
Long-Term Exercise Assistance: Group and One-on-One Interactions between a Social Robot and Seniors

 , ,
, ,
Abstract
:1. Introduction
2. Related Works
2.1. Socially Assistive Robots for Exercise Facilitation
2.1.1. Socially Assistive Robots for Exercise Facilitation in One-on-One Settings
2.1.2. Socially Assistive Robots for Exercise Facilitation in Group Settings
2.1.3. Socially Assistive Robots for Exercise Facilitation in Both One-on-One and Group Settings
2.2. General HRI Studies Comparing Group vs. One-on-One Interactions
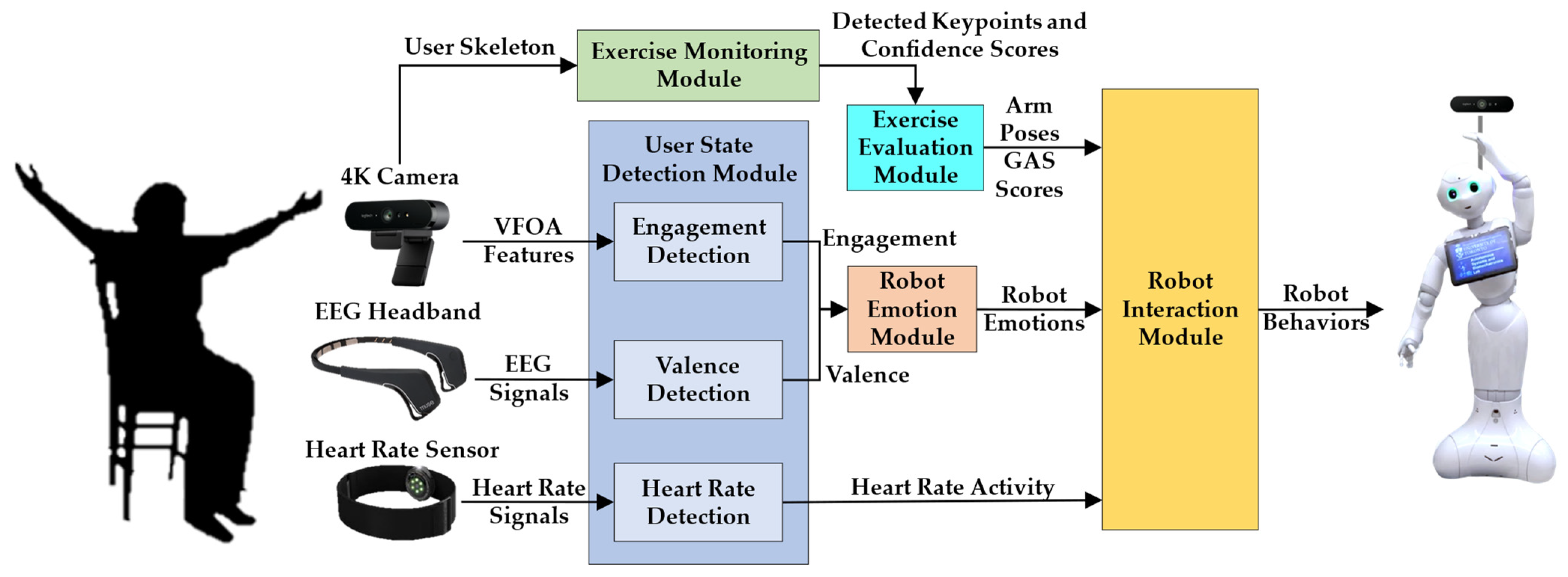
3. Social Robot Exercise Facilitator
3.1. Exercise Monitoring Module
3.2. Exercise Evaluation Module
3.3. User State Detection Module
3.3.1. Valence
3.3.2. Engagement
3.3.3. Heart Rate
3.4. Robot Emotion Module
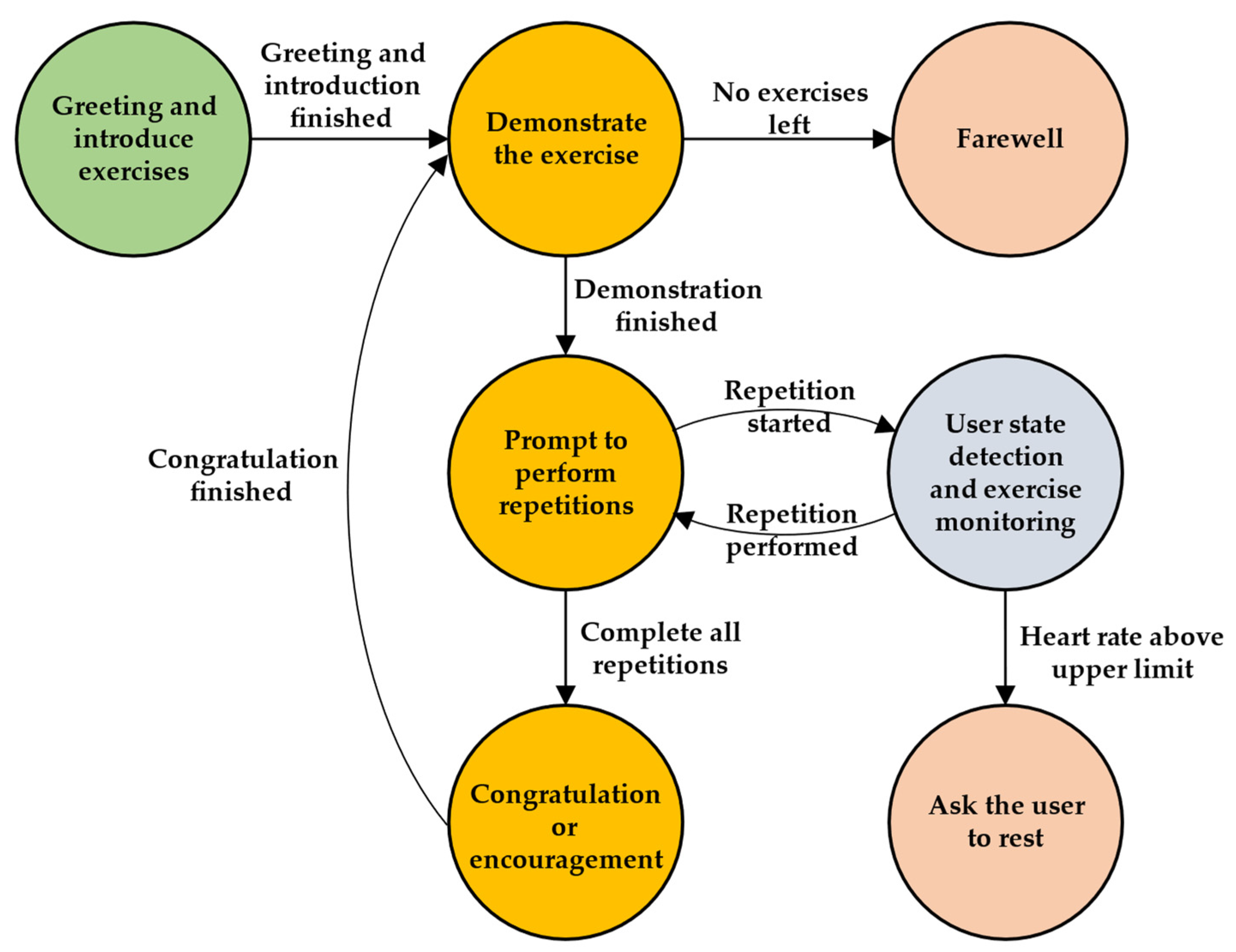
3.5. Robot Interaction Module
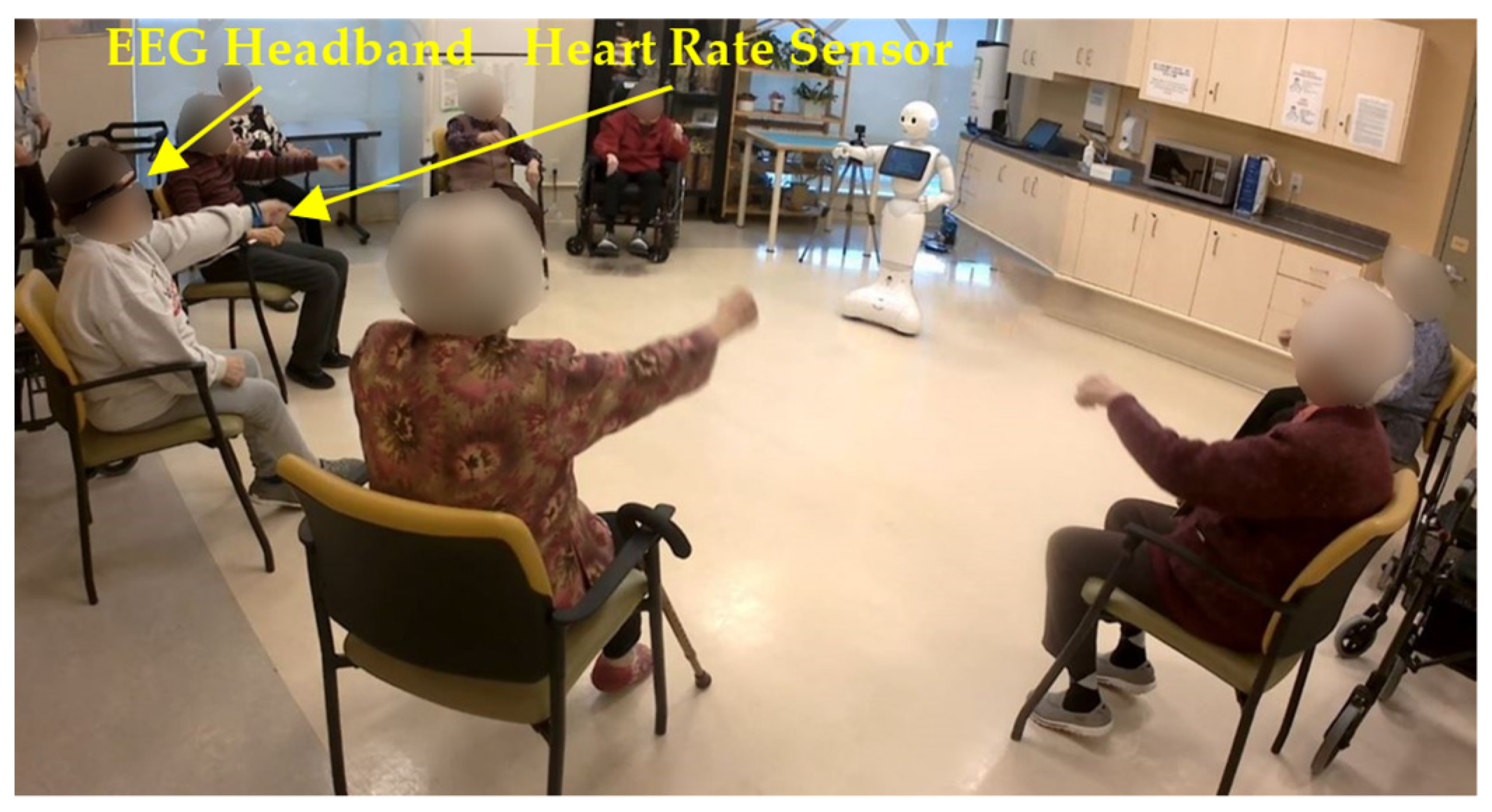
4. Exercise Experiments
4.1. Participants
4.2. Experimental Design
4.3. Experimental Procedure
4.4. Measures
5. Results
5.1. Exercise Evaluation Results
5.1.1. One-on-One Sessions
5.1.2. Group Sessions
5.2. User State Detection and Robot Emotion Results
5.2.1. One-on-One Sessions
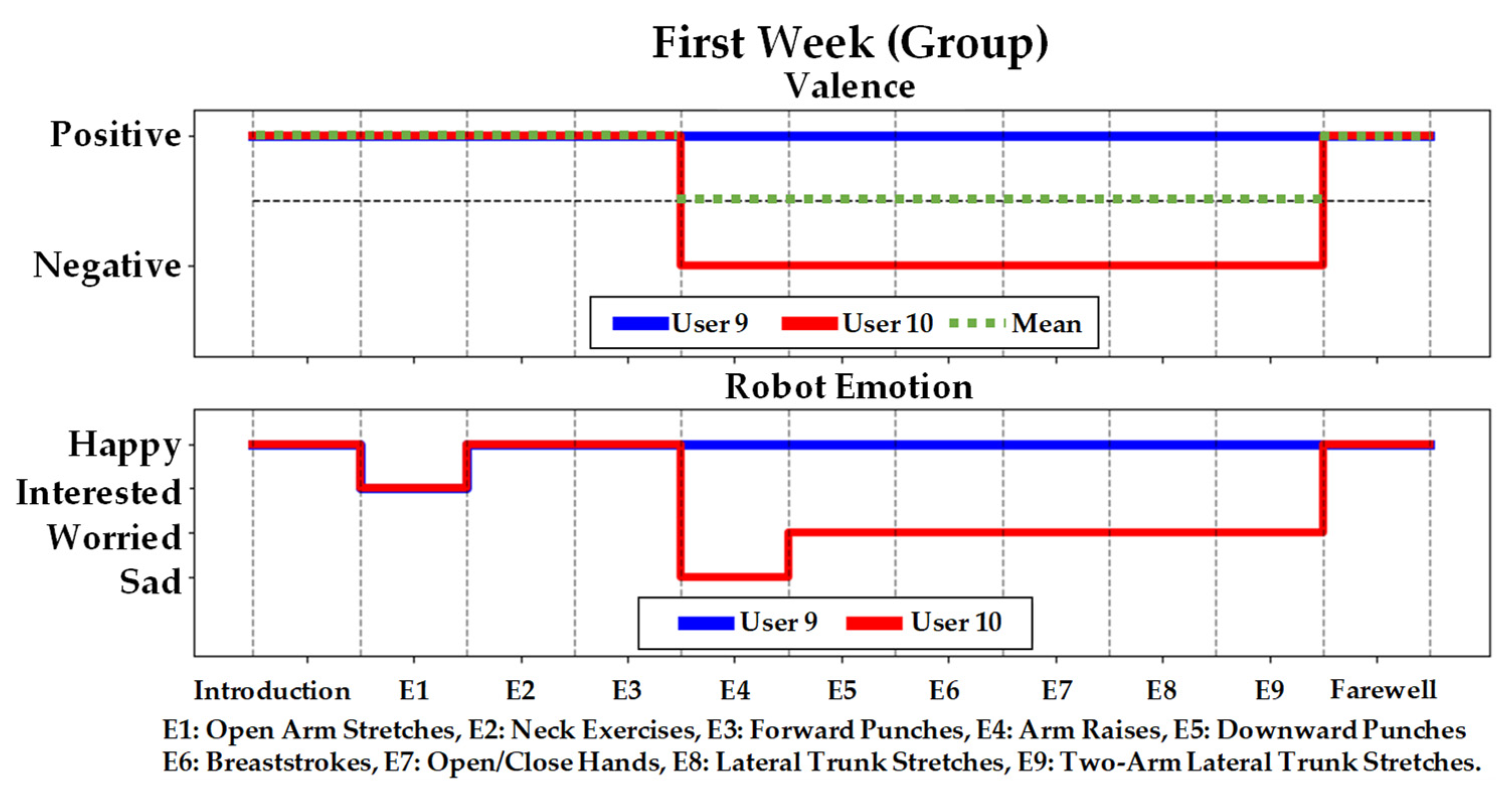
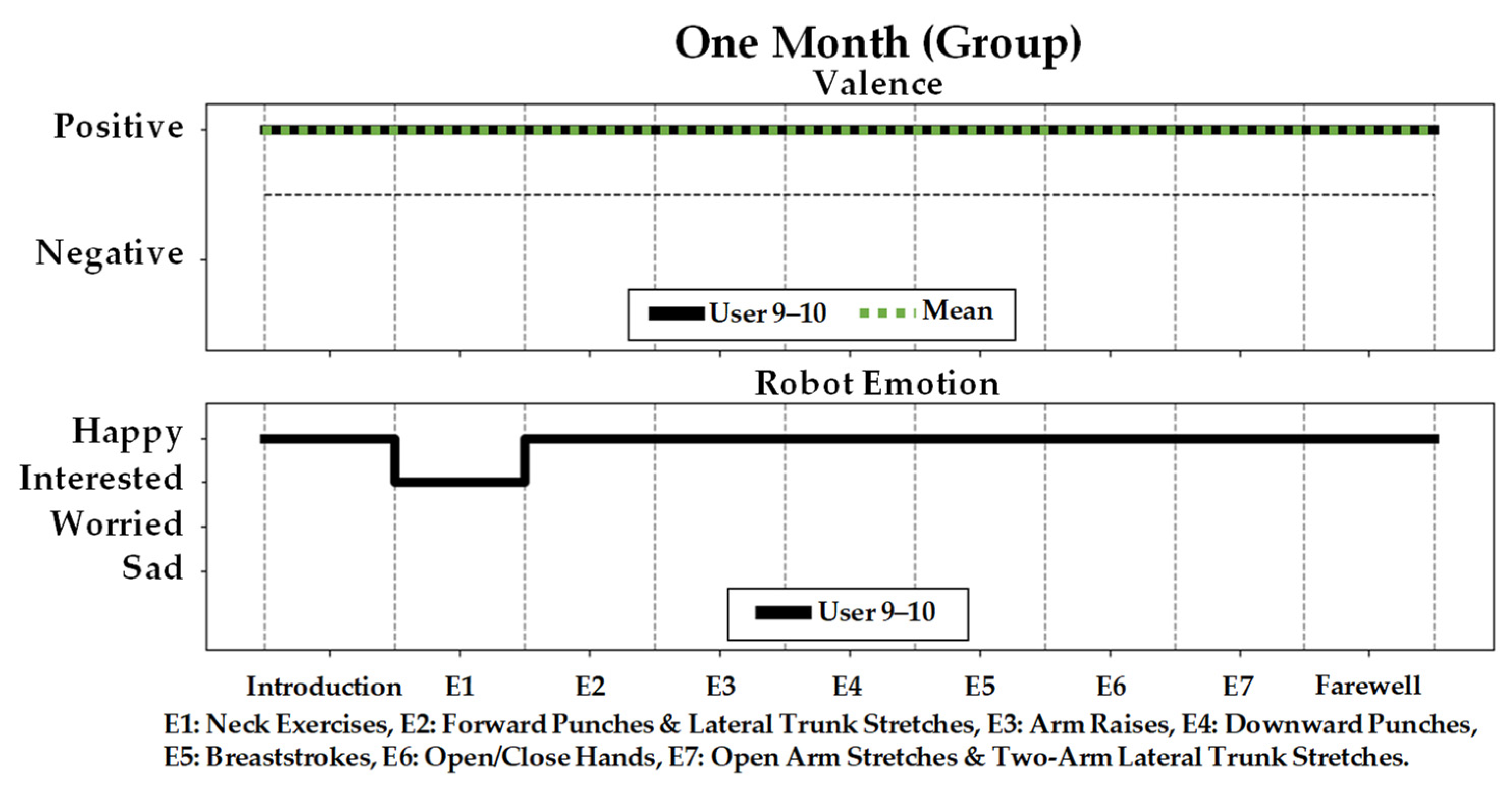
5.2.2. Group Sessions
5.3. Self-Reported Valence (SAM Scale)
5.4. Robot Perception Questionnaire
5.4.1. Acceptance
5.4.2. Perceived Usefulness and Ease of Use
5.4.3. Perceived Sociability and Intelligence
5.4.4. Robot Appearance and Movements
5.4.5. Overall Experience
5.4.6. Robot Features and Alternative Activities
6. Discussions
6.1. User State Detection and Robot Emotion Results
6.2. Self-Reported Valence (SAM Scale)
6.3. Acceptance
6.4. Perceived Usefulness and Ease of Use
6.5. Perceived Sociability and Intelligence
6.6. Robot Appearance and Movements
6.7. Considerations and Limitations
6.8. Future Research Directions
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Details of the Social Robot Exercise Facilitator
Appendix A.1. Exercise Monitoring Module
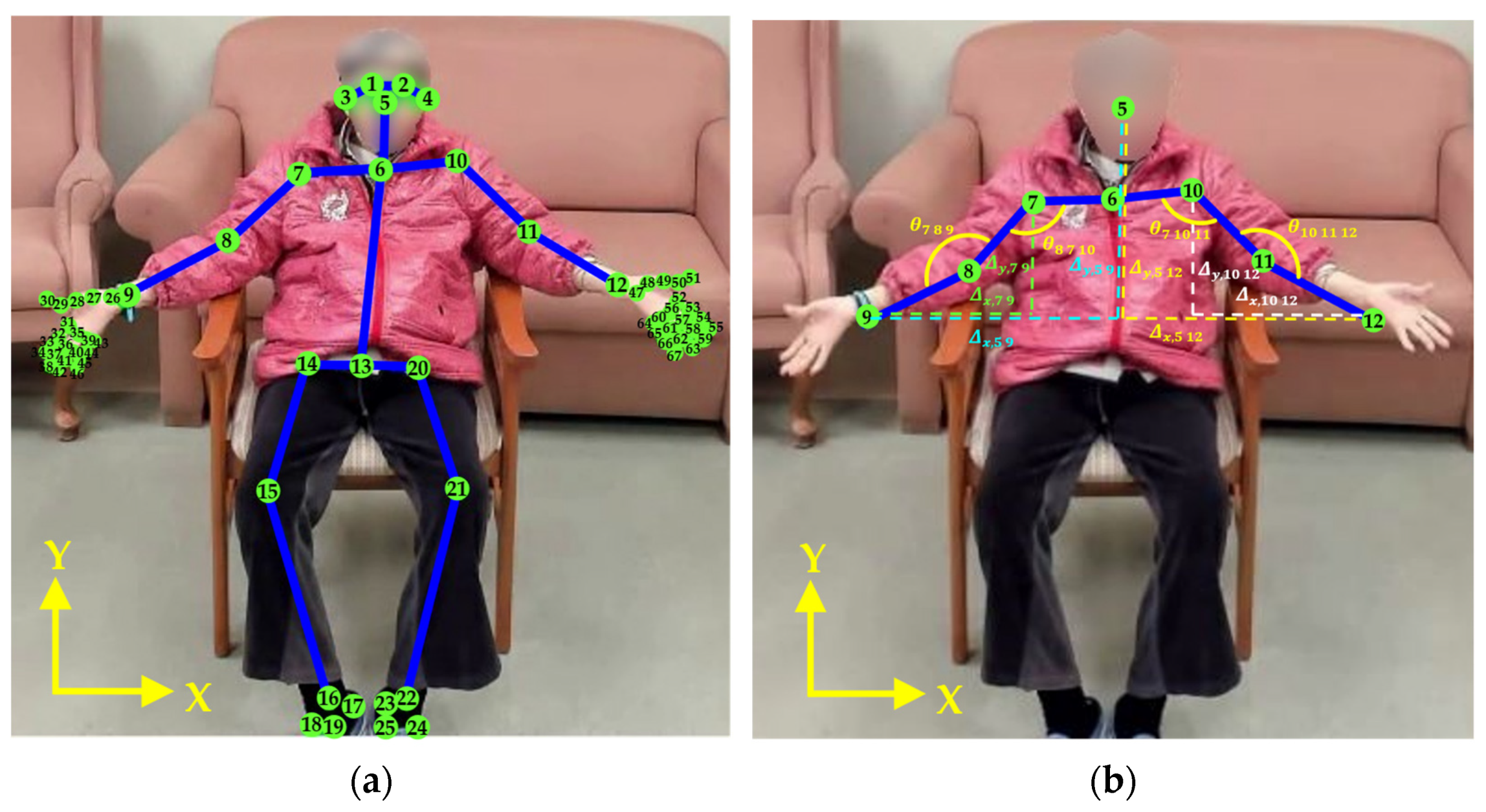
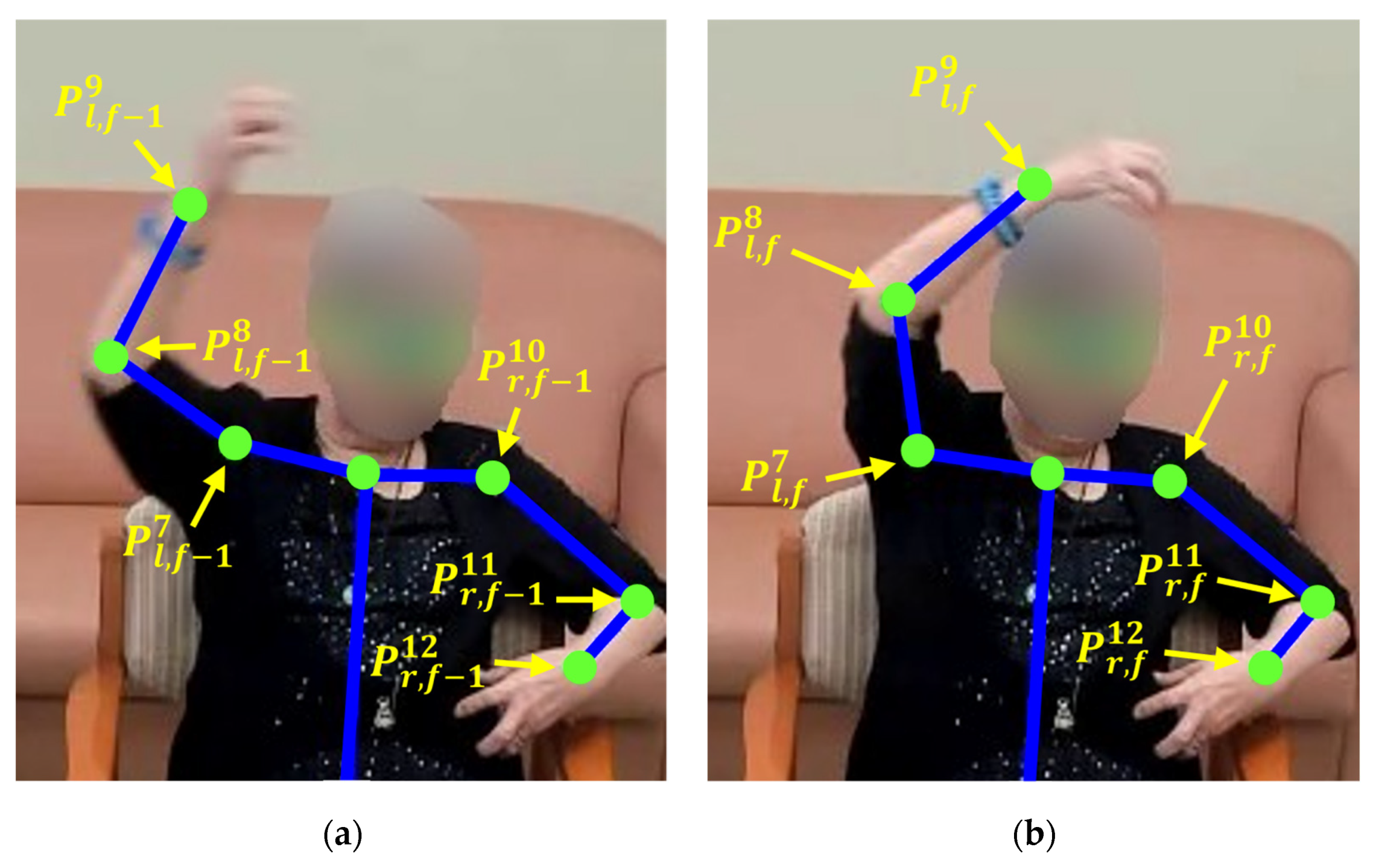
Appendix A.1.1. Keypoints and Features



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exercises | Complete Pose | Partially Complete Pose | Resting Pose |
|---|---|---|---|
| Open arm stretches | Open both arms from the center of the chest and raise them at least 65° from the sides of the body (i.e., and ≥ 155°) while opening both arms [117]. | Open both arms from the center of the chest but not raise at least one arm to or above 65° from the sides of the body (i.e., and/or < 155°) while opening both arms [117]. | |
| Neck exercises (up and down) | Move the neck in both up and down directions. | Move the neck in only up or down direction. | |
| Neck exercises (left and right) | Rotate the neck to the left or right to achieve a cervical rotation for at least 52° [118], which can be estimated when one of the ears is invisible from the front view of the person (i.e., confidence score or = 0) [116]. | Move the neck left or right but not to achieve a cervical rotation for at least 52° (i.e., confidence score and > 0) [118]. | |
| Arm raises | Raise both arms to at least 65° from the sides of the body (i.e., and ≥ 155°) [117]. | Raise at least one arm but not to at least 65° from the sides of the body (i.e., and/or < 155°) [117]. | Arms resting beside the waistline, on the armrest, or on the lap. |
| Downward punches | Raise both hands above the head (i.e., normalized and ≥ 0.025) before each downward punch [118]. | Raise at least one wrist but not above the head (i.e., normalized or < 0.025) [118]. | |
| Breaststrokes | Sweep both arms to the sides of the body (i.e., and > 0.05). | Sweep only one arm to the side of the body (i.e., or < 0.05). | |
| Open/close hands | Open and close both hands. | Open and close at least one hand. | |
| Forward punches | Extend each arm straight (i.e., or ≥ 155°) while punching [119]. | Punch forward but do not fully extend the arm straight (i.e., or < 155°) [119]. | |
| LTS | Raise each hand above the head (i.e., normalized and ≥ 0.025) while stretching [118]. | Raise each hand but not above the head (i.e., normalized or < 0.025) [118]. | |
| Two-arm LTS | Raise each hand above the head (i.e., normalized and ≥ 0.025) while the other arm is extending to the side of the body [118]. | Raise each hand but not above the head (i.e., normalized or < 0.025) [118]. |
| Exercise | Features |
|---|---|
| Open arm stretches | 1. Distances of the wrists-shoulders and elbows-shoulders for each arm in both x and y direction using Equation (A2). 2. Angles of elbows and shoulders for each arm using Equation (A3). |
| Neck exercises (up and down) | 1. Distances of the eyes-shoulders , nose-shoulders , and nose-neck in the y direction using Equation (A2). 2. Angles of the nose using Equation (A3). |
| Neck exercises (left and right) | ). |
| Arm raises | ) for each arm using Equation (A3). |
| Downward punches | ) for each arm in the y direction using Equation (A2). |
| Breaststroke | ) for each arm using Equation (A3) |
| Open/close hands | for the right hand) using Equation (A2) |
| Forward punches | ) for each arm using Equation (A3) |
| Lateral trunk stretch | ) for each arm using Equation (A3) |
| Two-arm lateral trunk stretch | ) for each arm in both x and y direction using Equation (A2) ) for each arm using Equation (A3) |
Appendix A.1.2. Pose Classification
| Classifier | ||||
|---|---|---|---|---|
| Exercise | K-Nearest Neighbor (k-NN) | Multilayer Perceptron Neural Network (NN) | Random Forest (RF) | Support Vector Machine (SVM) |
| Open arm stretches | 97.8% | 96.7% | 97.8% | 91.1% |
| Neck exercises (up and down) | 65.6% | 74.4% | 92.2% | 54.4% |
| Neck exercises (left and right) | 98% | 98.0% | 98.0% | 78% |
| Arm raises | 96.7% | 98.9% | 98.9% | 87.8% |
| Downward punches | 96.7% | 94.4% | 97.8% | 94.4% |
| Breast-stroke | 62.2% | 88.9% | 98.9% | 64.4% |
| Open/close hands | 88.3% | 50.0% | 97.5% | 94.9% |
| Forward punches | 71.4% | 80.0% | 92.7% | 54.3% |
| Lateral trunk stretch | 98.9% | 98.3% | 98.9% | 97.8% |
| Two-arm lateral trunk stretch | 97.8% | 96.7% | 98.4% | 95.6% |
| Average | 87.3% | 87.6% | 97.1% | 81.3% |
Appendix A.2. Exercise Evaluation Module
| Exercise | Agreed Completion (%) | Agreed Incompletion (%) | Disagreement (%) |
|---|---|---|---|
| Open arm stretches | 21.5 | 68.76 | 9.74 |
| Neck exercises (up and down) | 71.72 | 16.01 | 12.27 |
| Neck exercises (left and right) | 68.05 | 18.86 | 13.09 |
| Forward punches | 51.52 | 35.48 | 13 |
| Arm raises | 69.24 | 19.56 | 11.2 |
| Downward punches | 69.35 | 25.04 | 5.61 |
| Open/close hands | 77.33 | 12.35 | 10.32 |
| Breaststrokes | 95.89 | 1.03 | 3.08 |
| LTS | 77.85 | 13.41 | 8.74 |
| Two-arm LTS | 79.85 | 11.80 | 8.35 |
| Exercise | Classification Rate (%) |
|---|---|
| Open arm stretches | 86.86 |
| Neck exercises (up and down) | 85.12 |
| Neck exercises (left and right) | 87.17 |
| Forward punches | 88.34 |
| Arm raises | 89.07 |
| Downward punches | 92.98 |
| Breaststrokes | 96.87 |
| Open/close hands | 90.14 |
| LTS | 89.79 |
| Two-arm LTS | 88.01 |
| Average | 89.44 |
Appendix A.3. User State Detection Module
Appendix A.3.1. Valence

Appendix A.3.2. Engagement

Appendix A.4. Robot Emotion Module
Robot Emotion History Model
Appendix B. Robot Perception Questionnaire
| Construct | Question | One Month | Two Month | ||||||
|---|---|---|---|---|---|---|---|---|---|
| IQR | IQR | ||||||||
| C1: Acceptance | Q1. I like using the robot to do exercise | 4.04 | 1.07 | 4.00 | 2.00 | 4.11 | 1.13 | 5.00 | 2.00 |
| Q2. I would use the robot again | 3.78 | 1.40 | 4.00 | 2.00 | 3.96 | 1.40 | 5.00 | 1.00 | |
| Q3. The sensor headband is uncomfortable to wear * † | 1.40 | 0.92 | 1.00 | 1.00 | 1.60 | 0.80 | 1.00 | 0.00 | |
| C2: Perceived Usefulness and Ease of Use | Q4. The exercises the robot got me to do are good for my overall health | 4.30 | 0.97 | 5.00 | 1.00 | 4.26 | 1.11 | 5.00 | 1.00 |
| Q5. The robot is not helpful for doing exercise † | 1.70 | 1.15 | 1.00 | 2.00 | 2.04 | 1.35 | 1.00 | 1.25 | |
| Q6. The robot clearly displays each exercise | 4.44 | 1.10 | 5.00 | 1.00 | 4.37 | 0.82 | 4.00 | 0.25 | |
| Q7. The robot is difficult to use † | 2.04 | 1.37 | 1.00 | 2.00 | 2.52 | 1.29 | 3.00 | 2.00 | |
| Q8. I can use the robot without any help | 3.11 | 1.81 | 4.00 | 2.50 | 2.63 | 1.28 | 3.00 | 4.00 | |
| Q9. I don’t trust the robot’s advice † | 1.67 | 1.09 | 1.00 | 1.50 | 2.04 | 1.07 | 2.00 | 1.25 | |
| Q10. The robot motivates me to exercise | 4.33 | 1.09 | 5.00 | 2.00 | 3.85 | 1.24 | 4.00 | 1.00 | |
| C3: Perceived Sociability and Intelligence | Q11. After each exercise, the feedback the robot provided is appropriate | 3.82 | 1.09 | 4.00 | 2.00 | 3.70 | 1.24 | 4.00 | 2.00 |
| Q12. The robot understands what I am doing during exercising | 3.44 | 1.32 | 3.00 | 1.00 | 3.44 | 1.07 | 3.00 | 2.00 | |
| Q13. The robot displays appropriate emotions | 4.00 | 1.33 | 5.00 | 1.00 | 3.33 | 1.09 | 3.00 | 1.25 | |
| Q14. I am not able to identify the robot’s emotions through eye colors * † | 2.30 | 1.19 | 2.00 | 2.75 | 2.40 | 1.50 | 2.00 | 1.75 | |
| Q15. I am able to identify the robot’s emotions from vocal intonation * | 4.40 | 0.92 | 5.00 | 0.75 | 3.70 | 1.01 | 4.00 | 1.00 | |
| C4: Robot Appearance and Movements | Q16. The robot moves too fast for me to follow † | 1.82 | 1.36 | 1.00 | 2.00 | 2.00 | 1.31 | 1.00 | 2.00 |
| Q17. I think the robot has a clear voice | 4.33 | 1.16 | 5.00 | 1.50 | 4.19 | 1.25 | 5.00 | 1.00 | |
| Q18. I don’t understand the robot’s instructions † | 1.82 | 1.31 | 1.00 | 1.00 | 1.67 | 1.16 | 1.00 | 1.25 | |
| Q19. I think the robot’s size is appropriate for exercising | 4.22 | 1.23 | 5.00 | 2.00 | 3.74 | 1.29 | 4.00 | 1.25 | |
| Overall Experience (2 months) | Q20. I feel my physical health is improved from the exercise sessions with the robot | N/A | N/A | N/A | 2.00 | 3.70 | 1.24 | 4.00 | 2.00 |
| Q21. I find what I am doing in the weekly sessions confusing † | N/A | N/A | N/A | 1.00 | 1.67 | 1.12 | 1.00 | 1.00 | |
| Q22. As a result of these sessions, I am more motivated to perform daily physical exercises | N/A | N/A | N/A | 2.00 | 3.70 | 1.08 | 4.00 | 0.00 | |
| Q23. The robot always seemed interested in interacting with me | N/A | N/A | N/A | 1.50 | 3.56 | 1.13 | 3.00 | 1.00 | |
| Construct | Session Type | One Month | Two Months | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| C1: Acceptance (One-Month: = 0.75, Two-Months: = 0.88) | One-on-One | 1 | 5 | 4.0 | 4 | 1.00 | 2 | 5 | 4.5 | 5 | 2.00 |
| Group | 1 | 5 | 4.0 | 5 | 2.00 | 1 | 5 | 5.0 | 5 | 2.00 | |
| All | 1 | 5 | 4.0 | 5 | 1.75 | 1 | 5 | 5.0 | 5 | 2.00 | |
| C2: Perceived Usefulness and Ease of Use (One-Month: = 0.81, Two-Months: = 0.83) | One-on-One | 1 | 5 | 5.0 | 5 | 1.00 | 1 | 5 | 4.0 | 5 | 2.00 |
| Group | 1 | 5 | 5.0 | 5 | 2.00 | 1 | 5 | 4.0 | 5 | 2.00 | |
| All | 1 | 5 | 5.0 | 5 | 1.00 | 1 | 5 | 4.0 | 5 | 2.00 | |
| C3: Perceived Sociability and Intelligence (One-Month: = 0.79, Two-Months: = 0.68) | One-on-One | 1 | 5 | 4.5 | 5 | 1.25 | 2 | 5 | 4.0 | 5 | 2.00 |
| Group | 1 | 5 | 4.0 | 5 | 2.00 | 1 | 5 | 3.0 | 3 | 1.00 | |
| All | 1 | 5 | 4.0 | 5 | 2.00 | 1 | 5 | 3.0 | 3 | 2.00 | |
| C4: Robot Appearance and Movements (One-Month: = 0.80, Two-Months: = 0.72) | One-on-One | 1 | 5 | 5.0 | 5 | 1.25 | 1 | 5 | 5.0 | 5 | 1.00 |
| Group | 1 | 5 | 5.0 | 5 | 1.00 | 1 | 5 | 4.0 | 5 | 2.00 | |
| All | 1 | 5 | 5.0 | 5 | 1.00 | 1 | 5 | 5.0 | 5 | 2.00 | |
References
- Panton, L.; Loney, B. Exercise for Older Adults. Available online: https://file.lacounty.gov/SDSInter/dmh/216745_ExerciseforOlderAdultsHealthCareProviderManual.pdf (accessed on 27 September 2022).
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical Activity and Public Health in Older Adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sport. Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [Green Version]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.N.; Kohl, H.W.; Barlow, C.E.; Paffenbarger, R.S.; Gibbons, L.W.; Macera, C.A. Changes in Physical Fitness and All-Cause Mortality. A Prospective Study of Healthy and Unhealthy Men. JAMA 1995, 273, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Physical Activity, Self Reported, Adult, by Age Group (Table 13-10-0096-13). Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310009613 (accessed on 27 September 2022).
- Carros, F.; Meurer, J.; Löffler, D.; Unbehaun, D.; Matthies, S.; Koch, I.; Wieching, R.; Randall, D.; Hassenzahl, M.; Wulf, V. Exploring Human-Robot Interaction with the Elderly: Results from a Ten-Week Case Study in a Care Home. In Proceedings of the CHI Conference on Human Factors in Computing Systems, Honolulu, HI, USA, 25–30 April 2020; pp. 1–12. [Google Scholar]
- Fasola, J.; Matarić, M.J. A Socially Assistive Robot Exercise Coach for the Elderly. J. Hum.-Robot Interact. 2013, 2, 3–32. [Google Scholar] [CrossRef] [Green Version]
- Avelino, J.; Simão, H.; Ribeiro, R.; Moreno, P.; Figueiredo, R.; Duarte, N.; Nunes, R.; Bernardino, A.; Čaić, M.; Mahr, D. Experiments with Vizzy as a Coach for Elderly Exercise. In Workshop on Personal Robots for Exercising and Coaching-HRI Conference; PREC: Chicago, IL, USA, 2018; pp. 1–6. [Google Scholar]
- Görer, B.; Salah, A.A.; Akın, H.L. An Autonomous Robotic Exercise Tutor for Elderly People. Auton. Robot. 2017, 41, 657–678. [Google Scholar] [CrossRef]
- Costello, E.; Kafchinski, M.; Vrazel, J.; Sullivan, P. Motivators, Barriers, and Beliefs Regarding Physical Activity in an Older Adult Population. J. Geriatr. Phys. Ther. 2011, 34, 138–147. [Google Scholar] [CrossRef]
- Wada, K.; Shibata, T. Living with Seal Robots—Its Sociopsychological and Physiological Influences on the Elderly at a Care House. IEEE Trans. Robot. 2007, 23, 972–980. [Google Scholar] [CrossRef]
- Ybarra, O.; Burnstein, E.; Winkielman, P.; Keller, M.C.; Manis, M.; Chan, E.; Rodriguez, J. Mental Exercising through Simple Socializing: Social Interaction Promotes General Cognitive Functioning. Pers. Soc. Psychol. Bull. 2008, 34, 248–259. [Google Scholar] [CrossRef] [Green Version]
- van Stralen, M.M.; de Vries, H.; Mudde, A.N.; Bolman, C.; Lechner, L. The Long-Term Efficacy of Two Computer-Tailored Physical Activity Interventions for Older Adults: Main Effects and Mediators. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2011, 30, 442–452. [Google Scholar] [CrossRef]
- Marcus, B.H.; Bock, B.C.; Pinto, B.M.; Forsyth, L.H.; Roberts, M.B.; Traficante, R.M. Efficacy of an Individualized, Motivationally-Tailored Physical Activity Intervention. Ann. Behav. Med. Publ. Soc. Behav. Med. 1998, 20, 174–180. [Google Scholar] [CrossRef]
- Trampe, D.; Quoidbach, J.; Taquet, M. Emotions in Everyday Life. PLoS ONE 2015, 10, e0145450. [Google Scholar] [CrossRef] [Green Version]
- Cavallo, F.; Semeraro, F.; Fiorini, L.; Magyar, G.; Sinčák, P.; Dario, P. Emotion Modelling for Social Robotics Applications: A Review. J. Bionic Eng. 2018, 15, 185–203. [Google Scholar] [CrossRef]
- Uchida, M.C.; Carvalho, R.; Tessutti, V.D.; Bacurau, R.F.P.; Coelho-Júnior, H.J.; Capelo, L.P.; Ramos, H.P.; Dos Santos, M.C.; Teixeira, L.F.M.; Marchetti, P.H. Identification of Muscle Fatigue by Tracking Facial Expressions. PLoS ONE 2018, 13, e0208834. [Google Scholar] [CrossRef] [PubMed]
- Tanikawa, C.; Takata, S.; Takano, R.; Yamanami, H.; Edlira, Z.; Takada, K. Functional Decline in Facial Expression Generation in Older Women: A Cross-Sectional Study Using Three-Dimensional Morphometry. PloS ONE 2019, 14, e0219451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ketcham, C.J.; Stelmach, G.E. Movement Control in the Older Adult; Pew, R.W., Van Hemel, S.B., Eds.; National Academies Press (US) Steering Committee for the Workshop on Technology for Adaptive Aging: Washington, DC, USA, 2004. [Google Scholar]
- Al-Nafjan, A.; Hosny, M.; Al-Ohali, Y.; Al-Wabil, A. Review and Classification of Emotion Recognition Based on EEG Brain-Computer Interface System Research: A Systematic Review. Appl. Sci. 2017, 7, 1239. [Google Scholar] [CrossRef] [Green Version]
- Broelz, E.K.; Enck, P.; Niess, A.M.; Schneeweiss, P.; Wolf, S.; Weimer, K. The Neurobiology of Placebo Effects in Sports: EEG Frontal Alpha Asymmetry Increases in Response to a Placebo Ergogenic Aid. Sci. Rep. 2019, 9, 2381. [Google Scholar] [CrossRef] [Green Version]
- Céspedes, N.; Irfan, B.; Senft, E.; Cifuentes, C.A.; Gutierrez, L.F.; Rincon-Roncancio, M.; Belpaeme, T.; Múnera, M. A Socially Assistive Robot for Long-Term Cardiac Rehabilitation in the Real World. Front. Neurorobotics 2021, 15, 633248. [Google Scholar] [CrossRef]
- Pulido, J.C.; Suarez-Mejias, C.; Gonzalez, J.C.; Duenas Ruiz, A.; Ferrand Ferri, P.; Martinez Sahuquillo, M.E.; Ruiz De Vargas, C.E.; Infante-Cossio, P.; Parra Calderon, C.L.; Fernandez, F. A Socially Assistive Robotic Platform for Upper-Limb Rehabilitation: A Longitudinal Study with Pediatric Patients. IEEE Robot. Autom. Mag. 2019, 26, 24–39. [Google Scholar] [CrossRef]
- Back, I.; Makela, K.; Kallio, J. Robot-Guided Exercise Program for the Rehabilitation of Older Nursing Home Residents. Ann. Long-Term Care 2013, 21, 38–41. [Google Scholar]
- Fraune, M.R.; Šabanović, S.; Kanda, T. Human Group Presence, Group Characteristics, and Group Norms Affect Human-Robot Interaction in Naturalistic Settings. Front. Robot. AI 2019, 6, 48. [Google Scholar] [CrossRef] [Green Version]
- Fraune, M.R.; Sherrin, S.; Šabanović, S.; Smith, E.R. Is Human-Robot Interaction More Competitive between Groups than between Individuals? In Proceedings of the ACM/IEEE International Conference on Human-Robot Interaction, Daegu, Republic of Korea, 11–14 March 2019; pp. 104–113. [Google Scholar]
- Leite, I.; Mccoy, M.; Lohani, M.; Ullman, D.; Salomons, N.; Stokes, C.; Rivers, S.; Scassellati, B. Emotional Storytelling in the Classroom: Individual versus Group Interaction between Children and Robots. In Proceedings of the ACM/IEEE International Conference on Human-Robot Interaction, Portland, OR, USA, 2–5 March 2015. [Google Scholar]
- Harvard Health Publishing. The 4 Most Important Types of Exercise. Available online: https://www.health.harvard.edu/exercise-and-fitness/the-4-most-important-types-of-exercise (accessed on 27 September 2022).
- United States Department of Health and Human Services. Physical Activity and Health: A Report of the Surgeon General; Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion: Atlanta, GA, USA, 1996.
- Kiresuk, T.J.; Sherman, R.E. Goal Attainment Scaling: A General Method for Evaluating Comprehensive Community Mental Health Programs. Community Ment. Health J. 1968, 4, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Hidalgo, G.; Simon, T.; Wei, S.-E.; Sheikh, Y. OpenPose: Realtime Multi-Person 2D Pose Estimation Using Part Affinity Fields. IEEE Trans. Pattern Anal. Mach. Intell. 2021, 43, 172–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, T.; Joo, H.; Matthews, I.; Sheikh, Y. Hand Keypoint Detection in Single Images Using Multiview Bootstrapping. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4645–4653. [Google Scholar]
- Krasny-Pacini, A.; Hiebel, J.; Pauly, F.; Godon, S.; Chevignard, M. Goal Attainment Scaling in Rehabilitation: A Literature-Based Update. Ann. Phys. Rehabil. Med. 2013, 56, 212–230. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.C.; Walley, R.M.; Leech, A.; Paterson, M.; Common, S.; Metcalf, C. Using Goal Attainment Scaling to Evaluate a Needs-Led Exercise Programme for People with Severe and Profound Intellectual Disabilities. J. Intellect. Disabil. 2006, 10, 317–335. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Stolee, P.; Fox, R.A. Use of Goal Attainment Scaling in Measuring Clinically Important Change in the Frail Elderly. J. Clin. Epidemiol. 1993, 46, 1113–1118. [Google Scholar] [CrossRef]
- Stolee, P.; Rockwood, K.; Fox, R.A.; Streiner, D.L. The Use of Goal Attainment Scaling in a Geriatric Care Setting. J. Am. Geriatr. Soc. 1992, 40, 574–578. [Google Scholar] [CrossRef]
- Toto, P.E.; Skidmore, E.R.; Terhorst, L.; Rosen, J.; Weiner, D.K. Goal Attainment Scaling (GAS) in Geriatric Primary Care: A Feasibility Study. Arch. Gerontol. Geriatr. 2015, 60, 16–21. [Google Scholar] [CrossRef]
- Valadão, C.T.; Goulart, C.; Rivera, H.; Caldeira, E.; Bastos Filho, T.F.; Frizera-Neto, A.; Carelli, R. Analysis of the Use of a Robot to Improve Social Skills in Children with Autism Spectrum Disorder. Res. Biomed. Eng. 2016, 32, 161–175. [Google Scholar] [CrossRef] [Green Version]
- Cook, A.M.; Bentz, B.; Harbottle, N.; Lynch, C.; Miller, B. School-Based Use of a Robotic Arm System by Children with Disabilities. IEEE Trans. Neural Syst. Rehabil. Eng. 2005, 13, 452–460. [Google Scholar] [CrossRef]
- National Institute on Aging. Exercise: A Guide from the National Institude on Aging; National Institute on Aging: Bethesda, MD, USA, 2001. [Google Scholar]
- Su, S.W.; Huang, S.; Wang, L.; Celler, B.G.; Savkin, A.V.; Guo, Y.; Cheng, T.M. Optimizing Heart Rate Regulation for Safe Exercise. Ann. Biomed. Eng. 2010, 38, 758–768. [Google Scholar] [CrossRef]
- Barrett, L.F. Valence Is a Basic Building Block of Emotional Life. J. Res. Pers. 2006, 40, 35–55. [Google Scholar] [CrossRef]
- Shao, M.; Snyder, M.; Nejat, G.; Benhabib, B. User Affect Elicitation with a Socially Emotional Robot. Robotics 2020, 9, 44. [Google Scholar] [CrossRef]
- Spezialetti, M.; Placidi, G.; Rossi, S. Emotion Recognition for Human-Robot Interaction: Recent Advances and Future Perspectives. Front. Robot. AI 2020, 7, 532279. [Google Scholar] [CrossRef]
- Apicella, A.; Arpaia, P.; Mastrati, G.; Moccaldi, N. EEG-Based Detection of Emotional Valence towards a Reproducible Measurement of Emotions. Sci. Rep. 2021, 11, 21615. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, R.; Vamvakousis, Z. Detecting Emotion from EEG Signals Using the Emotive Epoc Device. In International Conference on Brain Informatics; Zanzotto, F.M., Tsumoto, S., Taatgen, N., Yao, Y., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 175–184. [Google Scholar]
- Chen, M.; Han, J.; Guo, L.; Wang, J.; Patras, I. Identifying Valence and Arousal Levels via Connectivity between EEG Channels. In Proceedings of the International Conference on Affective Computing and Intelligent Interaction, Xi’an, China, 21–24 September 2015; pp. 63–69. [Google Scholar]
- Sidner, C.L.; Lee, C.; Kidd, C.D.; Lesh, N.; Rich, C. Explorations in Engagement for Humans and Robots. Artif. Intell. 2005, 166, 140–164. [Google Scholar] [CrossRef] [Green Version]
- Sidner, C.L.; Kidd, C.D.; Lee, C.; Lesh, N. Where to Look: A Study of Human-Robot Engagement. In Proceedings of the 9th International Conference on Intelligent User Interfaces; Association for Computing Machinery: New York, NY, USA, 2004; pp. 78–84. [Google Scholar]
- Michalowski, M.P.; Sabanovic, S.; Simmons, R. A Spatial Model of Engagement for a Social Robot. In Proceedings of the IEEE International Workshop on Advanced Motion Control, Istanbul, Turkey, 27–29 March 2006; pp. 762–767. [Google Scholar]
- Moro, C.; Lin, S.; Nejat, G.; Mihailidis, A. Social Robots and Seniors: A Comparative Study on the Influence of Dynamic Social Features on Human–Robot Interaction. Int. J. Soc. Robot. 2019, 11, 5–24. [Google Scholar] [CrossRef]
- Li, J.; Louie, W.-Y.G.; Mohamed, S.; Despond, F.; Nejat, G. A User-Study with Tangy the Bingo Facilitating Robot and Long-Term Care Residents. In Proceedings of the IEEE International Symposium on Robotics and Intelligent Sensors, Tokyo, Japan, 17–20 December 2016; pp. 109–115. [Google Scholar]
- American Heart Association. Target Heart Rates Chart. Available online: https://www.heart.org/en/healthy-living/fitness/fitness-basics/target-heart-rates (accessed on 27 September 2022).
- Shao, M.; Alves, S.F.D.R.; Ismail, O.; Zhang, X.; Nejat, G.; Benhabib, B. You Are Doing Great! Only One Rep Left: An Affect-Aware Social Robot for Exercising. In Proceedings of the IEEE International Conference on Systems, Man and Cybernetics, Bari, Italy, 6–9 October 2019; pp. 3811–3817. [Google Scholar]
- Zhang, X.; Alves, S.; Nejat, G.; Benhabib, B. A Robot Emotion Model with History. In Proceedings of the IEEE International Symposium on Robotics and Intelligent Sensors, Ottawa, ON, Canada, 5–7 October 2017; pp. 230–235. [Google Scholar]
- Stødle, I.V.; Debesay, J.; Pajalic, Z.; Lid, I.M.; Bergland, A. The Experience of Motivation and Adherence to Group-Based Exercise of Norwegians Aged 80 and More: A Qualitative Study. Arch. Public Health 2019, 77, 26. [Google Scholar] [CrossRef] [Green Version]
- Yang, E.; Dorneich, M.C. The Effect of Time Delay on Emotion, Arousal, and Satisfaction in Human-Robot Interaction. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2015, 59, 443–447. [Google Scholar] [CrossRef] [Green Version]
- Rudovic, O.; Lee, J.; Mascarell-Maricic, L.; Schuller, B.W.; Picard, R.W. Measuring Engagement in Robot-Assisted Autism Therapy: A Cross-Cultural Study. Front. Robot. AI 2017, 4, 36. [Google Scholar] [CrossRef] [Green Version]
- Fasola, J.; Mataric, M.J. Using Socially Assistive Human–Robot Interaction to Motivate Physical Exercise for Older Adults. Proc. IEEE 2012, 100, 2512–2526. [Google Scholar] [CrossRef]
- Yee Hong Centre for Geriatric Care. MDS CIHI Data Jan 2020 for Yee Hong Centre Mississauga; Yee Hong Centre for Geriatric Care: Mississauga, ON, Canada, 2020. [Google Scholar]
- National Cancer Institute Division of Cancer Control and Population Sciences. SEER-Medicare: Minimum Data Set (MDS)—Nursing Home Assessment; National Cancer Institute: Bethesda, MD, USA, 2010. [Google Scholar]
- Morris, J.N.; Fries, B.E.; Mehr, D.R.; Hawes, C.; Phillips, C.; Mor, V.; Lipsitz, L.A. MDS Cognitive Performance Scale. J. Gerontol. 1994, 49, M174–M182. [Google Scholar] [CrossRef]
- Kurlowicz, L.; Wallace, M. The Mini-Mental State Examination (MMSE). J. Gerontol. Nurs. 1999, 25, 8–9. [Google Scholar] [CrossRef]
- Müller, B.C.N.; Chen, S.; Nijssen, S.R.R.; Kühn, S. How (Not) to Increase Older Adults’ Tendency to Anthropomorphise in Serious Games. PLoS ONE 2018, 13, e0199948. [Google Scholar] [CrossRef]
- Werner, C.; Kardaris, N.; Koutras, P.; Zlatintsi, A.; Maragos, P.; Bauer, J.M.; Hauer, K. Improving Gesture-Based Interaction between an Assistive Bathing Robot and Older Adults via User Training on the Gestural Commands. Arch. Gerontol. Geriatr. 2020, 87, 103996. [Google Scholar] [CrossRef]
- Gruneir, A.; Forrester, J.; Camacho, X.; Gill, S.S.; Bronskill, S.E. Gender Differences in Home Care Clients and Admission to Long-Term Care in Ontario, Canada: A Population-Based Retrospective Cohort Study. BMC Geriatr. 2013, 13, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Association for Long-Term Care Insurance Long Term Care—Important Information for Women. Available online: https://www.aaltci.org/long-term-care-insurance/learning-center/for-women.php (accessed on 4 December 2022).
- Burke, S.; Carron, A.; Eys, M.; Ntoumanis, N.; Estabrooks, P. Group versus Individual Approach? A Meta-Analysis of the Effectiveness of Interventions to Promote Physical Activity. Sport Exerc. Psychol. Rev. 2006, 2, 19–35. [Google Scholar]
- Cadore, E.L.; Rodríguez-Mañas, L.; Sinclair, A.; Izquierdo, M. Effects of Different Exercise Interventions on Risk of Falls, Gait Ability, and Balance in Physically Frail Older Adults: A Systematic Review. Rejuvenation Res. 2013, 16, 105–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glaros, N.M.; Janelle, C.M. Varying the Mode of Cardiovascular Exercise to Increase Adherence. J. Sport Behav. 2001, 24, 42–62. [Google Scholar]
- Bradley, M.M.; Lang, P.J. Measuring Emotion: The Self-Assessment Manikin and the Semantic Differential. J. Behav. Ther. Exp. Psychiatry 1994, 25, 49–59. [Google Scholar] [CrossRef]
- Heerink, M.; Kröse, B.; Evers, V.; Wielinga, B. Assessing Acceptance of Assistive Social Agent Technology by Older Adults: The Almere Model. Int. J. Soc. Robot. 2010, 2, 361–375. [Google Scholar] [CrossRef] [Green Version]
- Cronbach, L.J. Coefficient Alpha and the Internal Structure of Tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef] [Green Version]
- Kehoe, J. Basic Item Analysis for Multiple-Choice Tests. Pract. Assess. Res. Eval. 2019, 4, 10. [Google Scholar] [CrossRef]
- Pallant, J. SPSS Survival Manual: A Step by Step Guide to Data Analysis Using IBM SPSS, 4th ed.; Open University Press/McGraw-Hill: Maidenhead, Australia, 2011; ISBN 978-1-952533-63-1. [Google Scholar]
- Prakash, A.; Rogers, W.A. Why Some Humanoid Faces Are Perceived More Positively than Others: Effects of Human-Likeness and Task. Int. J. Soc. Robot. 2015, 7, 309–331. [Google Scholar] [CrossRef] [PubMed]
- Bedaf, S.; Marti, P.; De Witte, L. What Are the Preferred Characteristics of a Service Robot for the Elderly? A Multi-Country Focus Group Study with Older Adults and Caregivers. Assist. Technol. 2019, 31, 147–157. [Google Scholar] [CrossRef] [Green Version]
- Tu, Y.-C.; Chien, S.-E.; Yeh, S.-L. Age-Related Differences in the Uncanny Valley Effect. Gerontology 2020, 66, 382–392. [Google Scholar] [CrossRef]
- Ekkekakis, P.; Hall, E.E.; Petruzzello, S.J. The Relationship between Exercise Intensity and Affective Responses Demystified: To Crack the 40-Year-Old Nut, Replace the 40-Year-Old Nutcracker! Ann. Behav. Med. Publ. Soc. Behav. Med. 2008, 35, 136–149. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.E.; Eston, R.; Tempest, G.D.; Norton, B.; Parfitt, G. Patterning of Physiological and Affective Responses in Older Active Adults during a Maximal Graded Exercise Test and Self-Selected Exercise. Eur. J. Appl. Physiol. 2015, 115, 1855–1866. [Google Scholar] [CrossRef]
- Bixby, W.R.; Spalding, T.W.; Hatfield, B.D. Temporal Dynamics and Dimensional Specificity of the Affective Response to Exercise of Varying Intensity: Differing Pathways to a Common Outcome. J. Sport Exerc. Psychol. 2001, 23, 171–190. [Google Scholar] [CrossRef]
- Woo, M.; Kim, S.; Kim, J.; Petruzzello, S.J.; Hatfield, B.D. The Influence of Exercise Intensity on Frontal Electroencephalographic Asymmetry and Self-Reported Affect. Res. Q. Exerc. Sport 2010, 81, 349–359. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Kates, A. Can the Affective Response to Exercise Predict Future Motives and Physical Activity Behavior? A Systematic Review of Published Evidence. Ann. Behav. Med. 2015, 49, 715–731. [Google Scholar] [CrossRef]
- McAuley, E.; Jerome, G.J.; Elavsky, S.; Marquez, D.X.; Ramsey, S.N. Predicting Long-Term Maintenance of Physical Activity in Older Adults. Prev. Med. 2003, 37, 110–118. [Google Scholar] [CrossRef]
- Oppenauer, C.; Preschl, B.; Kalteis, K.; Kryspin-Exner, I. Technology in Old Age from a Psychological Point of View. In HCI and Usability for Medicine and Health Care; Holzinger, A., Ed.; Lecture Notes in Computer Science; Springer: Berlin/Heidelberg, Germany, 2007; Volume 4799, pp. 133–142. ISBN 978-3-540-76805-0. [Google Scholar]
- Tacken, M.; Marcellini, F.; Mollenkopf, H.; Ruoppila, I.; Széman, Z. Use and Acceptance of New Technology by Older People. Findings of the International MOBILATE Survey: “Enhancing Mobility in Later Life”. Gerontechnology 2005, 3, 126–137. [Google Scholar] [CrossRef]
- Chen, T.L.; Bhattacharjee, T.; Beer, J.M.; Ting, L.H.; Hackney, M.E.; Rogers, W.A.; Kemp, C.C. Older Adults’ Acceptance of a Robot for Partner Dance-Based Exercise. PLoS ONE 2017, 12, e0182736. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-H.; Wrobel, J.; Cornuet, M.; Kerhervé, H.; Damnée, S.; Rigaud, A.-S. Acceptance of an Assistive Robot in Older Adults: A Mixed-Method Study of Human-Robot Interaction over a 1-Month Period in the Living Lab Setting. Clin. Interv. Aging 2014, 9, 801–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hebesberger, D.; Koertner, T.; Gisinger, C.; Pripfl, J. A Long-Term Autonomous Robot at a Care Hospital: A Mixed Methods Study on Social Acceptance and Experiences of Staff and Older Adults. Int. J. Soc. Robot. 2017, 9, 417–429. [Google Scholar] [CrossRef]
- Cavallo, F.; Esposito, R.; Limosani, R.; Manzi, A.; Bevilacqua, R.; Felici, E.; Di Nuovo, A.; Cangelosi, A.; Lattanzio, F.; Dario, P. Robotic Services Acceptance in Smart Environments with Older Adults: User Satisfaction and Acceptability Study. J. Med. Internet Res. 2018, 20, e264. [Google Scholar] [CrossRef] [PubMed]
- Broadbent, E.; Tamagawa, R.; Kerse, N.; Knock, B.; Patience, A.; MacDonald, B. Retirement Home Staff and Residents’ Preferences for Healthcare Robots. In Proceedings of the 18th IEEE International Symposium on Robot and Human Interactive Communication, Toyama, Japan, 27 September–2 October 2009; pp. 645–650. [Google Scholar]
- Chu, L.; Chen, H.-W.; Cheng, P.-Y.; Ho, P.; Weng, I.-T.; Yang, P.-L.; Chien, S.-E.; Tu, Y.-C.; Yang, C.-C.; Wang, T.-M.; et al. Identifying Features That Enhance Older Adults’ Acceptance of Robots: A Mixed Methods Study. Gerontology 2019, 65, 441–450. [Google Scholar] [CrossRef]
- Deshmukh, A.; Lohan, K.S.; Rajendran, G.; Aylett, R. Social Impact of Recharging Activity in Long-Term HRI and Verbal Strategies to Manage User Expectations during Recharge. Front. Robot. AI 2018, 5, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanda, T.; Sato, R.; Saiwaki, N.; Ishiguro, H. A Two-Month Field Trial in an Elementary School for Long-Term Human–Robot Interaction. IEEE Trans. Robot. 2007, 23, 962–971. [Google Scholar] [CrossRef]
- Sung, J.; Christensen, H.I.; Grinter, R.E. Robots in the Wild: Understanding Long-Term Use. In Proceedings of the 4th ACM/IEEE International Conference on Human-Robot Interaction, La Jolla, CA, USA, 11–13 March 2009; pp. 45–52. [Google Scholar]
- Spink, K.S.; Carron, A.V. Group Cohesion Effects in Exercise Classes. Small Group Res. 1994, 25, 26–42. [Google Scholar] [CrossRef]
- Burke, S.M.; Carron, A.V.; Shapcott, K.M. Cohesion in Exercise Groups: An Overview. Int. Rev. Sport Exerc. Psychol. 2008, 1, 107–123. [Google Scholar] [CrossRef]
- Marcantonio, E.R.; Aneja, J.; Jones, R.N.; Alsop, D.C.; Fong, T.G.; Crosby, G.J.; Culley, D.J.; Cupples, L.A.; Inouye, S.K. Maximizing Clinical Research Participation in Vulnerable Older Persons: Identification of Barriers and Motivators. J. Am. Geriatr. Soc. 2008, 56, 1522–1527. [Google Scholar] [CrossRef] [Green Version]
- Soule, M.C.; Beale, E.E.; Suarez, L.; Beach, S.R.; Mastromauro, C.A.; Celano, C.M.; Moore, S.V.; Huffman, J.C. Understanding Motivations to Participate in an Observational Research Study: Why Do Patients Enroll? Soc. Work Health Care 2016, 55, 231–246. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, M.R.; Carron, A.V.; McCutcheon, S.; Harper, O. Older Adults’ Preferences for Exercising Alone versus in Groups: Considering Contextual Congruence. Ann. Behav. Med. 2007, 33, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Mansfield, J.; Marx, M.S.; Biddison, J.R.; Guralnik, J.M. Socio-Environmental Exercise Preferences among Older Adults. Prev. Med. 2004, 38, 804–811. [Google Scholar] [CrossRef]
- Fan, J.; Beuscher, L.; Newhouse, P.A.; Mion, L.C.; Sarkar, N. A Robotic Coach Architecture for Multi-User Human-Robot Interaction (RAMU) with the Elderly and Cognitively Impaired. In Proceedings of the 25th IEEE International Symposium on Robot and Human Interactive Communication, New York, NY, USA, 26–31 August 2016; pp. 445–450. [Google Scholar]
- Correia, F.; Mascarenhas, S.; Prada, R.; Melo, F.S.; Paiva, A. Group-Based Emotions in Teams of Humans and Robots. In Proceedings of the 13th ACM/IEEE International Conference on Human-Robot Interaction, Chicago, IL, USA, 5–8 March 2018; pp. 261–269. [Google Scholar]
- Kessler, T.; Hollbach, S. Group-Based Emotions as Determinants of Ingroup Identification. J. Exp. Soc. Psychol. 2005, 41, 677–685. [Google Scholar] [CrossRef]
- Affanni, A.; Aminosharieh Najafi, T.; Guerci, S. Development of an EEG Headband for Stress Measurement on Driving Simulators. Sensors 2022, 22, 1785. [Google Scholar] [CrossRef]
- Filippini, C.; Perpetuini, D.; Cardone, D.; Chiarelli, A.M.; Merla, A. Thermal Infrared Imaging-Based Affective Computing and Its Application to Facilitate Human Robot Interaction: A Review. Appl. Sci. 2020, 10, 2924. [Google Scholar] [CrossRef] [Green Version]
- Abd Latif, M.H.; Yusof, H.; Sidek, S.N.; Rusli, N. Thermal Imaging Based Affective State Recognition. In Proceedings of the IEEE International Symposium on Robotics and Intelligent Sensors, Langkawi, Malaysia, 18–20 October 2015; pp. 214–219. [Google Scholar]
- Manullang, M.C.T.; Lin, Y.-H.; Lai, S.-J.; Chou, N.-K. Implementation of Thermal Camera for Non-Contact Physiological Measurement: A Systematic Review. Sensors 2021, 21, 7777. [Google Scholar] [CrossRef]
- Silva, C.M.d.S.E.; Gomes Neto, M.; Saquetto, M.B.; da Conceição, C.S.; Souza-Machado, A. Effects of Upper Limb Resistance Exercise on Aerobic Capacity, Muscle Strength, and Quality of Life in COPD Patients: A Randomized Controlled Trial. Clin. Rehabil. 2018, 32, 1636–1644. [Google Scholar] [CrossRef]
- Whitall, J.; Waller, S.M.; Silver, K.H.C.; Macko, R.F. Repetitive Bilateral Arm Training with Rhythmic Auditory Cueing Improves Motor Function in Chronic Hemiparetic Stroke. Stroke 2000, 31, 2390–2395. [Google Scholar] [CrossRef] [Green Version]
- Vigorito, C.; Giallauria, F. Effects of Exercise on Cardiovascular Performance in the Elderly. Front. Physiol. 2014, 5, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, S.; Kummert, F. Comparing Robot and Human Guided Personalization: Adaptive Exercise Robots Are Perceived as More Competent and Trustworthy. Int. J. Soc. Robot. 2021, 13, 169–185. [Google Scholar] [CrossRef]
- Hong, A.; Lunscher, N.; Hu, T.; Tsuboi, Y.; Zhang, X.; Franco dos Reis Alves, S.; Nejat, G.; Benhabib, B. A Multimodal Emotional Human–Robot Interaction Architecture for Social Robots Engaged in Bidirectional Communication. IEEE Trans. Cybern. 2021, 51, 5954–5968. [Google Scholar] [CrossRef] [PubMed]
- Ficocelli, M.; Terao, J.; Nejat, G. Promoting Interactions between Humans and Robots Using Robotic Emotional Behavior. IEEE Trans. Cybern. 2016, 46, 2911–2923. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, Y.; Shah, Y.; Sharma, A. Implementation of Machine Learning Technique for Identification of Yoga Poses. In Proceedings of the IEEE 9th International Conference on Communication Systems and Network Technologies, Gwalior, India, 10–12 April 2020; pp. 40–43. [Google Scholar]
- Dias, P.A.; Malafronte, D.; Medeiros, H.; Odone, F. Gaze Estimation for Assisted Living Environments. In Proceedings of the IEEE Winter Conference on Applications of Computer Vision, Snowmass, CO, USA, 1–5 March 2020; pp. 279–288. [Google Scholar]
- Lazowski, D.A.; Ecclestone, N.A.; Myers, A.M.; Paterson, D.H.; Tudor-Locke, C.; Fitzgerald, C.; Jones, G.; Shima, N.; Cunningham, D.A. A Randomized Outcome Evaluation of Group Exercise Programs in Long-Term Care Institutions. J. Gerontol. A Biol. Sci. Med. Sci. 1999, 54, M621–M628. [Google Scholar] [CrossRef] [Green Version]
- Swank, A.M.; Funk, D.C.; Durham, M.P.; Roberts, S. Adding Weights to Stretching Exercise Increases Passive Range of Motion for Healthy Elderly. J. Strength Cond. Res. 2003, 17, 374–378. [Google Scholar] [CrossRef]
- Fiebert, I.; Fuhri, J.R.; New, M.D. Elbow, Forearm, and Wrist Passive Range of Motion in Persons Aged Sixty and Older. Phys. Occup. Ther. Geriatr. 1993, 10, 17–32. [Google Scholar] [CrossRef]
- Alves, S.F.; Shao, M.; Nejat, G. A Socially Assistive Robot to Facilitate and Assess Exercise Goals. In Proceedings of the IEEE International Conference of Robotics and Automation Workshop on Mobile Robot Assistants for the Elderly, Montreal, QC, Canada, 20–24 May 2019; pp. 1–5. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-Learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Trace, J.; Janssen, G.; Meier, V. Measuring the Impact of Rater Negotiation in Writing Performance Assessment. Lang. Test. 2017, 34, 3–22. [Google Scholar] [CrossRef]
- InteraXon Inc. Technical Specifications, Validation, and Research Use; InteraXon Inc.: Toronto, ON, Canada, 2016. [Google Scholar]
- Barachant, A.; Morrison, D.; Banville, H.; Kowaleski, J.; Shaked, U.; Chevallier, S.; Tresols, J.J.T. Muse-lsl. Available online: https://github.com/alexandrebarachant/muse-lsl (accessed on 31 May 2020).
- Al-Nafjan, A.; Hosny, M.; Al-Wabil, A.; Al-Ohali, Y. Classification of Human Emotions from Electroencephalogram (EEG) Signal Using Deep Neural Network. Int. J. Adv. Comput. Sci. Appl. 2017, 8, 419–425. [Google Scholar] [CrossRef] [Green Version]
- Zhao, G.; Zhang, Y.; Ge, Y. Frontal EEG Asymmetry and Middle Line Power Difference in Discrete Emotions. Front. Behav. Neurosci. 2018, 12, 225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castellano, G.; Leite, I.; Pereira, A.; Martinho, C.; Paiva, A.; McOwan, P.W. Affect Recognition for Interactive Companions: Challenges and Design in Real World Scenarios. J. Multimodal User Interfaces 2010, 3, 89–98. [Google Scholar] [CrossRef]
- Riether, N.; Hegel, F.; Wrede, B.; Horstmann, G. Social Facilitation with Social Robots? In Proceedings of the 7th ACM/IEEE International Conference on Human-Robot Interaction, Boston, MA, USA, 5–8 March 2012; pp. 41–47. [Google Scholar]
- Sanghvi, J.; Castellano, G.; Leite, I.; Pereira, A.; McOwan, P.W.; Paiva, A. Automatic Analysis of Affective Postures and Body Motion to Detect Engagement with a Game Companion. In Proceedings of the 6th International Conference on Human-Robot Interaction, Lausanne, Switzerland, 6–9 March 2011; pp. 305–312. [Google Scholar]
- Glenberg, A.M.; Schroeder, J.L.; Robertson, D.A. Averting the Gaze Disengages the Environment and Facilitates Remembering. Mem. Cogn. 1998, 26, 651–658. [Google Scholar] [CrossRef]
- Al Zoubi, O.; Ki Wong, C.; Kuplicki, R.T.; Yeh, H.-W.; Mayeli, A.; Refai, H.; Paulus, M.; Bodurka, J. Predicting Age from Brain EEG Signals-A Machine Learning Approach. Front. Aging Neurosci. 2018, 10, 184. [Google Scholar] [CrossRef] [Green Version]
- Zappasodi, F.; Marzetti, L.; Olejarczyk, E.; Tecchio, F.; Pizzella, V. Age-Related Changes in Electroencephalographic Signal Complexity. PLoS ONE 2015, 10, e0141995. [Google Scholar] [CrossRef] [Green Version]
- Koelstra, S.; Muhl, C.; Soleymani, M.; Lee, J.-S.; Yazdani, A.; Ebrahimi, T.; Pun, T.; Nijholt, A.; Patras, I. DEAP: A Database for Emotion Analysis Using Physiological Signals. IEEE Trans. Affect. Comput. 2012, 3, 18–31. [Google Scholar] [CrossRef] [Green Version]
- Abadi, M.K.; Subramanian, R.; Kia, S.M.; Avesani, P.; Patras, I.; Sebe, N. DECAF: MEG-Based Multimodal Database for Decoding Affective Physiological Responses. IEEE Trans. Affect. Comput. 2015, 6, 209–222. [Google Scholar] [CrossRef]
- Katsigiannis, S.; Ramzan, N. DREAMER: A Database for Emotion Recognition through EEG and ECG Signals from Wireless Low-Cost off-the-Shelf Devices. IEEE J. Biomed. Health Inform. 2018, 22, 98–107. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.-P.; Yang, Y.-H.; Jung, T.-P. Fusion of Electroencephalographic Dynamics and Musical Contents for Estimating Emotional Responses in Music Listening. Front. Neurosci. 2014, 8, 94. [Google Scholar] [CrossRef] [Green Version]
- Pandey, P.; Seeja, K.R. Subject Independent Emotion Recognition from EEG Using VMD and Deep Learning. J. King Saud Univ.-Comput. Inf. Sci. 2022, 34, 1730–1738. [Google Scholar] [CrossRef]
- McColl, D.; Louie, W.-Y.G.; Nejat, G. Brian 2.1: A Socially Assistive Robot for the Elderly and Cognitively Impaired. IEEE Robot. Autom. Mag. 2013, 20, 74–83. [Google Scholar] [CrossRef]
- Verduyn, P.; Delaveau, P.; Rotgé, J.-Y.; Fossati, P.; Van Mechelen, I. Determinants of Emotion Duration and Underlying Psychological and Neural Mechanisms. Emot. Rev. 2015, 7, 330–335. [Google Scholar] [CrossRef]













| Score | Predicted Attainment |
|---|---|
| −2 | Perform less than 8 (12) repetitions |
| −1 | Perform at least 8 (12) repetitions with partially complete poses only |
| 0 | Perform at least 8 (12) repetitions and achieve complete poses for less than 4 (6) repetitions |
| +1 | Perform at least 8 (12) repetitions and achieve complete poses for at least 4 (6) repetitions |
| +2 | Perform at least 8 (12) repetitions and achieve complete poses for at least 8 (12) repetitions of the total repetitions |
| Stage | Non-Verbal | Verbal |
|---|---|---|
| Greeting | Waves arms to the user | “Hello, my name is Pepper, your personal exercise coach. We are going to do nine different exercises together. Each cycle of an exercise has n repetitions. If you are tired, please stop doing the exercise, don’t force yourself!” “Are you ready?” |
| Introduceexercise (every week, visual shows exercise) | Performs the poses for the exercise | “First, we will do an exercise called open arm stretches. Let me show you how to do it.” |
| Introduce exercise (only week one shows with detailed instructions) | Performs the poses for the exercise | “Start by bringing your arms up to the middle of your chest. And open them sideways, like this. And then close your arms. Finally put your arms back down.” |
| Prompt to perform repetitions | Performs the poses for the exercise | “We are going to do eight repetitions.” “Let’s get started.” “Eight, seven …, last one!” |
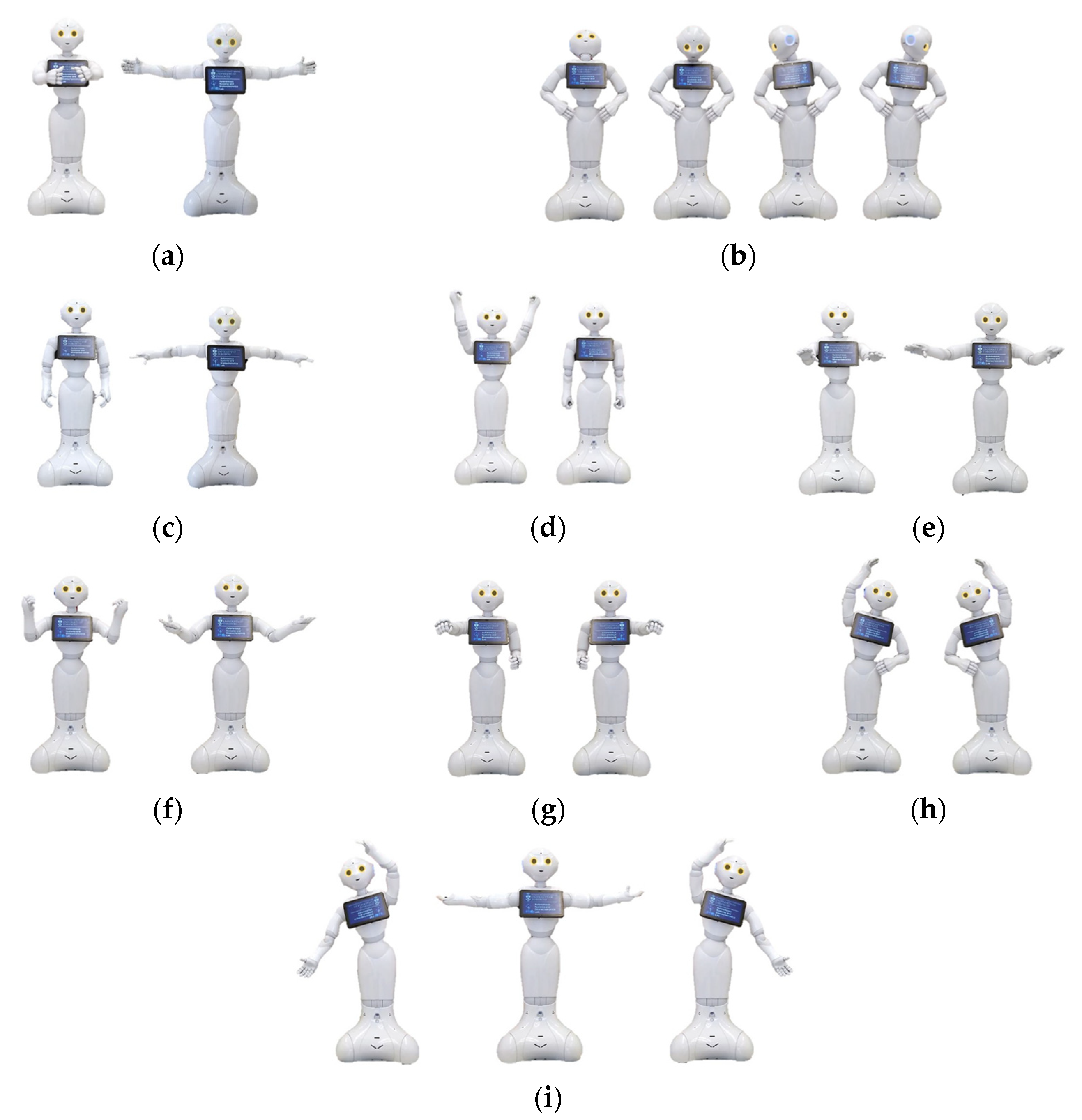
| Congratulate (happy) | Happy robot emotion display Example: Arms open  | “Excellent job! I really enjoy doing this exercise with you.” |
| Congratulate (interested) | Interested robot emotion display Example: Nodding  | “You did the exercise really well!” |
| Encouragement (worried) | Worried robot emotion display Example: Covering face  | “Let me know if you are feeling tired. Otherwise, we are going to move to the next exercise.” |
| Encouragement (sad) | Sad robot emotion display Example: Scratching head  | “It’s too bad you did not like this exercise. Hopefully you will like the next one more.” |
| Farewell | Waves goodbye to the user | “I hope the rest of your day goes well. Let’s do this again sometime. Bye for now!” |
| Session Type | First Week | One Month | Two Month | Entire Duration |
|---|---|---|---|---|
| One-on-One | 62.92 ± 6.03 | 64.29 ± 6.20 | 63.19 ± 5.13 | 64.03 ± 4.92 |
| Group | 64.72 ± 2.46 | 67.50 ± 1.40 | 67.78 ± 0.91 | 66.67 ± 2.11 |
| All users | 63.28 ± 5.50 | 64.95 ± 5.69 | 64.11 ± 4.94 | 64.27 ± 4.80 |
| User States | Time Period | One-on-One Percent of Interaction Time | Percent of Interaction Time | Percent of Interaction Time |
|---|---|---|---|---|
| Positive Valence (%) | First Week | 93.04 ± 3.30 | 92.26 ± 2.94 | 92.89 ± 3.09 |
| One Month | 90.34 ± 5.65 | 90.26 ± 11.04 | 90.32 ± 6.26 | |
| Two Month | 89.90 ± 13.69 | 97.49 ± 1.94 | 91.42 ± 12.51 | |
| Entire Duration | 86.88 ± 17.76 | 91.13 ± 10.39 | 87.73 ± 16.68 | |
| Engagement (%) | First Week | 98.49 ± 0.85 | N/A | 98.49 ± 0.85 |
| One Month | 98.93 ± 0.91 | N/A | 98.93 ± 0.91 | |
| Two Month | 98.41 ± 1.85 | N/A | 98.41 ± 1.85 | |
| Entire Duration | 97.29 ± 6.82 | N/A | 97.29 ± 6.82 | |
| Heart rate (bpm) | Entire Duration | 81.56 ± 3.91 | 85.61 ± 2.96 | 82.37 ± 3.97 |
| Session Type | First Week | One Month | Two Months | ||||||
|---|---|---|---|---|---|---|---|---|---|
| One-on-One | 1.25 | 0.83 | 1.50 | 1.25 | 0.83 | 1.50 | 1.38 | 0.70 | 1.50 |
| Group | 1.37 | 0.81 | 2.00 | 1.32 | 1.08 | 2.00 | 1.11 | 0.91 | 1.00 |
| All | 1.33 | 0.82 | 2.00 | 1.30 | 1.01 | 2.00 | 1.19 | 0.86 | 1.00 |
| Robot Features | Group Sessions | One-on-One Sessions | All Users Combined |
|---|---|---|---|
| Eyes | 1 (tied) | 3 | 2 |
| Arms and movement | 1 (tied) | 1 | 1 |
| Voice | 3 (tied) | 2 | 3 |
| Assistance | 5 | 4 (tied) | 5 |
| Size | 3 (tied) | 4 (tied) | 4 |
| Lower body | 6 | 6 | 6 |
| Activities | Rank |
|---|---|
| Dressing | 4 |
| Meal eating | 5 |
| Meal preparation | 6 |
| Play games | 1 |
| Reminder | 3 |
| Escorting | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shao, M.; Pham-Hung, M.; Alves, S.F.D.R.; Snyder, M.; Eshaghi, K.; Benhabib, B.; Nejat, G. Long-Term Exercise Assistance: Group and One-on-One Interactions between a Social Robot and Seniors. Robotics 2023, 12, 9. https://doi.org/10.3390/robotics12010009
Shao M, Pham-Hung M, Alves SFDR, Snyder M, Eshaghi K, Benhabib B, Nejat G. Long-Term Exercise Assistance: Group and One-on-One Interactions between a Social Robot and Seniors. Robotics. 2023; 12(1):9. https://doi.org/10.3390/robotics12010009
Chicago/Turabian StyleShao, Mingyang, Michael Pham-Hung, Silas Franco Dos Reis Alves, Matt Snyder, Kasra Eshaghi, Beno Benhabib, and Goldie Nejat. 2023. "Long-Term Exercise Assistance: Group and One-on-One Interactions between a Social Robot and Seniors" Robotics 12, no. 1: 9. https://doi.org/10.3390/robotics12010009