
Practical Guide for Anticoagulant and Antiplatelet Reversal in Clinical Practice
 , , , ,
, , , ,
Abstract
:1. Introduction
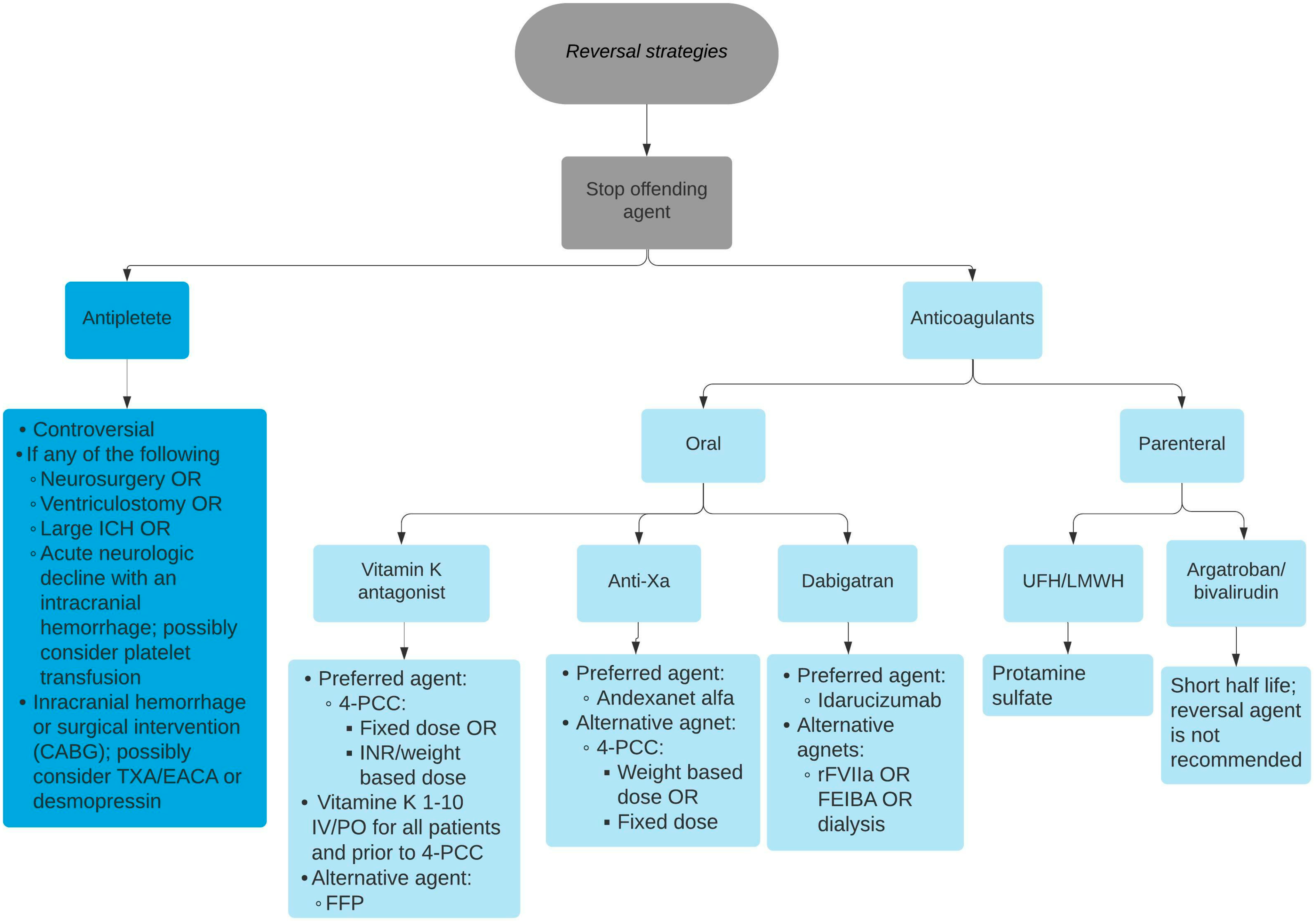
2. Specific Reversal Strategies
2.1. Antiplatelet Drugs
2.1.1. Desmopressin (DDAVP)
2.1.2. Platelet Transfusion
2.1.3. Tranexamic Acid (TXA) and Aminocaproic Acid (EACA)
2.2. Warfarin
2.2.1. Vitamin K (Phytonadione)
2.2.2. Prothrombin Complex Concentrate (PCC)
2.2.3. Fresh Frozen Plasma (FFP)
2.3. Direct Oral Anticoagulants (DOACs)
2.3.1. Coagulation Factor Xa Recombinant, Inactivated-Zhzo (Andexanet Alfa)
2.3.2. Prothrombin Complex Concentrate (PCC)
2.4. Unfractionated Heparin (UFH) and Low-Molecular-Weight Heparin (LMWH)
2.5. Direct Thrombin Inhibitors (Argatroban, Bivalirudin, and Dabigatran)
3. Future Directions
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ho, K.H.; Van Hove, M.; Leng, G. Trends in anticoagulant prescribing: A review of local policies in English primary care. BMC Health Serv. Res. 2020, 20, 279. [Google Scholar] [CrossRef]
- Thethi, I.; Lewis, B.E.; Walenga, J.M. Nonhemostatic Adverse Effects of Anticoagulants and Antiplatelet Agents. Semin. Thromb. Hemost. 2012, 38, 884–892. [Google Scholar] [CrossRef]
- Van Rein, N.; Heide-Jørgensen, U.; Lijfering, W.M.; Dekkers, O.M.; Sørensen, H.T.; Cannegieter, S.C. Major Bleeding Rates in Atrial Fibrillation Patients on Single, Dual, or Triple Antithrombotic Therapy: Results From a Nationwide Danish Cohort Study. Circulation 2019, 139, 775–786. [Google Scholar] [CrossRef]
- Hall, R.; Mazer, C.D. Antiplatelet Drugs: A Review of Their Pharmacology and Management in the Perioperative Period. Anesth. Analg. 2011, 112, 292–318. [Google Scholar] [CrossRef]
- Ageno, W.; Gallus, A.S.; Wittkowsky, A.; Crowther, M.; Hylek, E.M.; Palareti, G. Oral Anticoagulant Therapy. Chest 2012, 141, e44S–e88S. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, B.W.; Bissell, B.D.; Santiago, R.D.; Rech, M.A. Tracing the Lines: A Review of Viscoelastography for Emergency Medicine Clinicians. J. Emerg. Med. 2020, 59, 201–215. [Google Scholar] [CrossRef]
- Price, M.J.; Walder, J.S.; Baker, B.A.; Heiselman, D.E.; Jakubowski, J.A.; Logan, D.K.; Winters, K.J.; Li, W.; Angiolillo, D.J. Recovery of Platelet Function After Discontinuation of Prasugrel or Clopidogrel Maintenance Dosing in Aspirin-Treated Patients With Stable Coronary Disease. J. Am. Coll. Cardiol. 2012, 59, 2338–2343. [Google Scholar] [CrossRef]
- Walle, J.V.; Stockner, M.; Raes, A.; Nørgaard, J.P. Desmopressin 30 years in clinical use: A safety review. Curr. Drug Saf. 2007, 2, 232–238. [Google Scholar] [CrossRef]
- Naidech, A.M.; Maas, M.B.; Levasseur-Franklin, K.E.; Liotta, E.M.; Guth, J.C.; Berman, M.; Rosenow, J.M.; Lindholm, P.F.; Bendok, B.R.; Prabhakaran, S.; et al. Desmopressin Improves Platelet Activity in Acute Intracerebral Hemorrhage. Stroke 2014, 45, 2451–2453. [Google Scholar] [CrossRef] [PubMed]
- Feldman, E.A.; Meola, G.; Zyck, S.; Miller, C.D.; Krishnamurthy, S.; Cwikla, G.M.; Darko, W.; Jennings, S.; Sullivan, R.; Seabury, R. Retrospective Assessment of Desmopressin Effectiveness and Safety in Patients With Antiplatelet-Associated Intracranial Hemorrhage. Crit. Care Med. 2019, 47, 1759–1765. [Google Scholar] [CrossRef] [PubMed]
- Barletta, J.F.; Abdul-Rahman, D.; Hall, S.T.; Mangram, A.J.; Dzandu, J.K.; Frontera, J.A.; Zach, V. The Role of Desmopressin on Hematoma Expansion in Patients with Mild Traumatic Brain Injury Prescribed Pre-injury Antiplatelet Medications. Neurocritical Care 2020, 33, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Gratz, I.; Koehler, J.; Olsen, D.; Afshar, M.; DeCastro, N.; Spagna, P.M.; Ablaza, S.G.; Larijani, G.E. The effect of desmopressin acetate on postoperative hemorrhage in patients receiving aspirin therapy before coronary artery bypass operations. J. Thorac. Cardiovasc. Surg. 1992, 104, 1417–1422. [Google Scholar] [CrossRef]
- Tinegate, H.; Birchall, J.; Gray, A.; Haggas, R.; Massey, E.; Norfolk, D.; Pinchon, D.; Sewell, C.; Wells, A.; Allard, S. Guideline on the investigation and management of acute transfusion reactions Prepared by the BCSH Blood Transfusion Task Force. Br. J. Haematol. 2012, 159, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Baharoglu, M.I.; Cordonnier, C.; Salman, R.A.-S.; de Gans, K.; Koopman, M.M.; Brand, A.; Majoie, C.B.; Beenen, L.F.; Marquering, H.A.; Vermeulen, M.; et al. Platelet transfusion versus standard care after acute stroke due to spontaneous cerebral haemorrhage associated with antiplatelet therapy (PATCH): A randomised, open-label, phase 3 trial. Lancet 2016, 387, 2605–2613. [Google Scholar] [CrossRef] [PubMed]
- Arnone, G.D.; Kumar, P.; Wonais, M.C.; Esfahani, D.R.; Campbell-Lee, S.A.; Charbel, F.T.; Amin-Hanjani, S.; Alaraj, A.; Seicean, A.; Mehta, A.I. Impact of Platelet Transfusion on Intracerebral Hemorrhage in Patients on Antiplatelet Therapy–An Analysis Based on Intracerebral Hemorrhage Score. World Neurosurg. 2018, 111, e895–e904. [Google Scholar] [CrossRef]
- NaidechStorm, A.M.; Liebling, S.M.; Rosenberg, N.F.; Lindholm, P.F.; Bernstein, R.A.; Batjer, H.H.; Alberts, M.J.; Kwaan, H.C. Early Platelet Transfusion Improves Platelet Activity and May Improve Outcomes After Intracerebral Hemorrhage. Neurocritical Care 2012, 16, 82–87. [Google Scholar] [CrossRef]
- Jehan, F.; Zeeshan, M.; Kulvatunyou, N.; Khan, M.; O’Keeffe, T.; Tang, A.; Gries, L.; Joseph, B. Is There a Need for Platelet Transfusion After Traumatic Brain Injury in Patients on P2Y12 Inhibitors? J. Surg. Res. 2019, 236, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Blaine, K.P.; Press, C.; Lau, K.; Sliwa, J.; Rao, V.K.; Hill, C. Comparative effectiveness of epsilon-aminocaproic acid and tranexamic acid on postoperative bleeding following cardiac surgery during a national medication shortage. J. Clin. Anesthesia 2016, 35, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.W.; Shim, J.K.; Youn, Y.N.; Song, J.W.; Yang, S.Y.; Chung, S.C.; Kwak, Y.L. Effect of Tranexamic Acid on Transfusion Requirement in Dual Antiplatelet-Treated Anemic Patients Undergoing Off-Pump Coronary Artery Bypass Graft Surgery—A Randomized Controlled Study: A Randomized Controlled Study. Circ. J. 2012, 76, 96–101. [Google Scholar] [CrossRef]
- Weber, C.F.; Görlinger, K.; Byhahn, C.; Moritz, A.; Hanke, A.A.; Zacharowski, K.; Meininger, D. Tranexamic acid partially improves platelet function in patients treated with dual antiplatelet therapy. Eur. J. Anaesthesiol. 2011, 28, 57–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, J.; Ji, H.; Ren, F.; Wang, G.; Xu, M.; Xue, Y.; Chen, M.; Qi, J.; Li, L. Protective Effects of Tranexamic Acid on Clopidogrel Before Coronary Artery Bypass Grafting: A Multicenter Randomized Trial. JAMA Surg. 2013, 148, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Banihashem, N.; Khorasani, M.; Vaffai, H.; Naziri, F.; Khafri, S.; Seyfi, S. The effect of low- dose tranexamic acid on postoperative blood loss in patients treated with clopidogrel and aspirin. Casp. J. Intern. Med. 2019, 10, 156–161. [Google Scholar] [CrossRef]
- Pleym, H.; Stenseth, R.; Wahba, A.; Bjella, L.; Karevold, A.; Dale, O. Single-Dose Tranexamic Acid Reduces Postoperative Bleeding After Coronary Surgery in Patients Treated with Aspirin Until Surgery. Anesth. Analg. 2003, 96, 923–928. [Google Scholar] [CrossRef]
- Starke, R.M.; Kim, G.H.; Fernandez, A.; Komotar, R.J.; Hickman, Z.L.; Otten, M.L.; Ducruet, A.F.; Kellner, C.P.; Hahn, D.K.; Chwajol, M.; et al. Impact of a Protocol for Acute Antifibrinolytic Therapy on Aneurysm Rebleeding After Subarachnoid Hemorrhage. Stroke 2008, 39, 2617–2621. [Google Scholar] [CrossRef]
- Tomaselli, G.F.; Mahaffey, K.W.; Cuker, A.; Dobesh, P.P.; Doherty, J.U.; Eikelboom, J.W.; Florido, R.; Gluckman, T.J.; Hucker, W.J.; Mehran, R.; et al. 2020 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants. J. Am. Coll. Cardiol. 2020, 76, 594–622. [Google Scholar] [CrossRef] [PubMed]
- Lubetsky, A.; Yonath, H.; Olchovsky, D. Comparison of oral vs. intravenous phytonadione (vitamin K1) in patients with excessive anticoagulation: A prospective randomized controlled study. ACC Curr. J. Rev. 2004, 13, 16. [Google Scholar] [CrossRef]
- Shetty, H.G.; Backhouse, G.; Bentley, D.P.; Routledge, P.A. Effective reversal of warfarin-induced excessive anticoagulation with low dose vitamin K1. Thromb. Haemost. 1992, 67, 013–015. [Google Scholar]
- Pabinger, I.; Brenner, B.; Kalina, U.; Knaub, S.; Nagy, A.; Ostermann, H. Prothrombin complex concentrate (Beriplex® P/N) for emergency anticoagulation reversal: A prospective multinational clinical trial. J. Thromb. Haemost. 2008, 6, 622–631. [Google Scholar] [CrossRef]
- Cabral, K.P.; Fraser, G.L.; Duprey, J.; Gibbons, B.A.; Hayes, T.; Florman, J.E.; Seder, D.B. Prothrombin complex concentrates to reverse warfarin-induced coagulopathy in patients with intracranial bleeding. Clin. Neurol. Neurosurg. 2013, 115, 770–774. [Google Scholar] [CrossRef]
- Goldstein, J.N.; Refaai, M.A.; Milling, T.J.; Lewis, B.; Goldberg-Alberts, R.; Hug, B.A.; Sarode, R. Four-factor prothrombin complex concentrate versus plasma for rapid vitamin K antagonist reversal in patients needing urgent surgical or invasive interventions: A phase 3b, open-label, non-inferiority, randomised trial. Lancet 2015, 385, 2077–2087. [Google Scholar] [CrossRef]
- Sarode, R.; Milling, J.T.J.; Refaai, M.A.; Mangione, A.; Schneider, A.; Durn, B.L.; Goldstein, J.N. Efficacy and Safety of a 4-Factor Prothrombin Complex Concentrate in Patients on Vitamin K Antagonists Presenting With Major Bleeding: A Randomized, Plasma-Controlled, Phase IIIb Study. Circulation 2013, 128, 1234–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makris, M.; Greaves, M.; Phillips, W.S.; Kitchen, S.; Rosendaal, F.R.; Preston, F.E. Emergency Oral Anticoagulant Reversal: The Relative Efficacy of Infusions of Fresh Frozen Plasma and Clotting Factor Concentrate on Correction of the Coagulopathy. Thromb. Haemost. 1997, 77, 477–480. [Google Scholar] [CrossRef]
- Farsad, B.F.; Golpira, R.; Najafi, H.; Totonchi, Z.; Salajegheh, S.; Bakhshandeh, H.; Hashemian, F. Comparison between Prothrombin Complex Concentrate (PCC) and Fresh Frozen Plasma (FFP) for the Urgent Reversal of Warfarin in Patients with Mechanical Heart Valves in a Tertiary Care Cardiac Center. Iran. J. Pharm. Res. 2015, 14, 877. [Google Scholar]
- Momin, J.H.; Candidate; Hughes, G.J. Andexanet Alfa (Andexxa®) for the Reversal of Direct Oral Anticoagulants. Pharm. Ther. 2019, 44, 530–549. [Google Scholar]
- Siegal, D.M.; Curnutte, J.T.; Connolly, S.J.; Lu, G.; Conley, P.B.; Wiens, B.L.; Mathur, V.S.; Castillo, J.; Bronson, M.D.; Leeds, J.M.; et al. Andexanet Alfa for the Reversal of Factor Xa Inhibitor Activity. N. Engl. J. Med. 2015, 373, 2413–2424. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Crowther, M.; Eikelboom, J.W.; Gibson, C.M.; Curnutte, J.T.; Lawrence, J.H.; Yue, P.; Bronson, M.D.; Lu, G.; Conley, P.B.; et al. Full Study Report of Andexanet Alfa for Bleeding Associated with Factor Xa Inhibitors. N. Engl. J. Med. 2019, 380, 1326–1335. [Google Scholar] [CrossRef]
- Majeed, A.; Ågren, A.; Holmström, M.; Bruzelius, M.; Chaireti, R.; Odeberg, J.; Hempel, E.-L.; Magnusson, M.; Frisk, T.; Schulman, S. Management of rivaroxaban- or apixaban-associated major bleeding with prothrombin complex concentrates: A cohort study. Blood 2017, 130, 1706–1712. [Google Scholar] [CrossRef]
- Smith, M.N.; Deloney, L.; Carter, C.; Weant, K.A.; Eriksson, E.A. Safety, efficacy, and cost of four-factor prothrombin complex concentrate (4F-PCC) in patients with factor Xa inhibitor-related bleeding: A retrospective study. J. Thromb. Thrombolysis 2019, 48, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Berger, K.; Santibañez, M.; Lin, L.; Lesch, C.A. A Low-Dose 4F-PCC Protocol for DOAC-Associated Intracranial Hemorrhage. J. Intensive Care Med. 2020, 35, 1203–1208. [Google Scholar] [CrossRef]
- Holzmacher, J.L.; Sarani, B. Indications and Methods of Anticoagulation Reversal. Surg. Clin. North Am. 2017, 97, 1291–1305. [Google Scholar] [CrossRef] [PubMed]
- Sokolowska, E.; Kalaska, B.; Miklosz, J.; Mogielnicki, A. The toxicology of heparin reversal with protamine: Past, present and future. Expert Opin. Drug Metab. Toxicol. 2016, 12, 897–909. [Google Scholar] [CrossRef]
- Desmurs-Clavel, H.; Huchon, C.; Chatard, B.; Negrier, C.; Dargaud, Y. Reversal of the inhibitory effect of Fondaparinux on Thrombin generation by rFVIIa, aCCP and PCC. Thromb. Res. 2009, 123, 796–798. [Google Scholar] [CrossRef]
- Young, G.; Yonekawa, K.E.; Nakagawa, P.A.; Blain, R.C.; Lovejoy, A.E.; Nugent, D.J. Recombinant activated factor VII effectively reverses the anticoagulant effects of heparin, enoxaparin, fondaparinux, argatroban, and bivalirudin ex vivo as measured using thromboelastography. Blood Coagul. Fibrinolysis 2007, 18, 547–553. [Google Scholar] [CrossRef]
- Frontera, J.A.; Iii, J.J.L.; Rabinstein, A.A.; Aisiku, I.P.; Alexandrov, A.W.; Cook, A.M.; del Zoppo, G.J.; Kumar, M.A.; Peerschke, E.I.B.; Stiefel, M.F.; et al. Guideline for Reversal of Antithrombotics in Intracranial Hemorrhage: A Statement for Healthcare Professionals from the Neurocritical Care Society and Society of Critical Care Medicine. Neurocrit. Care 2015, 24, 6–46. [Google Scholar] [CrossRef] [PubMed]
- Pollack, C.V.; Reilly, P.A.; van Ryn, J.; Eikelboom, J.W.; Glund, S.; Bernstein, R.A.; Dubiel, R.; Huisman, M.V.; Hylek, E.M.; Kam, C.-W.; et al. Idarucizumab for Dabigatran Reversal—Full Cohort Analysis. N. Engl. J. Med. 2017, 377, 431–441. [Google Scholar] [CrossRef]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef]
- Bakhru, S.; Laulicht, B.; Jiang, X.; Chen, L.; Pan, D.; Grosso, M.; Morishima, Y.; Brown, K.; Masumoto, H.; Costin, J.; et al. A synthetic small molecule which reverses over-dosage and bleeding by the new oral anticoagulants. Circulation 2013, 128, A18809. [Google Scholar]
- Ansell, J.E.; Bakhru, S.H.; Laulicht, B.E.; Steiner, S.S.; Grosso, M.; Brown, K.; Dishy, V.; Noveck, R.J.; Costin, J.C. Use of PER977 to Reverse the Anticoagulant Effect of Edoxaban. N. Engl. J. Med. 2014, 371, 2141–2142. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Anticoagulant | aPTT | PT/INR | Elimination Half-Life | Effect of Dialysis |
|---|---|---|---|---|
| Warfarin | Increase or neutral | Increase | 7 days | Not dialyzable |
| Rivaroxaban | Increase or neutral | Increase or neutral | 5–9 h | Not dialyzable |
| Apixaban | Increase or neutral | Increase or neutral | 12 h | Poorly dialyzable |
| Edoxaban | Neutral | Increase or neutral | 10–14 h | Not dialyzable |
| Betrixaban | Increase | Increase | 19–27 h | Not dialyzable |
| Argatroban | Increase | Increase | 30–50 min | Poorly dialyzable |
| Dabigatran | Increase | Increase or neutral | 12–17 h | Dialyzable |
| Bivalirudin | Increase | Increase or neutral | 20–25 min | Poorly dialyzable |
| IV UFH | Increase | Neutral | 30 min | Not dialyzable |
| LMWH | Increase or neutral | Neutral | 4.5–5 h | Not dialyzable |
| Targeted Medication | Suggested Reversal Agent | Suggested Reversal Agent Dose | Adverse Reactions |
|---|---|---|---|
| DDAVP | 0.3–0.4 mcg/kg/dose |
|
| Platelet transfusion | Up to a single apheresis unit or equivalent. Greater doses are not more effective, and lower doses equal to one-half of a standard apheresis unit are equally effective |
| |
| TXA | Loading dose (IV bolus): 1 g, 100 mg/kg or 10 mg/kg Maintenance dose: 30 mg/kg, 200 mg/h, 10 mg/kg, 50 mg/kg or 10 mg/kg |
| |
| EACA | Loading dose (IV bolus): 4 g Maintenance dose (CIVI): 1 g/h, with a maximum infusion of 4 h |
| |
| Warfarin | Vitamin K | Minor bleed: 2–5 mg PO/IV Major bleed: 5–10 mg IV |
|
| 4F-PCC |
|
| |
| FFP | 10–30 mL/kg (1-unit FFP has a volume of 250 mL) |
| |
| 4F-PCC | 25–50 units/kg based on actual body weight |
|
| Andexanet alfa | Last dose within <8 h or time is unknown for rivaroxaban ≤ 10 mg and apixaban ≤ 5 mg or when last dose within >8 h with any dose given: Low dose: 400 mg at a target rate of 30 mg/min followed by 4 mg/min for up to 120 min (480 mg) Last dose within <8 h or time is unknown for rivaroxaban > 10 mg and apixaban > 5 mg: High dose: 800 mg at a target rate of 30 mg/min followed by 8 mg/min for up to 120 min (960 mg) |
| |
| Direct thrombin inhibitors: Dabigatran | 4F-PCC | 25–50 units/kg based on actual body weight |
|
| Idarucizumab | 5 g IV bolus (two separate doses of 2.5 g diluted in 50 mL vials) |
| |
| UFH and LMWH | Protamine sulfate | For UFH reversal: 1 mg for every 100 units when used within 2–4 h from the last UFH exposure For LMWH reversal: 1 mg for each 1 mg administered within the prior eight hours |
|
Direct thrombin inhibitors: Argatroban; Bivalirudin; Fondaparinux. | rFVIIa | 70–90 mcg/kg |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aldhaeefi, M.; Badreldin, H.A.; Alsuwayyid, F.; Alqahtani, T.; Alshaya, O.; Al Yami, M.S.; Bin Saleh, K.; Al Harbi, S.A.; Alshaya, A.I. Practical Guide for Anticoagulant and Antiplatelet Reversal in Clinical Practice. Pharmacy 2023, 11, 34. https://doi.org/10.3390/pharmacy11010034
Aldhaeefi M, Badreldin HA, Alsuwayyid F, Alqahtani T, Alshaya O, Al Yami MS, Bin Saleh K, Al Harbi SA, Alshaya AI. Practical Guide for Anticoagulant and Antiplatelet Reversal in Clinical Practice. Pharmacy. 2023; 11(1):34. https://doi.org/10.3390/pharmacy11010034
Chicago/Turabian StyleAldhaeefi, Mohammed, Hisham A. Badreldin, Faisal Alsuwayyid, Tariq Alqahtani, Omar Alshaya, Majed S. Al Yami, Khalid Bin Saleh, Shmeylan A. Al Harbi, and Abdulrahman I. Alshaya. 2023. "Practical Guide for Anticoagulant and Antiplatelet Reversal in Clinical Practice" Pharmacy 11, no. 1: 34. https://doi.org/10.3390/pharmacy11010034