
Local Tramadol Improves the Anesthetic Success in Patients with Symptomatic Irreversible Pulpitis: A Meta-Analysis
 , , , ,
, , , ,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
Study Design
3. Information Search
3.1. Population, Interventions, Control, and Outcome (PICO) Approach [31]
3.1.1. Inclusion Criteria
3.1.2. Exclusion Criteria
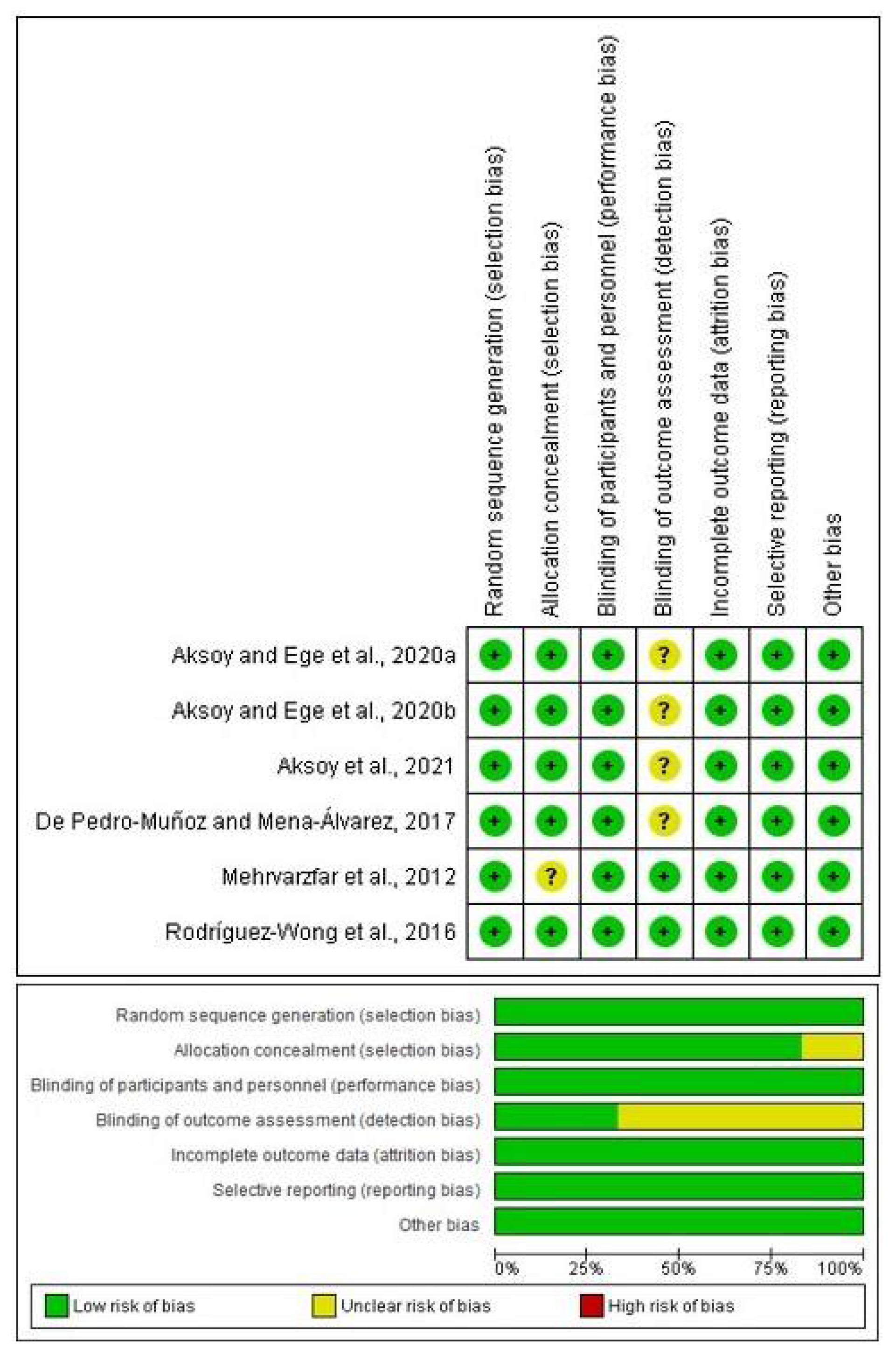
3.2. The Cochrane Collaboration’s Risk-of-Bias Tool
3.3. Extraction of Information
3.4. Statistical Analysis
4. Results
4.1. Search and Measurement of Bias
4.2. Qualitative Assessment
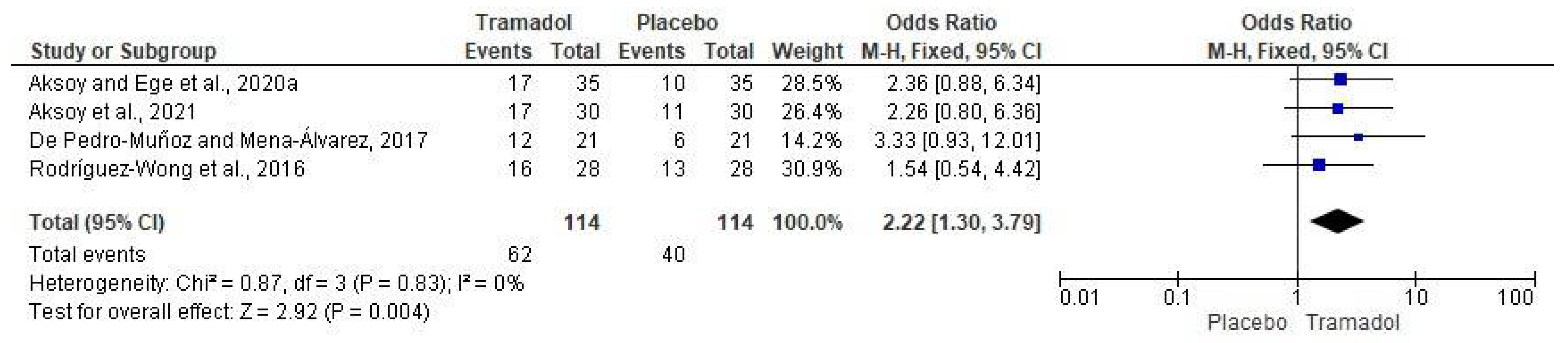
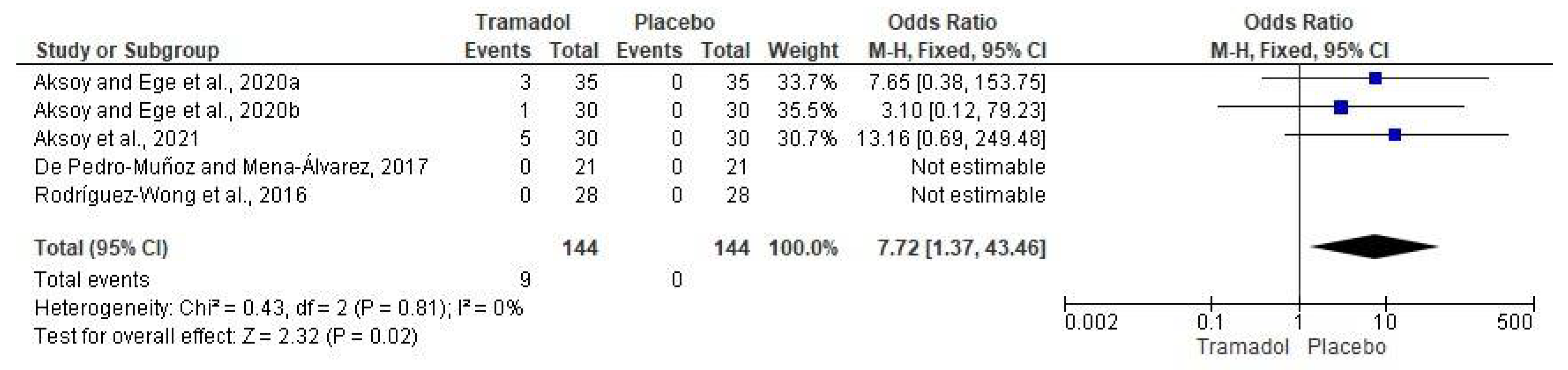
4.3. Quantitative Evaluation
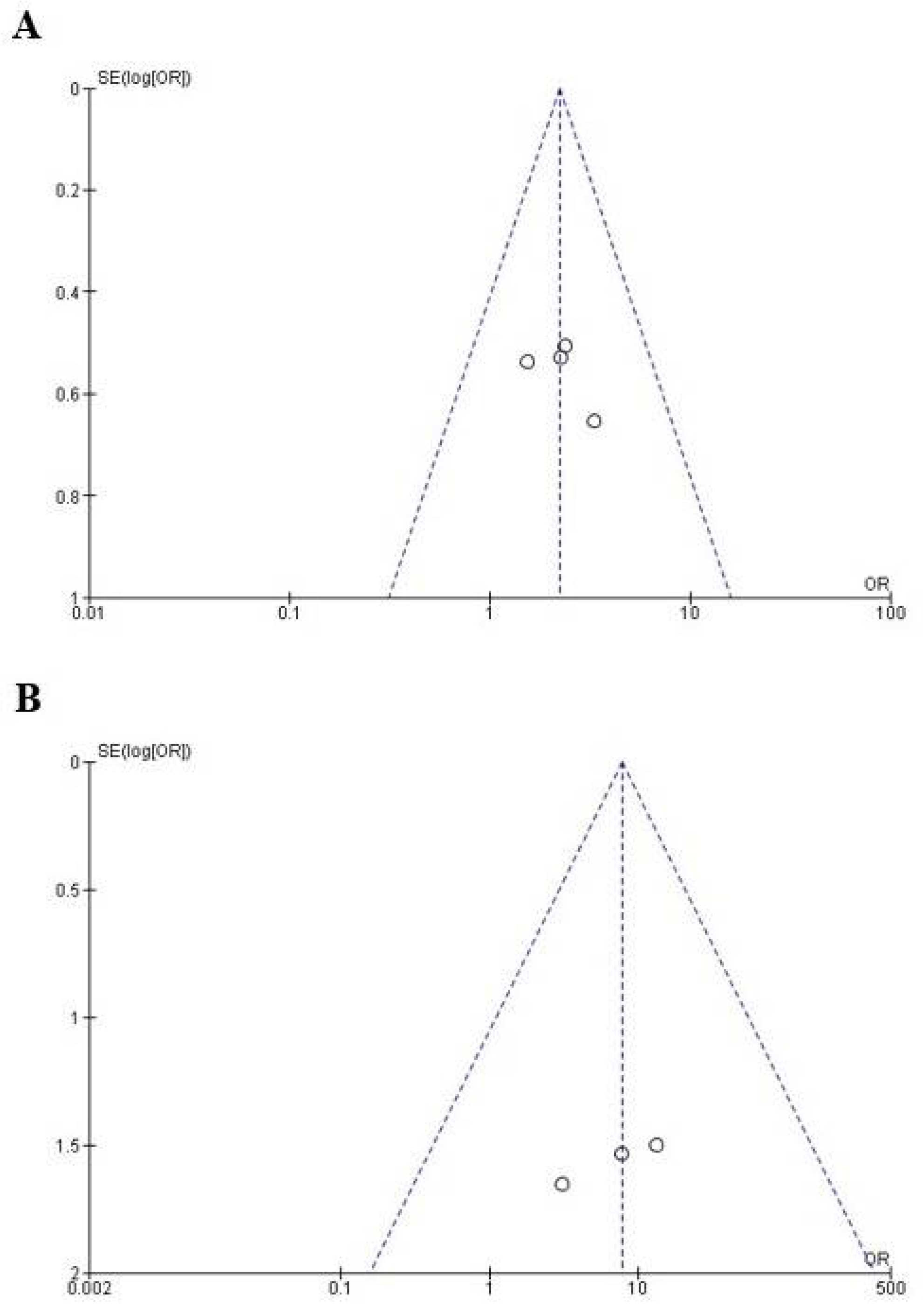
4.4. The Publication Bias
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eren, B.; Onay, E.O.; Ungor, M. Assessment of alternative emergency treatments for symptomatic irreversible pulpitis: A randomized clinical trial. Int. Endod. J. 2018, 51, e227–e237. [Google Scholar] [CrossRef]
- Schellenberg, J.; Drum, M.; Reader, A.; Nusstein, J.; Fowler, S.; Beck, M. Effect of Buffered 4% Lidocaine on the Success of the Inferior Alveolar Nerve Block in Patients with Symptomatic Irreversible Pulpitis: A Prospective, Randomized, Double-blind Study. J. Endod. 2015, 41, 791–796. [Google Scholar]
- MacDonald, E.; Drum, M.; Nusstein, J. Anesthetic Success Using Nitrous Oxide and a Combination of Lidocaine/Clonidine for the Inferior Alveolar Nerve Block and the Effects on Blood Pressure and Pulse in Patients with Symptomatic Irreversible Pulpitis: A Prospective, Randomized, Double-blind Study. J. Endod. 2021, 47, 558–565. [Google Scholar]
- de Geus, J.L.; Wambier, L.M.; Boing, T.F. Effect of ibuprofen on the efficacy of inferior alveolar nerve block in patients with irreversible pulpitis: A meta-analysis. Aust. Endod. J. 2019, 45, 246–258. [Google Scholar] [CrossRef]
- Nogueira, B.M.L.; Silva, L.G.; Mesquita, C.R.M.; Menezes, S.A.F.; Menezes, T.O.A.; Faria, A.G.M.; Porpino, M.T.M. Is the Use of Dexamethasone Effective in Controlling Pain Associated with Symptomatic Irreversible Pulpitis? A Systematic Review. J. Endod. 2018, 44, 703–710. [Google Scholar] [CrossRef]
- Elsharrawy, E.A.; Elbaghdady, Y.M. A double-blind comparison of a supplemental interligamentary injection of fentanyl and mepivacaine with 1:200,000 epinephrine for irreversible pulpitis. J. Pain Symptom Manag. 2007, 33, 203–207. [Google Scholar] [CrossRef]
- Uhle, R.A.; Reader, A.; Nist, R.; Weaver, J.; Beck, M.; Meyers, W.J. Peripheral opioid analgesia in teeth with symptomatic inflamed pulps. Anesth. Prog. 1997, 44, 90–95. [Google Scholar]
- Mohajeri, L.; Salehi, F.; Mehrvarzfar, P.; Arfaee, H.; Bohluli, B.; Hamedy, R. Anesthetic efficacy of meperidine in teeth with symptomatic irreversible pulpitis. Anesth. Prog. 2015, 62, 14–19. [Google Scholar] [CrossRef]
- Sehgal, N.; Smith, H.S.; Manchikanti, L. Peripherally acting opioids and clinical implications for pain control. Pain Physician 2011, 14, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, N.; Piché, M.; Hotta, H. Types of skin afferent fibers and spinal opioid receptors that contribute to touch-induced inhibition of heart rate changes evoked by noxious cutaneous heat stimulation. Mol. Pain 2015, 11, 4. [Google Scholar] [CrossRef]
- Lu, C.W.; Kuei-Huang, S.; Lin, T.Y.; Wang, S.J. Tapentadol Suppresses Glutamatergic Transmission and Neuronal Firing in Rat Hippocampal CA3 Pyramidal Neurons. Pharmacology 2020, 105, 445–453. [Google Scholar] [CrossRef] [PubMed]
- van de Donk, T.; van Velzen, M.; Dahan, A.; Niesters, M. Cornea nerve fibre state determines analgesic response to tapentadol in fibromyalgia patients without effective endogenous pain modulation. Eur. J. Pain 2019, 23, 1586–1595. [Google Scholar] [CrossRef] [PubMed]
- Aksoy, F.; Ege, B. Efficacy of submucosal tramadol and lidocaine on success rate of inferior alveolar nerve block in mandibular molars with symptomatic irreversible pulpitis. Odontology 2020, 108, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Aksoy, F.; Ege, B. The effect of pretreatment submucosal injections of tramadol and dexamethasone on post-endodontic pain in mandibular molar teeth with symptomatic irreversible pulpitis: A randomized controlled clinical trial. Int. Endod. J. 2020, 53, 176–185. [Google Scholar] [CrossRef]
- Aksoy, F.; Ege, B.; Tosun, S. The effect of pre-operative submucosal administration of dexamethasone, tramadol, articaine on the success rate of inferior alveolar nerve block on mandibular molars with symptomatic irreversible pulpitis: A randomized, double-blind placebo-controlled clinical trial. Int. Endod. J. 2021, 54, 1982–1992. [Google Scholar]
- De Pedro-Muñoz, A.; Mena-Álvarez, J. The effect of preoperative submucosal administration of tramadol on the success rate of inferior alveolar nerve block on mandibular molars with symptomatic irreversible pulpitis: A randomized, double-blind placebo-controlled clinical trial. Int. Endod. J. 2017, 50, 1134–1142. [Google Scholar] [CrossRef]
- Rodríguez-Wong, L.; Pozos-Guillen, A.; Silva-Herzog, D.; Chavarría-Bolaños, D. Efficacy of mepivacaine-tramadol combination on the success of inferior alveolar nerve blocks in patients with symptomatic irreversible pulpitis: A randomized clinical trial. Int. Endod. J. 2016, 49, 325–333. [Google Scholar] [CrossRef]
- Mehrvarzfar, P.; Abbott, P.V.; Saghiri, M.A.; Delvarani, A.; Asgar, K.; Lotfi, M.; Karamifar, K.; Kharazifard, M.J.; Khabazi, H. Effects of three oral analgesics on postoperative pain following root canal preparation: A controlled clinical trial. Int. Endod. J. 2012, 45, 76–82. [Google Scholar] [CrossRef]
- Isiordia-Espinoza, M.A.; de Jesús Pozos-Guillén, A.; Aragon-Martinez, O.H. Analgesic efficacy and safety of single-dose tramadol and non-steroidal anti-inflammatory drugs in operations on the third molars: A systematic review and meta-analysis. Br. J. Oral Maxillofac. Surg. 2014, 52, 775–783. [Google Scholar] [CrossRef]
- Isiordia-Espinoza, M.A.; Sánchez-Prieto, M.; Tobías-Azúa, F.; Reyes-García, J.G.; Granados-Soto, V. Pre-emptive analgesia with the combination of tramadol plus meloxicam for third molar surgery: A pilot study. Br. J. Oral Maxillofac. Surg. 2012, 50, 673–677. [Google Scholar] [CrossRef]
- Beakley, B.D.; Kaye, A.M.; Kaye, A.D. Tramadol, Pharmacology, Side Effects, and Serotonin Syndrome: A Review. Pain Physician 2015, 18, 395–400. [Google Scholar] [PubMed]
- Grond, S.; Sablotzki, A. Clinical pharmacology of tramadol. Clin. Pharmacokinet. 2004, 43, 879–923. [Google Scholar] [CrossRef]
- Mert, T.; Gunes, Y.; Ozcengiz, D.; Gunay, I.; Polat, S. Comparative effects of lidocaine and tramadol on injured peripheral nerves. Eur. J. Pharmacol. 2006, 543, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Haeseler, G.; Foadi, N.; Ahrens, J.; Dengler, R.; Hecker, H.; Leuwer, M. Tramadol, fentanyl and sufentanil but not morphine block voltage-operated sodium channels. Pain 2006, 126, 234–244. [Google Scholar] [CrossRef] [PubMed]
- Yalcin, I.; Aksu, F. Involvement of potassium channels and nitric oxide in tramadol antinociception. Pharmacol. Biochem. Behav. 2005, 80, 69–75. [Google Scholar] [CrossRef]
- de Oliveira Junior, J.O.; de Freitas, M.F.; Bullara de Andrade, C.; Chacur, M.; Ashmawi, H.A. Local analgesic effect of tramadol is mediated by opioid receptors in late postoperative pain after plantar incision in rats. J. Pain Res. 2016, 9, 797–802. [Google Scholar] [CrossRef]
- Pang, W.W.; Mok, M.S.; Chang, D.P.; Yang, T.F.; Lin, C.H.; Huang, M.H. Intradermal injection of tramadol has local anesthetic effect: A comparison with lidocaine. Acta Anaesthesiol. Sin. 1998, 36, 133–136. [Google Scholar]
- Pang, W.W.; Huang, P.Y.; Chang, D.P.; Huang, M.H. The peripheral analgesic effect of tramadol in reducing propofol injection pain: A comparison with lidocaine. Reg. Anesth. Pain Med. 1999, 24, 246–249. [Google Scholar]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Leonardo, R. PICO: Model for Clinical Questions. Evid. Based Med. Pract. 2018, 3, 2. [Google Scholar]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Collaboration: Oxford, UK, 2011; Available online: http://www.cochrane-handbook.org (accessed on 7 February 2022).
- Jones, A.; Steel, D. Evaluating the quality of medical evidence in real-world contexts. J. Eval. Clin. Pract. 2018, 24, 950–956. [Google Scholar] [CrossRef] [PubMed]
- Atkins, D.; Eccles, M.; Flottorp, S.; Guyatt, G.H.; Henry, D.; Hill, S.; Liberati, A.; O’Connell, D.; Oxman, A.D.; Phillips, B.; et al. GRADE Working Group. Systems for grading the quality of evidence and the strength of recommendations I: Critical appraisal of existing approaches the GRADE working group. BMC Health Serv. Res. 2004, 4, 38. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Figueroa-Fernández, N.P.; Hernández-Miramontes, Y.A.; Alonso-Castro, Á.J.; Isiordia-Espinoza, M.A. A meta-analysis on the efficacy of the ropivacaine infiltration in comparison with other dental anesthetics. Clin. Oral Investig. 2021, 25, 6779–6790. [Google Scholar] [CrossRef] [PubMed]
- Isiordia-Espinoza, M.A.; Franco-González, M.A.; Alonso-Castro, Á.J.; Franco-de la Torre, L. Analgesic effectiveness and safety of celecoxib versus non-opioid active controls after third molar surgery: A meta-analytical evaluation. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e1–e9. [Google Scholar] [CrossRef]
- Franco-de la Torre, L.; Figueroa-Fernández, N.P.; Franco-González, D.L.; Alonso-Castro, Á.J.; Rivera-Luna, F.; Isiordia-Espinoza, M.A. A Meta-Analysis of the Analgesic Efficacy of Single-Doses of Ibuprofen Compared to Traditional Non-Opioid Analgesics Following Third Molar Surgery. Pharmaceuticals 2021, 14, 360. [Google Scholar] [CrossRef]
- Lin, L.; Chu, H. Quantifying publication bias in meta-analysis. Biometrics 2018, 74, 785–794. [Google Scholar] [CrossRef]
- Mathur, M.B.; Vander Weele, T.J. Estimating publication bias in meta-analyses of peer-reviewed studies: A meta-meta-analysis across disciplines and journal tiers. Res. Synth. Methods. 2021, 12, 176–191. [Google Scholar] [CrossRef]
- Argimon-Pallás, J.M.; Jiménez-Villa, J. Métodos de Investigación Clínica y Epidemiológica, 5th ed.; Elsevier: Barcelona, Spain, 2019. [Google Scholar]
- Đanić, P.; Salarić, I.; Macan, D. New Findings on Local Tramadol Use in Oral Surgery. Acta Stomatol. Croat. 2017, 51, 336–344. [Google Scholar] [CrossRef]
- Al-Haideri, Y.A. Comparison of local anesthetic efficacy of tramadol hydrochloride (with adrenaline) versus plain tramadol hydrochloride in the extraction of upper molar teeth. J. Oral Maxillofac. Surg. 2013, 71, 2035–2038. [Google Scholar] [CrossRef]
- Pozos, A.J.; Martínez, R.; Aguirre, P.; Pérez, J. Tramadol administered in a combination of routes for reducing pain after removal of an impacted mandibular third molar. J. Oral Maxillofac. Surg. 2007, 65, 1633–1639. [Google Scholar] [CrossRef]
- Pozos, A.J.; Martinez, R.; Aguirre, P.; Pérez, J. The effects of tramadol added to articaine on anesthesia duration. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, 614–617. [Google Scholar] [CrossRef]
- Ceccheti, M.M.; Negrato, G.V.; Peres, M.P.; Deboni, M.C.; Naclério-Homem, M.G. Analgesic and adjuvant anesthetic effect of submucosal tramadol after mandibular third molar surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, e249–e254. [Google Scholar] [CrossRef] [PubMed]
- Isiordia-Espinoza, M.A.; Orozco-Solis, M.; Tobías-Azúa, F.J.; Méndez-Gutiérrez, E.P. Submucous tramadol increases the anesthetic efficacy of mepivacaine with epinephrine in inferior alveolar nerve block. Br. J. Oral Maxillofac. Surg. 2012, 50, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Isiordia-Espinoza, M.A.; Pozos-Guillén, A.J.; Martínez-Rider, R.; Herrera-Abarca, J.; Pérez-Urizar, J. Preemptive analgesic effectiveness of oral ketorolac plus local tramadol after impacted mandibular third molar surgery. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e776–e780. [Google Scholar] [CrossRef] [PubMed]
- Gönül, O.; Satılmış, T.; Bayram, F.; Göçmen, G.; Sipahi, A.; Göker, K. Effect of submucosal application of tramadol on postoperative pain after third molar surgery. Head Face Med. 2015, 11, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, Y.C.; Chang, P.J.; Jou, I.M. Direct tramadol application on sciatic nerve inhibits spinal somatosensory evoked potentials in rats. Anesth. Analg. 2001, 92, 1547–1551. [Google Scholar] [CrossRef] [PubMed]
- Altunkaya, H.; Ozer, Y.; Kargi, E.; Babuccu, O. Comparison of local anaesthetic effects of tramadol with prilocaine for minor surgical procedures. Br. J. Anaesth. 2003, 90, 320–322. [Google Scholar] [CrossRef]
- Kargi, E.; Babuccu, O.; Altunkaya, H.; Hosnuter, M.; Ozer, Y.; Babuccu, B.; Payasli, C. Tramadol as a local anaesthetic in tendon repair surgery of the hand. J. Int. Med. Res. 2008, 36, 971–978. [Google Scholar] [CrossRef]
- Tsaousi, G.G.; Chatzistravou, A.; Papazisis, G.; Grosomanidis, V.; Kouvelas, D.; Pourzitaki, C. Analgesic Efficacy and Safety of Local Infiltration of Tramadol in Pediatric Tonsillectomy Pain: A Systematic Review and Meta-Analysis. Pain Pract. 2020, 20, 550–563. [Google Scholar] [CrossRef] [PubMed]
- Mattar, O.M.; Abdalla, A.R.; Shehata, M.S.A.; Ali, A.S.; Sinokrot, M.; Abdelazeim, B.A.; Taher, A.; Samy, A.; Mahmoud, M.; Abbas, A.M. Efficacy and safety of tramadol in pain relief during diagnostic outpatient hysteroscopy: Systematic review and meta-analysis of randomized controlled trials. Fertil Steril. 2019, 111, 547–552. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID Study and, Study Design | Treatments (n) | Details of Patients, Dental Procedure, and Evaluation | Conclusions |
|---|---|---|---|
| Aksoy and Ege, 2020a [13]. Randomized, double-blind, parallel, clinical study. | Group A: Tramadol 100 mg (n = 35). Group B: Lidocaine 40 mg (n = 35). Group C: Normal saline (n = 35). All treatments were given (2 mL volume) across the mucobuccal fold of the mandibular molar. | Patients aged 18 to 60 years with symptomatic irreversible pulpitis diagnosis (moderate to severe pain) and, without periapical radiolucency on radiography at a mandibular molar were included. Patients without analgesic medication, at least, 24 h before the study. Positive Endo Ice F cold tests. A standard cartridge with 1.8 mL 2% lidocaine with 1:80,000 epinephrine was administered via the IANB route. Anesthesia was successful when the pain level of patients was no pain or mild pain. The anesthesia success rate and adverse effects were evaluated. | The results did not show any statistical difference between groups. |
| Aksoy and Ege, 2020b [14]. Randomized, double-blind, parallel, clinical trial. | Group A: Tramadol 100 mg (n = 30). Group B: Dexamethasone 8 mg (n = 30). Group C: Normal saline (n = 30). All treatments were given (2 mL volume) across the mucobuccal fold of the mandibular molar. | Healthy patients aged 18 to 65 years old with a diagnosis of symptomatic irreversible pulpitis (moderate to severe pain) in a mandibular molar, radiographically normal periapical area, and no pain on percussion were included. Patients without analgesic medication, at least, 12 h before the study. Positive Endo Ice F cold tests. An IANB using 4% articaine with 1:200,000 epinephrine was used. Postoperative pain intensity, rescue analgesic medication, and adverse effects were evaluated. | Submucosal tramadol was most effective for pain control when compared to saline. |
| Aksoy et al., 2021 [15]. Randomized, double-blind, parallel, clinical assay. | Group A: Tramadol 100 mg (n = 30). Group B: Dexamethasone 8 mg (n = 30). Group C: Articaine 4% (n = 30). Group D: Normal saline (n = 30). All treatments were given (2 mL volume) across the mucobuccal fold of the mandibular molar. | Healthy patients aged 18 to 65 years old with a diagnosis of symptomatic irreversible pulpitis (moderate to severe pain) in a mandibular molar, radiographically normal periapical area, and no pain on percussion were included. Patients without analgesic medication, at least, 24 h before the study. Positive Endo Ice F cold tests. An IANB using 4% articaine with 1:200,000 epinephrine was used. Anesthesia was successful when the pain level of patients was no pain or mild pain. Sensory blockade, duration of anesthesia, anesthetic success index, and adverse effects were assessed. | Submucosal articaine increased the success anesthesia rate and dexamethasone the duration of the anesthetic activity when compared to saline in patients with symptomatic irreversible pulpitis. |
| De Pedro-Muñoz and Mena-Álvarez, 2017 [16]. Randomized, double-blind, parallel, clinical investigation. | Group A: Tramadol 50 mg (n = 21). Group B: Normal saline (n = 21). All treatments were given (1 mL volume) across the mucobuccal fold of the mandibular molar. | Patients aged 18 to 64 years with symptomatic irreversible pulpitis diagnosis in a mandibular molar. Patients without analgesic medication, at least, 24 h before the study. Positive Endo Ice F cold tests. A standard cartridge with 1.8 mL 4% articaine with 1:100,000 epinephrine was administered via the IANB route. The access cavity, the anesthesia success rate, and adverse effects were evaluated. | Submucosal administration of tramadol increased the success rate of access cavity in patients with symptomatic irreversible pulpitis. |
| Mehrvarzfar et al., 2017 [18]. Randomized, double-blind, parallel, clinical study. | Group A: Tramadol 100 mg (n = 24). Group B: Acetaminophen 375 mg (n = 23). Group C: Naproxen 500 mg (n = 24). Group D: Placebo (n = 24). All treatments were administered orally. | Patients aged 20 and 60 years old without systemic illness and, no pregnant women. Patients without analgesic medication, at least, 12 h before the study. Anesthesia was done using 1 cartridge of lidocaine and adrenaline 1:80,000. Pain intensity was assessed pre-operatively, and at 6, 12, and 24 h. Adverse effects were not evaluated. | Tramadol was more effective for pain control after root channel therapy. |
| Rodríguez-Wong et al., 2016 [17]. Randomized, double-blind, parallel, clinical trial. | Group A: A cartridge with 1.3 mL of 2% mepivacaine with epinephrine 1:100 000 plus 0.5 mL of tramadol 25 mg/mL (n = 28). Group B: A cartridge with 1.8 mL of 2% mepivacaine with epinephrine 1:100 000 (n = 28). All treatments were given (1.8 mL volume) across the mucobuccal fold of the mandibular molar. | Patients aged 18 years or older with symptomatic irreversible pulpitis in a mandibular molar. Patients without analgesic medication, at least, 12 h before the study. Positive Endo Ice F cold tests. The IANB was performed according to the information of treatment groups. Anesthesia was successful when the pain level of patients was no pain or mild pain. Sensory blockade, duration of anesthesia, anesthetic success index, and adverse effects were assessed. | There was no statistical difference between treatment groups. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Sánchez, E.; Franco-de la Torre, L.; Bologna-Molina, R.E.; Molina-Frechero, N.; Serafín-Higuera, N.A.; Hernández-Gómez, A.; Alonso-Castro, Á.J.; Sat-Muñoz, D.; Isiordia-Espinoza, M.A. Local Tramadol Improves the Anesthetic Success in Patients with Symptomatic Irreversible Pulpitis: A Meta-Analysis. Healthcare 2022, 10, 1867. https://doi.org/10.3390/healthcare10101867
Gómez-Sánchez E, Franco-de la Torre L, Bologna-Molina RE, Molina-Frechero N, Serafín-Higuera NA, Hernández-Gómez A, Alonso-Castro ÁJ, Sat-Muñoz D, Isiordia-Espinoza MA. Local Tramadol Improves the Anesthetic Success in Patients with Symptomatic Irreversible Pulpitis: A Meta-Analysis. Healthcare. 2022; 10(10):1867. https://doi.org/10.3390/healthcare10101867
Chicago/Turabian StyleGómez-Sánchez, Eduardo, Lorenzo Franco-de la Torre, Ronell Eduardo Bologna-Molina, Nelly Molina-Frechero, Nicolás Addiel Serafín-Higuera, Adriana Hernández-Gómez, Ángel Josabad Alonso-Castro, Daniel Sat-Muñoz, and Mario Alberto Isiordia-Espinoza. 2022. "Local Tramadol Improves the Anesthetic Success in Patients with Symptomatic Irreversible Pulpitis: A Meta-Analysis" Healthcare 10, no. 10: 1867. https://doi.org/10.3390/healthcare10101867