


Evaluating Edge Computing and Compression for Remote Cuff-Less Blood Pressure Monitoring


Abstract
:1. Introduction
2. Background
2.1. Cuff-Less Blood Pressure Estimation
2.2. Compression Algorithms for ECG Signals
3. System and Experiment Design
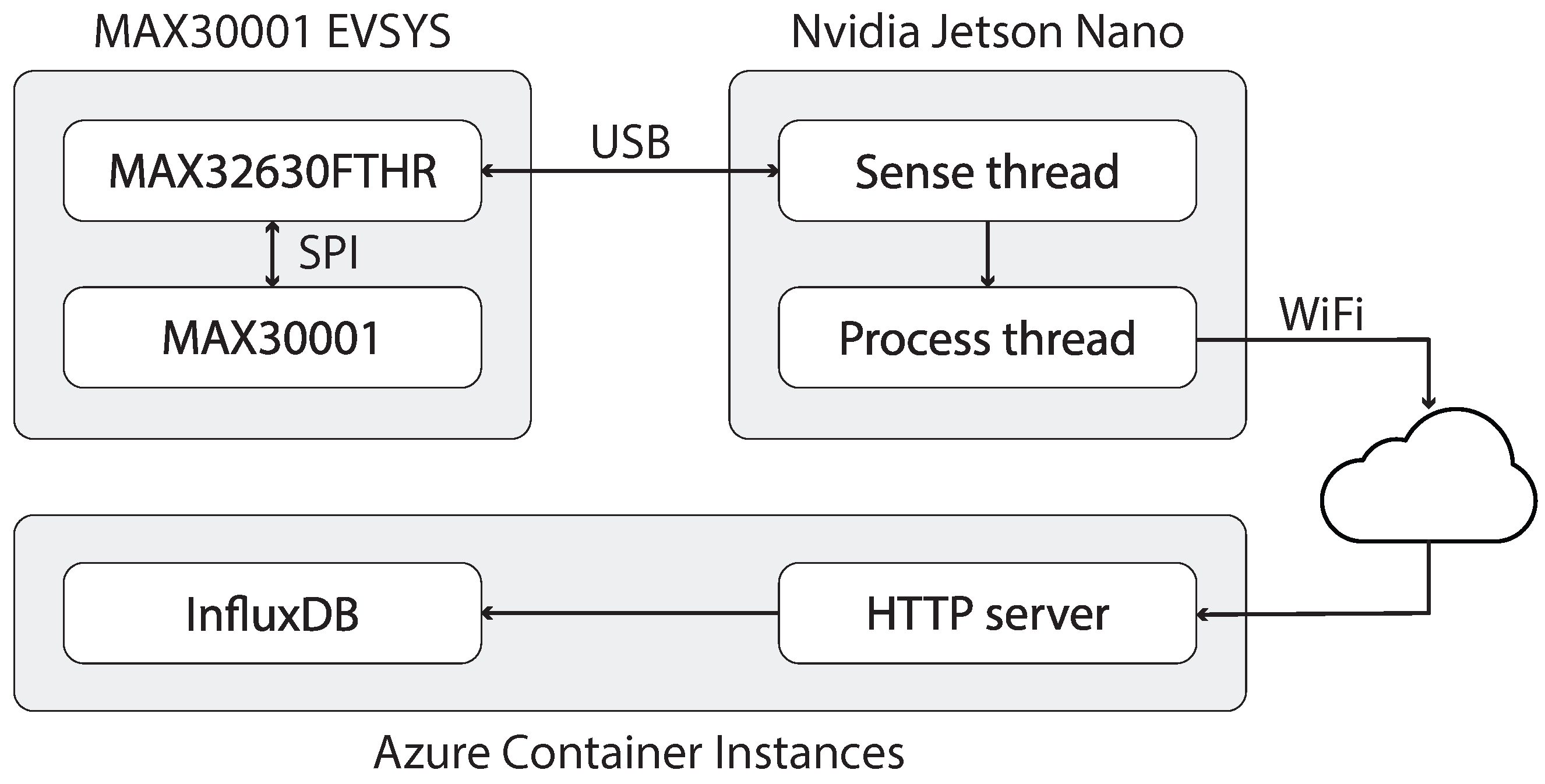
3.1. System Design
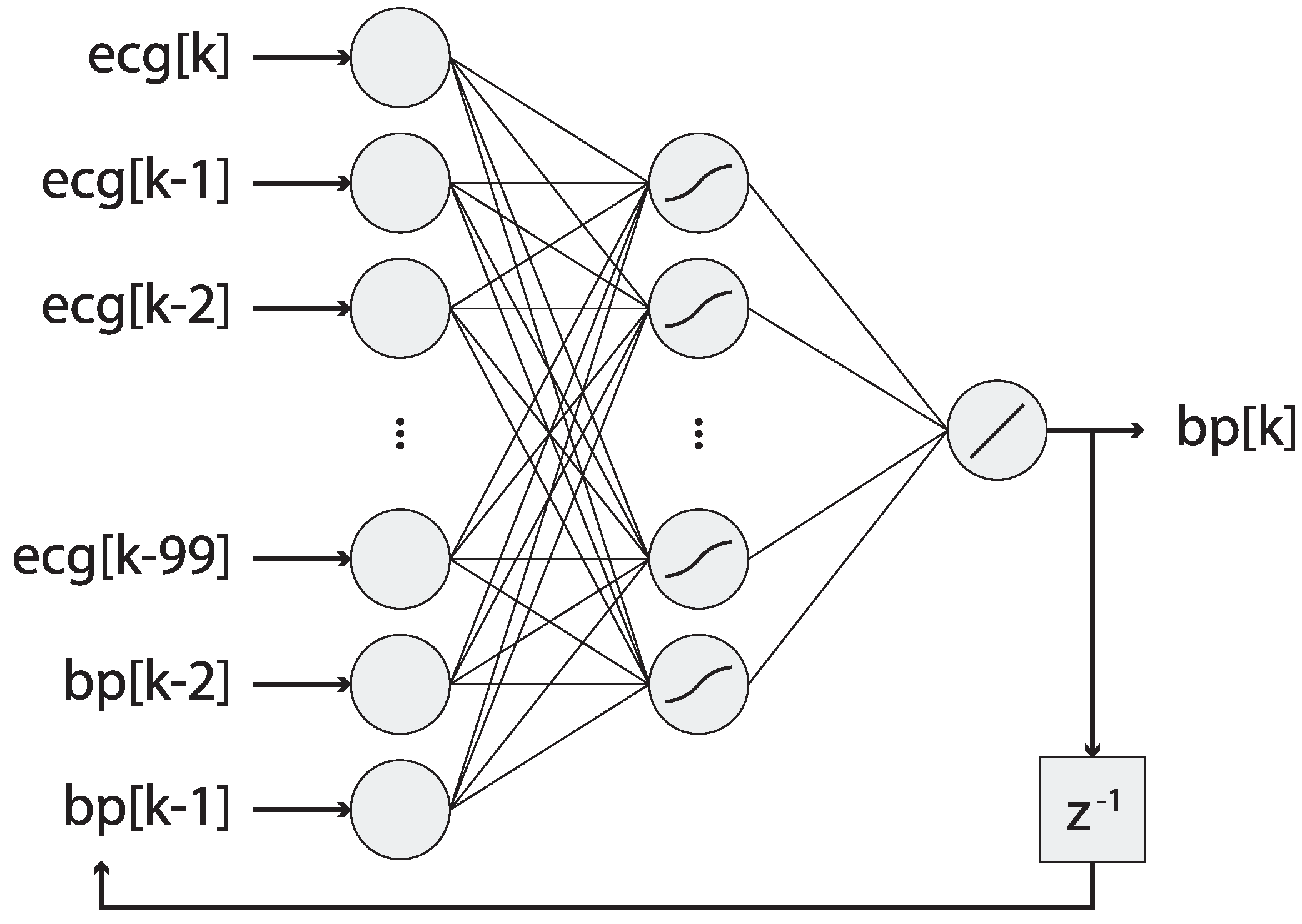
3.2. Bloodpressure Estimator
3.3. Metric Definitions
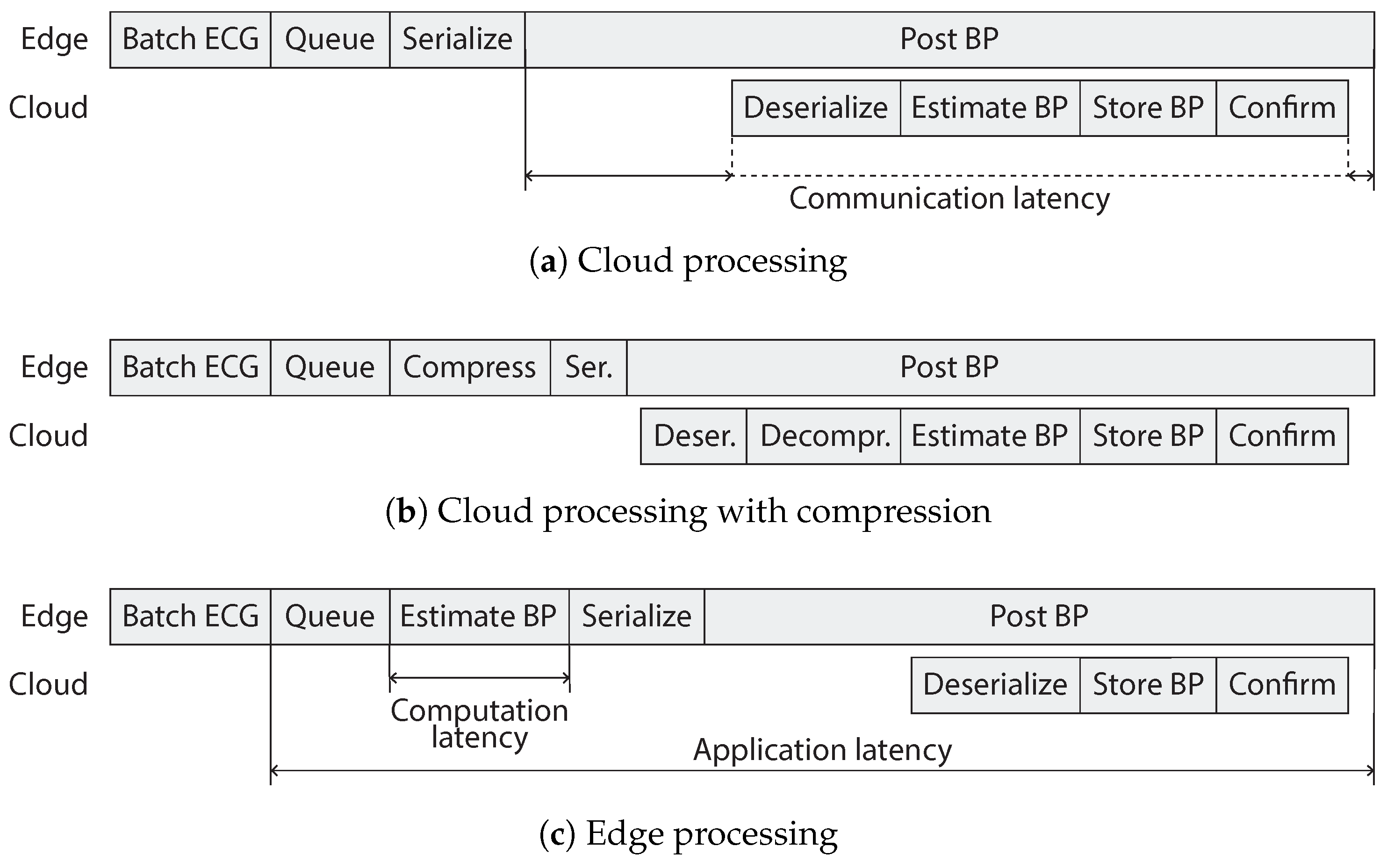
3.4. Experiments
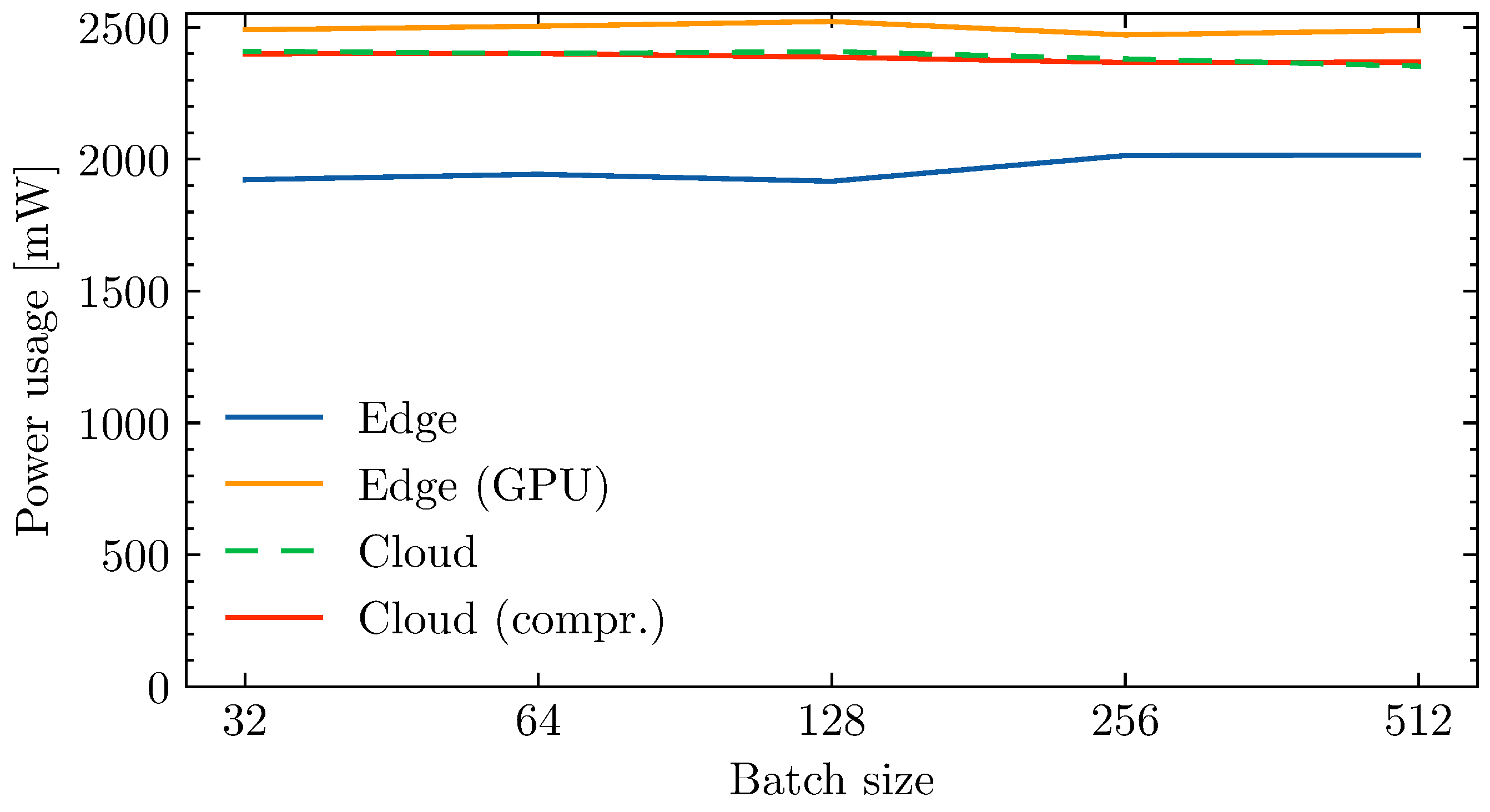
4. Results and Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BP | Blood pressure |
| ECG | Electrocardiogram |
| GPU | Graphics Processing Unit |
| SBP | Systolic blood pressure |
| DBP | Diastolic blood pressure |
| MAP | Mean arterial pressure |
| ML | Machine learning |
| NARX | Nonlinear autoregressive exogenous |
| ANN | Artificial neural network |
| LSTM | Long short term memory |
| BiLSTM | Bidirectional long short term memory |
| FC | Fully connected |
| MAE | Mean absolute error |
| ME | Mean error |
| RTT | Round trip time |
References
- Dumka, A.; Sah, A. Chapter 6—Smart ambulance system using concept of big data and internet of things. In Healthcare Data Analytics and Management; Dey, N., Ashour, A.S., Bhatt, C., James Fong, S., Eds.; Advances in Ubiquitous Sensing Applications for Healthcare; Academic Press: Cambridge, MA, USA, 2019; pp. 155–176. [Google Scholar] [CrossRef]
- Hartmann, M.; Hashmi, U.S.; Imran, A. Edge computing in smart health care systems: Review, challenges, and research directions. Trans. Emerg. Telecommun. Technol. 2019, 33, e3710. [Google Scholar] [CrossRef]
- Abdellatif, A.A.; Mohamed, A.; Chiasserini, C.F.; Tlili, M.; Erbad, A. Edge Computing for Smart Health: Context-Aware Approaches, Opportunities, and Challenges. IEEE Netw. 2019, 33, 196–203. [Google Scholar] [CrossRef] [Green Version]
- Jha, C.K.; Kolekar, M.H. Electrocardiogram Data Compression Techniques for Cardiac Healthcare Systems: A Methodological Review. IRBM 2021, 43, 217–228. [Google Scholar] [CrossRef]
- Fan, X.; Wang, H.; Xu, F.; Zhao, Y.; Tsui, K.L. Homecare-Oriented Intelligent Long-Term Monitoring of Blood Pressure Using Electrocardiogram Signals. IEEE Trans. Ind. Inform. 2020, 16, 7150–7158. [Google Scholar] [CrossRef]
- Simjanoska, M.; Gjoreski, M.; Gams, M.; Madevska Bogdanova, A. Non-Invasive Blood Pressure Estimation from ECG Using Machine Learning Techniques. Sensors 2018, 18, 1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mousavi, S.S.; Hemmati, M.; Charmi, M.; Moghadam, M.; Firouzmand, M.; Ghorbani, Y. Cuff-Less Blood Pressure Estimation Using Only the ECG Signal in Frequency Domain. In Proceedings of the 2018 8th International Conference on Computer and Knowledge Engineering (ICCKE), Mashhad, Iran, 25–26 October 2018; pp. 147–152. [Google Scholar] [CrossRef]
- Mousavi, S.S.; Charmi, M.; Firouzmand, M.; Hemmati, M.; Moghadam, M. A New Approach Based on Dynamical Model of The ECG Signal to Blood Pressure Estimation. In Proceedings of the 2019 4th International Conference on Pattern Recognition and Image Analysis (IPRIA), Tehran, Iran, 6–7 March 2019; pp. 210–215. [Google Scholar] [CrossRef]
- Landry, C.; Peterson, S.D.; Arami, A. Estimation of the Blood Pressure Waveform using Electrocardiography. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 7060–7063. [Google Scholar] [CrossRef]
- Fan, X.; Wang, H.; Zhao, Y.; Li, Y.; Tsui, K. An Adaptive Weight Learning-Based Multitask Deep Network for Continuous Blood Pressure Estimation Using Electrocardiogram Signals. Sensors 2021, 21, 1595. [Google Scholar] [CrossRef] [PubMed]
- Miao, F.; Wen, B.; Hu, Z.; Fortino, G.; Wang, X.P.; Liu, Z.D.; Tang, M.; Li, Y. Continuous blood pressure measurement from one-channel electrocardiogram signal using deep-learning techniques. Artif. Intell. Med. 2020, 108, 101919. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Wang, X.K.; Wang, L.H. Noninvasive Blood Pressure Classification based on ECG with ResNet Algorithm. In Proceedings of the 2021 IEEE International Conference on Consumer Electronics-Taiwan (ICCE-TW), Penghu, Taiwan, 15–17 September 2021; pp. 1–2. [Google Scholar] [CrossRef]
- Johnson, A.E.W.; Pollard, T.J.; Shen, L.; Lehman, L.w.H.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Anthony Celi, L.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kachuee, M.; Kiani, M.M.; Mohammadzade, H.; Shabany, M. Cuff-less high-accuracy calibration-free blood pressure estimation using pulse transit time. In Proceedings of the 2015 IEEE International Symposium on Circuits and Systems (ISCAS), Lisbon, Portugal, 24–27 May 2015; pp. 1006–1009. [Google Scholar] [CrossRef]
- Tiwari, A.; Falk, T.H. Lossless electrocardiogram signal compression: A review of existing methods. Biomed. Signal Process. Control 2019, 51, 338–346. [Google Scholar] [CrossRef]
- Tsai, T.H.; Kuo, W.T. An Efficient ECG Lossless Compression System for Embedded Platforms with Telemedicine Applications. IEEE Access 2018, 6, 42207–42215. [Google Scholar] [CrossRef]
- Cooke, R.A.; Fahmy, S.A. Quantifying the latency benefits of near-edge and in-network FPGA acceleration. In Proceedings of the Third ACM International Workshop on Edge Systems, Analytics and Networking; EdgeSys’20; Association for Computing Machinery: Heraklion, Greece, 2020; pp. 7–12. [Google Scholar] [CrossRef]
- Tarjan, D.; Skadron, K.; Micikevicius, P. The Art of Performance Tuning for Cuda and Manycore Architectures. In Birds-of-a-feather session at Supercomputing (SC). 2009. Available online: https://www.cs.virginia.edu/~skadron/Papers/cuda_tuning_bof_sc09_final.pdf (accessed on 29 April 2022).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | ECG Lead | Feature Extraction | Inference | Dataset | Result Metric | Results |
|---|---|---|---|---|---|---|
| [6] | I, II or III | ✓ | Stacked ML classifier Random forest regression | Self recorded | MAE | SBP: 7.72 ± 10.22 mmHg DBP: 9.45 ± 10.03 mmHg MAP: 8.13 ± 8.84 mmHg |
| [7] | II | ✓ | Random forest regression | MIMIC II v3.0 | MAE | SBP: 12.75 ± 12.15 mmHg DBP: 6.04 ± 6.42 mmHg MAP: 7.01 ± 7.00 mmHg |
| [8] | V5/V6 or V1/V2 | ✓ | AdaBoostR | CVES | ME | SBP: 1.125 ± 3.125 mmHg |
| [9] | Not reported | ✗ | NARX | MIMIC II v3.0 | ME | SBP: −4.0 ± 5.9 mmHg DBP: 1.13 ± 2.9 mmHg |
| [5] | II | ✗ | BiLSTM | MIMIC II v3.0 | MAE | SBP: 7.16 ± 10.83 mmHg DBP: 3.89 ± 5.90 mmHg MAP: 4.24 ± 6.47 mmHg |
| [11] | II | ✗ | Res-LSTM | MIMIC III | MAE | SBP: 7.10 ± 9.99 mmHg DBP: 4.61 ± 6.29 mmHg MAP: 4.66 ± 6.36 mmHg |
| [10] | II | ✗ | BiLSTM | MIMIC II v3.0 | MAE | SBP: 7.69 ± 12.3 mmHg DBP: 4.36 ± 6.88 mmHg MAP: 4.76 ± 7.52 mmHg |
| [12] | II | ✗ | ResNet-18 | Cuff-Less Blood Pressure Estimation Data Set | 87.89% accuracy (classification) |
| Method | Edge | Cloud | Cloud (Compr.) |
|---|---|---|---|
| Queue | 14.118 | 1.118 | 3.703 |
| Computation | 81.808 | 11.591 | 14.445 |
| Communication | 72.09 | 67.585 | 130.546 |
| Compression | - | - | 55.513 |
| Decompression | - | - | 16.612 |
| Application | 240.673 | 156.918 | 304.981 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goossens, W.; Mustefa, D.; Scholle, D.; Fotouhi, H.; Denil, J. Evaluating Edge Computing and Compression for Remote Cuff-Less Blood Pressure Monitoring. J. Sens. Actuator Netw. 2023, 12, 2. https://doi.org/10.3390/jsan12010002
Goossens W, Mustefa D, Scholle D, Fotouhi H, Denil J. Evaluating Edge Computing and Compression for Remote Cuff-Less Blood Pressure Monitoring. Journal of Sensor and Actuator Networks. 2023; 12(1):2. https://doi.org/10.3390/jsan12010002
Chicago/Turabian StyleGoossens, Ward, Dino Mustefa, Detlef Scholle, Hossein Fotouhi, and Joachim Denil. 2023. "Evaluating Edge Computing and Compression for Remote Cuff-Less Blood Pressure Monitoring" Journal of Sensor and Actuator Networks 12, no. 1: 2. https://doi.org/10.3390/jsan12010002