
Effect of Acupuncture on Functional Capacity and Health-Related Quality of Life of Hemodialysis Patients: Study Protocol for a Randomized Controlled Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Recruitment
2.3. Eligibility Criteria
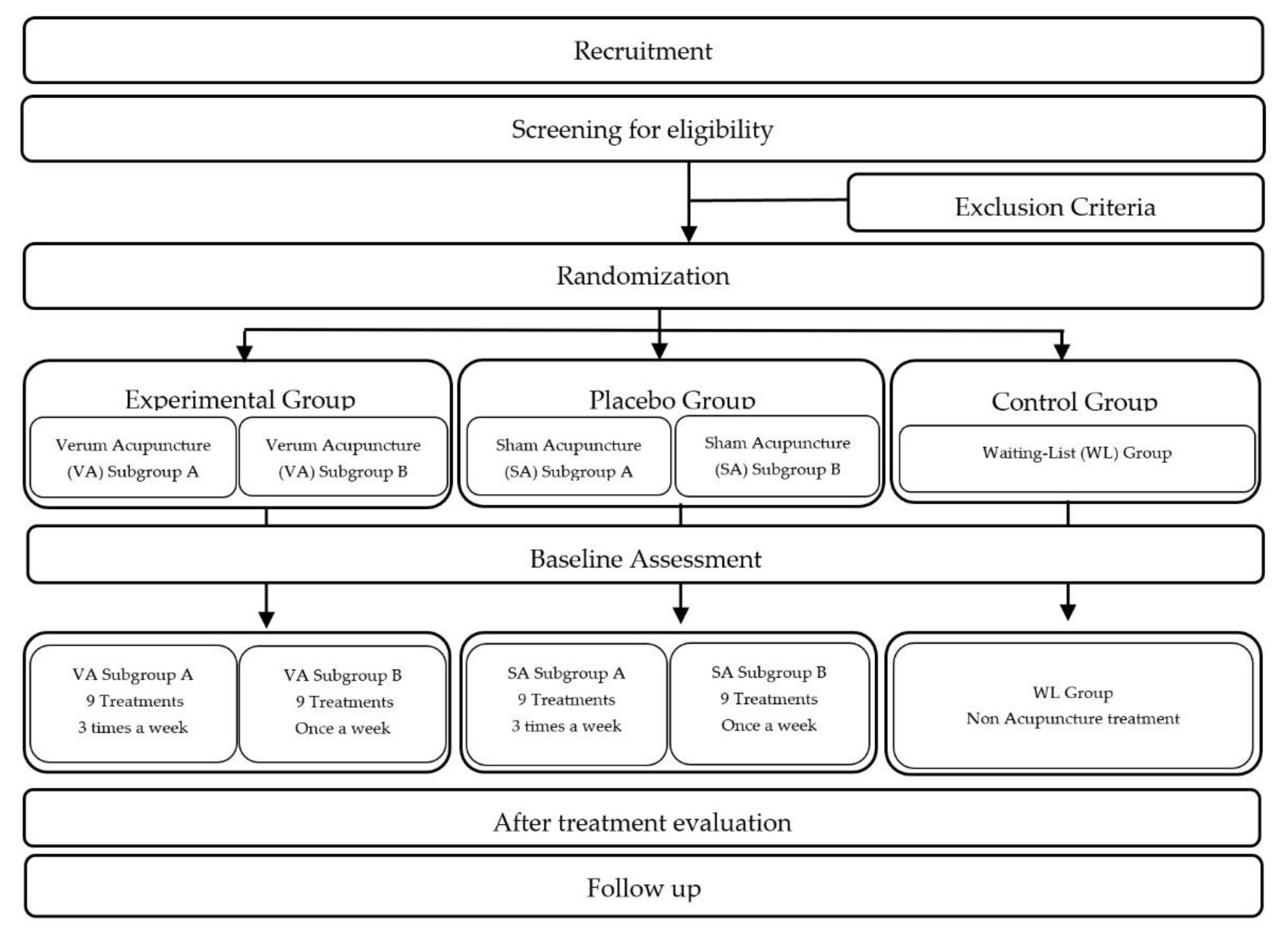
2.4. Randomization and Allocation
2.5. Blinding
2.6. Intervention
3. Outcome Measurement
3.1. Primary Outcome
3.2. Secondary Outcomes
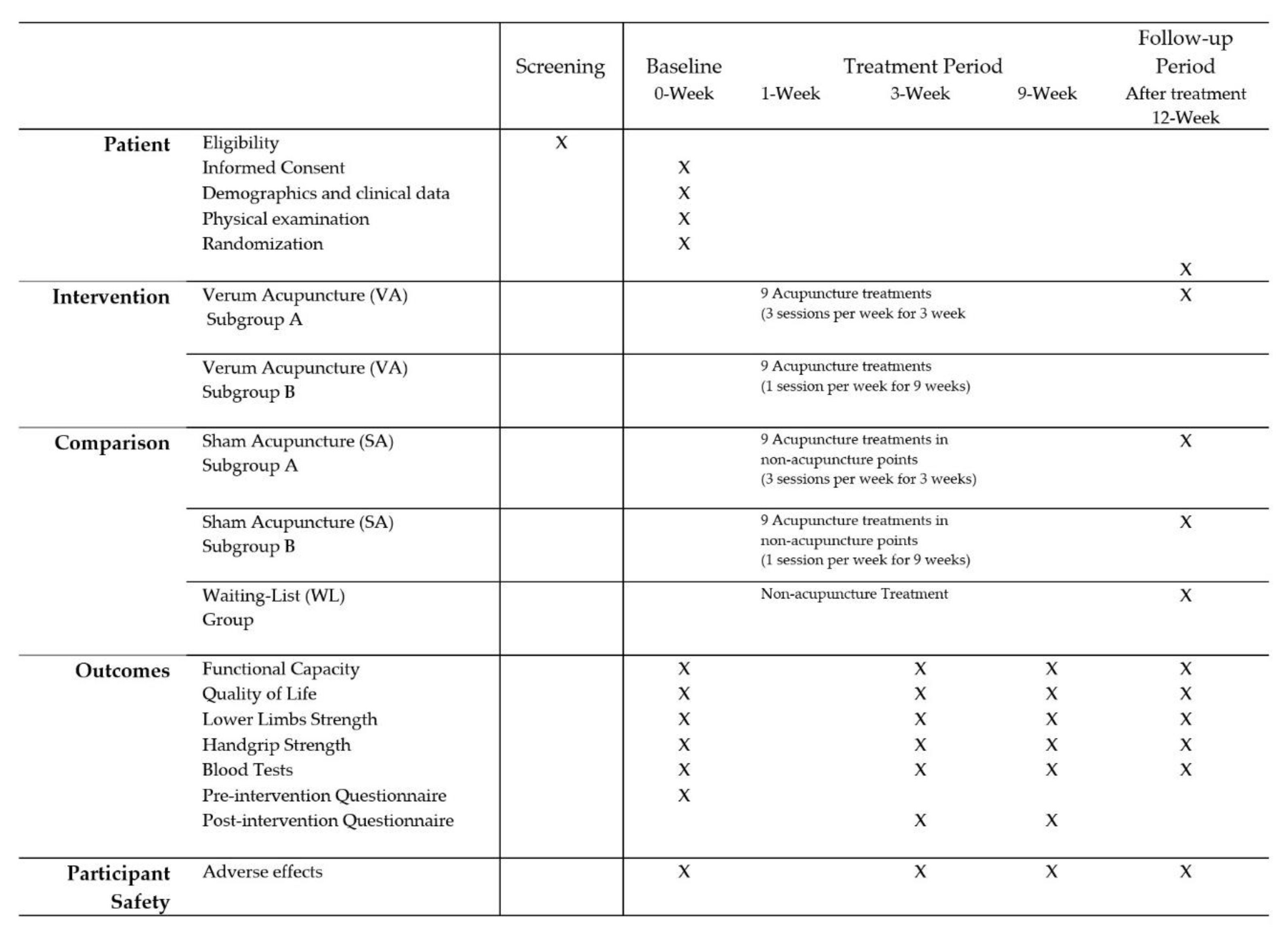
3.3. Participant Timeline
3.4. Statistical Analysis and Sample size
3.5. Adverse Events Assessment
3.6. Quality Control and Data Collection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Global Status Report on Noncommunicable Diseases 2014; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Foundation, N.K. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- Wang, V.; Vilme, H.; Maciejewski, M.L.; Boulware, L.E. The economic burden of chronic kidney disease and end-stage renal disease. Semin. Nephrol. 2016, 36, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar] [CrossRef] [Green Version]
- de Boer, I.H.; Caramori, M.L.; Chan, J.C.; Heerspink, H.J.; Hurst, C.; Khunti, K.; Liew, A.; Michos, E.D.; Navaneethan, S.D.; Olowu, W.A.; et al. KDIGO 2020 clinical practice guideline for diabetes management in chronic kidney disease. Kidney Int. 2020, 98, S1–S115. [Google Scholar] [CrossRef] [PubMed]
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.; Yang, C.W. Chronic kidney disease: Global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Liew, A. Perspectives in renal replacement therapy: Haemodialysis. Nephrology 2018, 23 (Suppl. 4), 95–99. [Google Scholar] [CrossRef] [Green Version]
- Golshayan, D.; Pascual, M. Burden of end-stage renal disease and evolving challenges in kidney transplantation. Transpl. Int. 2019, 32, 889–891. [Google Scholar] [CrossRef]
- Kittiskulnam, P.; Sheshadri, A.; Johansen, K.L. Consequences of CKD on functioning. Semin. Nephrol. 2016, 36, 305–318. [Google Scholar] [CrossRef] [Green Version]
- Goh, Z.S.; Griva, K. Anxiety and depression in patients with end-stage renal disease: Impact and management challenges—A narrative review. Int. J. Nephrol. Renovasc. Dis. 2018, 11, 93–102. [Google Scholar] [CrossRef] [Green Version]
- Painter, P. Physical functioning in end-stage renal disease patients: Update 2005. Hemodial. Int. 2005, 9, 218–235. [Google Scholar] [CrossRef]
- Napadow, V.; Ahn, A.; Longhurst, J.; Lao, L.; Stener-Victorin, E.; Harris, R.; Langevin, H.M. The status and future of acupuncture mechanism research. J. Altern. Complement. Med. 2008, 14, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Ifrim Chen, F.; Antochi, A.D.; Barbilian, A.G. Acupuncture and the retrospect of its modern research. Rom. J. Morphol. Embryol. 2019, 60, 411–418. [Google Scholar]
- Paterno, J.C.; Freire, A.O.; Soares, M.F.; Franco, M.F.; Schor, N.; Teixeira, V.P. Electroacupuncture and moxibustion attenuate the progression of renal disease in 5/6 nephrectomized rats. Kidney Blood Press. Res. 2008, 31, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Kim, T.H.; Kang, J.W.; Sul, J.U.; Lee, M.S.; Kim, J.I.; Shin, M.S.; Jung, S.Y.; Kim, A.R.; Kang, K.W.; et al. Acupuncture for symptom management in hemodialysis patients: A prospective, observational pilot study. J. Altern. Complement. Med. 2011, 17, 741–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bullen, A.; Awdishu, L.; Lester, W.; Moore, T.; Trzebinska, D. Effect of acupuncture or massage on health-related quality of life of hemodialysis patients. J. Altern. Complement. Med. 2018, 24, 1069–1075. [Google Scholar] [CrossRef]
- Yu, J.S.; Ho, C.H.; Wang, H.Y.; Chen, Y.H.; Hsieh, C.L. Acupuncture on renal function in patients with chronic kidney disease: A single-blinded, randomized, preliminary controlled study. J. Altern. Complement. Med. 2017, 23, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Garcia, G.E.; Ma, S.X.; Feng, L. Acupuncture and kidney disease. Adv. Chronic. Kidney Dis. 2005, 12, 282–291. [Google Scholar] [CrossRef]
- Kim, K.H.; Lee, M.S.; Kim, T.H.; Kang, J.W.; Choi, T.Y.; Lee, J.D. Acupuncture and related interventions for symptoms of chronic kidney disease. Cochrane Database Syst. Rev. 2016, 346, Cd009440. [Google Scholar] [CrossRef]
- Chan, A.W.; Tetzlaff, J.M.; Gøtzsche, P.C.; Altman, D.G.; Mann, H.; Berlin, J.A.; Dickersin, K.; Hróbjartsson, A.; Schulz, K.F.; Parulekar, W.R.; et al. SPIRIT 2013 explanation and elaboration: Guidance for protocols of clinical trials. BMJ 2013, 346, e7586. [Google Scholar] [CrossRef] [Green Version]
- James, K.E.; Bloch, D.A.; Lee, K.K.; Kraemer, H.C.; Fuller, R.K. An index for assessing blindness in a multi-centre clinical trial: Disulfiram for alcohol cessation–A VA cooperative study. Stat. Med. 1996, 15, 1421–1434. [Google Scholar] [CrossRef]
- Kolahi, J.; Bang, H.; Park, J. Towards a proposal for assessment of blinding success in clinical trials: Up-to-date review. Community Dent. Oral Epidemiol. 2009, 37, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Lim, S. WHO standard acupuncture point locations. Evid. Based Complement. Altern. Med. 2010, 7, 167–168. [Google Scholar] [CrossRef] [PubMed]
- MacPherson, H.; Altman, D.G.; Hammerschlag, R.; Youping, L.; Taixiang, W.; White, A.; Moher, D. Revised standards for reporting interventions in clinical trials of acupuncture (STRICTA): Extending the CONSORT statement. PLoS Med. 2010, 7, e1000261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maciocia, G. The Foundations of Chinese Medicine. A Comprehensive Text; Elsevier Health Sciences: Mumbai, India, 2015. [Google Scholar]
- Li, W.; Frierman, D. Clinical Nephrology in Chinese Medicine; Blue Poppy Press: Boulder, CO, USA, 2003. [Google Scholar]
- Matos, L.C.; Machado, J.P.; Monteiro, F.J.; Greten, H.J. Understanding traditional chinese medicine therapeutics: An overview of the basics and clinical applications. Healthcare 2021, 9, 257. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. American Thoracic Society. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Hays, R.D.; Kallich, J.; Mapes, D.; Coons, S.; Amin, N.; Carter, W.B.; Kamberg, C. Kidney Disease Quality of Life Short Form (KDQOL-SF &trade); Version 1.3: A Manual for Use and Scoring; RAND Corporation: Santa Monica, CA, USA, 1997. [Google Scholar]
- Bobos, P.; Nazari, G.; Lu, Z.; MacDermid, J.C. Measurement properties of the hand grip strength assessment: A systematic review with meta-analysis. Arch. Phys. Med. Rehabil. 2020, 101, 553–565. [Google Scholar] [CrossRef]
- Bohannon, R.W. Test-retest reliability of measurements of hand-grip strength obtained by dynamometry from older adults: A systematic review of research in the PubMed database. J. Frailty Aging 2017, 6, 83–87. [Google Scholar] [CrossRef]
- Figueiredo, P.H.S.; Veloso, L.R.S.; Lima, M.M.O.; Vieira, C.F.D.; Alves, F.L.; Lacerda, A.C.R.; Lima, V.P.; Rodrigues, V.G.B.; Maciel, E.H.B.; Costa, H.S. The reliability and validity of the 30-seconds sit-to-stand test and its capacity for assessment of the functional status of hemodialysis patients. J. Bodyw. Mov. Ther. 2021, 27, 157–164. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows; Version 27.0; IBM Corp.: Armonk, NY, USA, 2018. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Benjamin, O.; Lappin, S.L. End-Stage Renal Disease. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2021. [Google Scholar]
- Cabrera, V.J.; Hansson, J.; Kliger, A.S.; Finkelstein, F.O. Symptom management of the patient with CKD: The role of dialysis. Clin. J. Am. Soc. Nephrol. 2017, 12, 687–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.Y.; Kim, B.; Park, K.S.; Choi, J.Y.; Seo, J.J.; Park, S.H.; Kim, C.D.; Kim, Y.L. Health-related quality of life with KDQOL-36 and its association with self-efficacy and treatment satisfaction in korean dialysis patients. Qual. Life Res. 2013, 22, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Zazzeroni, L.; Pasquinelli, G.; Nanni, E.; Cremonini, V.; Rubbi, I. Comparison of Quality of Life in Patients Undergoing hemodialysis and peritoneal dialysis: A systematic review and meta-analysis. Kidney Blood Press. Res. 2017, 42, 717–727. [Google Scholar] [CrossRef]
- Garcia, R.S.A.; Lucinda, L.M.F.; Ramos, F.A.; Bueno, G.S.; de Oliveira, G.M.R.; Bonisson, L.S.; Silva, M.A.; Zolli, T.I.; Pinheiro, B.V.; Paula, R.B.; et al. Factors associated with functional capacity in hemodialysis patients. Artif. Organs 2017, 41, 1121–1126. [Google Scholar] [CrossRef]
- Johansen, K.L.; Shubert, T.; Doyle, J.; Soher, B.; Sakkas, G.K.; Kent-Braun, J.A. Muscle atrophy in patients receiving hemodialysis: Effects on muscle strength, muscle quality, and physical function. Kidney Int. 2003, 63, 291–297. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Wahner-Roedler, D.L.; Zhou, X.; Johnson, L.A.; Do, A.; Pachman, D.R.; Chon, T.Y.; Salinas, M.; Millstine, D.; Bauer, B.A. Acupuncture for palliative cancer pain management: Systematic review. BMJ Support. Palliat. Care 2021, 11, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Hou, Y.Q.; Yang, J.W.; Wang, L.Q.; Shao, J.K.; Zou, X.; Yang, N.N.; Huang, J.; Liu, C.Z. Acupuncture of different treatment frequency in postprandial distress syndrome: A pilot randomized clinical trial. Neurogastroenterol. Motil. 2020, 32, e13812. [Google Scholar] [CrossRef]
- Lin, L.L.; Tu, J.F.; Wang, L.Q.; Yang, J.W.; Shi, G.X.; Li, J.L.; Zhang, N.; Shao, J.K.; Zou, X.; Liu, C.Z. Acupuncture of different treatment frequencies in knee osteoarthritis: A pilot randomised controlled trial. Pain 2020, 161, 2532–2538. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Item | Detail | |
|---|---|---|
| 1. Acupuncture Rationale | (1a) Style of acupuncture | Manual acupuncture. |
| (1b) Reasoning for treatment provided, based on historical context, literature sources, and/or consensus methods, with references where appropriate. | The protocol treatment provided is based on traditional meridian theory, literature sources, clinical experience and consensus method of experts in Traditional Chinese Medicine, Acupuncture and Nephrology [25,26,27], members of research team. | |
| (1c) Extent to which treatment was varied | Experimental (verum acupuncture) group will receive a total of 9 acupuncture treatments, however, will be divided into subgroups A and B. Experimental subgroup A will receive three acupuncture sessions per week over 3 weeks and subgroup B will receive one a week for 9 weeks. The same choice of acupuncture points will be applied to both experimental subgroups A and B. | |
| 2. Details of Needling | (2a) Number of needle insertions per subject per session | A total of 5 fixed acupoints and a total of 8 needle insertions per subject and per session. |
| (2b) Names of points used | Taixi (KI3), bilateral; Sanyinjiao (SP6), bilateral; Zusanli (ST36), bilateral; Shenmen (HT7) unilateral, in the arm without arteriovenous fistula; Guanyuan (CV4), unilateral. Acupuncture points will be found according to the WHO points location method. | |
| (2c) Depth of insertion, based on a specified unit of measurement, or on a particular tissue level | After local area disinfection with alcohol wipes, acupoints CV4, ST36, KI3 and SP6 will be inserted perpendicularly (15 to 20 mm depth) and HT7 inserted slightly obliquely (10 mm depth). | |
| (2d) Response sought | De qi sensation (described as a compositional sensation including numbness, soreness, distention, heaviness) will be achieved through lifting, thrusting and twirling manipulations. | |
| (2e) Needle stimulation | Manual stimulation. After generating a needling sensation, needles will be manipulated for one minute every ten minutes during needle retention. | |
| (2f) Needle retention time | 25 min. | |
| (2g) Needle type | Sterilized stainless-steel needle (0.25 × 25 mm) Tewa, asia-med GmbH, Kirchplatz 1, 82049 Pullach, Germany. | |
| 3. Treatment Regimen | (3a) Number of treatment sessions | A total of 9 treatment sessions for both groups. |
| (3b) Frequency and duration of treatment sessions | Verum Acupuncture Subgroup A: three times a week for 3 weeks. Verum Acupuncture Subgroup B: once a week for 9 weeks. | |
| 4. Other Components of Treatment | (4a) Details of other interventions administered to the acupuncture group | Apart from the usual care routine for hemodialysis sessions, during the study period, no further intervention will be allowed. |
| (4b) Setting and context of treatment, including instructions to practitioners, and information and explanations to patients | Treatment sessions will take place at the Hemodialysis Center of TECSAM Tecnologia e Serviços Médicos, SA, in Mirandela, during hemodialysis sessions. Participants will be informed about the entire procedure and a clarification meeting will also be held with the hemodialysis clinical team before treatments starts. | |
| 5. Practitioner Background | (5) Description of participating acupuncturists | M.C.d.C is a licensed specialist in Traditional Chinese Medicine with professional card number C-006513 issued by the Regulator of Health System Central Administration in Portugal, ACSS (Administração Central do Sistema de Saúde, I.P.); five years of professional experience; a Traditional Chinese Medicine Master’s degree from Instituto de Ciências Biomédicas Abel Salazar, Universidade do Porto, Portugal; completion of Advanced Chinese Medicine Course from Guangzhou University of Chinese Medicine, Guangzhou, P.R. China. |
| 6. Control or Comparator Interventions | (6a) Rationale for the control or comparator in the context of the research question, with sources that justify this choice | Participants will randomly be assigned to experimental group (verum acupuncture), placebo group (sham acupuncture) or control group (waiting list). |
| (6b) Precise description of the control or comparator. If sham acupuncture or any other type of acupuncture-like control is used, provide details as for Items 1 to 3 above. | The placebo group (sham acupuncture) will receive a total of 9 acupuncture treatments, however, will be divided into subgroups A and B. Placebo subgroup A will receive three acupuncture sessions per week over 3 weeks and subgroup B will receive one a week for 9 weeks. Manual acupuncture will be performed as superficial needling (5 mm depth) at non-acupuncture points without an attempt to achieve a De qi sensation and without stimulation, lasting 25 min, using a sterilized stainless-steel needle (0.25 × 25 mm; Tewa, asia-med GmbH, Kirchplatz 1, 82049 Pullach, Germany).The control group (waiting list) will not receive any acupuncture treatment during the study period. List of Non-Acupuncture points used and their location In the present study, the non-acupuncture points selected will be the points located on the non-meridian but near the acupuncture points described above.
On the posteromedial aspect of the ankle, at the midpoint of KI3 (Taixi) and (Fuliu). KI7 (Fuliu) is located on the posteromedial aspect of the leg, anterior to the calcaneal tendon, 2 cun superior to the prominence of the medial malleolus.
On the leg, at the midpoint of the medial side of the tibia, 1 cun distal from SP6 (Sanyinjiao).
On the anterior aspect of the leg, at midpoint of ST37 (Shangjuxu) and the Gallbladder Meridian. ST37 (Shangjuxu) is located on the anterior aspect of the leg, on the line connecting ST35 with ST41, 6 cun inferior to ST35, on the tibialis anterior muscle.
On the wrist, at the transverse crease of the wrist, at the midpoint of HT7 (Shenmen) and PC7 (Daling), between the Pericardium Meridian and the Heart Meridian.
On the lower abdomen, 1 cun lateral from CV6 (Qihai). CV6 (Qihai) is located 1.5 cun inferior to the center of the umbilicus, on the anterior median line. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Correia de Carvalho, M.; Pereira Machado, J.; Laranjeira, M.; Nunes de Azevedo, J.; Azevedo, P. Effect of Acupuncture on Functional Capacity and Health-Related Quality of Life of Hemodialysis Patients: Study Protocol for a Randomized Controlled Trial. Healthcare 2022, 10, 2050. https://doi.org/10.3390/healthcare10102050
Correia de Carvalho M, Pereira Machado J, Laranjeira M, Nunes de Azevedo J, Azevedo P. Effect of Acupuncture on Functional Capacity and Health-Related Quality of Life of Hemodialysis Patients: Study Protocol for a Randomized Controlled Trial. Healthcare. 2022; 10(10):2050. https://doi.org/10.3390/healthcare10102050
Chicago/Turabian StyleCorreia de Carvalho, Marta, Jorge Pereira Machado, Manuel Laranjeira, José Nunes de Azevedo, and Pedro Azevedo. 2022. "Effect of Acupuncture on Functional Capacity and Health-Related Quality of Life of Hemodialysis Patients: Study Protocol for a Randomized Controlled Trial" Healthcare 10, no. 10: 2050. https://doi.org/10.3390/healthcare10102050