
Brain Tumor Segmentation Using a Patch-Based Convolutional Neural Network: A Big Data Analysis Approach

Abstract
:1. Introduction
- A big data analysis approach is employed for data preprocessing and enrichment, enhancing the quality of the medical data and improving the accuracy of the model.
- An early detection method and comparative analysis are provided to assist medical professionals in making accurate and timely diagnoses, thereby improving patient outcomes.
- The proposed method is compared with existing approaches and its advantages and limitations are highlighted.
2. Background
2.1. Brain Tumor Segmentation
2.2. Patch-Based Convolutional Neural Network
2.3. Big Data Analysis
2.4. Multi-Modal Brain Tumor Segmentation using a Patch-Based CNN
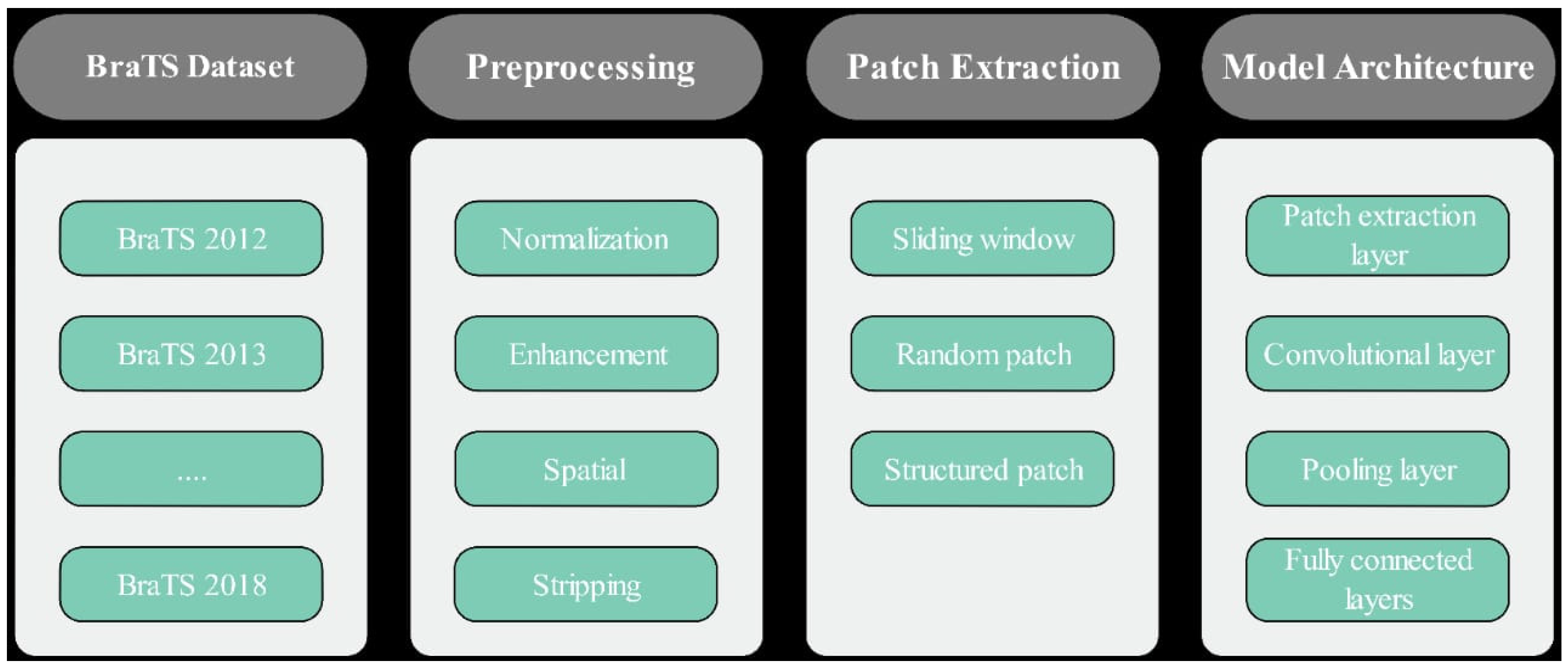
3. Methodology
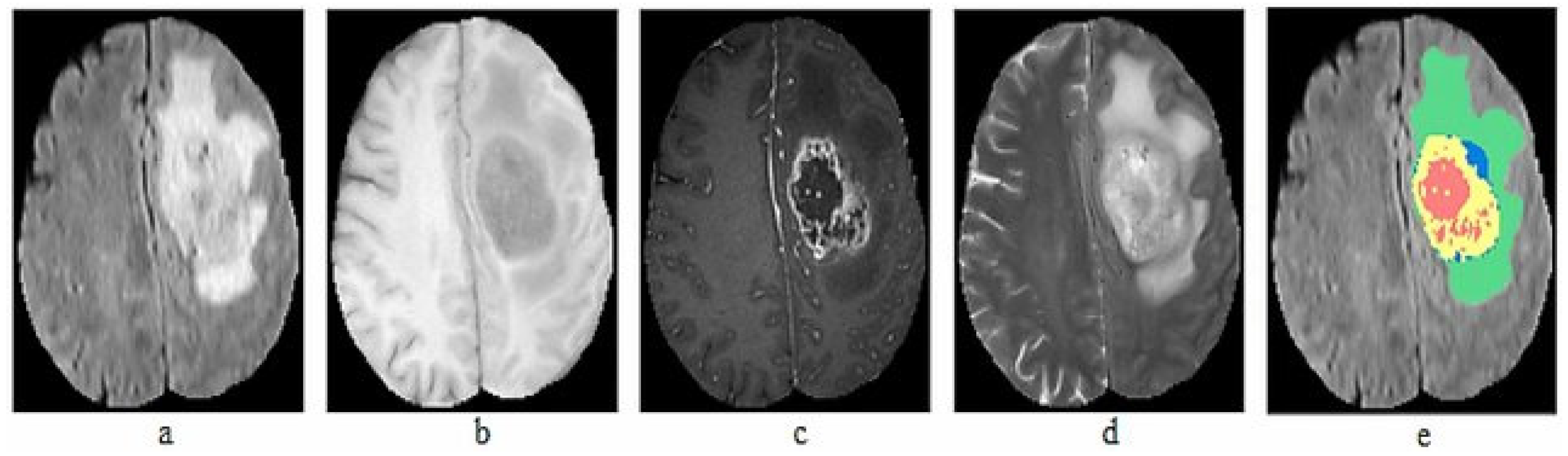
3.1. Data Acquisition
3.2. Data Preprocessing
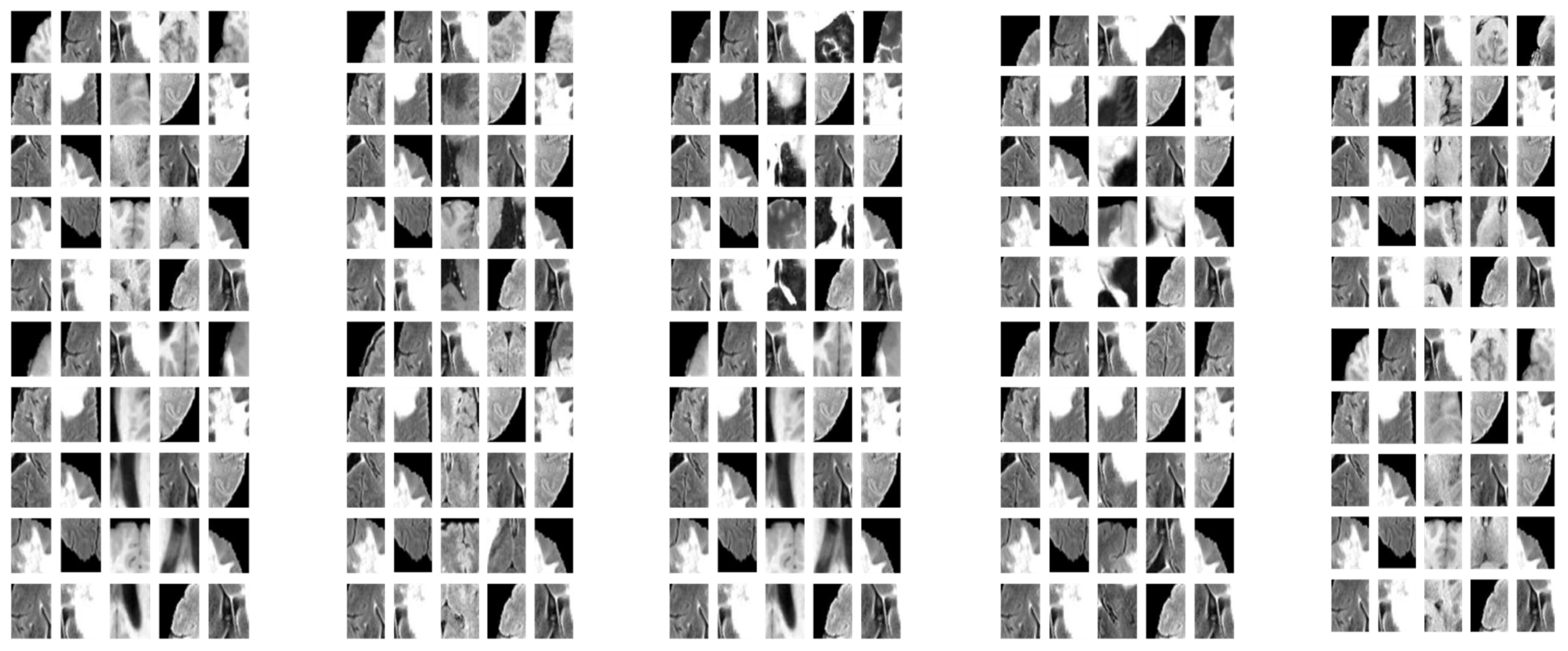
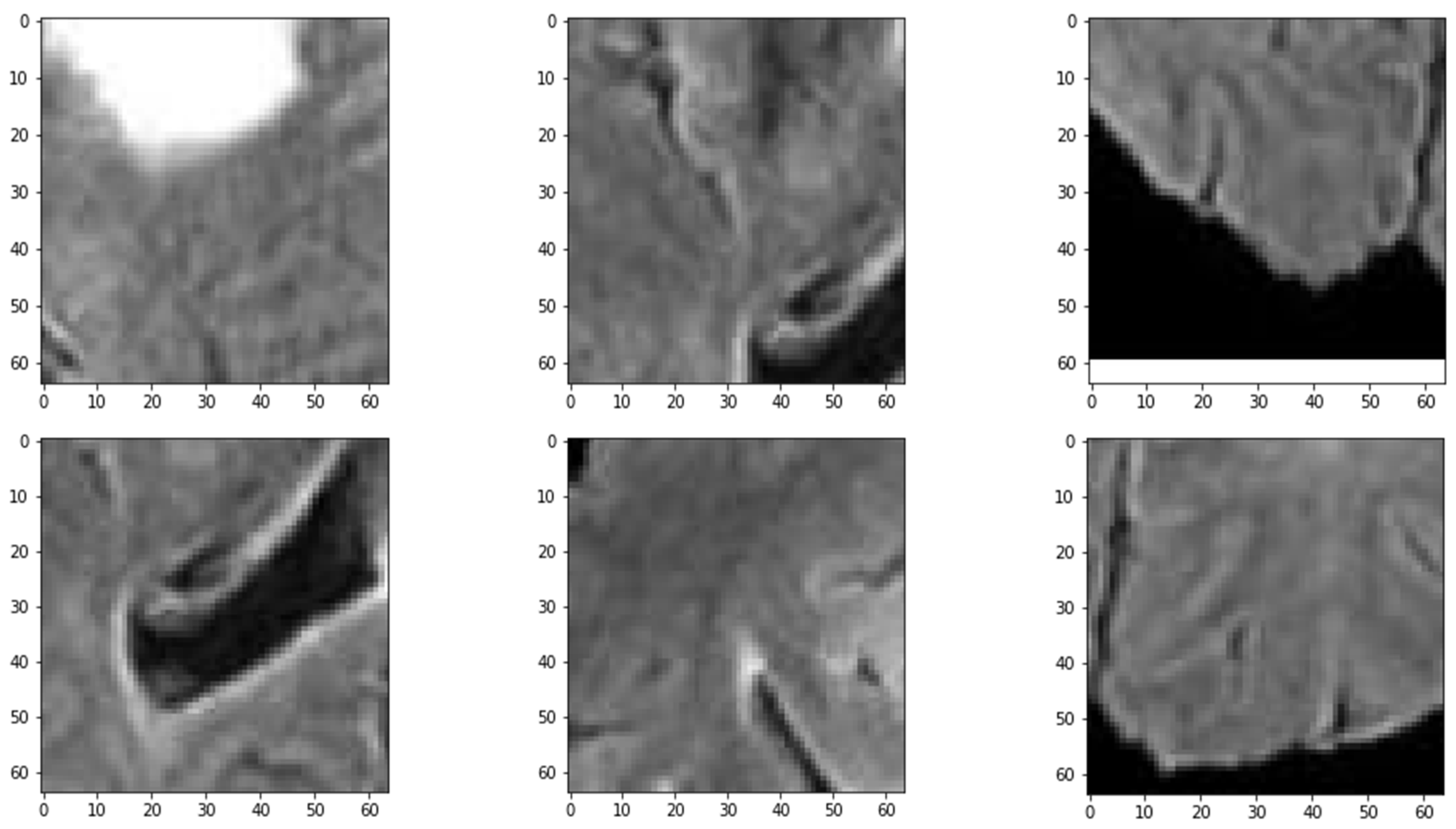
3.3. Patch Extraction
3.4. Training and Testing
3.5. Patch-Based Convolutional Neural Network (PBCNN)
4. Results and Discussion
4.1. Patches Extraction
4.2. Using Whole Images
4.3. Patch-Based CNN
4.4. Comparison of the PBCNN with State-of-the-Art Methods
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Akhavan, D.; Alizadeh, D.; Wang, D.; Weist, M.R.; Shepphird, J.K.; Brown, C.E. CAR T cells for brain tumors: Lessons learned and road ahead. Immunol. Rev. 2019, 290, 60–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, A.W.; Ilieş, I.; Benneyan, J.C.; Lokhnygina, Y.; Foy, K.R.; Lewis, S.S.; Wood, B.A.; Baker, E.; Crane, L.; Crawford, K.L. 93. Early Recognition and Response to Increases in Surgical Site Infections (SSI) using Optimized Statistical Process Control (SPC) Charts–the Early 2RIS Trial: A Multicenter Stepped Wedge Cluster Randomized Controlled Trial (RCT). Open Forum Infect. Dis. 2021, 8, S59–S60. [Google Scholar] [CrossRef]
- Sharma, P.; Diwakar, M.; Choudhary, S. Application of edge detection for brain tumor detection. Int. J. Comput. Appl. 2012, 58, 21–25. [Google Scholar] [CrossRef]
- Paul, T.U.; Bandhyopadhyay, S.K. Segmentation of brain tumor from brain MRI images reintroducing K–means with advanced dual localization method. Int. J. Eng. Res. Appl. 2012, 2, 226–231. [Google Scholar]
- Greenspan, H.; Van Ginneken, B.; Summers, R.M. Guest editorial deep learning in medical imaging: Overview and future promise of an exciting new technique. IEEE Trans. Med. Imaging 2016, 35, 1153–1159. [Google Scholar] [CrossRef]
- Yeganeh, A.; Shadman, A.; Shongwe, S.C.; Abbasi, S.A. Employing evolutionary artificial neural network in risk-adjusted monitoring of surgical performance. Neural Comput. Appl. 2023, 1–17. [Google Scholar] [CrossRef]
- Wang, S.; Yin, Y.; Wang, D.; Wang, Y.; Jin, Y. Interpretability-based multimodal convolutional neural networks for skin lesion diagnosis. IEEE Trans. Cybern. 2021, 52, 12623–12637. [Google Scholar] [CrossRef]
- Bakas, S.; Reyes, M.; Jakab, A.; Bauer, S.; Rempfler, M.; Crimi, A.; Shinohara, R.T.; Berger, C.; Ha, S.M.; Rozycki, M. Identifying the best machine learning algorithms for brain tumor segmentation, progression assessment, and overall survival prediction in the BRATS challenge. arXiv 2018, arXiv:1811.02629. [Google Scholar]
- Mittal, M.; Goyal, L.M.; Kaur, S.; Kaur, I.; Verma, A.; Hemanth, D.J. Deep learning based enhanced tumor segmentation approach for MR brain images. Appl. Soft Comput. 2019, 78, 346–354. [Google Scholar] [CrossRef]
- Kamnitsas, K.; Ledig, C.; Newcombe, V.F.; Simpson, J.P.; Kane, A.D.; Menon, D.K.; Rueckert, D.; Glocker, B. Efficient multi-scale 3D CNN with fully connected CRF for accurate brain lesion segmentation. Med. Image Anal. 2017, 36, 61–78. [Google Scholar] [CrossRef]
- Isensee, F.; Petersen, J.; Klein, A.; Zimmerer, D.; Jaeger, P.F.; Kohl, S.; Wasserthal, J.; Koehler, G.; Norajitra, T.; Wirkert, S. nnU-net: Self-adapting framework for u-net-based medical image segmentation. arXiv 2018, arXiv:1809.10486. [Google Scholar]
- Sandfort, V.; Yan, K.; Pickhardt, P.J.; Summers, R.M. Data augmentation using generative adversarial networks (CycleGAN) to improve generalizability in CT segmentation tasks. Sci. Rep. 2019, 9, 16884. [Google Scholar] [CrossRef] [Green Version]
- Bakas, S.; Makris, D.; Hunter, G.J.; Fang, C.; Sidhu, P.S.; Chatzimichail, K. Automatic identification of the optimal reference frame for segmentation and quantification of focal liver lesions in contrast-enhanced ultrasound. Ultrasound Med. Biol. 2017, 43, 2438–2451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.; Chen, C.; Ding, M.; Yu, H.; Zha, S.; Li, J. Transbts: Multimodal brain tumor segmentation using transformer. In Proceedings of the Medical Image Computing and Computer Assisted Intervention–MICCAI 2021: 24th International Conference, Strasbourg, France, 27 September–1 October 2021; pp. 109–119. [Google Scholar]
- Kofler, F.; Berger, C.; Waldmannstetter, D.; Lipkova, J.; Ezhov, I.; Tetteh, G.; Kirschke, J.; Zimmer, C.; Wiestler, B.; Menze, B.H. Brats toolkit: Translating brats brain tumor segmentation algorithms into clinical and scientific practice. Front. Neurosci. 2020, 14, 125. [Google Scholar] [CrossRef] [PubMed]
- Zikic, D.; Glocker, B.; Konukoglu, E.; Criminisi, A.; Demiralp, C.; Shotton, J.; Thomas, O.M.; Das, T.; Jena, R.; Price, S.J. Decision forests for tissue-specific segmentation of high-grade gliomas in multi-channel MR. In Proceedings of the MICCAI (3), Nice, France, 1–5 October 2012; pp. 369–376. [Google Scholar]
- Havaei, M.; Davy, A.; Warde-Farley, D.; Biard, A.; Courville, A.; Bengio, Y.; Pal, C.; Jodoin, P.-M.; Larochelle, H. Brain tumor segmentation with deep neural networks. Med. Image Anal. 2017, 35, 18–31. [Google Scholar] [CrossRef] [Green Version]
- You, L.; Qiu, A.; Huang, B.; Qiu, P. Early detection of high disease activity in juvenile idiopathic arthritis by sequential monitoring of patients’ health-related quality of life scores. Biom. J. 2020, 62, 1343–1356. [Google Scholar] [CrossRef]
- Hou, L.; Samaras, D.; Kurc, T.M.; Gao, Y.; Davis, J.E.; Saltz, J.H. Patch-based convolutional neural network for whole slide tissue image classification. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2424–2433. [Google Scholar]
- Çiçek, Ö.; Abdulkadir, A.; Lienkamp, S.S.; Brox, T.; Ronneberger, O. 3D U-Net: Learning dense volumetric segmentation from sparse annotation. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention–MICCAI 2016: 19th International Conference, Athens, Greece, 17–21 October 2016; pp. 424–432. [Google Scholar]
- Zhang, J.; Lv, X.; Sun, Q.; Zhang, Q.; Wei, X.; Liu, B. SDResU-net: Separable and dilated residual U-net for MRI brain tumor segmentation. Curr. Med. Imaging 2020, 16, 720–728. [Google Scholar] [CrossRef]
- Wu, W.; Li, D.; Du, J.; Gao, X.; Gu, W.; Zhao, F.; Feng, X.; Yan, H. An intelligent diagnosis method of brain MRI tumor segmentation using deep convolutional neural network and SVM algorithm. Comput. Math. Methods Med. 2020, 2020, 6789306. [Google Scholar] [CrossRef] [PubMed]
- Wulczyn, E.; Steiner, D.F.; Xu, Z.; Sadhwani, A.; Wang, H.; Flament-Auvigne, I.; Mermel, C.H.; Chen, P.-H.C.; Liu, Y.; Stumpe, M.C. Deep learning-based survival prediction for multiple cancer types using histopathology images. PLoS ONE 2020, 15, e0233678. [Google Scholar] [CrossRef] [PubMed]
- Sathornsumetee, S.; Reardon, D.A.; Desjardins, A.; Quinn, J.A.; Vredenburgh, J.J.; Rich, J.N. Molecularly targeted therapy for malignant glioma. Cancer 2007, 110, 13–24. [Google Scholar] [CrossRef]
- Molinaro, A.M.; Taylor, J.W.; Wiencke, J.K.; Wrensch, M.R. Genetic and molecular epidemiology of adult diffuse glioma. Nat. Rev. Neurol. 2019, 15, 405–417. [Google Scholar] [CrossRef] [PubMed]
- Moreno Lopez, M.; Ventura, J. Dilated convolutions for brain tumor segmentation in MRI scans. In Proceedings of the Brainlesion: Glioma, Multiple Sclerosis, Stroke and Traumatic Brain Injuries: Third International Workshop, BrainLes 2017, Held in Conjunction with MICCAI 2017, Quebec City, QC, Canada, 14 September 2017; pp. 253–262. [Google Scholar]
- Nie, D.; Lu, J.; Zhang, H.; Adeli, E.; Wang, J.; Yu, Z.; Liu, L.; Wang, Q.; Wu, J.; Shen, D. Multi-channel 3D deep feature learning for survival time prediction of brain tumor patients using multi-modal neuroimages. Sci. Rep. 2019, 9, 1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- BRATS—SICAS Medical Image Repository. 2012. Available online: https://www.smir.ch/BRATS/Start2012 (accessed on 2 February 2023).
- BRATS—SICAS Medical Image Repository. 2013. Available online: https://www.smir.ch/BRATS/Start2013 (accessed on 12 February 2023).
- BRATS 2014: Brain Tumor Image Segmentation Challenge. 2014. Available online: https://www.smir.ch/BRATS/Start2014 (accessed on 13 February 2023).
- BRATS 2015: Brain Tumor Image Segmentation Challenge. 2015. Available online: https://www.smir.ch/BRATS/Start2015 (accessed on 13 February 2023).
- BRATS 2016: Brain Tumor Image Segmentation Challenge. 2016. Available online: https://www.smir.ch/BRATS/Start2016 (accessed on 16 February 2023).
- Multimodal Brain Tumor Segmentation Challenge 2017. Available online: https://www.med.upenn.edu/sbia/brats2017/data.html (accessed on 10 February 2023).
- Multimodal Brain Tumor Segmentation Challenge 2018. Available online: https://www.med.upenn.edu/sbia/brats2018/data.html (accessed on 9 February 2023).
- Li, X.; Chen, H.; Qi, X.; Dou, Q.; Fu, C.-W.; Heng, P.-A. H-DenseUNet: Hybrid densely connected UNet for liver and tumor segmentation from CT volumes. IEEE Trans. Med. Imaging 2018, 37, 2663–2674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahuja, S.; Panigrahi, B.; Gandhi, T.K. Fully automatic brain tumor segmentation using DeepLabv3+ with variable loss functions. In Proceedings of the 2021 8th International Conference on Signal Processing and Integrated Networks (SPIN), Noida, India, 26–27 August 2021; pp. 522–526. [Google Scholar]
- Maji, D.; Sigedar, P.; Singh, M. Attention Res-UNet with Guided Decoder for semantic segmentation of brain tumors. Biomed. Signal Process. Control 2022, 71, 103077. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Techniques | Potential Strengths | Weaknesses |
|---|---|---|
| Brain Tumor Segmentation |
|
|
| Patch-Based Convolutional Neural Network (CNN) |
|
|
| Big Data Analysis |
|
|
| Brain Tumor Segmentation using a Patch-Based CNN |
|
|
| Dataset | Description |
|---|---|
| BraTS 2012 [28] | Thirty patients with glioblastoma multiforme (GBM) and thirty patients with lower-grade gliomas, along with manual segmentations of the tumors. The dataset included T1-weighted, T1-weighted with contrast enhancement, T2-weighted, and fluid-attenuated inversion recovery (FLAIR) MRI modalities. Link: https://www.smir.ch/BRATS/Start2012 (accessed on 2 February 2023) |
| BraTS 2013 [29] | Fifty-six patients with GBM, fifty-four patients with lower-grade gliomas, and five patients with brain metastases. It also introduced the use of the Dice similarity coefficient (DSC). Link: https://www.smir.ch/BRATS/Start2013 (accessed on 12 February 2023) |
| BraTS 2014 [30] | Forty-seven new patients with GBM and forty-two new patients with lower-grade gliomas, and included manual segmentations of the edema and non-enhancing tumor core regions. Link: https://www.smir.ch/BRATS/Start2014 (accessed on 13 February 2023) |
| BraTS 2015 [31] | Added 274 new patients with various types of brain tumors, including GBM, astrocytoma, oligodendroglioma, and mixed gliomas. Link: https://www.smir.ch/BRATS/Start2015 (accessed on 13 February 2023) |
| BraTS 2016 [32] | Consists of 220 HGG and 54 LGG. Its testing dataset consists of 191 cases with unknown grades. Link: https://www.smir.ch/BRATS/Start2016 (accessed on 16 February 2023) |
| BraTS 2017 [33] | Two hundred and eighty-five new patients with various types of brain tumors, and manual segmentations of the enhancing tumor, the necrotic and non-enhancing tumor core, and the edema regions. It also introduced a new sub-challenge for cross-institutional validation. Link: https://www.med.upenn.edu/sbia/brats2017/data.html (accessed on 10 February 2023) |
| BraTS 2018 [34] | Two hundred and eighty-five new patients with various types of brain tumors, and manual segmentations of the same tumor sub-regions as in the 2017 release. It also introduced a new sub-challenge for the detection of isocitrate dehydrogenase (IDH) mutation status. Link: https://www.med.upenn.edu/sbia/brats2018/data.html (accessed on 9 February 2023) |
| ID | Dataset | Reason for Discarding | Discard Method | Image Quality | Step 1 | Step 2 | Step 3 | Step 4 | Step 5 |
|---|---|---|---|---|---|---|---|---|---|
| 1 | BraTS | Motion artifact | Automated | Poor | Yes | Yes | Yes | Yes | Yes |
| 2 | BraTS | Scanner hardware issues | Automated | Poor | Yes | Yes | Yes | Yes | Yes |
| 3 | BraTS | Incomplete or missing image | Automated | Poor | Yes | Yes | Yes | Yes | Yes |
| 4 | BraTS | Low image quality | Automated | Fair | Yes | Yes | Yes | Yes | Yes |
| 5 | BraTS | Other | Automated | Poor | Yes | Yes | Yes | Yes | Yes |
| 6 | BraTS | Motion artifact | Automated | Fair | Yes | Yes | Yes | Yes | Yes |
| 7 | BraTS | Scanner hardware issues | Automated | Poor | Yes | Yes | Yes | Yes | Yes |
| 8 | BraTS | Incomplete or missing image | Automated | Poor | Yes | Yes | Yes | Yes | Yes |
| 9 | BraTS | Low image quality | Automated | Poor | Yes | Yes | Yes | Yes | Yes |
| 10 | BraTS | Other | Automated | Fair | Yes | Yes | Yes | Yes | Yes |
| Attribute | Description | Input Value | Output Value |
|---|---|---|---|
| Dataset | BraTS dataset | BraTS | - |
| MRI modality | T1-weighted | - | - |
| Patch size | Dimensions of each patch | 64 × 64 pixels | 64 × 64 pixels |
| Voxel size | Dimensions of each voxel in MRI image | 1 × 1 × 1 mm | 1 × 1 × 1 mm |
| Stride | Distance between centers of adjacent patches | 32 pixels | 32 pixels |
| Patch overlap | Amount of overlap between adjacent patches | 50% | - |
| No. of patches | Total number of patches extracted from image | - | 268 |
| Details | Any additional details relevant to patch extraction process | - | The patch size, voxel size, and stride were chosen based on prior work and the requirements of the specific machine learning model being trained. Overlapping patches were extracted with a 50% overlap between adjacent patches. |
| Image ID | Dataset | Patch Size | Stride | Patch Count |
|---|---|---|---|---|
| Brats_2012_001_1 | BraTS 2012 | 64 × 64 × 64 | 32 × 32 × 32 | 245 |
| Brats_2013_001_1 | BraTS 2013 | 64 × 64 × 64 | 32 × 32 × 32 | 246 |
| Brats_2014_001_1 | BraTS 2014 | 64 × 64 × 64 | 32 × 32 × 32 | 249 |
| Brats_2015_001_1 | BraTS 2015 | 64 × 64 × 64 | 32 × 32 × 32 | 248 |
| Brats_2016_001_1 | BraTS 2016 | 64 × 64 × 64 | 32 × 32 × 32 | 249 |
| Brats_2017_001_1 | BraTS 2017 | 64 × 64 × 64 | 32 × 32 × 32 | 250 |
| Brats_2017_002_1 | BraTS 2017 | 64 × 64 × 64 | 32 × 32 × 32 | 224 |
| Brats_2018_001_1 | BraTS 2018 | 64 × 64 × 64 | 32 × 32 × 32 | 289 |
| Brats_2018_002_1 | BraTS 2018 | 64 × 64 × 64 | 32 × 32 × 32 | 285 |
| Metric | Formula | Description |
|---|---|---|
| Dice coefficient | 2 × TP/(2 × TP + FP + FN) | Measures the overlap between the predicted and ground truth tumor segmentations. |
| Sensitivity | TP/(TP + FN) | Measures the proportion of actual positive cases that were correctly identified. |
| Specificity | TN/(TN + FP) | Measures the proportion of actual negative cases that were correctly identified. |
| Layer | Attributes | Purpose and Functionality |
|---|---|---|
| Patch Extraction | Patch size, Stride | Extract small sub-images (patches) from the original image using a sliding window technique. |
| Convolutional | Number of filters, Kernel size, Stride | Perform feature extraction on input patches using a set of learnable filters, which are convolved with the patches at each location to produce feature maps. |
| Activation | Type of activation function | Introduce non-linearity into the network by applying an activation function to the output of the convolutional layer. |
| Pooling | Type of pooling, Pooling size, Stride | Down sample the feature maps to reduce their spatial size while retaining important information. |
| Fully Connected | Number of neurons, Activation function | Combine the features and make a final prediction by passing the resulting features through one or more fully connected layers. |
| Layer | Filter Size | Stride | Filters | Input Data | Output Data |
|---|---|---|---|---|---|
| Conv1 | 3 × 3 | 1 | 32 | MR Images | Feature Maps |
| Conv2 | 3 × 3 | 1 | 64 | Feature Maps | Feature Maps |
| Conv3 | 3 × 3 | 1 | 128 | Feature Maps | Feature Maps |
| Conv4 | 3 × 3 | 1 | 256 | Feature Maps | Feature Maps |
| Conv5 | 3 × 3 | 1 | 512 | Feature Maps | Feature Maps |
| Conv6 | 3 × 3 | 1 | 1024 | Feature Maps | Feature Maps |
| Conv7 | 1 × 1 | 1 | 2048 | Feature Maps | Softmax Output |
| Layer | Filter Size | Stride | Filters | Input Data Size | Output Data Size |
|---|---|---|---|---|---|
| Input | N/A | N/A | N/A | 240 × 240 × 4 | 240 × 240 × 4 |
| Conv1 | 3 × 3 | 1 | 32 | 240 × 240 × 4 | 240 × 240 × 32 |
| Conv2 | 3 × 3 | 1 | 64 | 240 × 240 × 32 | 240 × 240 × 64 |
| Pool1 | 2 × 2 | 2 | N/A | 240 × 240 × 64 | 120 × 120 × 64 |
| Conv3 | 3 × 3 | 1 | 128 | 120 × 120 × 64 | 120 × 120 × 128 |
| Conv4 | 3 × 3 | 1 | 256 | 120 × 120 × 128 | 120 × 120 × 256 |
| Pool2 | 2 × 2 | 2 | N/A | 120 × 120 × 256 | 60 × 60 × 256 |
| Conv5 | 3 × 3 | 1 | 512 | 60 × 60 × 256 | 60 × 60 × 512 |
| Conv6 | 3 × 3 | 1 | 1024 | 60 × 60 × 512 | 60 × 60 × 512 |
| Pool3 | 2 × 2 | 2 | N/A | 60 × 60 × 512 | 30 × 30 × 512 |
| Conv7 | 3 × 3 | 1 | 2048 | 30 × 30 × 512 | 30 × 30 × 512 |
| Pool4 | 2 × 2 | 2 | N/A | 30 × 30 × 256 | 15 × 15 × 256 |
| Pool5 | 2 × 2 | 2 | N/A | 15 × 15 × 64 | 8 × 8 × 64 |
| FC1 | N/A | N/A | N/A | 8 × 8 × 64 | 1 × 4096 |
| FC2 | N/A | N/A | N/A | 1 × 4096 | 1 × 4096 |
| FC3 | N/A | N/A | N/A | 1 × 4096 | 1 × 5 |
| Feature | Description | Value |
|---|---|---|
| Dataset | Name of the dataset | BraTS (2012–2018) |
| Size | Number of MRI scans in the dataset | 3304 |
| MRI Modality | Modalities of the MRI scans in the dataset | T1, T1ce, T2, FLAIR |
| Tumor Types | Types of brain tumors in the dataset | Glioblastoma, astrocytoma, oligodendroglioma, and others |
| Annotations | Type of annotations in the dataset | Manual |
| Annotators | Number of annotators for each scan | Multiple |
| Data Split | Division of the dataset into training, validation, and testing sets | 2804 for training and validation, 500 for testing |
| Class Imbalance | Proportion of tumor and non-tumor scans in the dataset | 1993 tumor and 1311 non-tumor scans |
| Data Availability | Availability of the dataset for research purposes | Open access with proper permissions and approvals |
| Evaluation Metrics | Metrics used to evaluate the performance of segmentation methods | Dice coefficient, Hausdorff distance, sensitivity, specificity, and others |
| Baselines | Segmentation models used for comparison | U-Net, V-Net, 3D-FCN, DeepMedic, and others |
| Dataset | No. of Tumor Patches | No. of Normal Patches |
|---|---|---|
| Training | 9000 | 9000 |
| Validation | 1000 | 1000 |
| Testing | 2000 | 2000 |
| Tumor Type | Dice Coefficient | Sensitivity | Specificity | Precision | Recall |
|---|---|---|---|---|---|
| Edema | 0.72 | 0.82 | 0.87 | 0.73 | 0.82 |
| Non-enhancing tumor | 0.56 | 0.68 | 0.85 | 0.57 | 0.68 |
| Enhancing tumor | 0.57 | 0.70 | 0.86 | 0.58 | 0.70 |
| Necrosis | 0.29 | 0.32 | 0.89 | 0.30 | 0.32 |
| Tumor Type | Dice Coefficient | Sensitivity | Specificity | Precision | Recall |
|---|---|---|---|---|---|
| Edema | 0.81 | 0.89 | 0.91 | 0.81 | 0.89 |
| Non-enhancing tumor | 0.70 | 0.80 | 0.93 | 0.70 | 0.80 |
| Enhancing tumor | 0.66 | 0.81 | 0.92 | 0.66 | 0.81 |
| Necrosis | 0.55 | 0.62 | 0.95 | 0.55 | 0.62 |
| Metric | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 |
|---|---|---|---|---|---|---|---|
| Dice Coefficient | 0.82 | 0.79 | 0.86 | 0.83 | 0.85 | 0.86 | 0.87 |
| Sensitivity | 0.81 | 0.75 | 0.84 | 0.80 | 0.83 | 0.84 | 0.85 |
| Specificity | 0.99 | 0.99 | 0.99 | 0.99 | 0.99 | 0.99 | 0.99 |
| Positive Predictive Value | 0.88 | 0.85 | 0.91 | 0.89 | 0.90 | 0.92 | 0.93 |
| Negative Predictive Value | 0.98 | 0.97 | 0.98 | 0.98 | 0.98 | 0.98 | 0.98 |
| Accuracy | 0.97 | 0.96 | 0.98 | 0.97 | 0.98 | 0.98 | 0.98 |
| Method | Dice Coefficient | Sensitivity | Specificity | Accuracy |
|---|---|---|---|---|
| Proposed PBCNN | 0.91 | 0.89 | 0.98 | 0.96 |
| U-Net | 0.88 | 0.86 | 0.97 | 0.94 |
| DeepLab V3+ | 0.85 | 0.83 | 0.96 | 0.93 |
| ResUNet++ | 0.87 | 0.85 | 0.96 | 0.94 |
| Tumor Type | CNN Dice Coefficient | Patch-Based CNN Dice Coefficient | Improvement in Dice Coefficient |
|---|---|---|---|
| Edema | 0.72 | 0.91 | 0.14 |
| Non-enhancing tumor | 0.56 | 0.72 | 0.16 |
| Enhancing tumor | 0.57 | 0.75 | 0.18 |
| Necrosis | 0.29 | 0.47 | 0.18 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ullah, F.; Salam, A.; Abrar, M.; Amin, F. Brain Tumor Segmentation Using a Patch-Based Convolutional Neural Network: A Big Data Analysis Approach. Mathematics 2023, 11, 1635. https://doi.org/10.3390/math11071635
Ullah F, Salam A, Abrar M, Amin F. Brain Tumor Segmentation Using a Patch-Based Convolutional Neural Network: A Big Data Analysis Approach. Mathematics. 2023; 11(7):1635. https://doi.org/10.3390/math11071635
Chicago/Turabian StyleUllah, Faizan, Abdu Salam, Mohammad Abrar, and Farhan Amin. 2023. "Brain Tumor Segmentation Using a Patch-Based Convolutional Neural Network: A Big Data Analysis Approach" Mathematics 11, no. 7: 1635. https://doi.org/10.3390/math11071635