
Kidney Transplant: Survival Analysis and Prognostic Factors after 10 Years of Follow-Up
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analysis
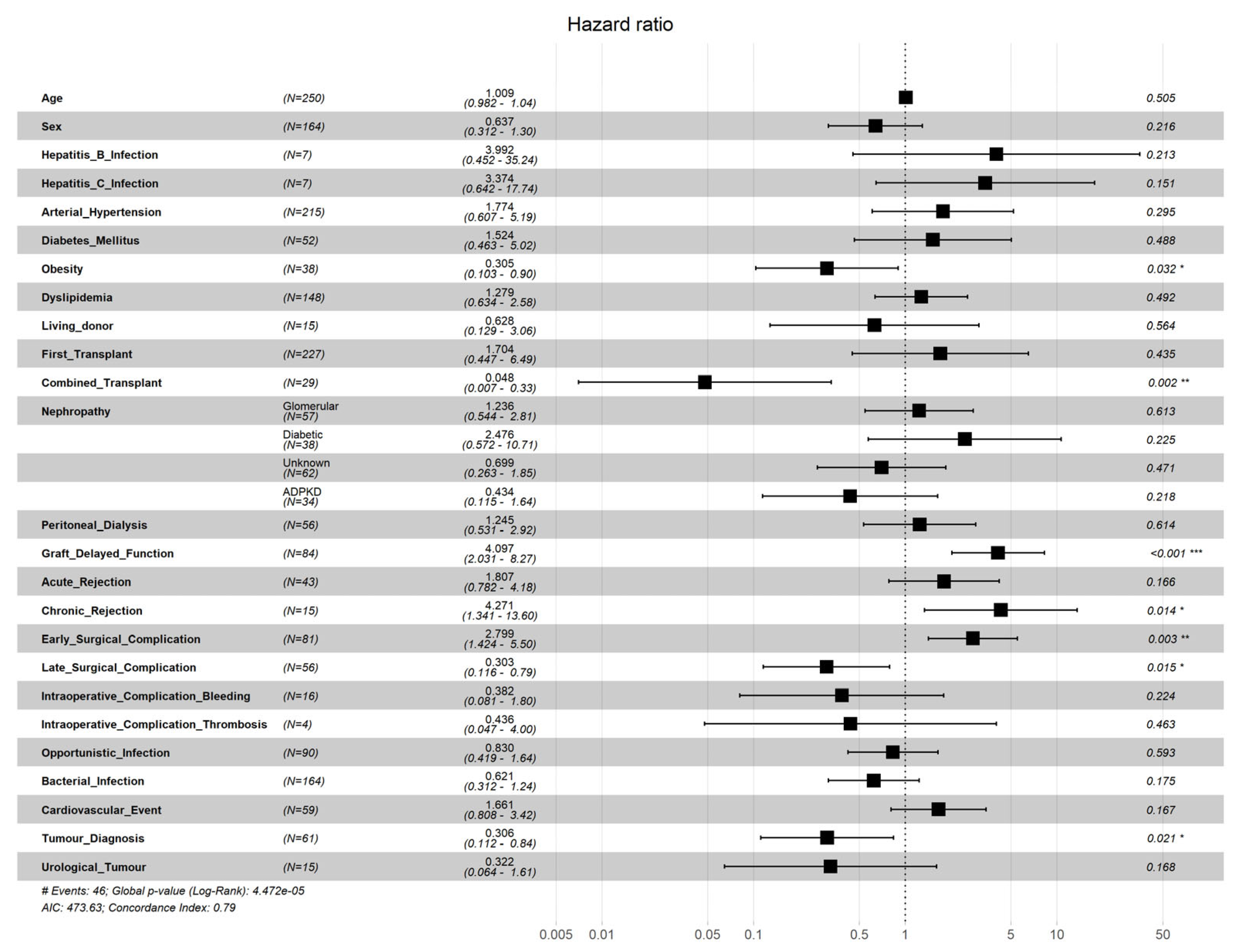
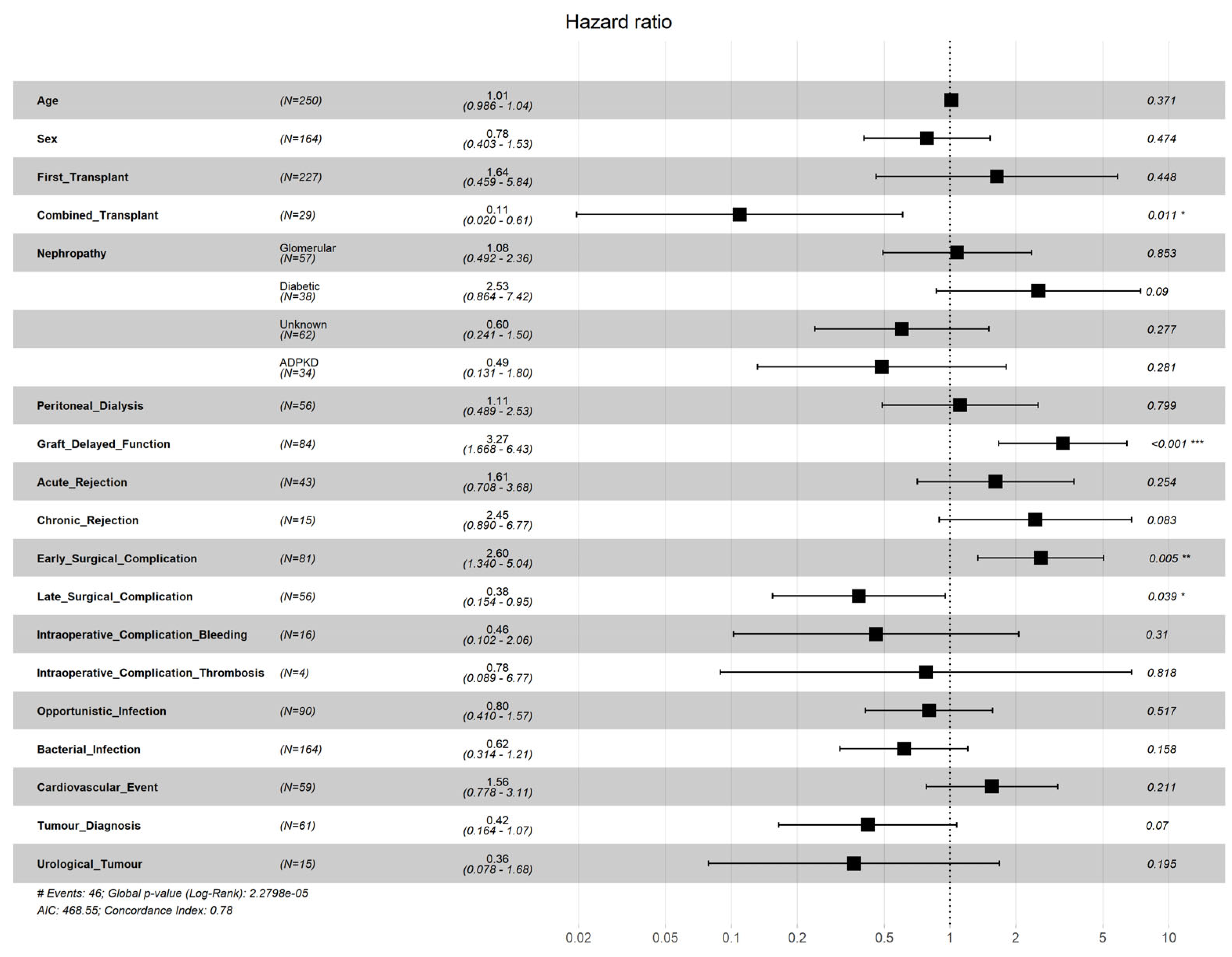
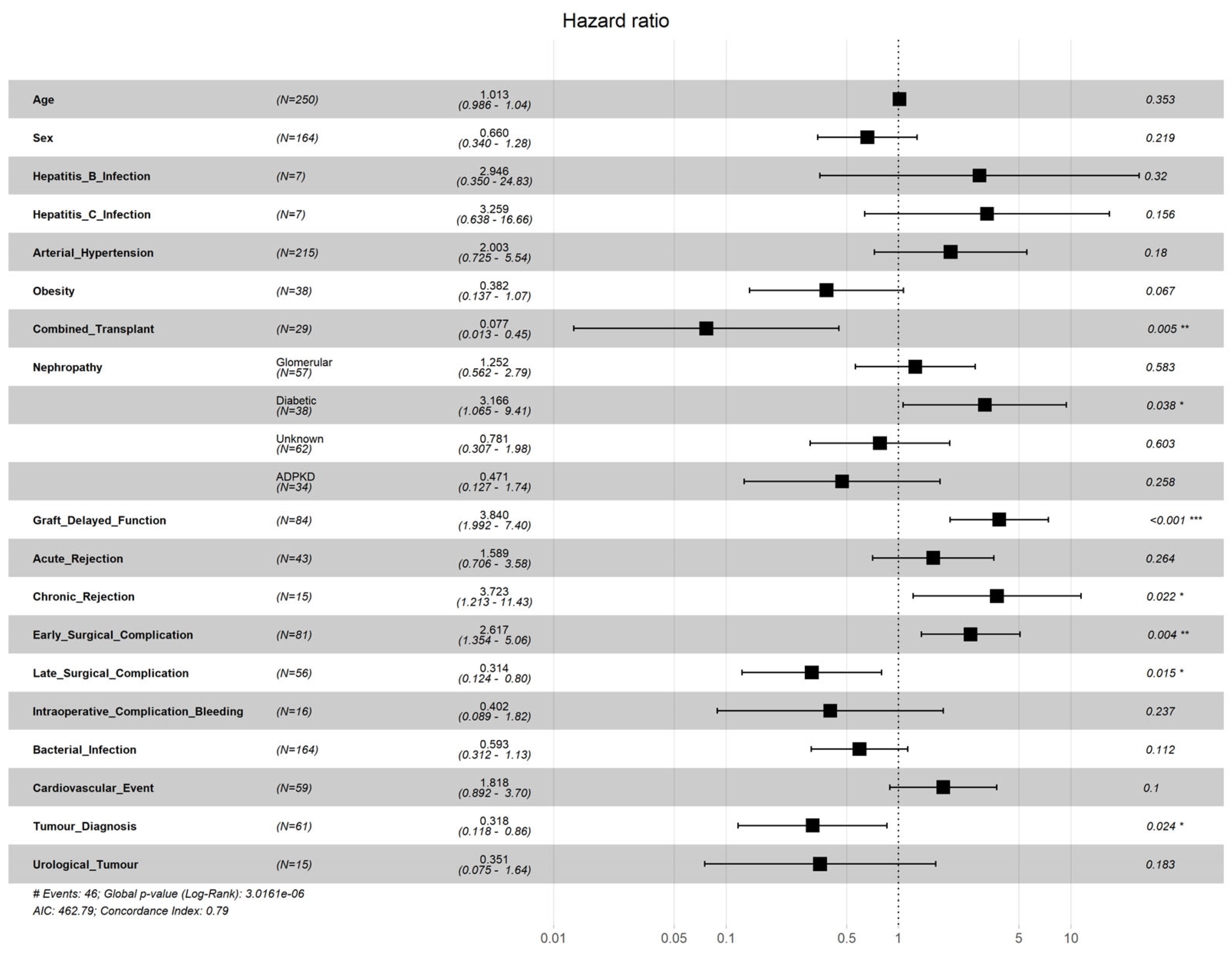
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Axelrod, D.A.; Schnitzler, M.A. An economic assessment of contemporary kidney transplant practice. Am. J. Transpl. 2018, 18, 1168–1176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Querard, A.H.; Foucher, Y. Comparison of survival outcomes between Expanded Criteria Donor and Standard Criteria Donor kidney transplant recipients: A systematic review and meta-analysis. Transpl. Int. 2016, 29, 403–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfe, R.A.; Ashby, V.B. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Organización Nacional de Trasplantes. Ministerio de Sanidad. Balance de actividad del 2021. Comunicado de Prensa, 2021 Gen, Madrid. Available online: http://www.ont.es/Documents/Balance%20de%20actividad%20Donaci%C3%B3n%20y%20Trasplante%202021_ONT.pdf (accessed on 28 November 2022).
- Van Loon, E.; Senev, A. Assessing the Complex Causes of Kidney Allograft Loss. Transplantation 2020, 104, 2557–2566. [Google Scholar] [CrossRef] [PubMed]
- Gondos, A.; Döhler, B. Kidney Graft Survival in Europe and the United States. Strikingly Different Long-Term Outcomes. Transpl. J. 2013, 95, 267–274. [Google Scholar] [CrossRef]
- Douglas, S.K.; Demattos, A. Effect of donor recipient age match on survival after first deceased donor renal transplantation. J. Am. Soc. Nephrol. 2004, 15, 1086–1091. [Google Scholar]
- Morath, C.; Döhler, B. Pre-transplant HLA Antibodies and Delayed Graft Function in the Current Era of Kidney Transplantation. Front Immunol. 2020, 11, 1886. [Google Scholar] [CrossRef]
- Chih-Yuan, L.; Ching-Yao, Y. Prognostic factors for renal transplant graft survival in a retrospective cohort of 1000 cases: The role of desensitization therapy. J. Formos. Med. Assoc. 2020, 119, 829–837. [Google Scholar]
- Jeon, J.Y.; Kim, S.J. Trends in the effects of pre-transplant diabetes on mortality and cardiovascular events after kidney transplantation. J. Diabetes Investig. 2021, 12, 811–818. [Google Scholar] [CrossRef]
- Erturk, T.; Berber, I. Effect of Obesity on Clinical Outcomes of Kidney Transplant Patients. Transpl. Proc. 2019, 51, 1093–1095. [Google Scholar] [CrossRef]
- Fellmann, M.; Loïc, B. Effects of Obesity on Postoperative Complications and Graft Survival After Kidney Transplantation. Transpl. Proc. 2020, 52, 3153–3159. [Google Scholar] [CrossRef]
- Prezelin, M.; Combe, C. Prolonged dialysis duration is associated with graft failure and mortality after kidney transplantation: Results from the French transplant database. Nephrol. Dial. Transpl. 2019, 34, 538–545. [Google Scholar] [CrossRef]
- Torres, A.; Hernández, D. Randomized Controlled Trial Assessing the Impact of Tacrolimus Versus Cyclosporine on the Incidence of Posttransplant Diabetes Mellitus. Kidney Int. Rep. 2018, 3, 1304–1315. [Google Scholar] [CrossRef] [Green Version]
- Barba, J.; Rinco, A. Complicaciones quirúrgicas en el trasplante renal y su influencia en la supervivencia del injerto. Actas Urológicas Españolas 2010, 34, 266–273. [Google Scholar] [CrossRef]
- Kramer, A.; Pippias, M. The European Renal Association – European Dialysis and Transplant Association (ERA-EDTA) Registry Annual Report 2016: A summary. Clin. Kidney J. 2019, 12, 702–720. [Google Scholar] [CrossRef] [Green Version]
- Álvarez, L.E.; Martínez, P. Supervivencia del paciente y del injerto a largo plazo en receptores de trasplante renal. Rev. Med. Inst. Mex. Seguro Soc. 2019, 57, 348–356. [Google Scholar]
- Sexton, D.J.; O’Kelly, P. Progressive improvement in short-, medium- and long-term graft survival in kidney transplantation patients in Ireland—A retrospective study. Transpl. Int. 2019, 32, 974–984. [Google Scholar] [CrossRef] [PubMed]
- Saucedo, H.; Haakinson, D.J. Prognostic factors in kidney transplantation in the septuagenarian: A multicenter analysis. Clin. Transpl. 2016, 30, 828–835. [Google Scholar] [CrossRef]
- Gopalakrishnan, V.; Agarwal, S.K. Infection is the chief cause of mortality and non-death censored graft loss in the first year after renal transplantation in a resource limited population: A single centre study. Nephrology 2019, 24, 456–463. [Google Scholar] [CrossRef]
- Noguchi, H.; Kitada, H. Outcome of renal transplantation in patients with type 2 diabetic nephropathy: A single-center experience. Transpl. Proc. 2015, 47, 608–611. [Google Scholar] [CrossRef]
- Butala, N.M.; Reese, P.P. Is delayed graft function causally associated with long-term outcomes after kidney transplantation? Instrumental variable analysis. Transplantation 2013, 95, 1008–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redfield, R.R.; Scalea, J.R. Predictors and outcomes of delayed graft function after living-donor kidney transplantation. Transpl. Int. 2016, 29, 81–87. [Google Scholar] [CrossRef]
- Kim, S.J.; Lee, H.H. Prognostic factors affecting graft and patient survival in cadaveric and living kidney transplantation. Transpl. Proc. 2004, 36, 2038–2039. [Google Scholar] [CrossRef] [PubMed]
- Vnucak, M.; Granak, K. The impact of different induction immunosuppression protocols on patient survival, graft survival and acute graft rejection after kidney transplantation. Bratisl. Lek. Listy 2022, 123, 730–735. [Google Scholar] [CrossRef]
- Pillot, P.; Bardonnaud, N. Risk factors for surgical complications after renal transplantation and impact on patient and graft survival. Transpl. Proc. 2012, 44, 2803–2808. [Google Scholar] [CrossRef]
- Tisserand, B.; Doré, B. Impact à long terme des complications chirurgicales sur la survie du transplant rénal. Progrès Urol. 2013, 23, 113–120. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Variables | n (%) |
|---|---|
| Age at transplant in years [µ ± SD] | 52.3 ± 14.0 |
| Sex | |
| Female | 86 (34.4) |
| Male | 164 (65.6) |
| Comorbidity | n (%) |
| Arterial Hypertension | 215 (86.0) |
| Diabetes Mellitus | 52 (20.8) |
| Obesity | 38 (15.2) |
| Dyslipidemia | 148 (59.2) |
| Hepatitis B Virus Infection | 7 (2.8) |
| Hepatitis C Virus Infection | 7 (2.8) |
| Aetiology of Chronic Kidney Disease | |
| Glomerular Nephropathy | 57 (22.8) |
| Diabetic nephropathy | 38 (12.2) |
| Autosomal Dominant Polycystic Kidney Disease | 34 (13.6) |
| Unknown | 62 (24.8) |
| Renal Replacement Therapy | |
| Type 1 | |
| Haemodialysis | 159 (64.1) |
| Peritoneal dialysis | 48 (19.4) |
| Both | 34 (13.7) |
| Pre-dialysis | 7 (2.8) |
| Mean time (years) in replacement therapy [µ± SD] | 4.4 ± 4.2 |
| Type of Complication | n (%) |
|---|---|
| Intraoperative Complication | 31 (12.4) |
| Bleeding | 16 (6.4) |
| Thrombosis | 4 (1.6) |
| Early Surgical Complication | 81 (32.4) |
| Late Surgical Complication | 56 (22.4) |
| Acute Rejection | 42 (16.8) |
| Chronic Rejection | 15 (6.0) |
| Graft Delayed Function | 84 (33.6) |
| Opportunistic Infection | 90 (36.0) |
| Bacterial Infection | 164 (65.6) |
| Cardiovascular Event | 59 (23.6) |
| Tumour Diagnosis | 61 (24.4) |
| Urological Tumour | 15 (6.0) |
| Graft loss | 49 (19.6) |
| Death | 55 (22.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beviá-Romero, Á.; Quereda-Flores, F.; Díaz-Carnicero, J.; Gómez-Palomo, F.; Ramos-Cebrián, M.; Espinosa-Vañó, J.; Castillo-Antón, D.J.; Broseta-Rico, E.; Vivas-Consuelo, D.; Budía-Alba, A. Kidney Transplant: Survival Analysis and Prognostic Factors after 10 Years of Follow-Up. Mathematics 2023, 11, 1640. https://doi.org/10.3390/math11071640
Beviá-Romero Á, Quereda-Flores F, Díaz-Carnicero J, Gómez-Palomo F, Ramos-Cebrián M, Espinosa-Vañó J, Castillo-Antón DJ, Broseta-Rico E, Vivas-Consuelo D, Budía-Alba A. Kidney Transplant: Survival Analysis and Prognostic Factors after 10 Years of Follow-Up. Mathematics. 2023; 11(7):1640. https://doi.org/10.3390/math11071640
Chicago/Turabian StyleBeviá-Romero, Álvaro, Francisco Quereda-Flores, Javier Díaz-Carnicero, Francisco Gómez-Palomo, María Ramos-Cebrián, Joaquín Espinosa-Vañó, Dario J. Castillo-Antón, Enrique Broseta-Rico, David Vivas-Consuelo, and Alberto Budía-Alba. 2023. "Kidney Transplant: Survival Analysis and Prognostic Factors after 10 Years of Follow-Up" Mathematics 11, no. 7: 1640. https://doi.org/10.3390/math11071640