
Acupuncture in Women with Human Polycystic Ovary/Ovarian Syndrome: Protocol for a Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
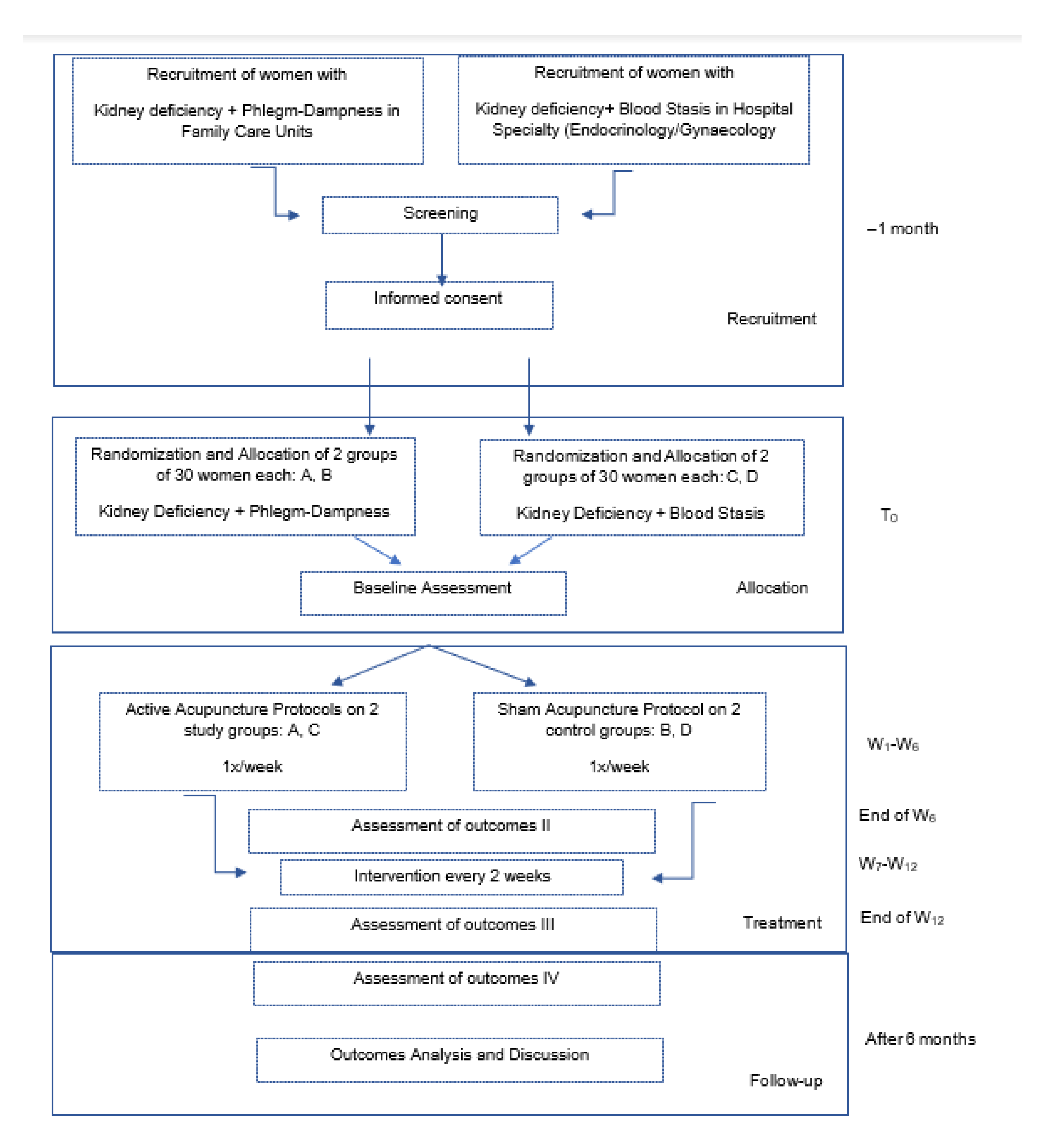
2.1. Study Design
2.2. Recruitment, Participants, and Randomization
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Intervention
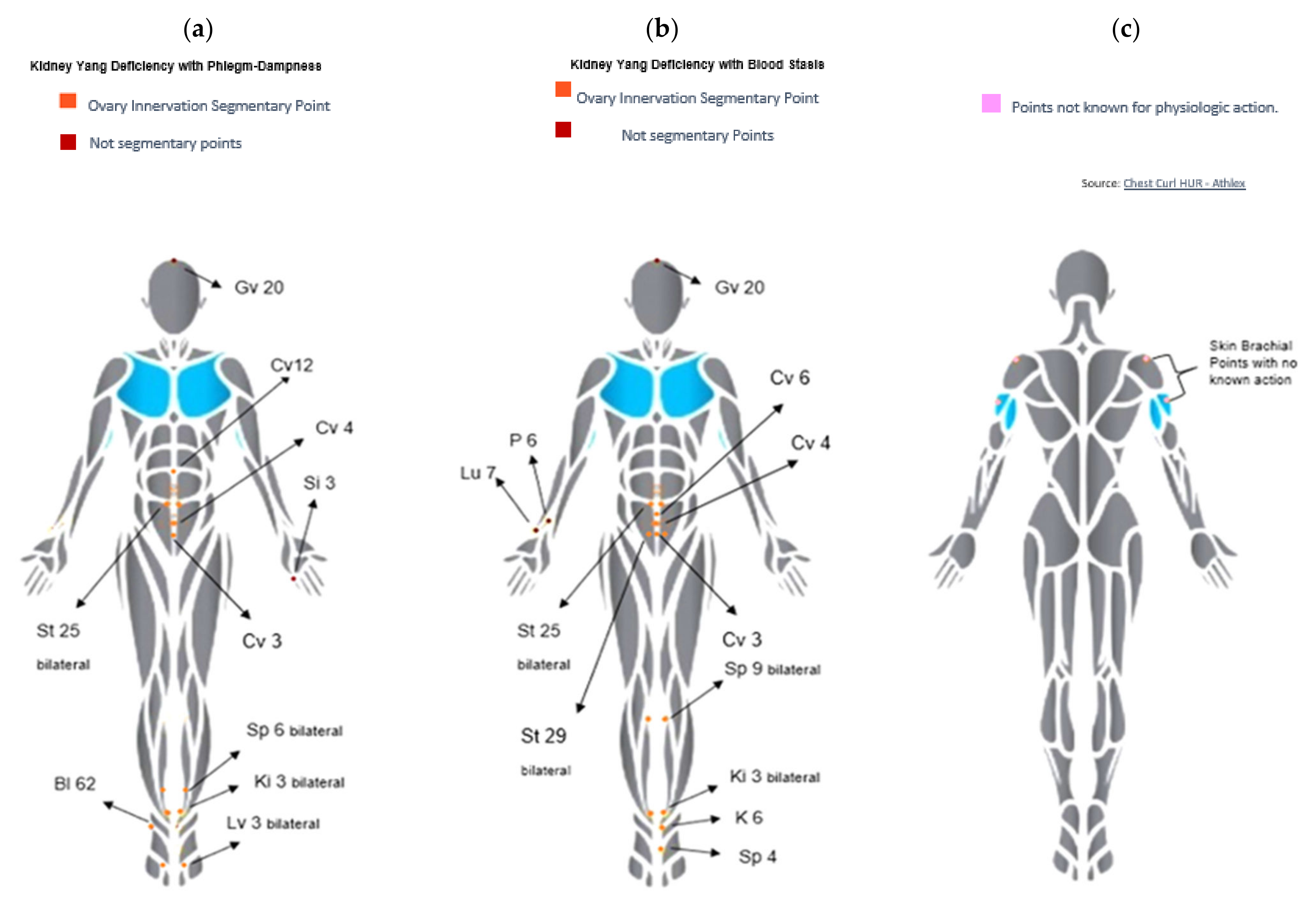
2.5.1. Active Acupuncture
2.5.2. Sham Acupuncture
3. Results
3.1. Blinded
3.2. Adverse Events/Serious Reactions
3.3. Data Collection and Statistical Analysis
3.4. Ethics and Dissemination
4. Discussion
4.1. Limitation of Previous Trials
4.2. Proposed Trial
4.3. What We Expect with the Trial
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Active Acupuncture | |||
|---|---|---|---|
| Group I–Kidney Yang Deficiency with Phlegm-Dampness | |||
| Acupoint | Location | Muscle Innervation | TCM Action |
| REN-3 (Zhōngjí) | 4 cun below the umbilicus on the mid-line | L1 | Resolve dampness on genital system |
| REN-4 (Gǔangyúan) | On the midline, 3 cun inferior to the umbilicus | Th12 | Tonify kidney yang |
| Ren-12 (Zhōngwăn) | 4 cun above centre of umbilicus | Th7-Th8 | Harmonize and strengthen stomach, spleen and the Middle Jiao vessels; Fortify Shen |
| Bilateral SP-6 (Sānyīnjiāo) | On the medial aspect of the lower leg, 3 cun above the medial malleolus, on the posterior border of the medial aspect of the tibia. | L4-L5; S1-S2 | Resolve dampness |
| Bilateral ST-25 (Tiānshū) | 2 cun lateral to center of umbilicus | Th6-Th12 | Remove Qi and blood stasis; harmonize spleen and stomach; resolve damp and damp-heat |
| Bilateral LIV-3 (Tàichōng) | Just distal to the junction of the bases of the 1st and 2nd metatarsals | S2-S3 | Resolve damp-heat in the lower burner; sooth the liver; direct Qi in the connecting vessels and quicken the blood. |
| Bilateral KID-3 (Tàixī) | In the depression between the medial malleolus and the Achilles tendon, level with the tip of the medial malleolus | L4 | Tonify kidney Yang |
| DU-20 (Bàihuì) | On the midline of the head, 7 cun directly above the posterior hairline, approximately on the midpoint of the line connecting the apexes of the two auricles. | C2-C3; Trigeminus nerve | Clears the mind, lifts the spirits, tonifies Yang, strengthens the ascending function of the spleen, eliminates interior wind |
| Right BL-62 (Shēnmài) coupled to Left SI-3 (Hòuxī) | Bl 62: On the lateral side of the foot, approximately 0.5 cun inferior to the inferior border of the lateral malleolus, in a depression posterior to the peroneal tendons. Si3: On the ulnar border of the hand, in the substantial depression proximal to the head of the fifth metacarpal bone. | S1 coupled to C8 | Clears the spirit-disposition; dispels interior heat; frees the governing vessel |
| Group II–Kidney Yang Deficiency with Blood Stasis | |||
| REN-3 (Zhōngjí) | 4 cun below the umbilicus on the mid-line | L1 | Resolve dampness on genital system |
| REN-4 (Gǔangyúan) | On the midline, 3 cun inferior to the umbilicus | Th12 | Tonify kidney Yang |
| REN-6 (Qìhăi) | 4 cun above centre of umbilicus | Th7-Th8 | Harmonize and strengthen stomach, spleen and the Middle Jiao vessels; fortify Shen |
| Bilateral SP-9 (Yīlíngqúan) | Under the medial condyle of the tibia, in the depression posterior and inferior to the medial border of the tibia. | S1-S2 | Resolve dampness |
| Bilateral ST-25 (Tiānshū) | 2 cun lateral to center of umbilicus | Th6-Th12 | Remove Qi and blood stasis; harmonize spleen and stomach; resolve damp and damp-heat |
| Bilateral ST-29 (Guīlái) | On the lower abdomen, 4 cun below the center of the umbilicus, 2 cun lateral to the anterior median line. | Th6-Th12 | Invigorate blood and eliminate stasis |
| Bilateral KID-3 (Tàixī) | In the depression between the medial malleolus and the Achilles tendon, level with the tip of the medial malleolus | L4 | Tonify kidney Yang |
| Left KID-6 (Zhàohăi) coupled with Right LU-7 (Lièquè) | K6:1 cun inferior to the tip of the medial malleolus, in a depression formed by two ligamentous bundles Lu 7: 1.5 cun proximal to the most distal skin crease of the wrist, proximal to the styloid of the radius in a depression between the tendons of brachioradialis and abductor pollicis longus. | S1 coupled with C7 | Regulate the directing vessel and strengthen the uterus; help to dissolve the masses |
| DU-20 (Bàihuì) | On the midline of the head, 7 cun directly above the posterior hairline, approximately on the midpoint of the line connecting the apexes of the two auricles. | C2-C3; Trigeminus nerve | Clears the mind, lifts the spirits, tonifies Yang, strengthens the ascending function of the spleen, eliminates interior wind |
| P-6 (Nèiguān) coupled to Left SP-4 (Gōngsūn) | P6: on the palmar aspect of the forearm, 2 cun above the transverse crease of the wrist, on the line connecting PC 3 and PC 7, between the tendons of m. palmaris longus and m. flexor carpi radialis. Sp4: just distal and inferior to the proximal end of the metatarsal bone of the big toe | C8-Th1 coupled to L4? | Nourish blood in Chong Mai and strengthen the uterus |
| Sham Acupuncture | |||
| Acupoint | Location | Skin Innervation | TCM Action |
| No known point | On top of acromion | C3-4, n. Supraclavicularis | No known action |
| No known point | On umerus lateral side of the upper arm | C5-6, n. cutaneous brachiilateralis | No known action |
References
- Rasquin Leon, L.I.; Mayrin, J.V. Polycystic Ovarian Disease; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Azziz, R. PCOS: A diagnostic challenge. Reprod. Biomed. Online 2004, 8, 644–648. [Google Scholar] [CrossRef]
- Rotterdam ESHRE/ASRM; Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. 2004, 81, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.-W.; Chen, H.-H.; Hsieh, M.-C.; Chen, C.-C.; Hsu, S.-P.; Yip, H.-T.; Kao, C.-H. Increased Risk of Polycystic Ovary Syndrome and It’s Comorbidities in Women with Autoimmune Thyroid Disease. Int. J. Environ. Res. Public Health 2020, 17, 2422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewailly, D.; Barbotin, A.-L.; Dumont, A.; Catteau-Jonard, S.; Robin, G. Role of Anti-Müllerian Hormone in the Pathogenesis of Polycystic Ovary Syndrome. Front. Endocrinol. 2020, 11, 641. [Google Scholar] [CrossRef]
- Chen, Z.-J.; Shi, Y.; Sun, Y.; Zhang, B.; Liang, X.; Cao, Y.; Yang, J.; Liu, J.; Wei, D.; Weng, N.; et al. Fresh versus Frozen Embryos for Infertility in the Polycystic Ovary Syndrome. N. Engl. J. Med. 2016, 375, 523–533. [Google Scholar] [CrossRef]
- Zhang, Y.; Hu, M.; Jia, W.; Liu, G.; Zhang, J.; Wang, B.; Li, J.; Cui, P.; Li, X.; Lager, S.; et al. Hyperandrogenism and insulin resistance modulate gravid uterine and placental ferroptosis in PCOS-like rats. J. Endocrinol. 2020, 246, 247–263. [Google Scholar] [CrossRef]
- Cox, M.J.; Edwards, M.C.; Paris, V.R.; Aflatounian, A.; Ledger, W.L.; Gilchrist, R.B.; Padmanabhan, V.; Handelsman, D.J.; A Walters, K. Androgen Action in Adipose Tissue and the Brain are Key Mediators in the Development of PCOS Traits in a Mouse Model. Endocrinology 2020, 161, bqaa061. [Google Scholar] [CrossRef]
- Brown, J.; Farquhar, C.; Beck, J.; Boothroyd, C.; Hughes, E. Clomiphene and anti-oestrogens for ovulation induction in PCOS. Cochrane Database Syst. Rev. 2009, 4, CD002249. [Google Scholar]
- Szilágyi, A.; Szabó, I. Endocrine characteristics of polycystic ovary syndrome (PCOS). Indian J. Exp. Biol. 2003, 41, 694–700. [Google Scholar]
- Witchel, S.F.; Teede, H.J.; Peña, A.S. Curtailing PCOS. Pediatr Res. 2020, 87, 353–361. [Google Scholar] [CrossRef]
- Podfigurna, A.; Meczekalski, B.; Petraglia, F.; Luisi, S. Clinical, hormonal and metabolic parameters in women with PCOS with different combined oral contraceptives (containing chlormadinone acetate versus drospirenone). J. Endocrinol. Investig. 2019, 43, 483–492. [Google Scholar] [CrossRef] [Green Version]
- Gunning, M.N.; Petermann, T.S.; Crisosto, N.; van Rijn, B.B.; A de Wilde, M.; Christ, J.P.; Uiterwaal, C.S.P.M.; de Jager, W.; Eijkemans, M.J.C.; Kunselman, A.R.; et al. Cardiometabolic health in offspring of women with PCOS compared to healthy controls: A systematic review and individual participant data meta-analysis. Hum. Reprod. Updat. 2019, 26, 104–118. Available online: https://pubmed.ncbi.nlm.nih.gov/31867675 (accessed on 3 February 2021). [CrossRef]
- Wang, H.; Ruan, X.; Li, Y.; Cheng, J.; Mueck, A.O. Oxidative stress indicators in Chinese women with PCOS and correlation with features of metabolic syndrome and dependency on lipid patterns. Arch. Gynecol. Obstet. 2019, 300, 1413–1421. [Google Scholar] [CrossRef]
- Szosland, K.; Karzkowiak, A.; Lewinski, A. Metabolic characteristics of women diagnosed with polycystic ovary syndrome (PCOS) according to the Rotterdam criteria—Our own experience. Neuro Endocrinol. Lett. 2019, 39, 434–440. [Google Scholar]
- Gainder, S.; Sachdeva, G.; Suri, V.; Sachdeva, N.; Chopra, S. Comparison of the different PCOS phenotypes based on clinical metabolic, and hormonal profile, and their response to clomiphene. Indian J. Endocrinol. Metab. 2019, 23, 326–331. [Google Scholar] [CrossRef]
- Kakoly, N.S.; Moran, L.J.; Teede, H.J.; E Joham, A. Cardiometabolic risks in PCOS: A review of the current state of knowledge. Expert Rev. Endocrinol. Metab. 2018, 14, 23–33. [Google Scholar] [CrossRef]
- Torchen, L.C. Cardiometabolic Risk in PCOS: More than a Reproductive Disorder. Curr. Diabetes Rep. 2017, 17, 137. [Google Scholar] [CrossRef] [Green Version]
- Barry, J.; Qu, F.; Hardiman, P. An exploration of the hypothesis that testosterone is implicated in the psychological functioning of women with polycystic ovary syndrome (PCOS). Med. Hypotheses 2018, 110, 42–45. [Google Scholar] [CrossRef]
- Jiskoot, G.; Benneheij, S.; Beerthuizen, A.; de Niet, J.; de Klerk, C.; Timman, R.; Busschbach, J.; Laven, J. A three-component cognitive behavioural lifestyle program for preconceptional weight-loss in women with polycystic ovary syndrome (PCOS): A protocol for a randomized controlled trial. Reprod. Health 2017, 14. [Google Scholar] [CrossRef] [Green Version]
- Ilie, I.R. Neurotransmitter, neuropeptide and gut peptide profile in PCOS-pathways contributing to the pathophysiology, food intake and psychiatric manifestations of PCOS. Adv. Clin. Chem. 2020, 96, 85–135. [Google Scholar]
- Azizi Kutenaee, M.; Amirjani, S.; Asemi, Z.; Taghavi, S.-A.; Allan, H.; Kamalnadian, S.-N. The impact of depression, self-esteem, and body image on sleep quality in patients with PCOS: A cross-sectional study. Sleep Breath. 2020, 24, 1027–1034. [Google Scholar] [CrossRef]
- Damone, A.L.; Joham, A.E.; Loxton, D.; Earnest, A.; Teede, H.J.; Moran, L.J. Depression, anxiety and perceived stress in women with and without PCOS: A community-based study. Psychol Med. 2019, 49, 1510–1520. [Google Scholar] [CrossRef] [PubMed]
- Karjula, S.; Morin-Papunen, L.; Auvinen, J.; Ruokonen, A.; Puukka, K.; Franks, S.; Järvelin, M.-R.; Tapanainen, J.S.; Jokelainen, J.; Miettunen, J.; et al. Psychological Distress Is More Prevalent in Fertile Age and Premenopausal Women with PCOS Symptoms: 15-Year Follow-Up. J. Clin. Endocrinol. Metab. 2017, 102, 1861–1869. [Google Scholar] [CrossRef] [PubMed]
- Copp, T.; Hersch, J.; Muscat, D.M.; McCaffery, K.J.; Doust, J.; Dokras, A. The benefits and harms of receiving a polycystic ovary syndrome diagnosis: A qualitative study of women’s experiences. Hum. Reprod. Open 2019, 4, hoz026. Available online: http://europepmc.org/abstract/MED/31687475 (accessed on 3 February 2021). [CrossRef] [PubMed]
- Dokras, A. Mood and anxiety disorders in women with PCOS. Steroids 2012, 77, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.J.; Misso, M.L.; Boyle, J.A.; Garad, R.M.; McAllister, V.; Downes, L. Translation and implementation of the Australian-led PCOS guideline: Clinical summary and translation resources from the International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. Med. J. Aust. 2018, 209, S3–S8. [Google Scholar] [CrossRef] [PubMed]
- Azziz, R.; Kintziger, K.; Li, R.; Laven, J.; Morin-Papunen, L.; Merkin, S.S.; Teede, H.; O Yildiz, B. Recommendations for epidemiologic and phenotypic research in polycystic ovary syndrome: An androgen excess and PCOS society resource. Hum. Reprod. 2019, 34, 2254–2265. [Google Scholar] [CrossRef]
- Lie Fong, S.; Douma, A.; Verhaeghe, J. Implementing the international evidence-based guideline of assessment and management of polycystic ovary syndrome (PCOS): How to achieve weight loss in overweight and obese women with PCOS? J. Gynecol. Obstet. Hum. Reprod. 2020, 50, 101894. Available online: https://www.sciencedirect.com/science/article/pii/S2468784720302518 (accessed on 3 February 2021). [CrossRef]
- Sun, J.; Jin, C.; Wu, H.; Zhao, J.; Cui, Y.; Liu, H. Effects of electro-acupuncture on ovarian P450arom, P450c17α and mRNA expression induced by letrozole in PCOS rats. PLoS ONE 2013, 8, e79382. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Cui, W.; Sun, W.; Zhang, Q.-Y.; Guan, Q. Effect of electro-acupuncture on the spindle and oocytes quality in patients with PCOS. Zhongguo Zhong Xi Yi Jie He Za Zhi Zhongguo Zhongxiyi Jiehe Zazhi Chin. J. Integr. Tradit. West. Med. 2015, 35, 304–309. [Google Scholar]
- Mannerås, L.; Cajander, S.; Lönn, M.; Stener-Victorin, E. Acupuncture and exercise restore adipose tissue expression of sympathetic markers and improve ovarian morphology in rats with dihydrotestosterone-induced PCOS. Am. J. Physiol. Integr. Comp. Physiol. 2009, 296, R1124–R1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, L.; Qiao, X. Acupuncture is not as effective as infertility treatment in women with PCOS. Evid.-Based Med. 2017, 22, 229–230. [Google Scholar] [CrossRef]
- Wang, Q.; Deng, H.; Cheng, K.; Huang, Z.; Yin, X.; Zhou, Y.; Yang, Y.; Shen, W.; Zhao, L.; Shen, X. Manual acupuncture for the infertile female with polycystic ovary syndrome (PCOS): Study protocol for a randomized sham-controlled trial. Trials 2019, 20, 564. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.-L.; Huo, Z.-J.; Wang, H.-N.; Wang, W.; Chang, C.-Q.; Shi, L.; Li, D.; Li, R.; Qiao, J. Acupuncture ameliorates negative emotion in PCOS patients: A randomized controlled trial. Zhongguo Zhen Jiu Chin. Acupunct. Moxibustion 2020, 40, 385–390. [Google Scholar]
- Chen, S.-Z. An analysis on correlation between acupoint and target organs of acupuncture-moxibustion from the perspective of modern medical sciences. Zhen Ci Yan Jiu Acupunct. Res. 2019, 44, 620–624. [Google Scholar]
- Chen, H.; Lim, C.E.D. The efficacy of using acupuncture in managing polycystic ovarian syndrome. Curr. Opin. Obstet. Gynecol. 2019, 31, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Xu, L.; Pan, X.; Zhang, J.; Wu, T.; Liu, G.J. Ultrasound-guided transvaginal ovarian needle drilling for clomiphene-resistant polycystic ovarian syndrome in subfertile women. Cochrane Database Syst. Rev. 2019, 7, CD008583. [Google Scholar] [CrossRef]
- Lim, C.E.D.; Ng, R.W.C.; Cheng, N.C.L.; Zhang, G.S.; Chen, H. Acupuncture for polycystic ovarian syndrome. Cochrane Database Syst. Rev. 2019, 7, CD007689. [Google Scholar] [CrossRef]
- Yang, E.S.; Li, P.-W.; Nilius, B.; Li, G. Ancient Chinese medicine and mechanistic evidence of acupuncture physiology. Pflügers Arch. Eur. J. Physiol. 2011, 462, 645. [Google Scholar] [CrossRef] [Green Version]
- Lim, D.C.E.; Chen, W.; Cheng, L.N.C.; Xue, C.C.; Wong, F.W.S.; O’Sullivan, A.J.; Liu, J.P. Acupuncture for polycystic ovarian syndrome. Cochrane Database Syst. Rev. 2011, CD007689. [Google Scholar] [CrossRef]
- Lim, C.E.D.; Wong, W.S.F. Current evidence of acupuncture on polycystic ovarian syndrome. Gynecol. Endocrinol. 2010, 26, 473–478. [Google Scholar] [CrossRef]
- Johansson, J.; Mannerås-Holm, L.; Shao, L.; Olsson, A.; Lönn, M.; Billig, H.; Stener-Victorin, E. Electrical vs Manual Acupuncture Stimulation in a Rat Model of Polycystic Ovary Syndrome: Different Effects on Muscle and Fat Tissue Insulin Signaling. PLoS ONE 2013, 8, e54357. Available online: https://pubmed.ncbi.nlm.nih.gov/23349861 (accessed on 3 February 2021). [CrossRef]
- Lin, M.-J.; Chen, H.-W.; Liu, P.-H.; Cheng, W.-J.; Kuo, S.-L.; Kao, M.-C. The prescription patterns of traditional Chinese medicine for women with polycystic ovary syndrome in Taiwan: A nationwide population-based study. Medicine 2019, 98, e15890. Available online: https://journals.lww.com/md-journal/Fulltext/2019/06140/The_prescription_patterns_of_traditional_Chinese.17.aspx (accessed on 3 February 2021). [CrossRef]
- Lyttleton, J. Treatment of Infertility with Chinese Medicine; E-Book; Churchill Livingstone, Elsevier Health Sciences: London, UK, 2013. [Google Scholar]
- Lizneva, D.V.; Kirubakaran, R.; Mykhalchenko, K.; Suturina, L.; Chernukha, G.; Diamond, M.P.; Azziz, R. Phenotypes and body mass in women with polycystic ovary syndrome identified in referral versus unselected populations: Systematic review and meta-analysis. Fertil. Steril. 2016, 106, 1510–1520.e2. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Gao, J.; Cai, W.; Xie, L.; Ma, H.; Zhang, Y.; Cong, J.; Jian-Ping, L.; Ernest, H.N.; Wu, X.K. Characteristics and obstetrics outcomes of different traditional Chinese medicine syndromes in women with polycystic ovary syndrome: A secondary analysis. J. Obstet. Gynaecol. Res. 2017, 43, 136–157. [Google Scholar] [CrossRef] [Green Version]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J.; on behalf of the International PCOS Network. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil. Steril. 2018, 110, 364–379. [Google Scholar] [CrossRef] [Green Version]
- Ross, J. Acupuncture Point Combinations: The Key to Clinical Success; Churchill Livingstone: Edinburgh, UK, 1995. [Google Scholar]
- Ciconelli, R.M. Medical Outcomes Study 36-Item Short-Form Heal. Doutorado Thesis, Universidade Federal de São Paulo, São Paulo, Brazil, 1997. [Google Scholar]
- Ponciano, E.; Vaz Serra, A.; Relvas, J. Afericao da Escala de Auto-valiacao de Ansiedade de SAS numa amostra da populacao portuguesa-IR da aplicacao numa amostra de populacao normal. Psiquiatr. Clín. 1982, 3, 191–202. [Google Scholar]
- Chagas, M.H.; Tumas, V.; Loureiro, S.R.; Hallak, J.E.; Trzesniak, C.; De Sousa, J.P.; Rodrigues, G.G.; Santos Filho, A.; Crippa, J.A. Validity of a Brazilian version of the Zung self-rating depression scale for screening of depression in patients with Parkinson’s disease. Park. Relat. Disord. 2010, 16, 42–45. Available online: https://www.sciencedirect.com/science/article/pii/S1353802009001989 (accessed on 3 February 2021). [CrossRef]
- Johansson, J.; Stener-Victorin, E. Polycystic Ovary Syndrome: Effect and Mechanisms of Acupuncture for Ovulation Induction. Evid.-Based Complement. Altern. Med. 2013, 2013, 762615. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.; Chen, H.; Zhao, D.; Zhang, L.; Yu, X.; Zhou, X.; Liu, Z. The efficacy of Tung’s acupuncture for sex hormones in polycystic ovary syndrome: A randomized controlled trial. Complement. Ther. Med. 2019, 44, 182–188. [Google Scholar] [CrossRef]
- El-Shamy, F.F.; El-Kholy, S.S.; El-Rahman, M.M.A. Effectiveness of Laser Acupoints on Women with Polycystic Ovarian Syndrome: A Randomized Controlled Trial. J. Lasers Med Sci. 2018, 9, 113–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, W.; Zhao, K.; Yang, H. Effect of acupoint catgut embedding therapy combined with Chinese medicine for nourishing the kidneys and promoting blood circulation and improving blood glucose and lipid levels as well as the pregnancy rate in obese PCOS patients with infertility. Exp. Ther. Med. 2016, 12, 2909–2914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacPherson, H.; Altman, D.G.; Hammerschlag, R.; Youping, L.; Taixiang, W.; White, A.; Moher, D. Revised Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): Extending the CONSORT statement. Acupunct. Relat. Ther. 2015, 3, 35–46. [Google Scholar] [CrossRef]


| Phenotype | Description |
|---|---|
| Rotterdam Phenotype A (classical PCOS) [46] | Hyperandrogenism + polycystic ovary morphology + ovulatory dysfunction—28.7% |
| TCM phenotype [47] | Spleen deficiency and phlegm stasis SP’s—32.27% |
| Rotterdam Phenotype B [46] | Hyperandrogenism + Ovulatory disfunction—19.0% |
| TCM phenotype [47] | Phlegm stasis and blood stasis—16.55% |
| Rotterdam Phenotype C [46] | Ovulatory disfunction + polycystic ovary morphology—37.3% |
| TCM phenotype [47] | Kidney deficiency and liver stasis—40.29% |
| Rotterdam Phenotype D [46] | Hyperandrogenism + polycystic ovary morphology—15.0% |
| TCM phenotype [47] | Kidney deficiency and blood stasis—10.89% |
| STUDY PERIOD | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Enrolment | Allocation | Post-Allocation | Close-Out | ||||||||||||
| TIMEPOINT | −1 month | 0 | W1 | W2 | W3 | W4 | W5 | W6 | W7 | W8 | W9 | W10 | W11 | W12 | After 6 months |
| ENROLMENT: | |||||||||||||||
| Eligibility screen | X | ||||||||||||||
| Informed consent | X | ||||||||||||||
| Baseline assessments | X | ||||||||||||||
| Allocation | X | ||||||||||||||
| INTERVENTIONS: | |||||||||||||||
| Active acupuncture |  | ||||||||||||||
| X | X | X | X | X | X | X | X | ||||||||
| Sham acupuncture |  | ||||||||||||||
| X | X | X | X | X | X | X | X | ||||||||
| ASSESSMENTS: | |||||||||||||||
| Diagnostic examination | X | ||||||||||||||
| Primary and secondary outcomes | X | X | X | X | |||||||||||
| Life quality related questionnaires | X | X | X | X | X | ||||||||||
| Primary | Secondary | Exploratory |
|---|---|---|
| Hormonal Parameters: Modified Ferriman-Gallwey score Ludwig visual score LH, mean (SD), mIU/mL FSH, mean (SD), mIU/mL LH/FSH Total free testosterone Androstenedione Progesterone, median (IQR), ng/mL Estradiol, median (IQR), pg/mL Sex hormone–binding globulin (SHBG), mean (SD), μg/mL Ovulation rate (%) | Anthropometric parameters Age (years) Height (cm) Weight (Kg) BMI (kg/m2) Waist circumference (cm) Waist Hip Ratio | Quality-of-life scores: Medical Outcomes Study 36-Item Short Form Health Survey Zung Self-Rating Anxiety Scale Zung Self-Rating Depression |
| Metabolic parameters TG (mg/dL) Total cholesterol, mean (SD), mg/dL LDL/HDL LDL-C (mg/dL) HDL-C(mg/dL) HOMA-IR Fasting glucose (mg/dL) Fasting insulin, mean (SD), μIU/mL Serum insulin (mU/L) Metabolic syndrome, No/total (%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Oliveira, N.M.; Machado, J.; Huang, Z.; Criado, M.B. Acupuncture in Women with Human Polycystic Ovary/Ovarian Syndrome: Protocol for a Randomized Controlled Trial. Healthcare 2022, 10, 1999. https://doi.org/10.3390/healthcare10101999
de Oliveira NM, Machado J, Huang Z, Criado MB. Acupuncture in Women with Human Polycystic Ovary/Ovarian Syndrome: Protocol for a Randomized Controlled Trial. Healthcare. 2022; 10(10):1999. https://doi.org/10.3390/healthcare10101999
Chicago/Turabian Stylede Oliveira, Natália M., Jorge Machado, Zaiwei Huang, and Maria Begoña Criado. 2022. "Acupuncture in Women with Human Polycystic Ovary/Ovarian Syndrome: Protocol for a Randomized Controlled Trial" Healthcare 10, no. 10: 1999. https://doi.org/10.3390/healthcare10101999