1. Background
Wastage and improper disposal of pharmaceuticals is a global issue that impacts every continent on Earth [
1,
2,
3] and, with medicine usage in the UK alone predicted to double by 2050, is an issue that will only increase in severity [
4]. With an estimated GBP 300 million being spent annually on unused medicines by the UK National Health Service (NHS) [
5], significant quantities of medication being wasted across Europe [
6,
7], and a large disparity between patients being unable to afford treatment, while huge quantities of medicines are being discarded in the USA [
8,
9], the economic effects of medicine waste can be felt across multiple countries. Pharmaceutical waste, defined as hazardous or in some cases cytotoxic [
10], has been found in wastewater, rivers, and even sources of drinking water [
11,
12,
13]. This includes every major estuary tested in the UK [
14] and at every point tested along the Thames [
11]. Active Pharmaceutical Ingredients (APIs) have been shown to impact plants and animals in the wild [
15,
16,
17,
18]. This may also affect humans through the consumption of drinking water and produce plants, as the consequences of long-term exposure to multiple APIs at a low concentration is unknown [
19]. If not properly disposed of, unused medicines can be a danger to the public. Through abuse, self-medication without a prescription, or acquisition from an illegitimate source, the misuse of prescription drugs can lead to addiction, long-term health complications, and death [
20,
21,
22,
23]. While there are many papers on waste reducing behaviours [
24,
25,
26,
27], there are relatively few surrounding the reuse of discarded medicines.
Medicine reuse is a solution that can reduce medicine wastage and its impacts worldwide. In the USA, legislation has been passed in 40 states and Guam legalising medicine reuse [
28]. There are 27 individual state-endorsed programs that accept medicines from around the country to redistribute within their area [
29,
30,
31]. SIRUM and GIVMED are the two existing large-scale systems for medicine reuse [
32,
33]. SIRUM operates in the USA. Since its foundation in 2013, SIRUM has aided in USD 89.6 million worth of prescriptions and aims to have helped 70% of the 10 million most in need by 2030 [
32]. Since 2016, GIVMED has operated in Greece, receiving over EUR 3.33 million of medicine and healthcare products [
33]. All organisations state that donated medicines must be unopened, unexpired, and stored correctly [
29,
30,
31,
32,
33]. Most US states express that medicines must be assessed by a pharmacist, controlled medicines cannot be donated, donors cannot be financially compensated, and donors or recipients are not liable for faulty medicines [
29,
30,
31].
The concept of a circular economy (CE) has been gaining traction in recent years and could be applied to pharmacy to aid in reducing the amount of excess medicine wastage [
34]. As seen in
Table 1, CE revolves around minimising the amount of waste produced by a system by redefining the process of product design and manufacturing, allowing every opportunity for the product or its components to be reused, and even to the recovery of energy being produced from the incineration of waste. Examples of CE include the phasing out of single-use plastics (with open sourced technology allowing consumers to recycle plastic into 3D printing materials [
35]), encouraging the sharing of rarely used items [
36], and the reuse of items that will be outgrown or outdated [
37].
Reverse logistics (RL) is a methodology used by companies when handling products moving backwards through a supply chain [
38]. Through repurposing these products or their components, the system can reduce the number of components needed for the forward supply chain, and can be further utilised to enable a CE. The overseeing of daily operations in the reverse supply chain (i.e., transport, storage, and reimbursement for returns) are typically handled by a third-party logistics company (3PL). Examples of RL can be seen in the return of malfunctioning products to a manufacturer by a customer or retailer for repair, or the redistribution of products unsold due to a surplus.
With the introduction of Industry 4.0, there has been an increase in the application of technologies to CE and RL systems. One example of this includes the use of Blockchain and Internet of Things (IoT) to trace stock (such as asbestos or wine) and throughout a circular economy [
39,
40,
41]. A further application of this has been the inclusion of machine learning to predict the need of goods or equipment requiring maintenance to enable closer organisation between the reverse and service supply chains [
42]. Research applying Industry 4.0 to the Pharmaceutical Supply Chain (PSC) has included posing the improvement of a supply chain as a decision-making problem and using mathematical and machine learning methods to optimise the solution. This can be seen in studies on optimising a Pharmaceutical Supply Chain Network and designing a reverse supply chain to recycle COVID-19 waste [
43,
44].
CE ideals are also being applied within the PSC, with research and campaigns extending into the topics of: maximising patient adherence through altering prescription quantity and frequency [
24,
25]; education of the public into medicine waste [
26,
45]; the extension of use-by dates on EpiPens during a shortage [
46]; the efficacy of waste reduction measures in pharmacies [
27,
47]; the sharing of cancer medications in clinics for maximum stock use [
48]; the recycling of the outer packaging/cartridges for inhalers [
49]; medicine return programs to ensure appropriate disposal of medicines [
50,
51]; the recovery of APIs for remanufacturing [
52,
53]; and the burning of medicines through pyrolysis to recover any energy from wasted medicines [
54].
The two main aims of this research are to investigate the state of the research regarding medicine reuse to identify the recurring concerns, major barriers, and advancements within the field and to provide a novel solution that builds on existing technologies to address repeated concerns and the gaps within the literature.
In
Section 2, we carry out a literature review to assess the state of medicine reuse as a field, investigating the barriers facing the implementation of a large-scale medicine reuse system. This is the first literature review to explore the field of medicine reuse as a whole and combine research from a variety of viewpoints (i.e., feasibility, stakeholder opinions, technological solutions, and circular economy) to paint a more complete picture of the field.
In
Section 3, we design a conceptual model of a circular pharmaceutical supply chain (CPSC), inspired by the use of CE and RL found in the literature. Two models are presented to show the proposed supply chain through forward and reverse flows, as well as grouping of stages that will be controlled by similar legislation and operating procedures. The two models are then explored to identify the barriers preventing the implementation of a CPSC and propose key changes and future work that needs to be done to enable medicine reuse. The novelty of the theoretical CPSC is that the assessment and reverse flow of medicines is placed in the context of the existing forward supply chain and that each stage of the model contains waste-reducing measures inspired by the principles of circular economy.
In
Section 4, we then propose SPaRAS (a smart packaging and returns assessment system), confirming the safe storage of medicines in patient care while streamlining the assessment of returned medicines. This is done to address the most common concerns found in the literature and overcome the most pressing barriers preventing the implementation of a CPSC. SPaRAS is composed of a Smart Packaging System (SPS) and a companion Returns Assessment system (RAS). The SPS is a device that is inserted in medicine boxes to record the storage conditions of medicines while in patient care. The RAS is an application on an NFC-enabled Android tablet that (on dispensation) configures the device’s settings to the needs of its assigned medicine and (on return) validates the medicine’s storage conditions against corresponding criteria. The novelty of SPaRAS is the use of technology to enable a circular economy of medicines, the combination of key concepts from other proposed technologies to address the recurring concerns found within the literature, and the non-intrusive recording of conditions within patient care, which enables the management of medicines in patient care as another stage in the PSC.
The key contributions of this work are as follows:
The combination of the varied aspects of medicine reuse outlining the barriers and proposed solutions in the literature;
The proposal of a device to address several of the most common concerns from pharmaceutical stakeholders surrounding medicine reuse;
The presentation of a theoretical CPSC to signpost a long-term goal and break down the key changes that must be made to reduce medicine wastage.
2. A Systematic Review into Medicine Reuse
A systematic literature review was carried out to assess the state of medicine reuse as a field of study. The review found that there has been significant work done with the intention of enabling medicine reuse. Although the field is in its infancy, the key areas of research include evaluating opinions on medicine reuse, determining at what level medicine reuse is feasible, and developing both hypothetical and practical medicine reuse systems.
2.1. Methods
The search string was built in the following basic structure: Medicine AND (Reuse OR Waste). This was expanded upon with synonyms and other similar words to create the final search string: (Medicine* OR Medication* OR Medical OR Prescription* OR Drug* OR Pill*) AND ((Reus* OR Recycl* OR Redistribut* OR Reallocat* OR Reclaim* OR Salvag*) OR (Was* OR Unused OR Excess OR spare OR discard OR Thrown away OR Leftover OR Surplus OR Extra)).
The search string was entered into the following databases:
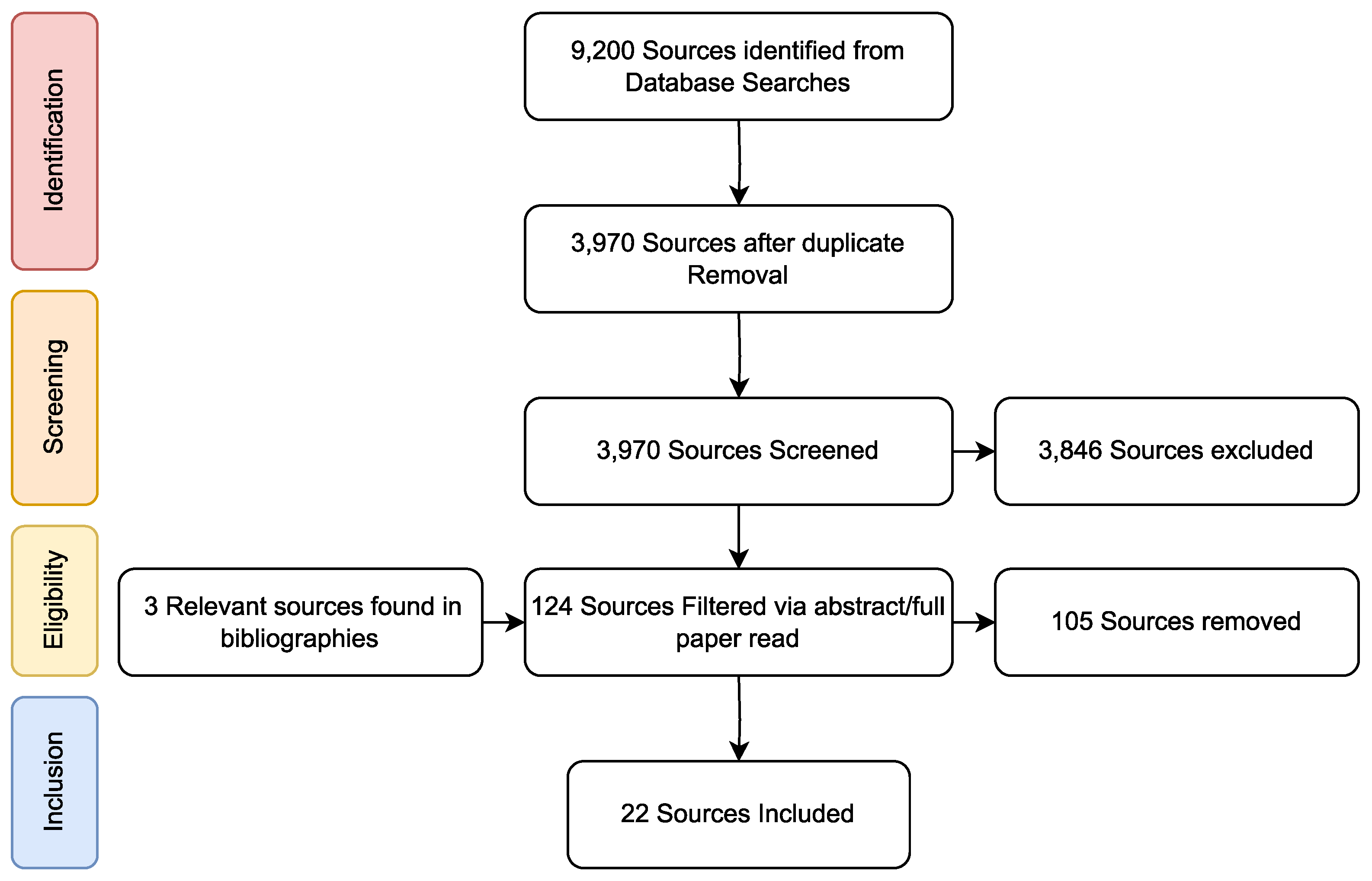
Source selection was carried out according to the PRISMA flow of identification, screening, eligibility, and inclusion, as shown in
Figure 1 [
55]. The search returned 3970 unique results, whose titles were screened to remove 3846 irrelevant papers. The remaining 124 papers were assessed first by their abstract and then by their entire contents. Papers with a subject specifically relating to the reuse of prescription medications were included. Papers not in English or those with a focus on reusing medicines in hospitals or other methods of waste reduction were excluded. In total, 21 papers from 13 authors were included in this study. Of those papers, 18 were found in the original search, with an addition 3 sources being added from the references of relevant papers.
As ’medicine reuse’ is a broad subject, to better structure the review and identify the key gaps in the literature, the papers were sorted into several categories. One paper was included in two categories, as it discussed both technologies and reverse logistics within the PSC. The breakdown of papers are as follows: five papers debated “The Feasibility of Medicine Reuse”, ten papers evaluated “Opinions on Medicine Reuse”, three papers outlined the “Technology Developed to Enable Medicine Reuse”, and five papers discussed “The use of Circular Economy and Reverse Logistics Principles to Enable Medicine Reuse”.
2.2. Key Authors
The largest source of papers in this review was the combined work from the ReMINDS team, having published eight papers that were included in this study [
56,
57,
58,
59,
60,
61,
62,
63]. ReMINDS is an interdisciplinary team, including professionals from the fields of pharmacy, biomedical engineering and psychology, at the University of Reading that aims at enabling the Reuse of Medicines through informatics, networks and digital sensors (
www.reading.ac.uk/ReMINDS/) (accessed on 1 June 2023). The work carried out by the ReMINDS team involves gauging both public and professional opinions on medicine reuse, and the assessment and development of technologies to enable medicine reuse. This work is addressed in the relevant sections. To demonstrate the interdisciplinary nature of medicine reuse, a ReMINDS ecosystem was also presented by [
59]. The proposal outlined the flow of information necessary to maintain and monitor the operation of a medicine reuse system and demonstrates the need for professionals in pharmacy (to handle medicines and research their stability), law (to encourage legislation and policy change), computing (to maintain the flow of information regarding medicines), psychology (to encourage public participation), business (to encourage participation of organisations), and engineering (to create and maintain necessary technologies).
Dr. Charlotte Bekker is another significant source of papers in this study, being the lead author on three studies on the theme of the feasibility of medicine reuse and two studies researching opinions on medicine reuse [
64,
65,
66,
67,
68]. Bekker is a postdoctoral researcher at the pharmacy department of the Radboud University Medical Centre carrying out work in the field of sustainable pharmaceutical care (with a focus on medication waste, adherence, and the optimal dosing of expensive medication).
2.3. The Feasibility of Medicine Reuse
The three studies determining the eligibility of returned medicines all define medicines eligible for reuse as sealed in their boxes and undamaged. However, two of the studies stated that medicines must be at least 6 months before expiry [
61,
64], whereas the third only specifies that medicines must be unexpired [
69]. The two studies, specifying a greater than 6 month shelf life, found that only a minority of returns were eligible for reuse (19.1% in [
61] and 29% in [
64]). The third study found that out of all patient-donated medicines, 88.4% were eligible for reuse. As this is only a small group of studies, carried out over different lengths in different countries, the apparent trend between the amount returns being eligible and differing criteria cannot be relied upon. However, these studies all demonstrate that a significant quantity of unused medicines returned to the pharmacy may be eligible for reuse.
Additionally, a study into the waste of anti-cancer drugs (OACDs) and biologic disease modifying anti-rheumatic drugs (bDMARDs) found that an estimated EUR 6 million could be wasted yearly throughout the Netherlands [
65]. In total, 80.1% of the total economic value of unused medicines found was made up of sealed packages. It can be assumed that these medicines were unexpired as all participants were within two weeks of their prescription end-date. This can be extrapolated to show that up to EUR 4.8 million of unused OACDs and bDMARDs could be eligible for redispensation in the Netherlands every year. This figure can only be considered an estimate, as the sample size of the study was relatively small (N = 71).
A study into the cost of medicine reuse showed that the assessment and redispensation of returned medicines is only economically viable for more expensive medicines with standard storage requirements due to the cost of resources and staff [
66]. However, the minimum value for medicines to be worth redispensation can be decreased by increasing the quantity of high-quality returns, making the process yield more in a shorter time. It has been shown that there are a significant amount of high-quality medicines which may allow for medicine reuse to become cost effective [
61,
64,
69]. This could be aided by a public campaign to encourage more returns, and a higher standard of returns. The affordability of medicine reuse could also be aided by redesigning the assessment process with time and cost efficiency in mind.
2.4. Opinions on Medicine Reuse
Nine sources that assess beliefs on medicine reuse, from professionals in pharmacy and members of the public, have been included. These studies were carried out between 2016 and 2021 and were composed of two originating from the Netherlands and seven from the UK. Three of the studies focused specifically on the opinions of professionals in the field of pharmacy (including doctors, nurses, pharmacists, and industry representatives) [
57,
67,
70], seven were available for the members of the public [
56,
57,
62,
63,
68,
71,
72], with one study gathering opinions from both groups [
57]. The sample sizes in these papers ranged from 19 to 5584. With four studies having a sample size of over 1000 [
56,
63,
68,
71]. The most commonly used method of primary data collection was through a questionnaire, used by five papers. Other methods included semi-structured interviews, a two-round Delphi study, and notation of open discussions.
Seven papers were aimed at gathering primary data on the public’s opinions of reuse (including their intentions to engage in a system, concerns, and potential solutions to overcome barriers facing medicine reuse) [
56,
57,
62,
67,
68,
70,
71]. One study aimed at making a predictive theory of planned behaviour using the questionnaire responses from another and showed that, while the majority of patients were in favour of medicine reuse, social norms were extremely influential on whether or not an individual supported medicine reuse [
63]. This study did not outline participant’s specific concerns surrounding medicine reuse. The use of the theory of planned behaviour for medicine reuse was later validated in another source by the same authors [
58]. One of the included studies investigated the effect that quality checking returned medicines and including a sensor to validate the medicines’ storage conditions would have on subjects’ willingness to participate in a system [
72]. It was found that participants were significantly more likely to support medicine reuse in the scenarios that included medicine being quality checked by a pharmacist or being validated by a sensor. The scenario involving both the quality checks and the embedded sensor generated the highest confidence in participants.
Overall, it was found that a majority of participants in all studies supported the dispensation of prescription medicines. However, similar concerns could be found in multiple studies. These can be separated into two distinct categories. The first type of concern raised in the studies surrounded the redistribution of unsafe medicines. Most commonly, this involved the need for medicines to have been stored in a hygienic and uncontaminated environment at the required conditions (i.e., temperature, humidity, and light level) and that only medicines in the original unopened and undamaged packaging be dispensed. Some concerns were also raised about potentially dangerous counterfeit medicines and the possibility of errors being made within the pharmacy leading to the redistribution of incorrectly returned medicines. The most common solutions for suggested to alleviate these concerns were the returned medicines being quality-checked by a pharmacist before being redispensed, the inclusion of a sensor in the medicine packaging to assess the storage conditions of the medicines, and the addition of a tamper-evident seal. The second type of issue present throughout the studies involved the feasibility of medicines being reused from a supply chain perspective. This included the increased costs and resources required when assessing and storing returned medicines, the need for a change in legislation and professional standards, concerns surrounding liability, and the need for the public to trust and engage in an implemented system. The solutions presented for these issues were to only reuse expensive medicines and to ensure pharmacies were presented as concerned about wasted medicines, not savings.
2.5. Technology Developed to Enable Medicine Reuse
Three papers outlining technologies developed/repurposed for medicine reuse have been included. These are a paper proposing the use of RFID tags to streamline reverse flows within the PSC [
73], a literature review of sensors that can be appropriated for medicine reuse [
59], and a DTTHI (digital time temperature humidity indicator) that tracks the storage conditions of medicines while in patient care [
60].
Kongar et al. [
73] proposed that RFID tags be embedded within each medicine box. Each tag would contain a unique identification number, information identifying and describing the medicine, an expiry date, the history of the medicine, i.e., manufacturing, selling point and return point information, and the reason for the medicine’s return. When the medicines are returned for assessment, the long-range RFID antennas would upload this information to a centralised database with the date and time of the medicine’s arrival. Kongar et al. [
73] further outlined the use of this technology within the assessment of returns. By scanning the RFID Tag, the assessor could instantly identify the medicines and expiration status. This would significantly reduce the amount of time spent assessing each medicine. The use of RFID tags in pharmaceutical packages would reduce the need for data entry in inventory management and save significant time and money. The use of long-range antennas would allow a live feed of stock entering or exiting storage. Through future application of this, medicine shortages or surpluses can be identified or even predicted based on previous trends. These tags could also be electronically fitted with an anti-counterfeiting measure, such as encryption of a unique identification.
Hui et al. [
59] carried out a systematic review of sensors to be appropriated for medicine reuse, and proposed a smart packaging system to create an internet of pharmaceutical things (IoPT) network [
60]. This system consisted of two sensors that recorded the temperature and humidity that the medicines were stored in, and an internet connection to provide a live feed of storage conditions to a companion cloud network. An E-ink display was included as a user interface (UI) that showed the key features of the system, such as activation date, expiry date, bars providing data on the storage conditions (temperature/humidity) and time towards expiry, and an indicator on whether or not the medicine can be reused. The system is able to communicate with a companion cloud system to upload information at regular intervals and download any required updates. Challenges the system faces are power consumption, size, security of users’ information, cost of adding components to packaging, and the usability of the system. However, the use of off-the-shelf components for the prototype increases the cost, size, and power consumption. The system could benefit from a redesign to remove potentially unnecessary components. A detailed breakdown of the design and alterations needed for the DTTHI can be found in
Section 4.1.
2.6. The Use of Circular Economy and Reverse Logistics Principles to Enable Medicine Reuse
In addition to the charitable medicine reuse programs that utilise RL, five papers have been included that propose systems and evaluate the use of CE and RL to enable medicine reuse.
In 2015, an RL system was proposed by Kongar et al. [
73] using RFID technology (as previously discussed) to streamline the supply chain. This paper focuses on reverse logistics of managing the returned medicines from a supply chain perspective. The model involves three phases: Phase 1, the forward supply chain: the forward flow of pharmaceuticals and the reverse flow of information; Phase 2, the decision process, which consisted of controllable and uncontrollable factors, targets, and constraints to be considered when planning and controlling the daily operations of the system; Phase 3, reverse logistics, which includes the medicine’s returns and processing (i.e., screening, cleaning, and sorting).
Unexpired medicines would be checked for stability and be assigned an updated expiry date. Medicines in short supply are redistributed or remanufactured, while unneeded medicines are placed into storage. Expired medicines could be assigned an updated expiry date, remanufactured, or disposed of safely (based on their stability and toxicity). The proposed processing system should be considered as a long-term goal due to the current restrictions on reusing non-toxic, unstable medicines. However, the regulations on medicine reuse may be changed through campaign and should, therefore, be considered a semi-permanent obstacle but not an uncontrollable factor.
A machine learning algorithm has been able to devise a near optimal plan for implementing medicine reuptake in an area, with the goal of keeping costs (especially government-paid subsidiaries) low [
74]. The model was given the layout of drugstores, waste treatment sections, and residential areas of a hypothetical region, along with the population and the drug amount needing to be recycled in each residential section. The algorithm can then select the best pharmacies and waste treatment plants in each area to be upgraded to recycling centres and drug disposal centres in order to keep governmental costs low while ensuring both pharmacies and individuals receive enough of an incentive to participate in the implemented system. This technology could be extremely valuable in ensuring any proposed medicine reuse system is economically viable.
In 2019, Viegas et al. [
75] reviewed and evaluated reverse pharmaceutical flows (i.e., donations for humanitarian purposes, RL, and CE). The main issues found with RL systems were poor planning and inventory management. The need for standardisation and prescription organisation was stressed to ensure a circular economy runs efficiently as most medicine reuse systems are run less formally (i.e., non-profit organisations). Donations to other countries were found to be irrelevant, of poor quality, or subject to misappropriation. Due to the lack of literature on end-of-use medicines in a CE, it was also suggested that medicines may be perpetually circulated until expiry, and therefore, not reducing waste. They showed that a large barrier to medicine reuse is a lack of detailed literature on reverse flows with end-of-use/end-of-life medicines.
Two sources evaluating the use of CE in the PSC were published in 2020. One paper, evaluating the possibility of implementing a CPSC, outlined key points of waste creation throughout the PSC, their associated countermeasures, and an evaluation of the methods used for medicine waste disposal with regard to their cost and environmental impact [
76]. Further lists were generated outlining the key barriers to reusing patient owned medicines, application of CE principles throughout the PSC, and key enablers and barriers to the adoption of a CPSC.
This was used to propose changes needed to enable a CPSC on multiple levels (global, national, organisational, and individual). On a global level, there needs to be official recognition of medicine waste levels and waste reduction targets. On a national level, there needs to be increased provision of resources and financial support for technologies and measures to reduce pharmaceutical waste, as well as official endorsement and an effort in raising awareness for CE in the PSC for professionals and patients. On an organisational level, proposed changes included the introduction of efficient systems to manage waste reduction and reuse and safely dispose of medicines; training for professionals and increased awareness for patients on the sources and methods of reducing of medicine waste; teams to recollect and assess medicines from wards for safe disposal; and individuals to support and endorse waste reduction practices. On an individual level, it was suggested that stakeholders alter their attitudes to engage with educational programs on medicine waste, its reduction and impacts as well as design simple systems to advocate medicine reuse.
A model for medicine returns was created by Liu et al. [
77] that classed returned medication into three categories: (A) medicines with over two years before expiry to be resold or donated, (B) medicines with over one year before expiry to be donated, and (C) expired drugs or those with less than one year before expiry to be disposed of. A 3PL company handles the returns of (A) and (B) to the producer and disposal of (C) in return for recovery fees. The producer can then sell (A) for profit and donate (A) and (B) for tax incentives. The novelty of this system was the economic benefits to all parties through the resale of (A), the social benefits of the donation of (A) and (B), and the environmental benefits of properly disposing of (C). However, there is little mention given to the safety assessment of returned medication, which is a heavily criticised aspect of medicine reuse.
2.7. The State of the Literature
Although medicine reuse is a very new academic field with few, far-spread sources, some areas have seen considerable progress. There are two main gaps in the literature that this paper tries to address. There is a lack of technological applications addressing the concerns surrounding medicine reuse, with the only suggested devices being the DTTHI- [
60] and RFID-tagged medicine boxes [
73]. To address the lack of research, this paper proposes a device, inspired by the DTTHI- and RFID-tagged boxes, to simultaneously validate the safety of medicines while in patient care and reduce the cost of medicine reuse by streamlining the assessment of returns. There have been several papers on CE and RL within the PSC, with three papers suggesting systems for enabling medicine reuse (two papers taking an economic approach and the other focusing on logistics). There are no papers outlining the logistics of a full Circular Pharmaceutical Supply Chain in relation to the existing PSC. This paper addresses this gap through detailing a CPSC with CE principles applied at every stage, and a reverse flow to enable medicine reuse.
Research into the feasibility of medicine reuse has already shown that the cost of assessing, storing, and redistributing medicines currently only allows the reuse of expensive medicines, but there is a significant amount of eligible medicines in patient’s homes that could lower the cost of medicine reuse if returned. Further work could be carried out on assessing the quantity of high-quality medicines currently in patient care to strengthen the legitimacy of current findings. Any additional research on this should aim to define a standardised criteria for assessing medicines and a larger sample size. There has also been significant work into discerning the beliefs of professionals and the public surrounding medicine reuse. Future research aimed at enabling medicine reuse should focus on methods of increasing public engagement, such as the effect of public campaigns on opinions surrounding reuse, or the proposition of alternative solutions to the raised issues.
3. Proposal for a Circular Pharmaceutical Supply Chain (CPSC)
Using inspiration from the previous research, two novel models describing a circular economy for medicine reuse are presented in this work. This includes the flow of first- and second-hand medicines, medicine waste, and information on stock management. These models are to be viewed as long-term goals, and to aid in selecting the issues with the highest priority. This differs from other papers attempting to optimise the PSC, as they approach the problem by modelling the issue as being mathematical and developing heuristic algorithms to find an optimal solution in terms of reducing cost, increasing efficiency, and ensuring reliability of the supply chain [
43]. However, this paper proposes conceptual models of a circular economy of medicines to be combined with the findings from the literature to demonstrate the factors that should be taken into consideration when devising a technological application aimed at enabling medicine reuse.
3.1. A CPSC Organised by Flows
Figure 2 proposes a model for a CPSC composed of two parts: a forward flow and a reverse flow. The aims of this model are to minimise waste by creating a reverse flow that allows the reuse of medicines, highlighting the importance of communication between stages in the PSC, and minimising waste at each stage of the PSC through the implementation of positive behaviours.
The forward flow of the supply chain involves both the movement of medicines (from manufacturer to patient) and the flow of information (from general practitioners (GPs) prescribing medicines to the pharmacies ordering from the manufacturer). The flow of information is vital to prevent shortages/surpluses. The main alterations to the forward flow are the return of any stagnant medicine throughout the PSC to the reverse flow for assessment/reuse and the reuse of medicines within the hospital (as these can be easily assessed).
The reverse flow, inspired by Kongar et al. [
73], will provide every opportunity to minimise wastage through redistribution of eligible medicines, recovering APIs from ineligible but non-harmful medicines, and recovering energy from medicines requiring disposal. Medicines that expire or are damaged within storage are immediately ineligible for reuse and are sent directly to the test for API recovery. The flow of information in the reverse flow informs the manufacturers of quantities within prereuse and preremanufacture storage to allow a more accurate view of the demand for new medicines throughout the entire CPSC.
The principles of CE have been applied throughout the CPSC to reduce strain on the reverse flow by minimising excess waste. These applications include the production of appropriate quantities of medicines with minimal waste, better storage of patient’s own medicines, the reuse of medicines within a hospital, increasing patient adherence by considering alternative prescribing patterns, and closer communication between patients/care homes and the GP regarding medication that is in a patient’s possession. At every point in the CPSC, proper inventory management, stock rotation, and closer communication would aid in reducing medicine waste through stagnation. A specialised tool that shows expiration dates and allows easier communication throughout the supply chain can aid in this by confirming an order is correct, showing trends in data for manufacturers to predict medicine demand, and enabling communication to share medicines between facilities when needed.
The overall reduction of waste and reintroduction of medicines/APIs into the forward supply chain will lead to a reduction in demand for freshly manufactured medicines. This will reduce waste further by minimising excess production. Single-use packaging and fuel consumption is an indirect form of waste in the CPSC and can be countered by employing reusable packaging (i.e., durable boxes or crates to transport medicine), promoting the use of electric vehicles, and minimising the movement of medicines.
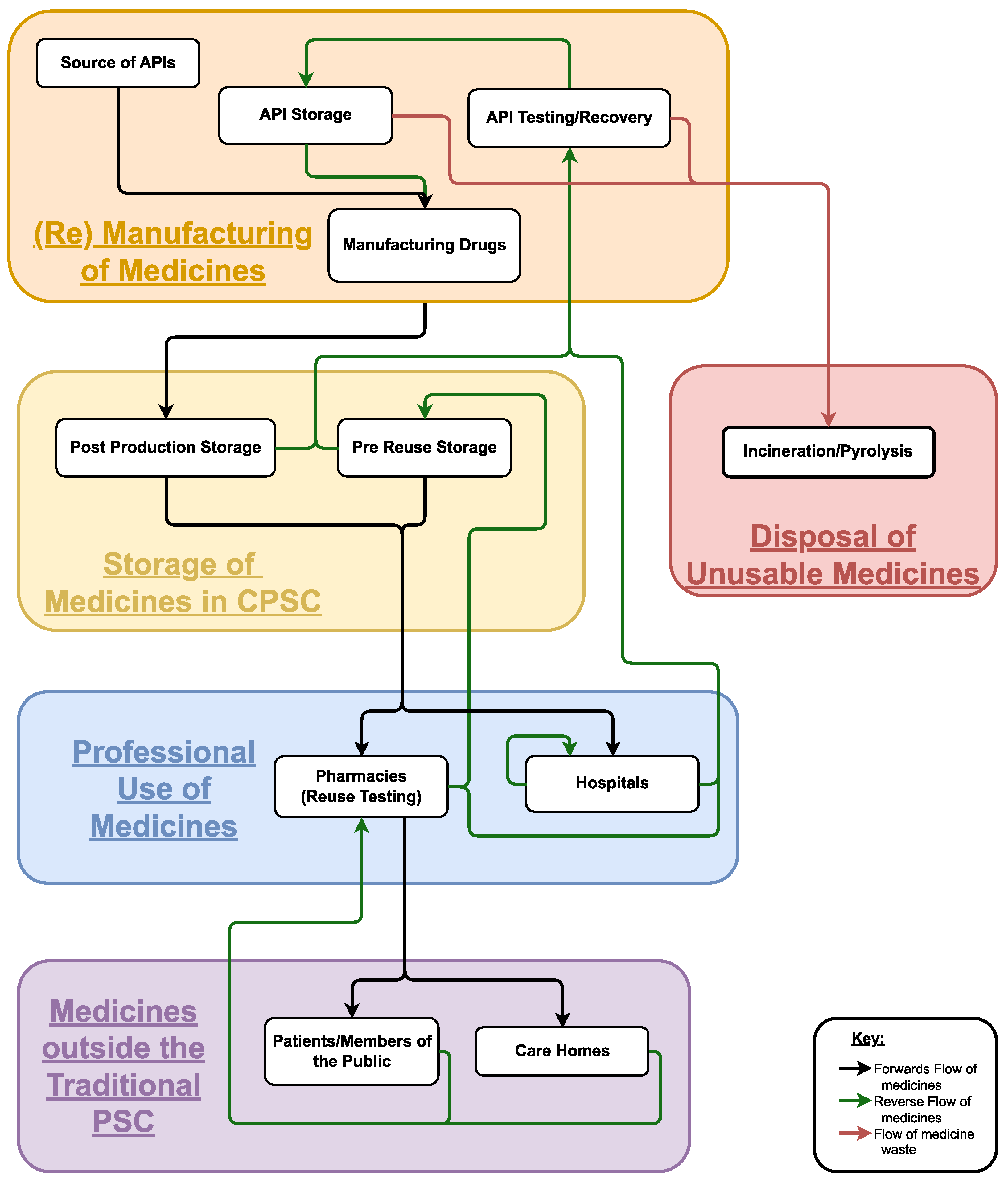
3.2. A CPSC Sorted by Areas of Control
Figure 3 shows the proposed CPSC through a more logistical scope by grouping similar stages by their roles showing the different areas of control. This simplifies the reverse flow, as it allows medicines under the same group to be controlled together.
Through using a system that efficiently assesses returned medicines, the reuse testing can be carried out at a pharmacy, removing the need for a separate stage. These medicines can then be sent to storage if there is a surplus. Through the public returning unused medicines to the pharmacy there is a minimal change to their required behaviour and less of a strain than creating alternative returns assessment facilities. Storage and transport of medicines are handled by the same 3PL for both forward and reverse flows, as they require the same standard protocol. To further simplify the CPSC, API testing and recovery should be carried out by the manufacturer or a related company, as the tasks would require similar equipment and staff training.
The simplification of the CPSC would also allow easier standardisation, monitoring, and updating of operations/policies throughout the CPSC. The proposed CPSC should be seen as a long-term goal and will require surpassing multiple barriers, including changing government and company policies, addressing the concerns of the public/participating organisations to inspire engagement, researching API recovery and dynamic expiry dates, developing safety requirements for medicine reuse, and creating technologies aimed at the supply chain’s safety and efficiency.
To create a feasible system, a model must be agreed upon through a multidisciplinary perspective, requiring work from psychology, politics, pharmacy, engineering, and business [
59,
76]. Attempting to undertake multiple issues simultaneously is likely to reduce the impact of each solution. The best approach is to focus on a single issue, while proposing an expandable system to be used to enable, monitor, and update a CPSC.
3.3. Future Work to Enable a Circular Pharmaceutical Supply Chain
Both the participation from pharmaceutical organisations (by altering everyday operations) and the public (by returning medicines) are required in a CPSC. The next step towards a CPSC should be to enable the reuse of prescription medicines through addressing both the public’s concerns on safety and the stakeholders’ apprehensions of impracticality and excessive cost. This could be done by developing a device to ensure the safety of returns and streamline the assessment process.
To ensure engagement in the system, guidelines can be produced by viewing the problem through the scope of influencing the main groups into adopting large-scale change, as shown in
Table 2. Reduced costs can be achieved through using cheaper/reusable components, ensuring a streamlined assessment process, and creating a reliable system to reduce the chance of legal proceedings. To generate more sales, new or repeat customers can be attracted through reducing costs, broadening product functionality (i.e., ensuring the safety of medicines), or public engagement. Large organisations and the public affect each other. A consumer base can inspire change through purchasing trends and an official endorsement of a public campaign can improve public opinion. When attempting to influence the public, there must be an education program, awareness campaign, or advertisement to inform and encourage the desired behaviours. In a campaign for medicine reuse, the functionality of a system should be presented as at least an equal if not an improvement to its predecessor. It is crucial to consider usability and highlight inclusivity for the entire population. The morality of a change should also be highlighted (i.e., through the additional use of reusable/recyclable components).
Through viewing large-scale changes in recent years, it can be seen that some members of the public have an aversion to required behavioural/routine changes (e.g., recycling and COVID-19 countermeasures). Therefore, minimising changes to the public’s behaviours can increase engagement in the new system. Returning medicines is a crucial change that must be adopted, as the collection of medicines would pose an insurmountable logistical and financial challenge. However, alteration of the outward appearance and functionality of medicine boxes can be minimised. If an updated design is required, this alteration can be staggered by implementing a reuse system to allow the public to adjust to a gradual change. For the purpose of this proposal, the implemented system should have a minimal effect on the exterior of the box.
4. A Smart Packaging and Returns Assessment System (SPaRAS)
As shown in
Table 2, a reliable and efficient system of assessing returned medicines is the vital next step to enable medicine reuse. It will not only ensure the safety of the system, but will also address public and professional concerns surrounding cost efficiency. A practical Smart Packaging and Returns Assessment System (SPaRAS) will ensure medication has been returned before expiry (or a specified threshold), stored in the correct conditions, and unaltered/unadulterated. The inclusion of RFID technology will allow for an effective method of information transfer to reduce the cost and human error in the assessment process.
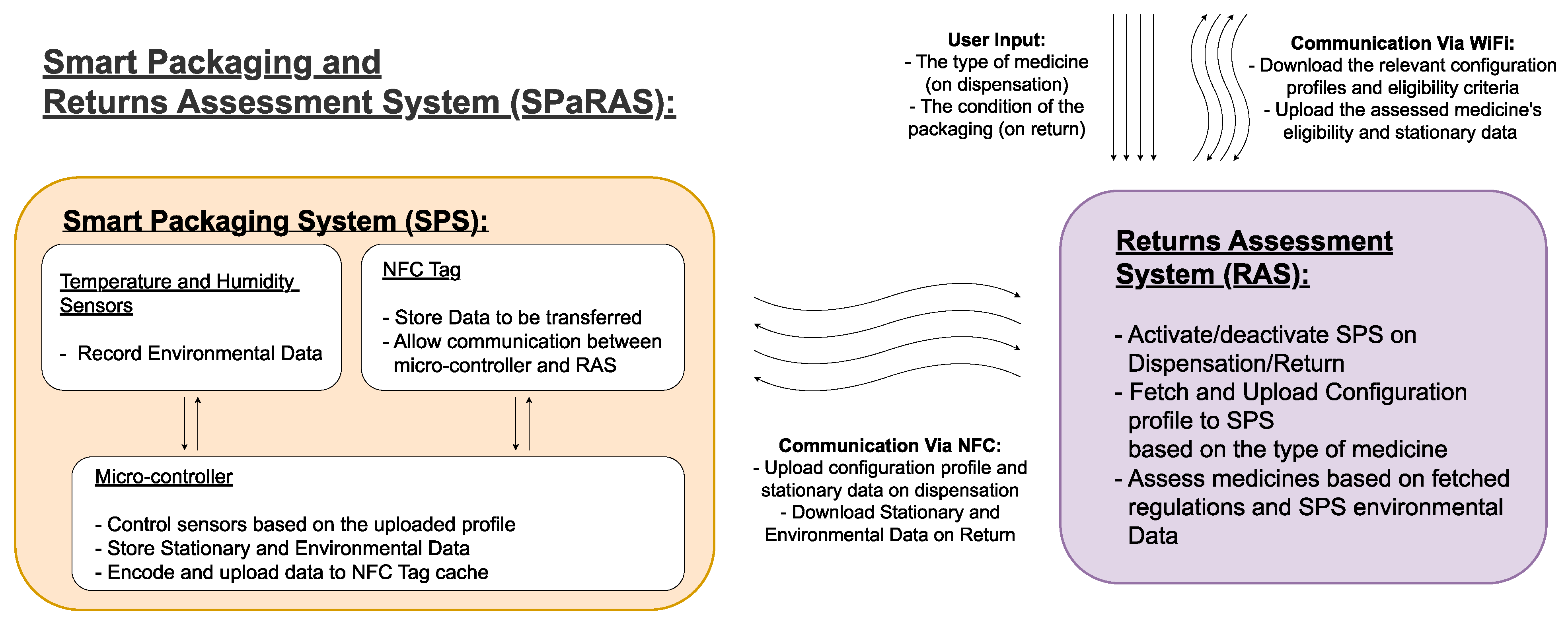
As shown in
Figure 4, SPaRAS will be split into two main components: the smart packaging system (SPS) and the returns assessment system (RAS). The SPS will be a device inserted into medicine packaging that will store key information on the assigned medication and record its storage conditions while in patient care. The RAS will be an application on a pharmacy owned device that will assess returns by comparing the data collected from the SPS to current reuse regulations.
As different medicines require different levels of attention, the SPS will be a generic solution that can be tailored to its assigned medicine. When the medicines are assigned, the RAS will activate the sensors and upload vital data on the medicine. However, this system can also be used to upload a profile to the system that will alter the frequency that the environmental conditions are checked. This will allow less stable medicines with a shorter lifespan (i.e., anti-neoplastic drugs) to be checked more regularly with less concern over the power consumption, while longer lasting medicines can be checked less frequently with a longer lifespan and less data to transfer during assessment.
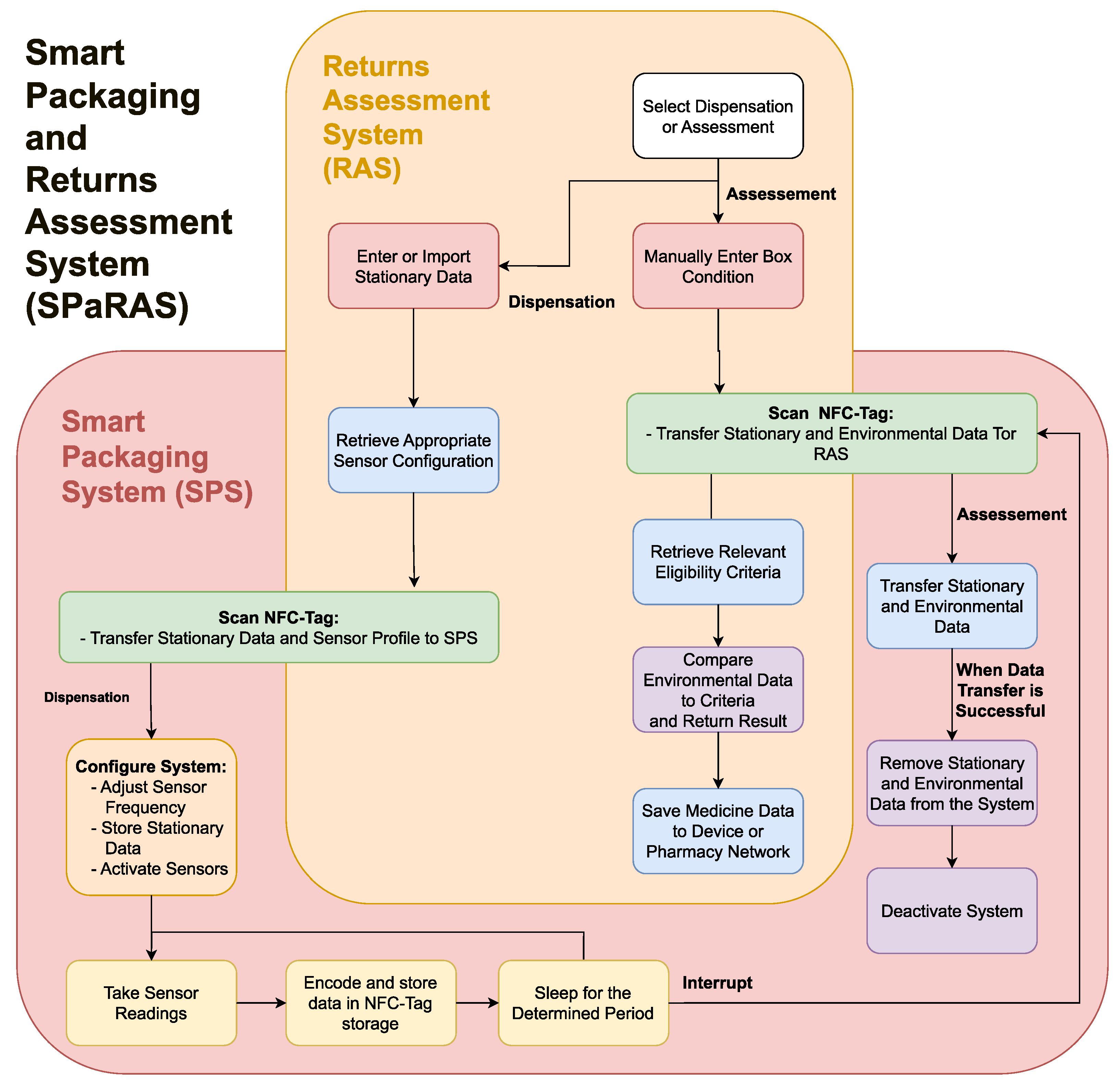
The system will work as an interconnected flow through the two devices, as shown in
Figure 5. This is further broken down to describe the flows of the SPS and RAS in their respective sections. As previously discussed in
Table 2, to ensure public and stakeholder engagement, the system should be cost efficient and reusable, have a minimal change to the exterior of pharmaceutical packaging, and be accessible to those with additional needs. To ensure the system has real world use, stakeholders should be consulted for feedback on the SPS and RAS, while members of the public should be consulted regarding the SPS only. Stakeholders could also be consulted on the feasibility of the potential development of the SPaRAS and the integration of the SPS into a future CPSC.
In order to be successful, the SPS will need to:
Work reliably for the patient-owned duration;
Efficiently communicate with the assessment system;
Fit within a medicine box.
The RAS will need to:
Efficiently transfer data with the smart packaging system;
Control functionality of the SPS;
Accurately compare data from the SPS to determine eligibility;
Be easy to use without extensive training.
4.1. A Streamlined Smart Pharmaceutical Packaging System
A practical smart packaging system can be developed by using the DTTHI and RFID proposals, as influenced by the literature [
60,
73]. The SPS will function as shown in
Figure 6. On dispensation, the SPS will need to receive the stationary data on the medicine (i.e., name, brand, dosage, quantity, and expiry date) from the RAS, as this will be used when the medicines are assessed upon return. The SPS will also need to receive and setup the system using the profile uploaded by the RAS, as this will define the intervals at which environmental readings are taken and could be used to define the eligibility criteria used upon assessment.
Once activated, the system will record the environmental conditions at the preset intervals. The environmental data will need to be encoded to ensure a minimal amount of data is transferred upon assessment. This will be done at regular intervals to ensure all relevant data is ready to be scanned, and to reduce the power consumption. Upon return, the data will be downloaded by the RAS and deleted to enable the system’s reuse.
At the most basic level, the SPS will need a power source, temperature and humidity sensors to record environmental data, a processing unit to store medicine information, control the sensors and manipulate/encode environmental data, and a writable RFID-tag to allow communication with the RAS. Optional additions or future developments to the system are a tamper-proof seal and a physical indicator of the medicine’s eligibility on the exterior of the packaging.
Assuming the devices will not be charged by members of the public, they will need to last until the medicines pass the expiry threshold, which may take years. Once returned to the PSC, it is possible that devices could be recharged wirelessly before being redispensed. Energy harvesting may be considered to simplify the process of recharging a large quantity of devices simultaneously, as this is being developed within the field of wireless sensors [
78]. As the long-term goal is for the system to be used for the majority of medications, the prototype system should be designed with a lifespan of at least one year when the system is configured for more stable medicines. This will require the use of ultra-low power components and simplification of the tasks carried out by the system. The main challenge with selecting a power source will be increasing its longevity while minimizing its size and cost.
The environmental sensors must be able to read the main factors that accelerate medicine degradation (temperature, humidity, and direct light). An ultra-low-power temperature and humidity sensor can be used similar to the DTTHI. However, an electric light sensor may be redundant, as medicines that are exposed to direct light will have a broken tamper-proof seal and will likely be discarded. A physical indicator of medicines’ eligibility (i.e., a small colour indicator on the exterior of the packaging) is unlikely to be included, as this would require a system to self-determine eligibility, requiring more processing power. It could also be considered an unnecessary change by stakeholders and the public.
The DTTHI included a temperature and humidity sensor, power source, micro-controller, WiFi connection, and E-ink display [
60]. A companion cloud database was developed to store the environmental data, which was uploaded in intervals through a WiFi connection. The issues that should be addressed by the SPS include: a battery life (while in active use) of only 6 months, substantial changes to the exterior design and functionality of the packaging, and large/costly components. Although this latter issue could be improved by not using off-the-shelf components and through the creation of an economy of scale, excluding expensive components or those with limited functionality could drastically reduce the cost and power consumption of the SPS.
The visual E-ink display posed several issues. They are relatively expensive, an unnecessary drain on the power and excessively alter the exterior of the box. The display contains a lot of information in various methods that may confuse patients with poor eyesight, learning conditions, or those that are less technically capable. The majority of information displayed is either irrelevant to the general public (e.g., bar graphs displaying the storage conditions and time until expiry, the activation date of the system, and an indicator on the reusability of the medicine) or can be printed on the packaging (the expiry date). The QR code displayed to allow patients to track environmental data in real time can also be printed on the packaging, but is unnecessary as the public do not need specific information to store medicines correctly.
A WiFi connection also presented some problems. The components are expensive, consume relatively high amounts of power, and reduce the functionality of the system. The box would have to be connected to the WiFi to update the server when in the owner’s care. This poses a complicated and time-consuming task and a potential privacy risk. If the user was to travel with the medicines (i.e., on a daily routine or on holiday), or simply did not connect the packages to WiFi within the home, the packages would either not record the data or would have a limit to the amount of data they could record before uploading them to the cloud system. The upload of a large section of the data after being offline could also require large amounts of power. A large portion of the data stored on the database would also be unnecessary, as most medicines would be fully consumed and some medicines would be discarded without being returned. This means that in a large-scale system, the vast majority of the database’s space would be wasted.
RFID technology is a low-cost, low-power alternative method to the method developed by Hui et al. [
60], which would allow efficient transfer or viewing of data by professionals while minimising changes to the appearance or functionality of the packaging. RFID is a technology that has been gaining popularity in recent years, and it is more likely to be developed further, which will more easily allow future developments to increase and expand the functionality of the SPS in the near future [
79]. RFID is used in everyday life without much of a learning curve for the user or a need for additional training to edit the contents of the tag in the case of ID cards and key fobs. RFID tags have been shown to be a reliable method of transferring environmental data when used to record the temperature and humidity of a controlled environment [
80]. An implant to monitor the internal temperature of individual cattle shows the ability for RFID technology to communicate environmental information for an extended period without maintenance [
81].
The use of an RFID tag would reduce the time and human error involved in data transfer as the user would only have to scan the tag and manually approve the condition of the box. A wired connection is less practical when considering the time taken to connect many devices individually as well as the risk of damage while in patient care. RFID is becoming more commonplace in inventory management with its use in the chain Decathlon, allowing a store-wide inventory every 1–4 weeks as opposed to twice a year under the bar-code system and the tracking of stock throughout the supply chain. The benefits of an RFID system far outweigh the costs of its implementation, with Decathlon reporting gains within 5 years of initial testing in 2010 [
82]. In the agro-food industry, the use of RFID tags has increased the safety of food products and transparency with the customer, allowing the tracking of pigs, including monitoring the pig’s diet and tracking the meat as it is processed. This allows the customer to scan the tag and read the information gathered (i.e., date, location, and facility) as the meat goes through the supply chain [
83].
The technology could allow a proposed smart packaging system to be used throughout a CPSC in a passive state for efficient inventory management, similar to the method proposed by Kongar et al. [
73].
4.2. A Returns Assessment System
The RAS will be an application on a smartphone or tablet with an RFID reader and wireless connection to allow communication with the SPS and the pharmacy’s network. The system will be needed to communicate with the SPS on both the dispensation of the medicines and upon its return, as shown in
Figure 7.
On dispensation, the RAS will update the SPS’s stationary data (i.e., name, brand, expiry date, dosage, quantity) based on a user’s input or through scanning the barcode on the medicine packaging, use the stationary information to configure the SPS to the relevant profile based on current regulations, and activate the system. On return, the user will scan the packaging, allowing the RAS to deactivate the system and download the stationary and environmental data. The user will then need to input the condition of the box, as this cannot be measured electronically. The RAS will then fetch the eligibility criteria relevant to the medicine being assessed, compare this to the data from the SPS, and return a pass/fail result. The system will then present the user with the option to save the gathered information for the purposes of inventory management or studying trends in medicine returns. The RAS will require bi-directional communication with the SPS to upload the medicine’s stationary data, configure the SPS for the assigned medicine, and download the environmental data upon return. The connection with the pharmacy’s network is essential to ensure the criteria for reuse eligibility is up to date and to upload the information on the medicine to the pharmacy’s network.
4.3. Context of the Research and Future Applications
The aim of this system is to aid in enabling the reuse of prescription medicines by providing a safe and efficient method for assessing returned medicines. Through the introduction of medicine reuse, SPaRAS could be further developed or used in conjunction with other devices to continue to improve implemented medicine reuse systems. Once a viable SPS is developed and can be implemented, it can be expanded further to carry out other functions. Additional sensors could also be incorporated for medication with specific needs (i.e., those that are light or motion-sensitive). The addition of a wire that breaks with the tamper-proof seal can serve as an electronic method of preventing adulteration of medicines. This would be a useful future addition, as it would cut down on the time an examiner must spend visually assessing each box.
The SPS could later be upgraded to authenticate any returned medicines. With the system involving data transfer, the authentication system can include encrypting the data or adding an authentication code to the data being transferred, but this would fall under a separate project, as the authentication of medicines is currently being heavily researched as a separate topic. The SPS could be further developed to log when medicines are collected or returned by patients to supplement their medical record and a wire mesh could be added to blister packaging to track when medicines are taken. This would allow health services to track adherence in the case of mentally unwell patients and could be used in studies regarding alternative prescription methods. However, this should be limited to areas where consent is given to maintain the public’s right to privacy.
A specialised tool for inventory management would reduce waste at every stage of the pharmaceutical supply chain. With the use of RFID within inventory management becoming more commonplace, the RFID tags in the SPS system could be further developed to integrate with an electronic inventory management database. A centralised inventory management database tailored for a circular pharmaceutical supply chain would need to be developed to minimise waste at all medicine handling facilities. This would entail adjusting the functionality of the system for each separate stage (i.e., a pharmacy would not need the same functionality as a warehouse). At each stage of the CPSC, the database would be able to track the expiry dates of stored medicines, allowing easier stock rotation. If the system’s database was centralised, each facility would be able to share information on quantities of medicines stored throughout the supply chain. This could allow sharing of medicines in times of shortage and redistribution of medicines when there is a surplus to reduce the amount of waste generated by stagnation. The use of RFID not only allows for faster stock management but would also enable the tracking of medicines throughout the PSC. The tracking of flows throughout the supply chain would allow for a more accurate prediction of trends in demand to minimise excess manufacturing.
5. Conclusions
This research assessed the literature surrounding medicine reuse to identify the key barriers to the field and gaps within the literature. Ultimately the review was limited by the infancy of the field, as there were few sources spread over a wide range of themes. However, the novelty of this review is that by sorting sources into separate themes, we were able to consolidate medicine reuse into a distinct field for the first time, draw conclusions from the wide range of topics, and identify the key gaps within the literature. The literature review revealed that two major concerns, the safety and the feasibility of redistributing returned medicines, were raised in multiple studies. The main gap that was addressed within this study was a lack of technological solutions addressing the concerns presented by pharmaceutical stakeholders. However, additional research should be carried out into standardising the criteria for medicine reuse and assessing the different needs of different medication. Further appraisal of the quantity of high-quality unused medicines in patient care is needed, as the current sample size is small. There should also be a focus on methods of increasing public engagement or altering key behaviours, such as the effect of public campaigns on opinions surrounding reuse, to ensure that any solution implemented on a national scale gathers enough participation to be effective.
Building upon previously proposed CE and RL systems for the PSC, a conceptual CPSC model is presented to further explore potential directions of work to facilitate medicine reuse. The original aspects of the presented CPSC were that the proposed reverse flow was placed within the context of the existing PSC and CE principles were applied to each stage of the model to minimise the production of unnecessary medicine waste. Through exploring the changes that would need to be made in order to implement this system, we found that it was vital to ensure the engagement of the public and large pharmaceutical companies in the assessment and redistribution of returned medicines. It is shown by the concerns raised within the literature that any proposed system aimed at enabling medicine reuse should have a basis in increasing the safety while reducing the costs of dispensing medicines. Through considering methods of engaging the public as a consumer base and large pharmaceutical companies, it was decided that in order of any system to be widely accepted, it should be cost effective, be usable by the entire population, and minimise the change to an individual’s routine. This should be applied to any future proposed methods of implementing a CPSC to increase the likelihood of large-scale acceptance. The main constraint of the conceptual framework presented is that it is theoretical. Although there is no way of trialling a CPSC without drastic change to legislation and policies, conceptual frameworks such as this research are tools that can be used to instigate such change. Another limitation of the presented model is that it is such a long-term goal. There may be many unforeseen changes (i.e., technological developments, adjustment of policies, or a shift in public opinions) that could alter how a CPSC would develop. To overcome this issue, future work could be done to revise the model and ensure its continued relevance within the context of contemporary research.
This paper proposes SPaRAS, a novel system able to non-intrusively record the storage conditions of medicines while in patient care, alter its functionality based on the needs of its assigned medicines, and increase the efficiency of assessing returns using RFID technology. To ensure the benefits of SPaRAS outweigh its costs, it will be used for more expensive medicines, especially those with a higher risk of damaging the environment as well as medicines with a shorter lifespan and those that degrade more easily if stored outside the desired conditions. SPaRAS will have a cost similar to clothes tags and the smart tags used within the agro-food industry. The increase of cost or waste from smart packaging systems would be minimised through recharging and reusing each system. Any devices at the end of their lifespan would be recycled. To mitigate the risk of a SPS malfunctioning or running out of power while in patient care, the proposed system would have to be tested and approved by a regulatory body. Once in use, any SPS would be checked by a pharmacist before being used, and any returned medicine with a system that cannot be scanned would be discarded. To negate the risk of information being available to unwanted parties, no personal information (e.g., patient’s name) would be stored on the SPS. To increase the chance of public approval, SPaRAS was designed in response to concerns and suggestions laid out by pharmaceutical stakeholders in previous studies. However, to further improve the engagement with medicine reuse, campaigns to educate the public could be employed to encourage desired behaviours. Future work will be carried out to build and assess an SPaRAS prototype. The system will be assessed to ensure its unsupervised functionality over an extended period. Stakeholders will be shown a prototype and questioned on how SPaRAS affects their confidence in medicine reuse and any alterations that could increase the chance of large-scale acceptance of the system. The precise cost of a smart packaging system will be calculated, considering the battery life and overall lifespan of the device to estimate how many times the system can be reused. The reduction in cost per unit due to an economy of scale would need to be taken into consideration.
The proposal of a CPSC has been shown to pose some risks, including the chance of redistributing damaged, expired, counterfeit, or adulterated medicines. SPaRAS would minimise these risks through enabling the assessment of the storage conditions and expiry date of the medicines. However further application of this system could include an electronic anti-counterfeit mechanism. Further methods to mitigate the risks of redistributing unsafe medicines should include having medicines checked over by pharmacists, introducing new training so that all relevant pharmacy staff can identify and remove unsafe medicines from stock, and provide official guidance from regulatory bodies with standardised criteria for assessing returned medicines.
The key contributions in this paper were the systematic literature review into the field of medicine reuse, the use of a conceptual CPSC model to outline guidelines for the direction of future work, and the proposal of a novel technology aiming at increasing the safety and efficiency of assessing and redistributing returned medicines. The contributions from this research are important, as they build upon findings from previous works to facilitating the reuse of previously owned prescription medicines, which, if achieved, will have major economic and environmental benefits worldwide.












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}