
Markov Models for Economic Evaluation in Osteoporosis Treatment

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
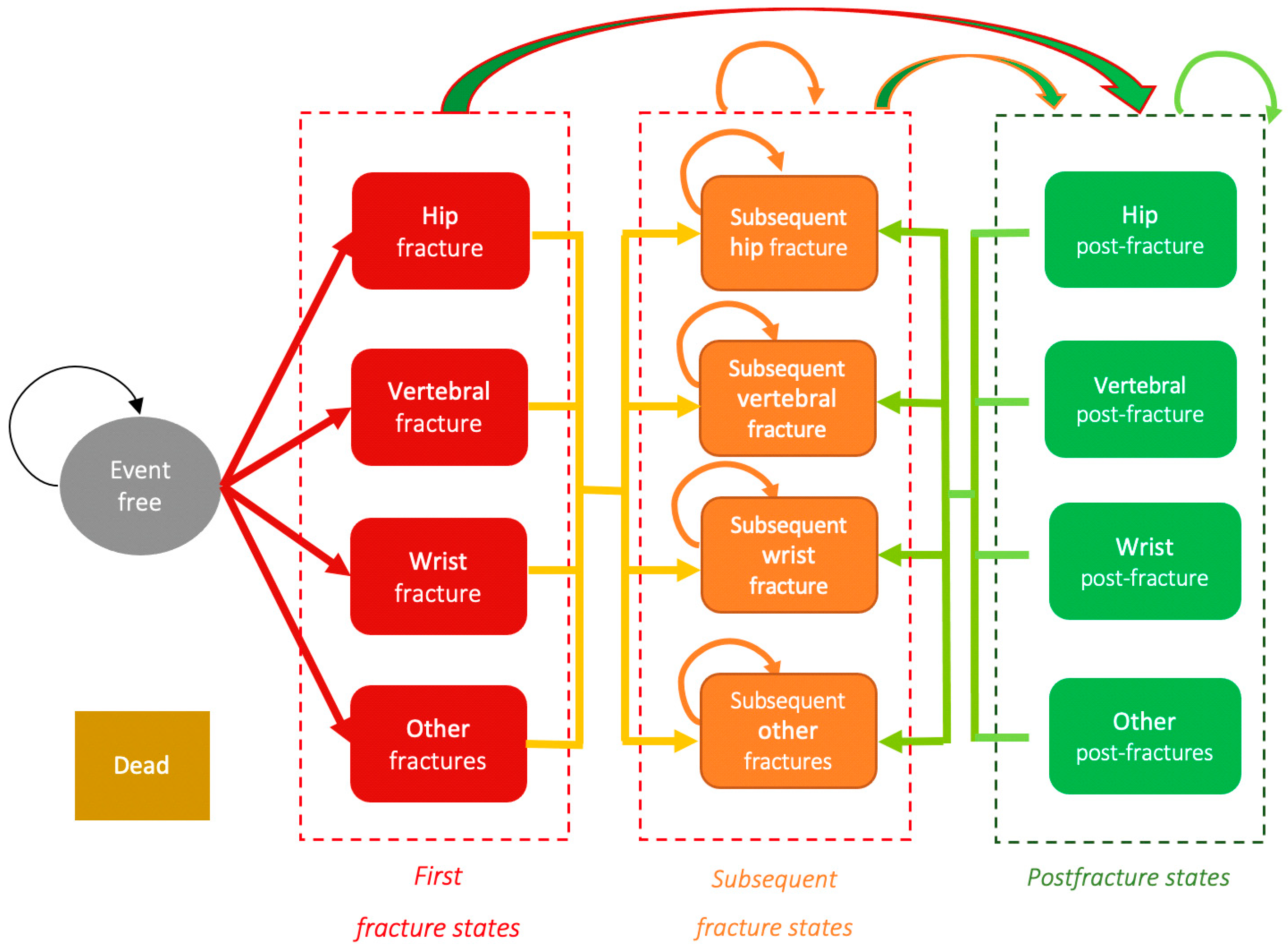
2.1. Design of the Markov Models
- The duration of treatment with denosumab is extended to 10 years, once its efficacy and safety are demonstrated [32].
- Treatment with teriparatide is started at the beginning of the model in patients without fractures.
2.2. Materials
2.2.1. Incidence of Fractures without Intervention
2.2.2. Efficacy and Safety in the Pharmaceutical Treatments
2.2.3. Costs of Fractures and Treatments
2.2.4. Mortality
2.2.5. Utility or Quality of Life
2.2.6. Treatment Adherence and Persistence
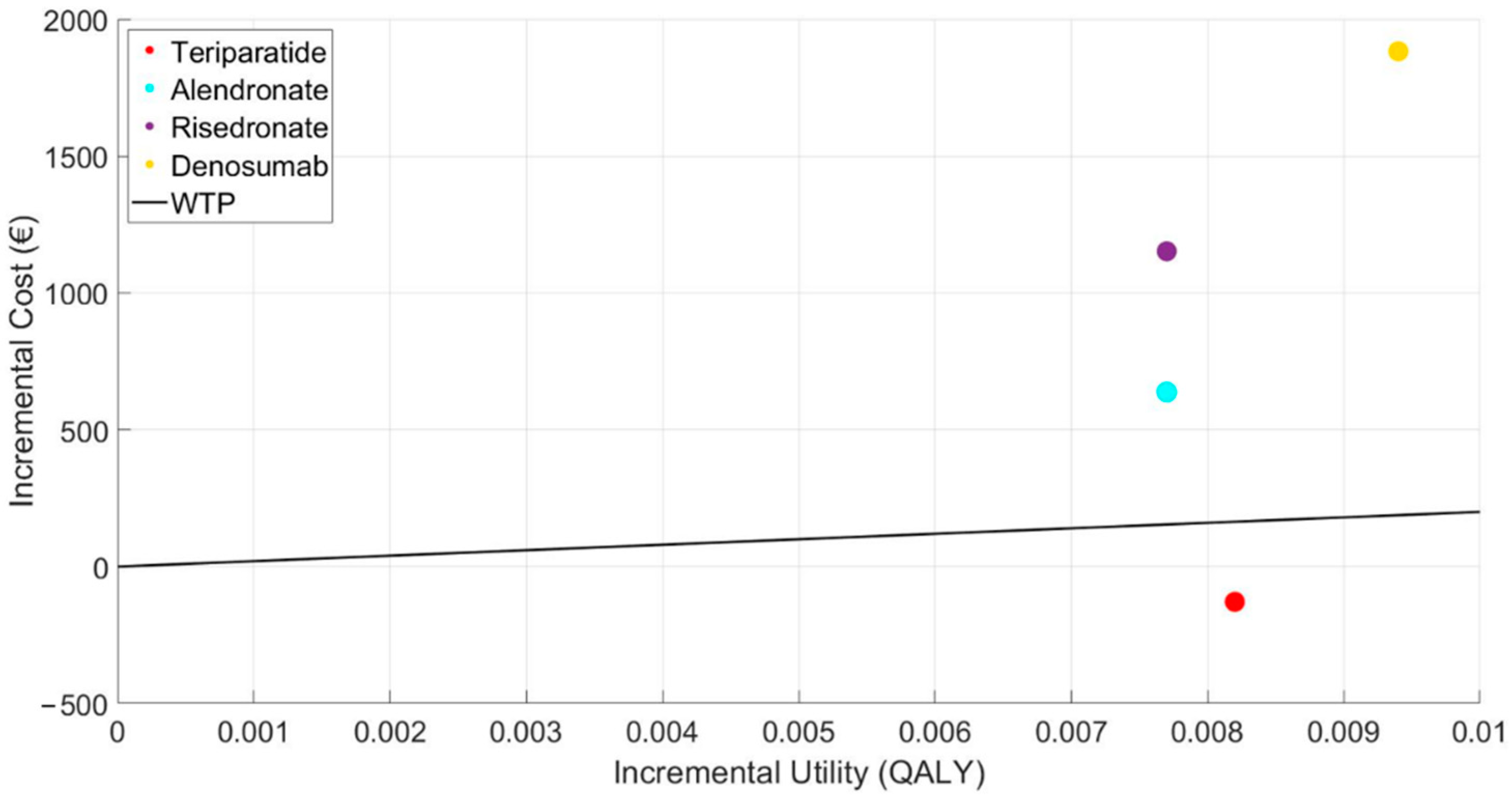
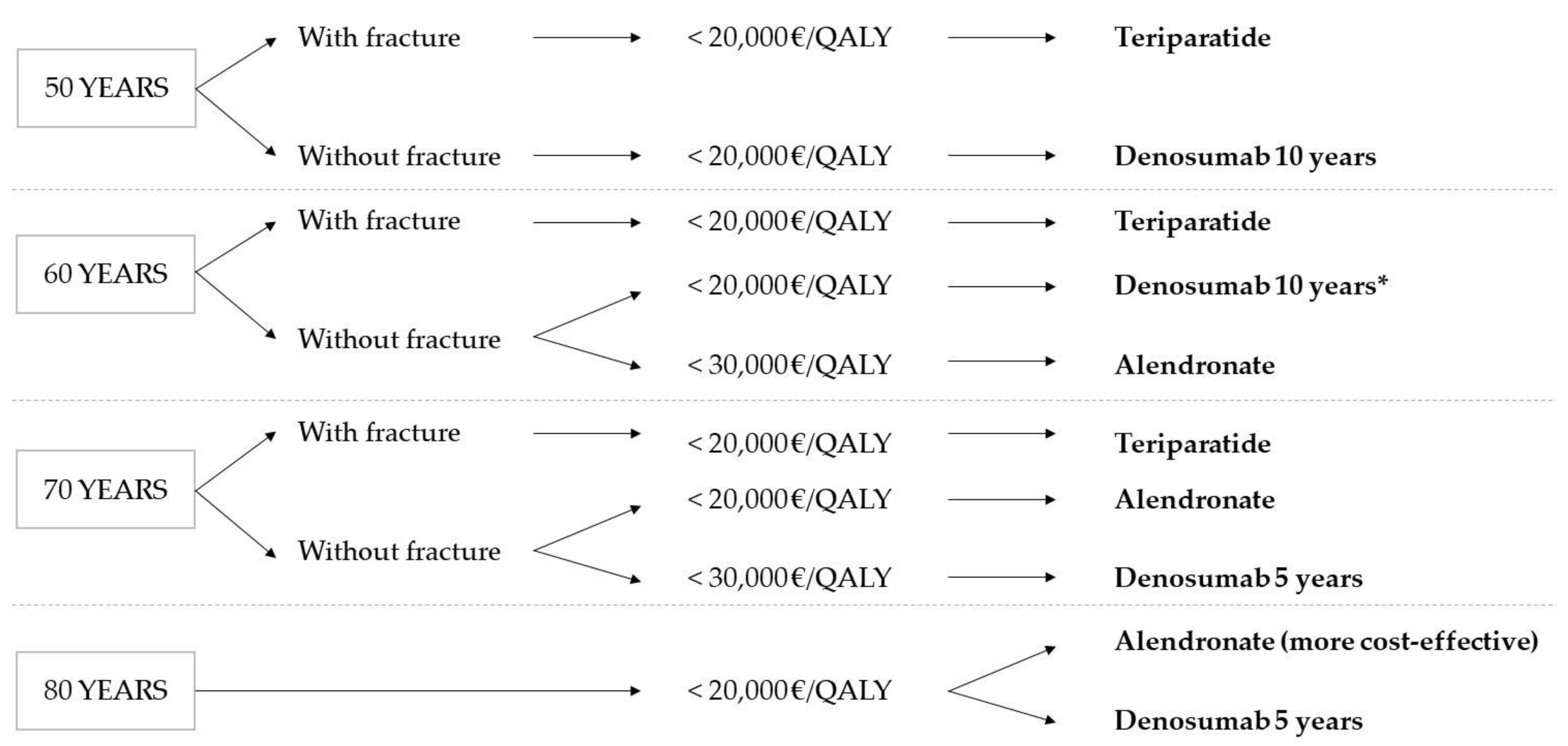
3. Results
3.1. Sensitivity Analysis
3.1.1. Denosumab for 10 Years
3.1.2. Teriparatide Given at the Start of the Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kanis, J.A.; on behalf of the World Healthy Organization Collaborating Centre for Metabolic Bone Diseases. Assessment of Osteoporosis at the Primary Health Care Level; University of Sheffield: Sheffield, UK, 2007. [Google Scholar]
- Osteoporosis: Assessing the Risk of Fragility Fracture; (NICE Clinical Guidelines, No. 146). National Institute for Health and Care Excellence (UK): London, UK, 2012. Available online: https://www.nice.org.uk/guidance/cg146 (accessed on 17 May 2021).
- Klotzbuecher, C.M.; Ross, P.D.; Landsman, P.B.; Abbott, T.A.; Berger, M. Patients with Prior Fractures Have an Increased Risk of Future Fractures: A Summary of the Literature and Statistical Synthesis. J. Bone Miner. Res. 2010, 15, 721–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanis, J.; Johnell, O.; De Laet, C.; Johansson, H.; Oden, A.; Delmas, P.; Eisman, J.; Fujiwara, S.; Garnero, P.; Kroger, H.; et al. A meta-analysis of previous fracture and subsequent fracture risk. Bone 2004, 35, 375–382. [Google Scholar] [CrossRef]
- Christodoulou, C.; Cooper, C. What is osteoporosis? Postgrad. Med. J. 2002, 79, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A.; Johnell, O. Requirements for DXA for the management ofosteoporosis in Europe. Osteoporos. Int. 2005, 16, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Viktoria Stein, K.; Dorner, T.; Lawrence, K.; Kunze, M. Economic concepts for measuring the costs of illness of osteoporosis: An international comparison. Wien. Med. Wochenschr. 2009, 159, 253–261. [Google Scholar] [CrossRef]
- Hernlund, E.; Svedbom, A.; Ivergard, M.; Compston, J.; Cooper, C.; Stenmark, J.; McCloskey, E.V.; Jonsson, B.; Kanis, J.A. Osteoporosis in the European Union: Medical management, epidemiology and economic Burden: A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch. Osteoporos. 2013, 8, 136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Cock, E.; Miravitlles, M.; González-Juanatey, J.R.; Azanza-Perea, J.R. Valor umbral del coste por año de vida ganado para recomendar la adopción de tecnologías sanitarias en España: Evidencias procedentes de una revisión de la literatura. PharmacoEcon. Span. Res. Artic. 2007, 4, 97–107. [Google Scholar] [CrossRef]
- Svedbom, A.; Hernlund, E.; Ivergård, M.; Compston, J.; Cooper, C.; Stenmark, J.; McCloskey, E.V.; Jönsson, B.; Kanis, J.A.; the EU review panel of the IOF. Osteoporosis in the European Union: A compendium of country-specific reports. Arch. Osteoporos. 2013, 8, 1–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, D.M.; Thompson, D.E.; Bauer, D.C.; Ensrud, K.; Musliner, T.; Hochberg, M.C.; Nevitt, M.C.; Suryawanshi, S.; Cummings, S.R. Fracture Risk Reduction with Alendronate in Women with Osteoporosis: The Fracture Intervention Trial. J. Clin. Endocrinol. Metab. 2000, 85, 4118–4124. [Google Scholar] [CrossRef]
- Harris, S.T.; Watts, N.B.; Genant, H.K.; Mckeever, C.D.; Hangartner, T.; Keller, M.; Iii, C.H.C.; Brown, J.; Miller, P.D.; Page, P. Effects of Risedronate Treatment on Vertebral and Nonvertebral Fractures in women with postmenopausal osteoporosis. J. Am. Med. Assoc. 1999, 282, 1344–1352. [Google Scholar] [CrossRef] [Green Version]
- Boonen, S.; Adachi, J.D.; Man, Z.; Cummings, S.R.; Lippuner, K.; Törring, O.; Gallagher, J.C.; Farrerons, J.; Wang, A.; Franchimont, N.; et al. Treatment with Denosumab Reduces the Incidence of New Vertebral and Hip Fractures in Postmenopausal Women at High Risk. J. Clin. Endocrinol. Metab. 2011, 96, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Pang, Y.; Shi, Y.; Xu, M.; Xu, X.; Zhang, J.; Ji, L.; Zhao, D. Indirect comparison of teriparatide, denosumab, and oral bisphosphonates for the prevention of vertebral and nonvertebral fractures in postmenopausal women with osteoporosis. Menopause 2015, 22, 1021–1025. [Google Scholar] [CrossRef]
- Fahrleitner-Pammer, A.; Langdahl, B.L.; Marin, F.; Jakob, F.; Karras, D.; Barrett, A.; Ljunggren, Ö.; Walsh, J.B.; Rajzbaum, G.; Barker, C.; et al. Fracture rate and back pain during and after discontinuation of teriparatide: 36-month data from the European Forsteo Observational Study (EFOS). Osteoporos. Int. 2011, 22, 2709–2719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comité de Expertos de la SEIOMM. La Guías de Práctica Clínica en la osteoporosis posmenopaáusica, glucocorticoidea y del Varón. Sociedad Española de investigación Ósea y del metabolismo mineral. Rev. Clín. Esp. 2014, 208, 1–153. [Google Scholar]
- Etxebarria-Foronda, I.; Caeiro-Rey, J.R.; Larrainzar-Garijo, R.; Vaquero-Cervino, E.; Roca-Ruiz, L.; Mesa-Ramos, M.; Merino Pérez, J.; Carpintero-Benítez, P.; Fernández Cebrián, A.; Gil-Garay, E. Guía SECOT-GEIOS en osteoporosis y fractura por fragilidad. Actualización/SECOT-GEIOS guidelines in osteoporosis and fragility fracture. An update. Rev. Esp. Cir. Ortop. Traumatol. 2015, 59, 373–393. [Google Scholar] [CrossRef] [PubMed]
- Borgström, F.; Carlsson, A.; Sintonen, H.; Boonen, S.; Haentjens, P.; Burge, R.; Johnell, O.; Jönsson, B.; Kanis, J.A. The cost-effectiveness of risedronate in the treatment of osteoporosis: An international perspective. Osteoporos. Int. 2006, 17, 996–1007. [Google Scholar] [CrossRef]
- Ström, O.; Borgström, F.; Sen, S.S.; Boonen, S.; Haentjens, P.; Johnell, O.; Kanis, J.A. Cost-effectiveness of alendronate in the treatment of postmenopausal women in 9 European countries—An economic evaluation based on the fracture intervention trial. Osteoporos. Int. 2007, 18, 1047–1061. [Google Scholar] [CrossRef] [PubMed]
- Imaz-Iglesia, I.; Rubio-Gonzalez, B.; Lopez-Delgado, M.E.; Amate, J.M.; Gomez-Pajuelo, P.; Gonzalez-Enriquez, J.; Agencia de Evaluación de Tecnologías Sanitarias (AETS), Instituto de Salud Carlos III—Ministerio de Ciencia e Innovación. Análisis Coste-Utilidad de los Tratamientos Farmacológicos para la prevención de Fracturas en Mujeres con Osteoporosis en ESPAÑA; IPE 63/2010; AETS—Instituto de Salud Carlos III: Madrid, Spain, December 2010.
- Darba, J.; Kaskens, L.; Sorio, F.; Lothgren, M. Cost-utility of denosumab for the treatment of postmenopausal osteoporosis in Spain. Clin. Outcomes Res. 2015, 7, 105–117. [Google Scholar] [CrossRef] [Green Version]
- Hart, W.M.; Rubio-Terrés, C.; Burrell, A.; Arístegui, I.; Escobar-Jiménez, F. Análisis farmacoeconómico del tratamiento de la osteoporosis postmenopáusica con risedronato o alendronato. Rev. Esp. Enferm. Metab. Oseas 2002, 11, 97–104. [Google Scholar]
- Cortés, J.-C.; Navarro-Quiles, A.; Romero, J.-V.; Roselló, M.-D. Randomizing the parameters of a Markov chain to model the stroke disease: A technical generalization of established computational methodologies towards improving real applications. J. Comput. Appl. Math. 2017, 324, 225–240. [Google Scholar] [CrossRef] [Green Version]
- Barrachina-Martínez, I.; Navarro-Quiles, A.; Ramos, M.; Romero, J.-V.; Roselló, M.-D.; Vivas-Consuelo, D. Probabilistic Study of the Effect of Anti-Epileptic Drugs Under Uncertainty: Cost-Effectiveness Analysis. Mathematics 2020, 8, 1120. [Google Scholar] [CrossRef]
- Herdman, M.; Badia, X.; Berra, S. El EuroQol-5D: Una alternativa sencilla para la medición de la calidad de vida relacionada con la salud en atención primaria. Atención Primaria 2001, 28, 425–429. [Google Scholar] [CrossRef] [Green Version]
- Vilagut, G.; Valderas, J.M.; Ferrer, M.; Garin, O.; López-García, E.; Alonso, J. Interpretación de los cuestionarios de salud SF-36 y SF-12 en España: Componentes físico y mental. Med. Clin. 2008, 130, 726–735. [Google Scholar] [CrossRef] [Green Version]
- Bastida, J.L.; Oliva, J.; Antoñanzas, F.; García-Altés, A.; Gisbert, R.; Mar, J.; Puig-Junoy, J. Propuesta de guía para la evaluación económica aplicada a las tecnologías sanitarias. Gac. Sanit. 2010, 24, 154–170. [Google Scholar] [CrossRef] [Green Version]
- Compston, J.; Cooper, A.; Cooper, C.; Gittoes, N.; Gregson, C.; Harvey, N.; Hope, S.; Kanis, J.A.; McCloskey, E.V.; Poole, K.E.S.; et al. UK clinical guideline for the prevention and treatment of osteoporosis. Arch. Osteoporos. 2017, 12, 43. [Google Scholar] [CrossRef]
- Hernández, A.N.; del Campo Fontecha, P.D.; Acín, M.P.A.; Rodríguez, L.A.; Burgos, E.C.; Castañeda, S.; Aresté, J.F.; Gifre, L.; Vaquero, C.G.; Rodríguez, G.C.; et al. Recomendaciones de la Sociedad Española de Reumatología sobre osteoporosis. Reumatol. Clínica 2019, 15, 188–210. [Google Scholar] [CrossRef] [PubMed]
- Pinto, J.L.; Rodríguez, R. Cuánto Vale la Pena Gastarse para Ganar un Año de Vida Ajustado por la Calidad? Un Estudio empírIco. En: El Valor Monetario de la Salud; Springer: Barcelona, Spain, 2001. [Google Scholar]
- Sacristán, J.; Oliva-Moreno, J.; Del Llano, J.; Prieto, L.; Pinto, J. ¿Qué es una tecnología sanitaria eficiente en España? Gac. Sanit. 2002, 16, 334–343. [Google Scholar] [CrossRef] [Green Version]
- Bone, H.G.; Wagman, R.B.; Brandi, M.L.; Brown, J.P.; Chapurlat, R.; Cummings, S.R.; Czerwiński, E.; Fahrleitner-Pammer, A.; Kendler, D.L.; Lippuner, K.; et al. 10 years of denosumab treatment in postmenopausal women with osteoporosis: Results from the phase 3 randomised FREEDOM trial and open-label extension. Lancet Diabetes Endocrinol. 2017, 5, 513–523. [Google Scholar] [CrossRef]
- Davis, S.; Simpson, E.; Hamilton, J.; James, M.M.-S.; Rawdin, A.; Wong, R.; Goka, E.; Gittoes, N.; Selby, P. Denosumab, raloxifene, romosozumab and teriparatide to prevent osteoporotic fragility fractures: A systematic review and economic evaluation. Health Technol. Assess. 2020, 24, 1–314. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Patrones de Mortalidad en España, 2016; Ministerio de Sanidad, Servicios Sociales e Igualdad: Madrid, Spain, 2019. [Google Scholar]
- Abimanyi-Ochom, J.; Watts, J.J.; Borgström, F.; Nicholson, G.; Shore-Lorenti, C.; Stuart, A.L.; Zhang, Y.; Iuliano, S.; Seeman, E.; Prince, R.; et al. Changes in quality of life associated with fragility fractures: Australian arm of the International Cost and Utility Related to Osteoporotic Fractures Study (AusICUROS). Osteoporos. Int. 2015, 26, 1781–1790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cramer, J.A.; Roy, A.; Burrell, A.; Fairchild, C.J.; Fuldeore, M.J.; Ollendorf, D.A.; Wong, P.K. Medication Compliance and Persistence: Terminology and Definitions. Value Health 2008, 11, 44–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mori, T.; Crandall, C.J.; Ganz, D.A. Cost-effectiveness of denosumab versus oral alendronate for elderly osteoporotic women in Japan. Osteoporos. Int. 2017, 28, 1733–1744. [Google Scholar] [CrossRef] [PubMed]
- Parthan, A.; Kruse, M.; Agodoa, I.; Silverman, S.; Orwoll, E. Denosumab: A cost-effective alternative for older men with osteoporosis from a Swedish payer perspective. Bone 2014, 59, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Parthan, A.; Kruse, M.; Yurgin, N.; Huang, J.; Viswanathan, H.N.; Taylor, U. Cost Effectiveness of Denosumab versus Oral Bisphosphonates for Postmenopausal Osteoporosis in the US. Appl. Health Econ. Health Policy 2013, 11, 485–497. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Zheng, B.; Liu, M.; Zhou, H.; Zhao, L.; Cai, H.; Huang, J. Cost-effectiveness of antiosteoporosis strategies for postmenopausal women with osteoporosis in China. Menopause 2019, 26, 906–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tosteson, A.N.A.; Melton, L.J.; Dawson-Hughes, B.; Baim, S.; Favus, M.J.; Khosla, S.; Lindsay, R.L. Cost-effective osteoporosis treatment thresholds: The United States perspective. Osteoporos. Int. 2008, 19, 437–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makras, P.; Athanasakis, K.; Boubouchairopoulou, N.; Rizou, S.; Anastasilakis, A.D.; Kyriopoulos, J.; Lyritis, G.P. Cost-effective osteoporosis treatment thresholds in Greece. Osteoporos. Int. 2015, 26, 1949–1957. [Google Scholar] [CrossRef] [PubMed]
- Pueyo, M.J.; Larrosa, M.; Surís, X.; Garcia-Ruiz, A.J. Análisis de coste-utilidad e impacto presupuestario de la prevención primaria con alendronato de la fractura osteoporótica de cadera en Cataluña. Reumatol. Clín. 2012, 8, 128–134. [Google Scholar] [CrossRef]
- González, D.J.; Marco, G.M.; Henríquez, S.M. Coste anual de los fármacos utilizados en el tratamiento de la osteoporosis tras la revisión de los precios de referencia Bibliografía. Rev. Osteoporos. Metab. Miner. 2012, 41, 43–44. [Google Scholar]
- Braithwaite, R.S.; Meltzer, D.O.; King, J.T.; Leslie, D.; Roberts, M.S. What Does the Value of Modern Medicine Say About the $50,000 per Quality-Adjusted Life-Year Decision Rule? Med. Care 2008, 46, 349–356. [Google Scholar] [CrossRef]
- Rawlins, M.D.; Culyer, A.J. Education and debate. National Institute for Clinical Excellence and ist value judgments. BMJ 2004, 329, 224–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devlin, N.; Parkin, D. Does NICE have a cost-effectiveness threshold and what other factors influence its decisions? A binary choice analysis. Health Econ. 2004, 13, 437–452. [Google Scholar] [CrossRef]
- Murray, C.J.; Evans, D.B.; Acharya, A.; Baltussen, R.M. Development of WHO guidelines on generalized cost-effectiveness analysis. Health Econ. 2000, 9, 235–251. [Google Scholar] [CrossRef]
- Murphy, D.R.; Smolen, L.J.; Klein, T.M.; Klein, R.W. The cost effectiveness of teriparatide as a first-line treatment for glucocorticoid-induced and postmenopausal osteoporosis patients in Sweden. BMC Musculoskelet. Disord. 2012, 13, 213. [Google Scholar] [CrossRef] [Green Version]
- Taheri, S.; Fashami, F.M.; Peiravian, F.; Yousefi, P. Teriparatide in the Treatment of Severe Postmenopausal Osteoporosis: A Cost-Utility Analysis. Iran. J. Pharm. Res 2019, 18, 1073–1085. [Google Scholar]
- Silverman, S.; Agodoa, I.; Kruse, M.; Parthan, A.; Orwoll, E. Denosumab for elderly men with osteoporosis: A cost-effectiveness analysis from the us payer perspective. J. Bone Miner. Res. 2013, 28, 627631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seidner, M.; Institute for Clincial and Economic Review. Anabolic Therapies for Osteoporosis in Postmenopausal Women: Effectiveness and Value. 2017. Available online: https://icer-review.org/wp-con-tent/uploads/2016/11/CTAF_Osteoporosis_Final_Evidence (accessed on 17 May 2021).
- Mori, T.; Crandall, C.J.; Ganz, D.A. Cost-Effectiveness of Sequential Teriparatide/Alendronate Versus Alendronate-Alone Strategies in High-Risk Osteoporotic Women in the US: Analyzing the Impact of Generic/Biosimilar Teriparatide. JBMR Plus 2019, 3, e10233. [Google Scholar] [CrossRef] [Green Version]
- Yoshizawa, T.; Nishino, T.; Okubo, I.; Yamazaki, M. Cost-effectiveness analysis of drugs for osteoporosis treatment in elderly Japanese women at high risk of fragility fractures: Comparison of denosumab and weekly alendronate. Arch. Osteoporos. 2018, 13, 94. [Google Scholar] [CrossRef]
- Karnon, J.; Shafie, A.S.; Orji, N.; Usman, S.K. What are we paying for? A cost-effectiveness analysis of patented denosumab and generic alendronate for postmenopausal osteoporotic women in Australia. Cost Eff. Resour. Alloc. 2016, 14, 11. [Google Scholar] [CrossRef] [Green Version]
- Freemantle, N.; Satram-Hoang, S.; Tang, E.-T.; Kaur, P.; Macarios, D.; Siddhanti, S.; Borenstein, J.; Kendler, D.L. Final results of the DAPS (Denosumab Adherence Preference Satisfaction) study: A 24-month, randomized, crossover comparison with alendronate in postmenopausal women. Osteoporos. Int. 2012, 23, 317–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiligsmann, M.; Reginster, J.-Y. Cost-effectiveness of gastro-resistant risedronate tablets for the treatment of postmenopausal women with osteoporosis in France. Osteoporos. Int. 2019, 30, 649–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| AGE (Years) | Hip Women | Hip Men | Vertebral Women | Vertebral Men | Wrist Women | Wrist Men | Others Women | Others Men |
|---|---|---|---|---|---|---|---|---|
| 50–54 | 8 | 5 | 21 | 14 | 51 | 5 | 53 | 23 |
| 55–59 | 24 | 17 | 65 | 30 | 181 | 26 | 207 | 159 |
| 60–64 | 44 | 42 | 78 | 102 | 166 | 80 | 170 | 417 |
| 65–69 | 75 | 54 | 110 | 85 | 183 | 81 | 258 | 347 |
| 70–74 | 179 | 103 | 253 | 157 | 322 | 66 | 508 | 527 |
| 75–79 | 386 | 190 | 375 | 219 | 376 | 54 | 811 | 507 |
| 80–84 | 858 | 387 | 540 | 269 | 537 | 75 | 1460 | 1029 |
| >85 | 1709 | 811 | 804 | 545 | 729 | 149 | 2870 | 2349 |
| Location of Previous Fracture | Location of Subsequent Fracture | ||||
|---|---|---|---|---|---|
| Wrist | Vertebral | Others | Hip | All | |
| Wrist | 3.3 | 1.7 | 2.4 | 1.9 | 2.0 |
| Vertebral | 1.4 | 4.4 | 1.8 | 2.3 | 1.9 |
| Others | 1.8 | 1.9 | 1.9 | 2.0 | 1.9 |
| Hip | 1.9 * | 2.5 | 1.9 | 2.3 | 2.4 |
| All | 1.9 | 2.0 | 1.9 | 2.0 | 2.0 |
| Value | Range | Reference | |
|---|---|---|---|
| Teriparatide | |||
| Efficacy (hazard ratio) | |||
| Hip fracture | 0.35 | 0.15–0.73 | [33] |
| Clinical vertebral fracture | 0.23 | 0.16–0.32 | [33] |
| Wrist fracture | 0.66 | 0.33–1.26 | [33] |
| Other osteoporotic fracture | 0.58 | 0.45–0.66 | [33] |
| Treatment duration (years) | 2 | ||
| Alendronate | |||
| Efficacy (hazard ratio) | |||
| Hip fracture | 0.64 | 0.45–0.88 | [33] |
| Clinical vertebral fracture | 0.50 | 0.40–0.64 | [33] |
| Wrist fracture | 0.83 | 0.51–1.30 | [33] |
| Other osteoporotic fracture | 0.77 | 0.64–0.90 | [33] |
| Treatment duration (years) | 5 | ||
| Denosumab | |||
| Efficacy (hazard ratio) | |||
| Hip fracture | 0.56 | 0.31–0.94 | [33] |
| Clinical vertebral fracture | 0.30 | 0.23–0.43 | [33] |
| Wrist fracture * | 0.86 | 0.69–1.12 | [33] |
| Other osteoporotic fracture | 0.86 | 0.69–1.12 | [33] |
| Treatment duration (years) | 5 | ||
| Risedronate | |||
| Efficacy (hazard ratio) | |||
| Hip fracture | 0.66 | 0.46–0.99 | [33] |
| Clinical vertebral fracture | 0.52 | 0.42–0.65 | [33] |
| Wrist fracture | 0.82 | 0.50–1.30 | [33] |
| Other osteoporotic fracture | 0.73 | 0.59–0.88 | [33] |
| Treatment duration (years) | 5 | ||
| Costs (2018 Euros) | |||
| Formal health care sector (Euros) | |||
| Alendronate, annual | 147.28 | ||
| Denosumab, annual | 418.48 | ||
| Risedronate, annual | 258.65 | ||
| Teriparatide, annual | 4888.10 | ||
| Treatment costs ** (Euros) | |||
| Hip fracture, first year | |||
| 50–64 years | 11,758.00 | [20] | |
| 65–74 years | 12,592.00 | [20] | |
| 75–84 years | 13,613.00 | [20] | |
| 85–100 years | 19,887.00 | [20] | |
| Hip fracture, second year and subsequent | |||
| 50–64 years | 4874.00 | [20] | |
| 65–74 years | 5062.00 | [20] | |
| 75–84 years | 4782.00 | [20] | |
| 85–100 years | 7329.00 | [20] | |
| Clinical vertebral fracture | |||
| 50–64 years | 4382.00 | [20] | |
| 65–100 years | 15,016.00 | [20] | |
| Wrist fracture, first year | 2277.00 | [20] | |
| Other osteoporotic fracture | 2277.00 | [20] |
| Age | Hip Fracture | Vertebral Fracture | Other Fractures |
|---|---|---|---|
| 50–54 | 1130 | 1379 | 20 |
| 55–59 | 1273 | 1471 | 28 |
| 60–64 | 1649 | 1806 | 46 |
| 65–69 | 1970 | 2041 | 71 |
| 70–74 | 2419 | 2360 | 109 |
| 75–79 | 3089 | 2818 | 186 |
| 80–84 | 3669 | 3062 | 339 |
| 85–89 | 4886 | 3640 | 627 |
| >90 | 6273 | 3958 | 1100 |
| Age | Mortality Rate × 100,000 Inhabitants for Both Sexes |
|---|---|
| 50–54 | 294.43 |
| 55–59 | 455.74 |
| 60–64 | 692.86 |
| 65–69 | 1023.48 |
| 70–74 | 1568.69 |
| 75–79 | 2731.29 |
| 80–84 | 4998.71 |
| >85 | 13,116.13 |
| Type of Fracture | Moment of Fracture | At 12 Months Post-Fracture |
|---|---|---|
| Hip | 0.26 | 0.74 |
| Wrist | 0.58 | --- |
| Vertebral | 0.43 | 0.73 |
| Other fractures | 0.37 | --- |
| Strategy | Annual Cost (Euros) (a) | Incremental Annual cost (Euros) (b) = (a) − Control | Utility (QALYs) (c) | Incremental Utility (QALYs) (d) = (c) − Control | ICER (e) = (b)/(d) | Incremental Utility (QALYs) (f) = (c) − (c*) | ICER (g) = (b)/(f) | Dominance |
|---|---|---|---|---|---|---|---|---|
| Starting age 50 | ||||||||
| No intervention (control) | 3183.37 | 0.00 | 19.6667 | 0.0000 | 0.00 | −0.0082 (Teriparatide) | −15,586.74 | Dominated |
| Teriparatide | 3054.80 | −128.56 | 19.6749 | 0.0082 | −15,586.74 | 0.0000 (Teriparatide) | 0.00 | - |
| Alendronate | 3821.32 | 637.95 | 19.6744 | 0.0077 | 82,662.94 | −0.0005 (Teriparatide) | −1,443,877.15 | Dominated |
| Risedronate | 4335.63 | 1152.26 | 19.6744 | 0.0077 | 150,216.55 | −0.0006 (Teriparatide) | −2,217,253.75 | Dominated |
| Denosumab | 5066.16 | 1882.80 | 19.6761 | 0.0094 | 200,005.65 | 0.0012 (Teriparatide) | 1,725,951.35 | - |
| Starting age 60 | ||||||||
| No intervention (control) | 4085.46 | 0.00 | 15.7688 | 0.0000 | 0.00 | −0.0114 (Teriparatide) | −14,173.67 | Dominated |
| Teriparatide | 3923.98 | −161.48 | 15.7802 | 0.0114 | −14,173.67 | 0.000 | 0.00 | - |
| Alendronate | 4618.54 | 533.08 | 15.7886 | 0.0199 | 26,838.09 | 0.0085 (Teriparatide) | 81,999.39 | - |
| Risedronate | 5129.66 | 1044.20 | 15.7885 | 0.0198 | 52,846.09 | −0.0001 (Alendronate) | −4,933,710.38 | Dominated |
| Denosumab | 5832.93 | 1747.47 | 15.7927 | 0.0240 | 72,905.15 | 0.0041 (Alendronate) | 295,745.24 | - |
| Starting age 70 | ||||||||
| No intervention (control) | 4921.87 | 0.00 | 11.2751 | 0.0000 | 0.00 | −0.0159 (Teriparatide) | −13,850.43 | Dominated |
| Teriparatide | 4701.44 | −220.43 | 11.2910 | 0.0159 | −13,850.43 | 0.0000 | 0.00 | - |
| Alendronate | 5162.58 | 240.71 | 11.3162 | 0.0411 | 5854.99 | 0.0252 (Teriparatide) | 18,301.50 | - |
| Risedronate | 5669.80 | 747.93 | 11.3158 | 0.0407 | 18,379.85 | −0.0004 (Alendronate) | −1,209,891.07 | Dominated |
| Denosumab | 6280.28 | 1358.41 | 11.3248 | 0.0496 | 27,372.36 | 0.0085 (Alendronate) | 131,266.50 | - |
| Starting age 80 | ||||||||
| No intervention (control) | 5136.44 | 0.00 | 6.5968 | 0.0000 | 0.00 | −0.0773 (Alendronate) | −6449.00 | Dominated |
| Teriparatide | 4876.26 | −260.18 | 6.6186 | 0.0217 | −11,973.75 | −0.0556 (Alendronate) | −4289.55 | Dominated |
| Alendronate | 4637.80 | −498.65 | 6.6742 | 0.0773 | −6449.00 | 0.0000 | 0.00 | - |
| Risedronate | 5109.83 | −26.61 | 6.6741 | 0.0773 | −344.42 | −0.0001 (Alendronate) | −7,423,931.48 | Dominated |
| Denosumab | 5488.50 | 352.06 | 6.6853 | 0.0884 | 3982.26 | 0.0111 (Alendronate) | 76,739.95 | - |
| Strategy | Annual Cost (Euros) (a) | Incremental Annual Cost (Euros) (b) = (a) − Control | Utility (QALYs) (c) | Incremental Utility (QALYs) (d) = (c) − Control | ICER (e) = (b)/(d) | Incremental Utility (QALYs) (f) = (c) − (c*) | ICER (g) = (b)/(f) | Dominance |
|---|---|---|---|---|---|---|---|---|
| Non-intervention (control) | 3183.37 | 0.00 | 19.6667 | 0.0000 | 0.00 | −0.0082 (Teriparatide) | −15,586.74 | Dominated |
| Teriparatide | 3054.80 | −128.56 | 19.6749 | 0.0082 | −15,586.74 | 0.0000 (Teriparatide) | 0.00 | - |
| Alendronate | 3821.32 | 637.95 | 19.6744 | 0.0077 | 82,662.94 | −0.0005 (Teriparatide) | −1,443,877.15 | Dominated |
| Risedronate | 4337.28 | 1153.91 | 19.6744 | 0.0077 | 150,431.72 | −0.0006 (Teriparatide) | −2,220,110.96 | Dominated |
| Denosumab | 5630.65 | 2447.28 | 19.8440 | 0.1774 | 13,799.04 | 0.1691 (Teriparatide) | 15,232.39 | - |
| Strategy | Annual Cost (Euros) (a) | Incremental Annual Cost (Euros) (b) = (a) − Control | Utility (QALYs) (c) | Incremental Utility (QALYs) (d) = (c) − Control | ICER (e) = (b)/(d) | Incremental Utility (QALYs) (f) = (c) − (c*) | ICER (g) = (b)/(f) | Dominance |
|---|---|---|---|---|---|---|---|---|
| Non-intervention (control) | 3183.37 | 0.00 | 19.6667 | 0.0000 | 0.00 | −0.0000 | 0.00 | - |
| Teriparatide | 12,621.64 | 9438.27 | 19.6716 | 0,0049 | 1,937,157.55 | −0.0045 (Denosumab) | −1,663,652.17 | Dominated |
| Alendronate | 3821.32 | 637.95 | 19.6744 | 0.0077 | 82,662.94 | −0.0077 (Non-intervention) | 82,662.94 | - |
| Risedronate | 4335.63 | 1152.26 | 19.6744 | 0.0077 | 150,215.80 | −0.0000 (Alendronate) | −10,991,760.24 | Dominated |
| Denosumab | 5066.16 | 1882.79 | 19.6761 | 0.0094 | 200,004.81 | 0.0017 (Alendronate) | 15,232.39 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osca-Guadalajara, M.; Díaz-Carnicero, J.; González-de-Julián, S.; Vivas-Consuelo, D. Markov Models for Economic Evaluation in Osteoporosis Treatment. Mathematics 2021, 9, 2331. https://doi.org/10.3390/math9182331
Osca-Guadalajara M, Díaz-Carnicero J, González-de-Julián S, Vivas-Consuelo D. Markov Models for Economic Evaluation in Osteoporosis Treatment. Mathematics. 2021; 9(18):2331. https://doi.org/10.3390/math9182331
Chicago/Turabian StyleOsca-Guadalajara, Marta, Javier Díaz-Carnicero, Silvia González-de-Julián, and David Vivas-Consuelo. 2021. "Markov Models for Economic Evaluation in Osteoporosis Treatment" Mathematics 9, no. 18: 2331. https://doi.org/10.3390/math9182331