simone, M.; Carfora, A.; Mansueto, G.; Campobasso, C.P. Sudden Unexpected Death Caused by Cardiac Metastasization from Histiocytic Sarcoma. Int. J. Environ. Res. Public Health 2021, 18, 12911. [Google Scholar] [CrossRef] [PubMed]
- Greiner-Perth, R.; Neubauer, U.; Schenke, H. Chronic encapsulated intracerebral hematoma--a well-defined disease. Report on two cases and review of the literature. Neurosurg. Rev. 1997, 20, 231–238. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feola, A.; De Simone, M.; Ciamarra, P.; Sica, S.; Buonomo, C.; Carfora, A.; Campobasso, C.P. Chronic Encapsulated Intracerebral Hematoma as an Occasional Finding in Sudden Cardiac Death. Healthcare 2022, 10, 2053. https://doi.org/10.3390/healthcare10102053
Feola A, De Simone M, Ciamarra P, Sica S, Buonomo C, Carfora A, Campobasso CP. Chronic Encapsulated Intracerebral Hematoma as an Occasional Finding in Sudden Cardiac Death. Healthcare. 2022; 10(10):2053. https://doi.org/10.3390/healthcare10102053
Chicago/Turabian StyleFeola, Alessandro, Mariavictoria De Simone, Paola Ciamarra, Stefania Sica, Carmela Buonomo, Anna Carfora, and Carlo Pietro Campobasso. 2022. "Chronic Encapsulated Intracerebral Hematoma as an Occasional Finding in Sudden Cardiac Death" Healthcare 10, no. 10: 2053. https://doi.org/10.3390/healthcare10102053