
Lightweight Bioinspired Exoskeleton for Wrist Rehabilitation Powered by Twisted and Coiled Artificial Muscles

 , , and
, , and
Abstract
:1. Introduction
2. TCAMs-Exo Design
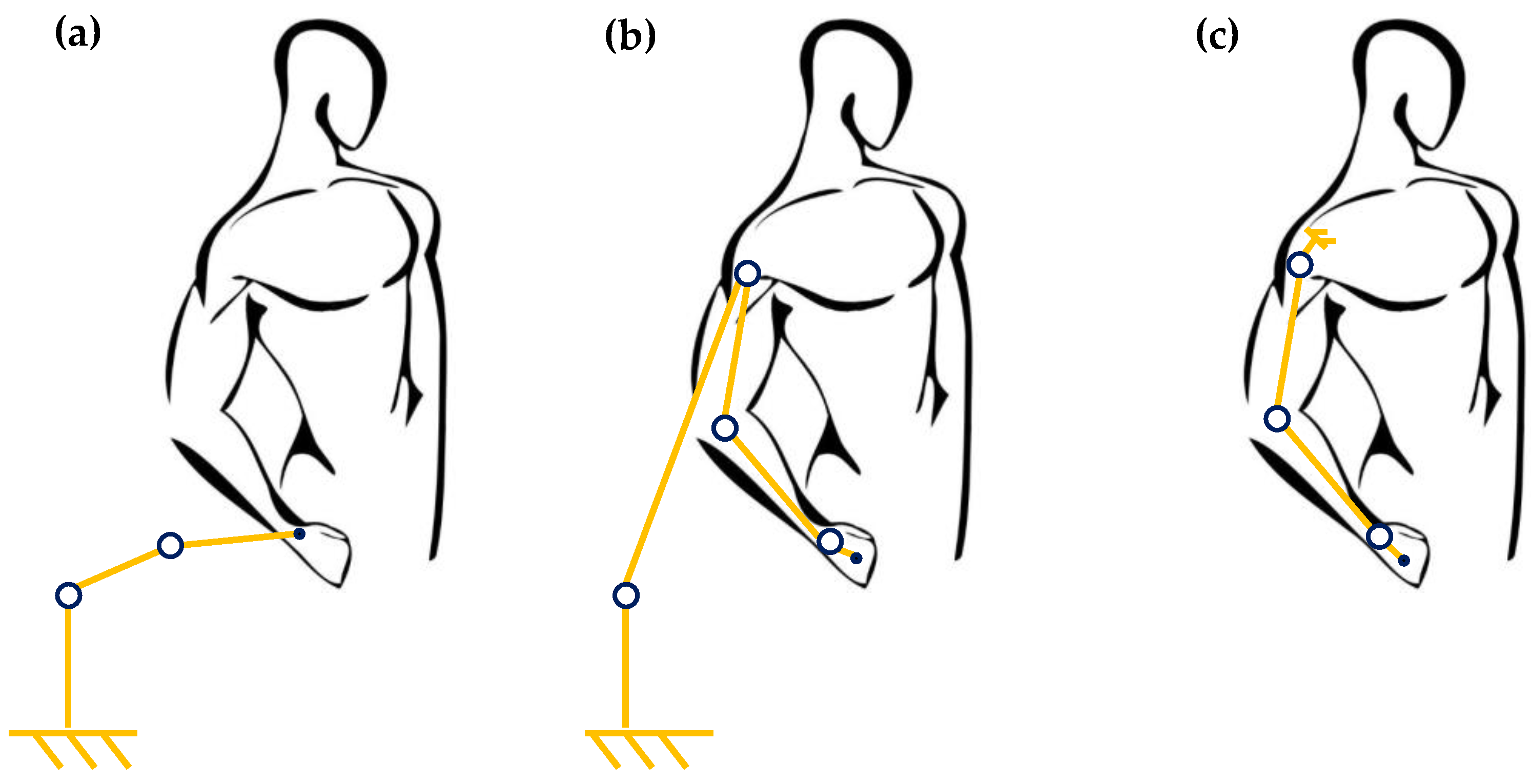
2.1. Bioinspired Design

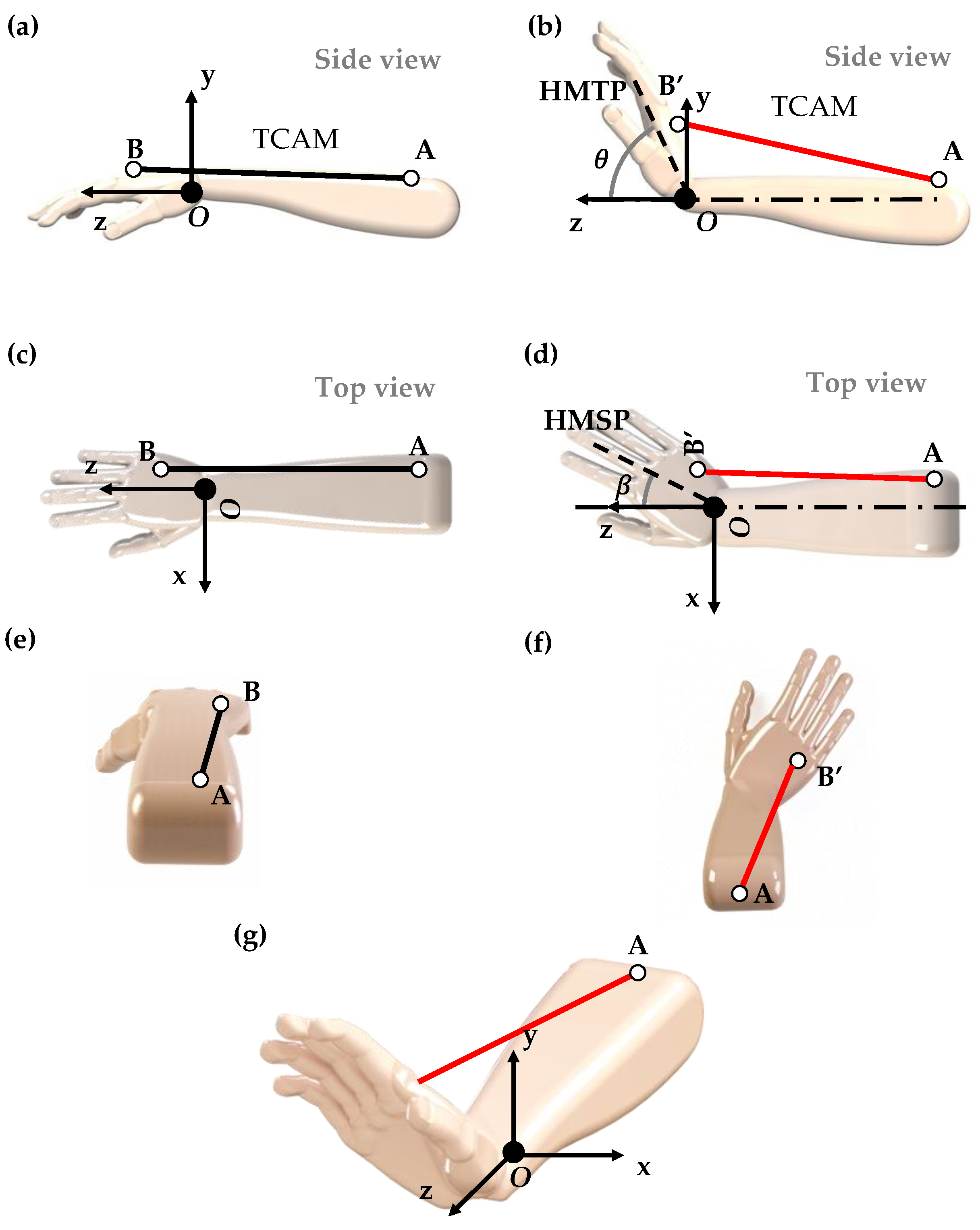
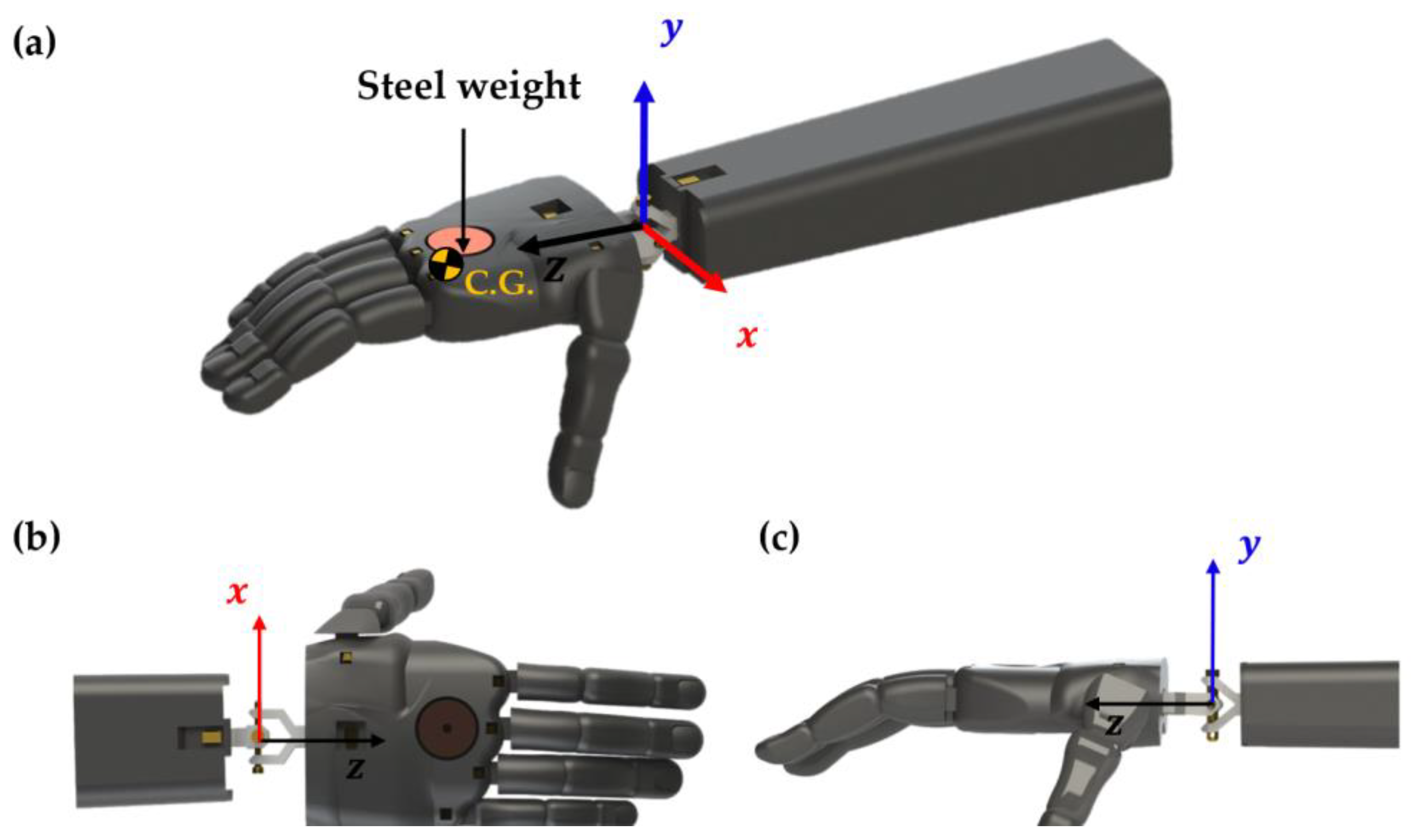
2.2. Geometrical and Biomechanical Considerations
2.3. TCAMs Contraction and ROM
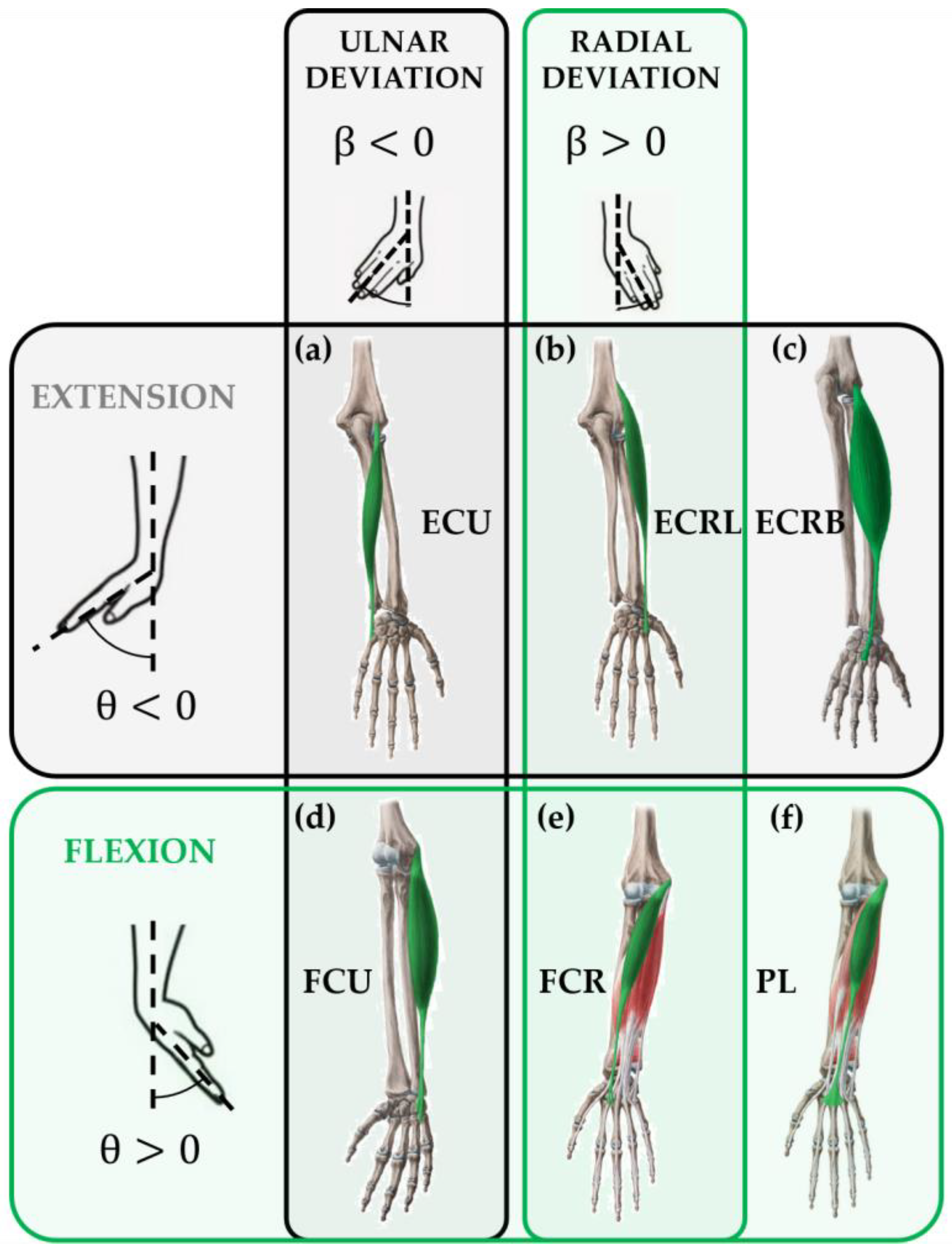
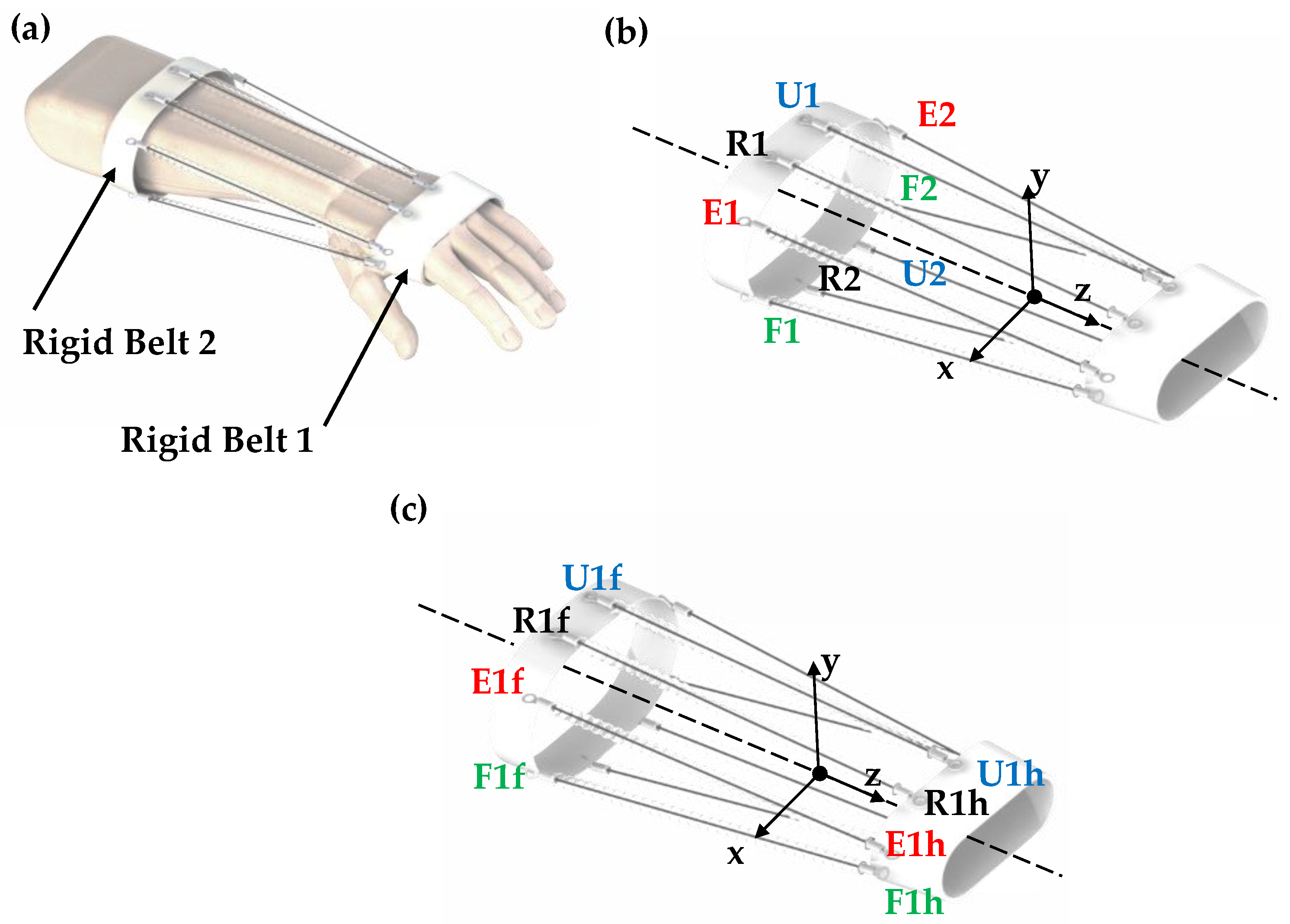
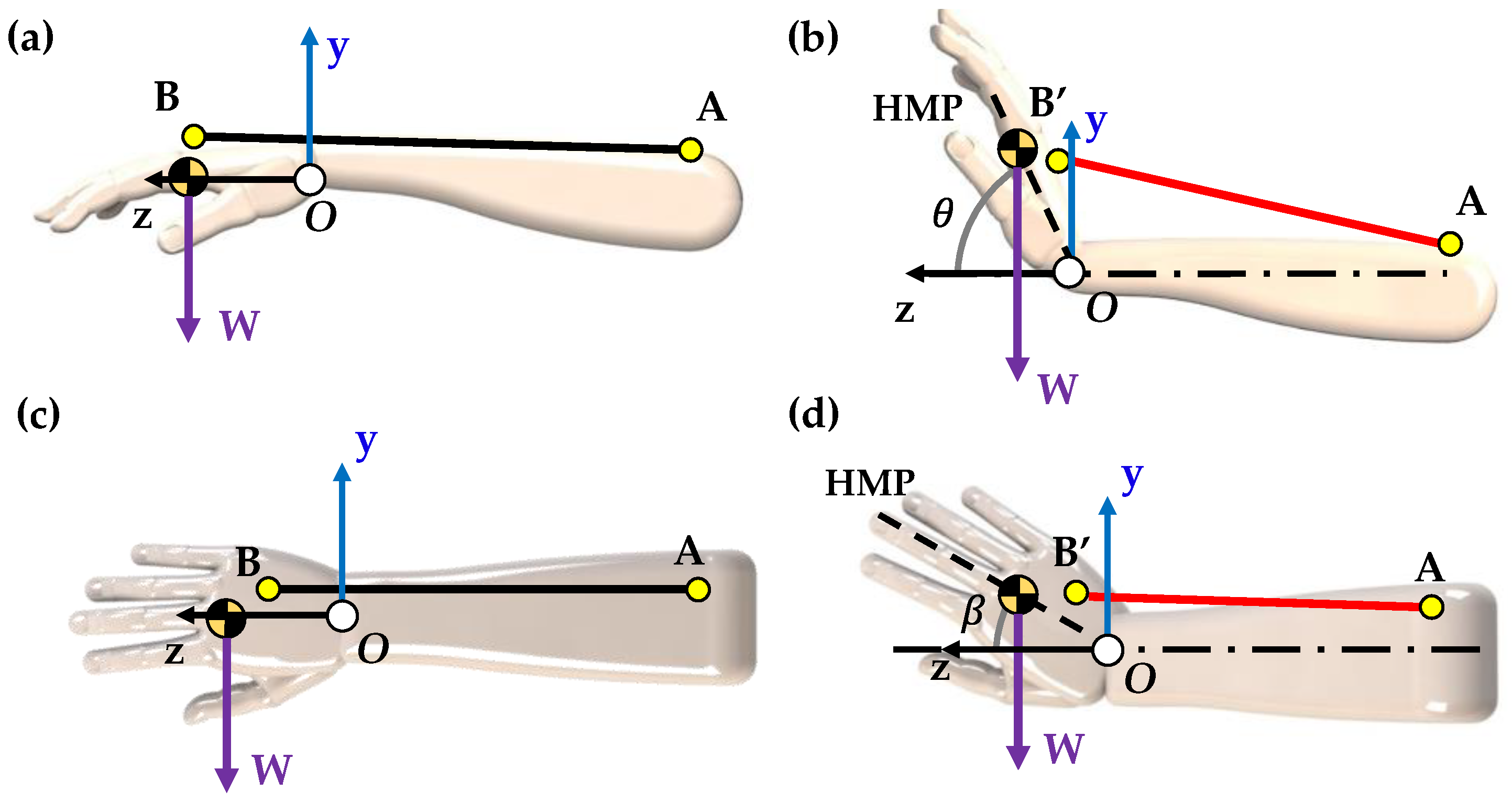
2.4. Extensional and Flexional Motions

2.5. Ulnar and Radial Deviation Motions
2.6. Load Capacity of TCAMs
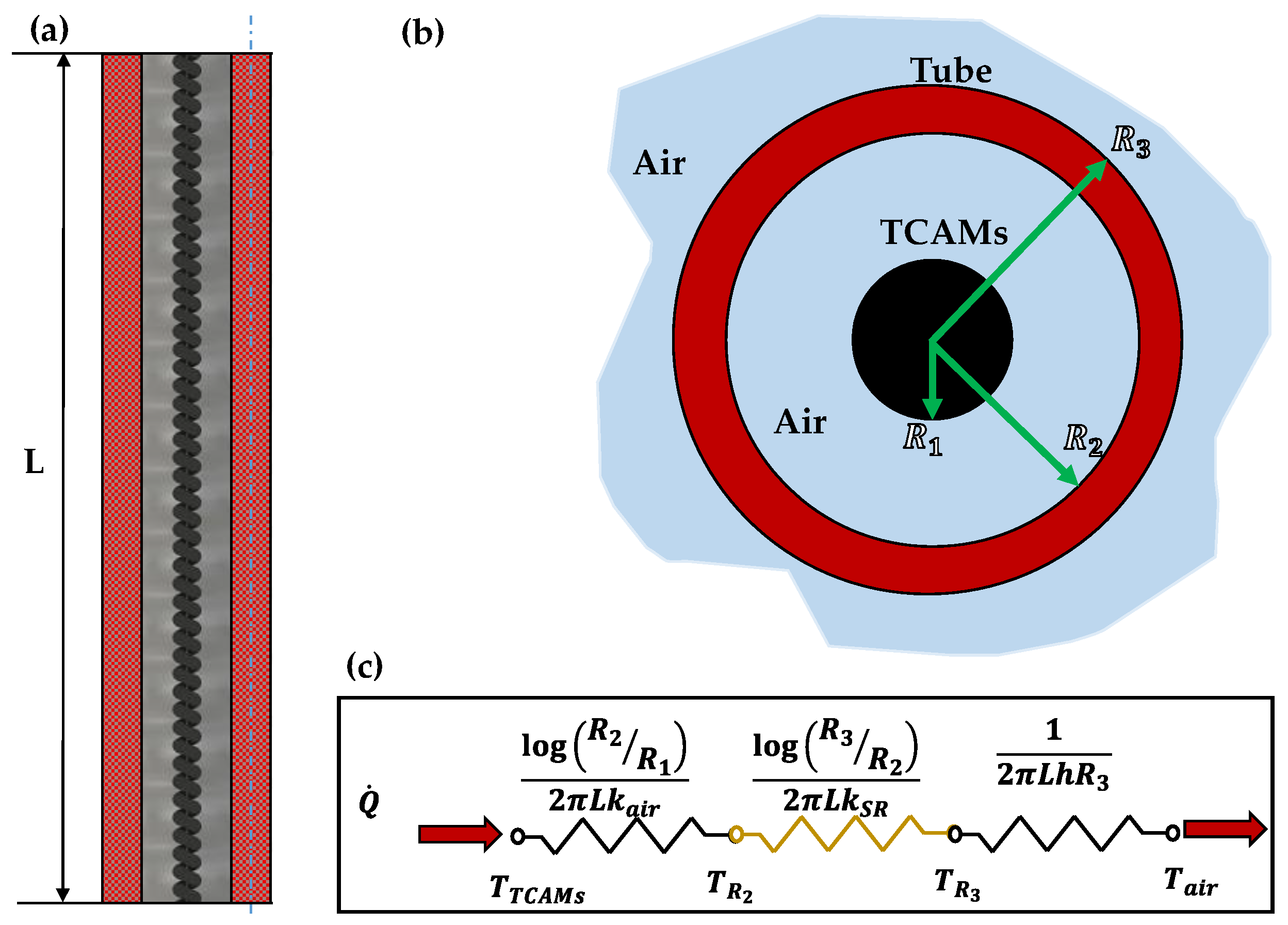
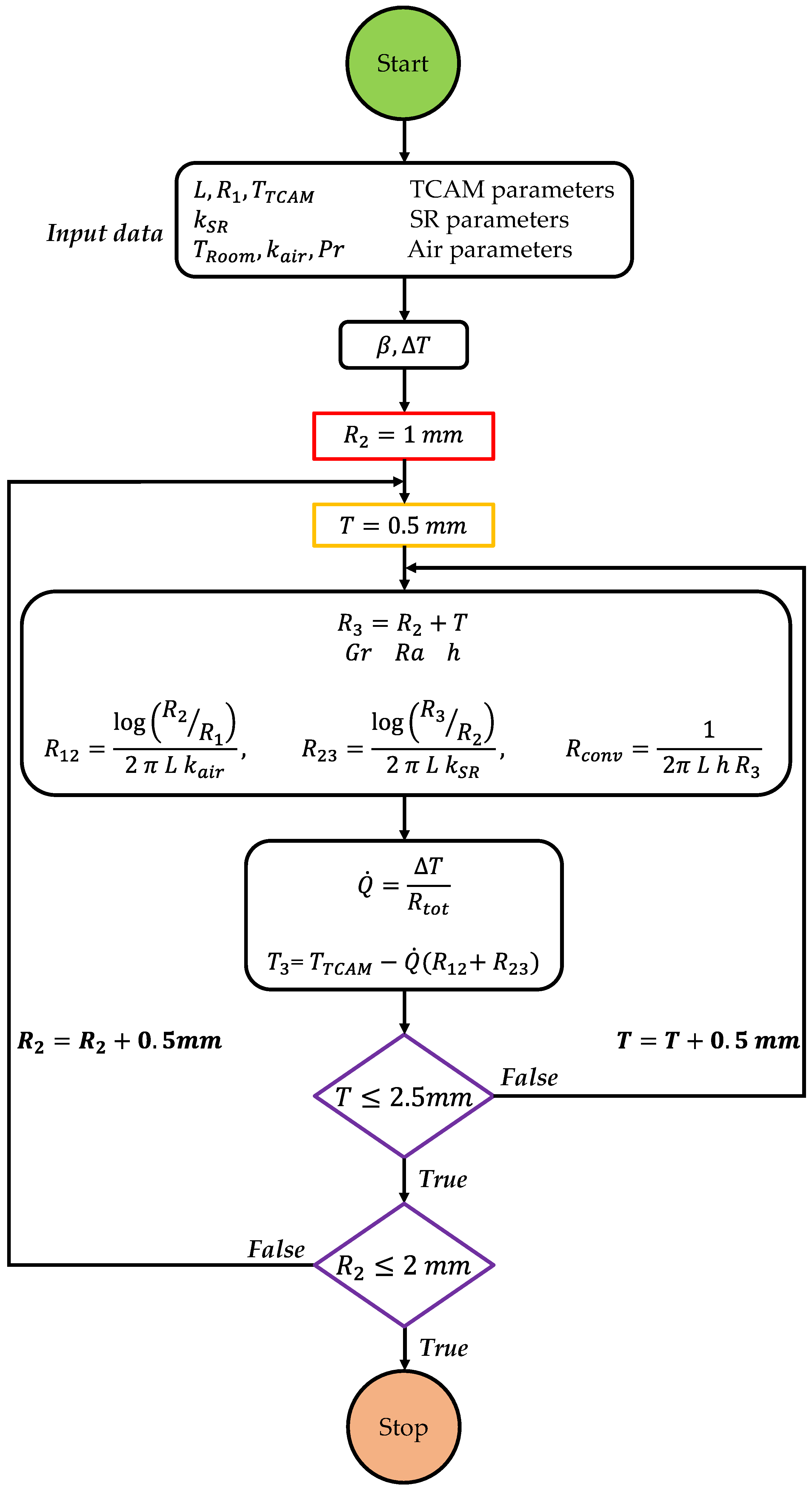
3. Theory of TCAM Insulation Model
4. Experimental Setup
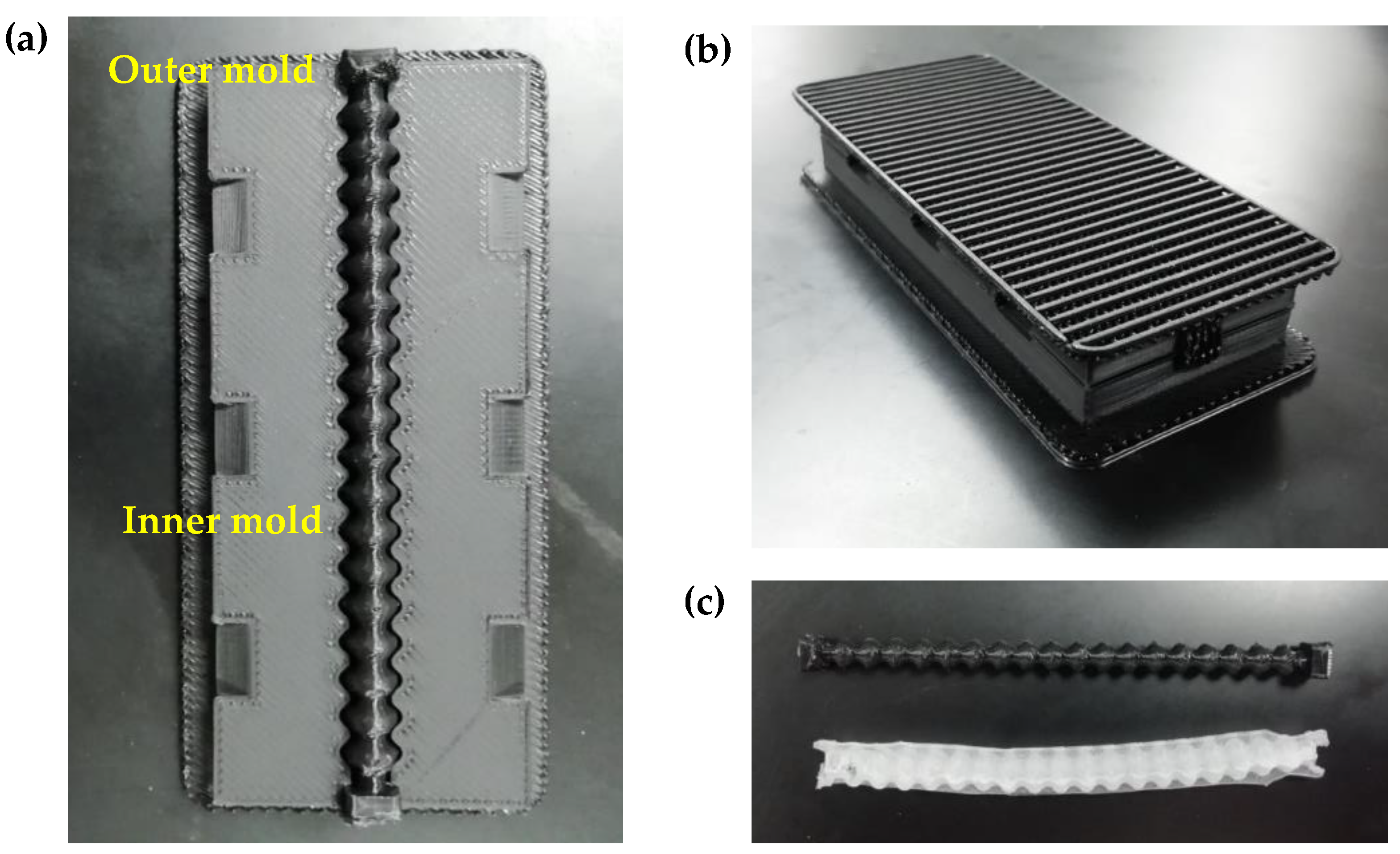
4.1. Three-Dimensional Prototype of the TCAM-Exo
4.2. The NDL
4.3. Thermal Insulating Tubes
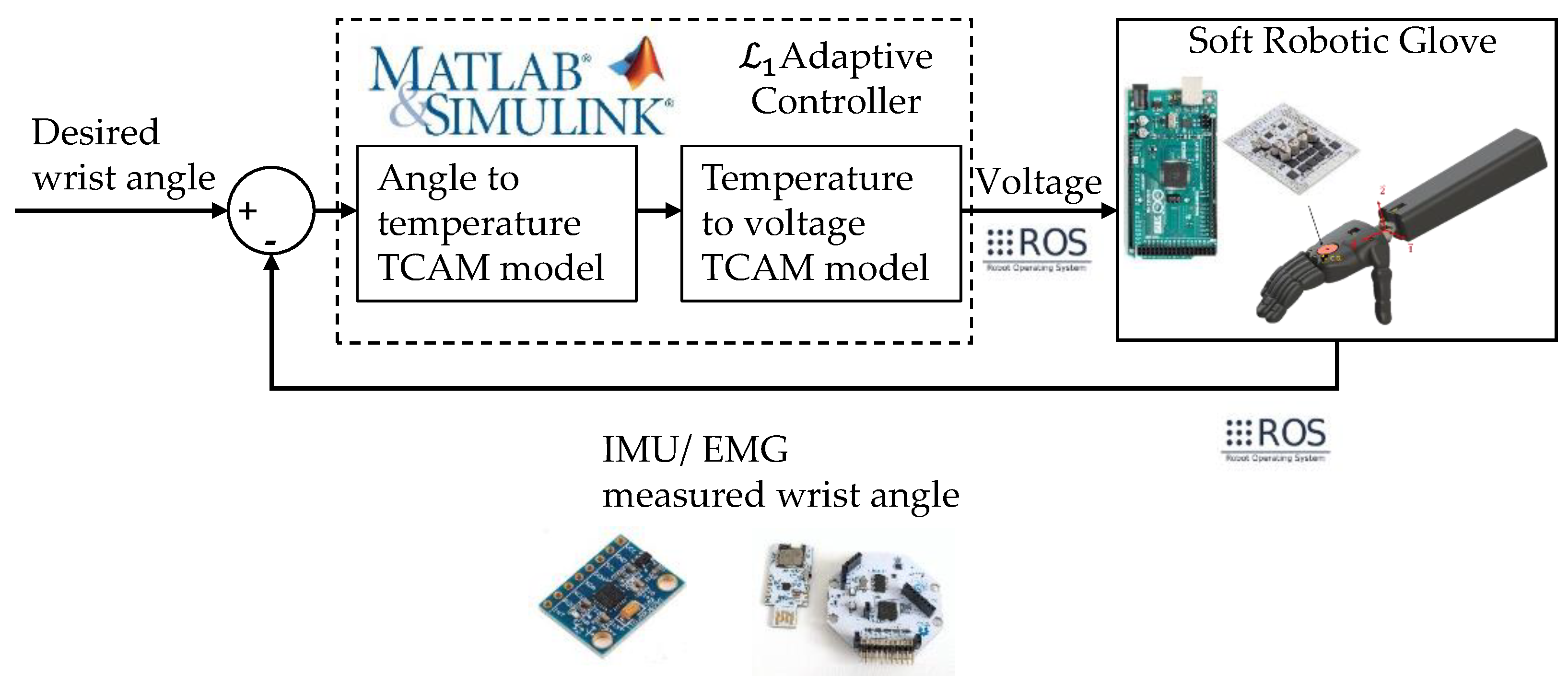
4.4. The Adaptive Controller for Robust Actuation of the TCAMs
5. Results and Discussion
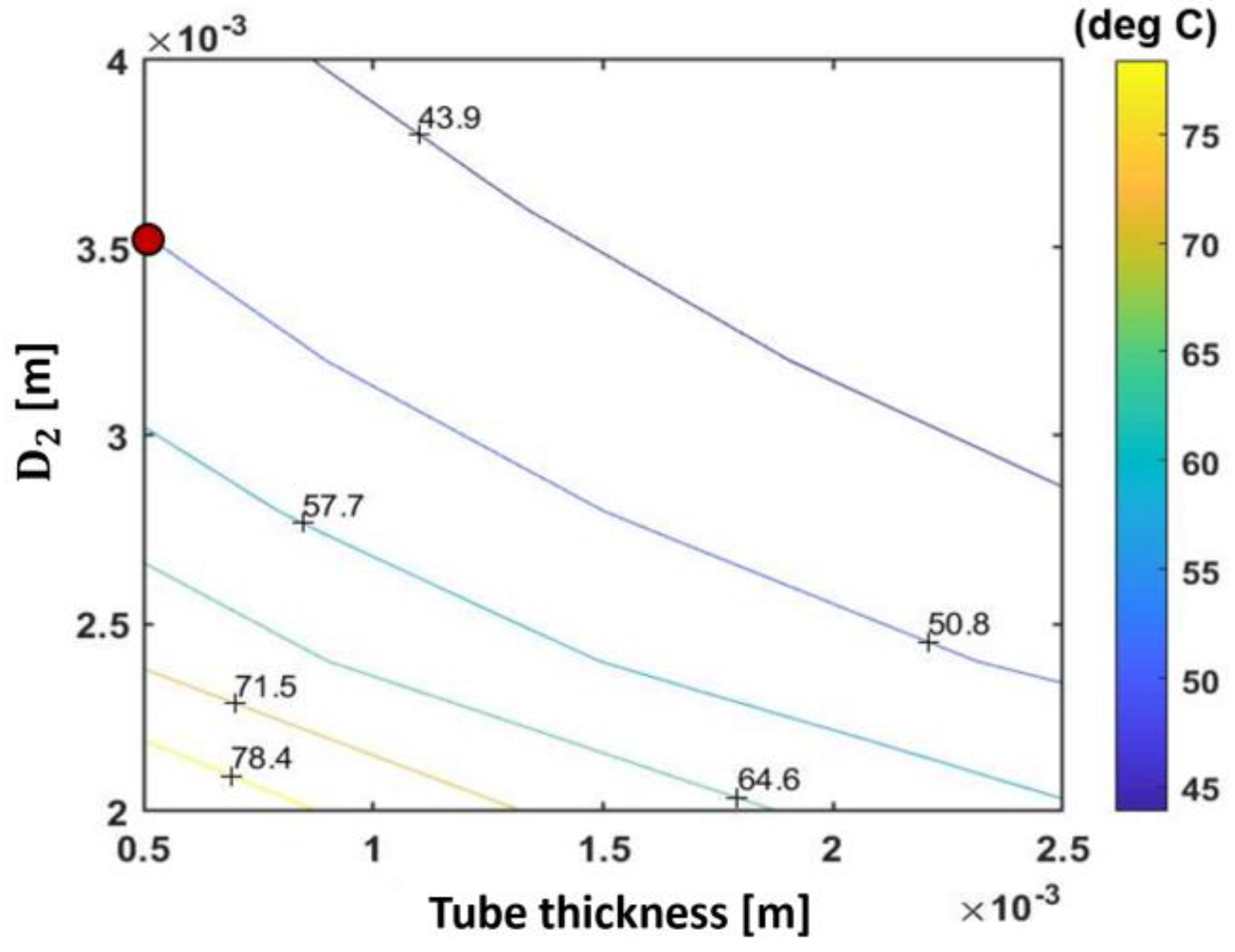
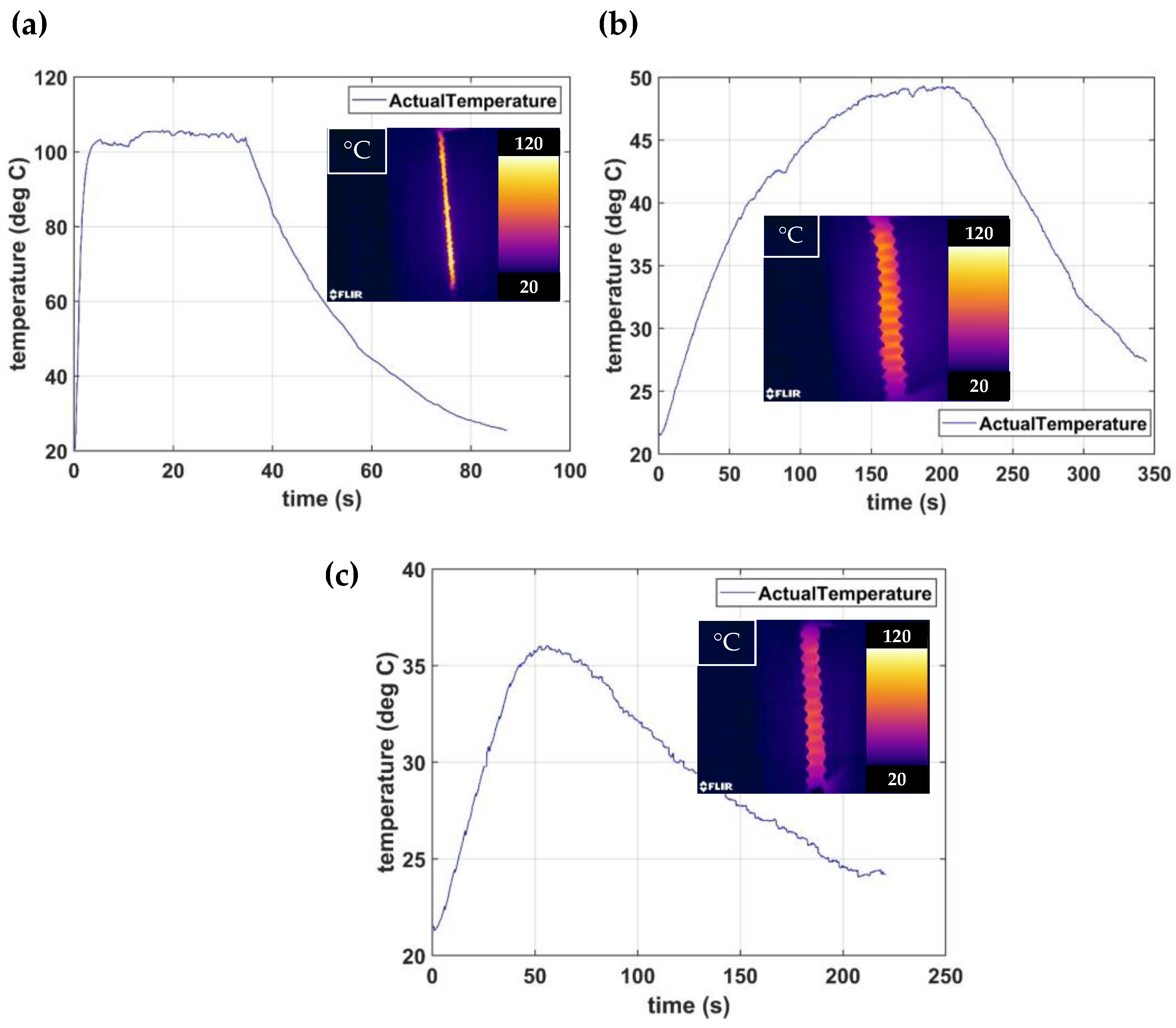
5.1. Thermal Insulation System Assessment
5.2. Passive Rehabilitation Exercise
5.3. Active Rehabilitation Exercise
5.4. Human–Machine Interaction
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Krigger, K.W. Cerebral palsy: An overview. Am. Fam. Physician 2006, 73, 91–100. [Google Scholar]
- Aisen, M.L.; Kerkovich, D.; Mast, J.; Mulroy, S.; Wren, T.A.L.; Kay, R.M.; Rethlefsen, S.A. Cerebral palsy: Clinical care and neurological rehabilitation. Lancet Neurol. 2011, 10, 844–852. [Google Scholar] [CrossRef]
- Øtensjø, S.; Carlberg, E.B.; Vøllestad, N.K. Motor impairments in young children with cerebral palsy: Relationship to gross motor function and everyday activities. Dev. Med. Child Neurol. 2004, 46, 580–589. [Google Scholar] [CrossRef]
- Snoek, G.J.; Ijzerman, M.J.; Hermens, H.J.; Maxwell, D.; Biering-Sorensen, F. Survey of the needs of patients with spinal cord injury: Impact and priority for improvement in hand function in tetraplegics. Spinal Cord 2004, 42, 526–532. [Google Scholar] [CrossRef]
- Cox, R.J.; Amsters, D.I.; Pershouse, K.J. The need for a multidisciplinary outreach service for people with spinal cord injury living in the community. Clin. Rehabil. 2001, 15, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart disease and stroke statistics—2020 update: A report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef]
- Delph, M.A.; Fischer, S.A.; Gauthier, P.W.; Luna, C.H.M.; Clancy, E.A.; Fischer, G.S. A soft robotic exomusculature glove with integrated sEMG sensing for hand rehabilitation. In Proceedings of the 2013 IEEE 13th International Conference on Rehabilitation Robotics (ICORR), Seattle, WA, USA, 24–26 June 2013; pp. 1–7. [Google Scholar] [CrossRef]
- Canning, C.G.; Ada, L.; Adams, R.; O’Dwyer, N.J. Loss of strength contributes more to physical disability after stroke than loss of dexterity. Clin. Rehabil. 2004, 18, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, S. Motor Impairments Following Stroke. 2015. Available online: https://www.researchgate.net/publication/281198195_Motor_impairments_following_stroke (accessed on 18 January 2023).
- Raghavan, P. Upper Limb Motor Impairment after Stroke. Phys. Med. Rehabil. Clin. 2015, 26, 599–610. [Google Scholar] [CrossRef]
- Wolfe, C.D.A. The Impact of Stroke; British Medical Bulletin: London, UK, 2000; Volume 56, pp. 275–286. [Google Scholar]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics—2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef] [PubMed]
- Nichols, M.; Townsend, N.; Rayner, M. European cardiovascular disease statistics. Eur. Heart Netw. Eur. Soc. Cardiol. 2012, 1, 10–123. [Google Scholar]
- Olsen, T.S. Arm and leg paresis as outcome predictors in stroke rehabilitation. Stroke 1990, 21, 247–251. [Google Scholar] [CrossRef] [Green Version]
- Bütefisch, C.; Hummelsheim, H.; Denzler, P.; Mauritz, K.H. Repetitive training of isolated movements improves the outcome of motor rehabilitation of the centrally paretic hand. J. Neurol. Sci. 1995, 130, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Carey, J.R.; Kimberley, T.J.; Lewis, S.M.; Auerbach, E.J.; Dorsey, L.; Rundquist, P.; Ugurbil, K. Analysis of fMRI and finger tracking training in subjects with chronic stroke. Brain 2002, 125, 773–788. [Google Scholar] [CrossRef] [PubMed]
- Carey, J.R.; Durfee, W.K.; Bhatt, E.; Nagpal, A.; Weinstein, S.A.; Anderson, K.M.; Lewis, S.M. Comparison of finger tracking versus simple movement training via telerehabilitation to alter hand function and cortical reorganization after stroke. Neurorehabil. Neural Repair 2007, 21, 216–232. [Google Scholar] [CrossRef] [PubMed]
- Lum, P.; Reinkensmeyer, D.; Mahoney, R.; Rymer, W.Z.; Burgar, C. Robotic devices for movement therapy after stroke: Current status and challenges to clinical acceptance. Top. Stroke Rehabil. 2002, 8, 40–53. [Google Scholar] [CrossRef]
- Hu, X.L.; Tong, K.Y.; Song, R.; Zheng, X.J.; Lui, K.H.; Leung, W.W.F.; Ng, S.; Au-Yeung, S.S.Y. Quantitative evaluation of motor functional recovery process in chronic stroke patients during robot-assisted wrist training. J. Electromyogr. Kinesiol. 2009, 19, 639–650. [Google Scholar] [CrossRef]
- Volpe, B.T.; Krebs, H.I.; Hogan, N.; Edelstein, L.; Diels, C.; Aisen, M. A novel approach to stroke rehabilitation: Robot-aided sensorimotor stimulation. Neurology 2000, 54, 1938–1944. [Google Scholar] [CrossRef]
- Norouzi-Gheidari, N.; Archambault, P.S.; Fung, J. Effects of robot-assisted therapy on stroke rehabilitation in upper limbs: Systematic review and meta-analysis of the literature. J. Rehabil. Res. Dev. 2012, 49, 479–496. [Google Scholar] [CrossRef]
- Dombovy, M.L. Emerging therapies in neurorehabilitation. Contin. Lifelong Learn. Neurol. 2011, 17, 530–544. [Google Scholar] [CrossRef]
- Fasoli, S.E.; Krebs, H.I.; Stein, J.; Frontera, W.R.; Hogan, N. Effects of robotic therapy on motor impairment and recovery in chronic stroke. Arch. Phys. Med. Rehabil. 2003, 84, 477–482. [Google Scholar] [CrossRef]
- Prange, G.B.; Jannink, M.J.A.; Groothuis-Oudshoorn, C.G.M.; Hermens, H.J.; Ijzerman, M.J. Systematic review of the effect of robot-aided therapy on recovery of the hemiparetic arm after stroke. J. Rehabil. Res. Dev. 2006, 43, 171–184. [Google Scholar] [CrossRef] [Green Version]
- Brewer, B.R.; McDowell, S.K.; Worthen-Chaudhari, L.C. Poststroke upper extremity rehabilitation: A review of robotic systems and clinical results. Top. Stroke Rehabil. 2007, 14, 22–44. [Google Scholar] [CrossRef]
- Maciejasz, P.; Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Troy, A.; Leonhardt, S. A survey on robotic devices for upper limb rehabilitation. J. NeuroEng. Rehabil. 2014, 11, 3. [Google Scholar] [CrossRef]
- Mehrholz, J.; Pohl, M. Electromechanical-assisted gait training after stroke: A systematic review comparing end-effector and exoskeleton devices. J. Rehabil. Med. 2012, 44, 193–199. [Google Scholar] [CrossRef]
- Chu, C.Y.; Patterson, R.M. Soft robotic devices for hand rehabilitation and assistance: A narrative review. J. NeuroEng. Rehabil. 2018, 15, 9. [Google Scholar] [CrossRef]
- Lo, H.S.; Xie, S.Q. Exoskeleton robots for upper-limb rehabilitation: State of the art and future prospects. Med. Eng. Phys. 2012, 34, 261–268. [Google Scholar] [CrossRef]
- Molteni, F.; Gasperini, G.; Cannaviello, G.; Guanziroli, E. Exoskeleton and End-Effector Robots for Upper and Lower Limbs Rehabilitation: Narrative Review. PMR 2018, 10, S174–S188. [Google Scholar] [CrossRef]
- Aggogeri, F.; Mikolajczyk, T.; O’Kane, J. Robotics for rehabilitation of hand movement in stroke survivors. Adv. Mech. Eng. 2019, 11, 1–14. [Google Scholar] [CrossRef]
- Lee, S.H.; Park, G.; Cho, D.Y.; Kim, H.Y.; Lee, J.Y.; Kim, S.; Park, S.B.; Shin, J.H. Comparisons between end-effector and exoskeleton rehabilitation robots regarding upper extremity function among chronic stroke patients with moderate-to-severe upper limb impairment. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Piggott, L.; Wagner, S.; Ziat, M. Haptic neurorehabilitation and virtual reality for upper limb paralysis: A review. Crit. Rev. Biomed. Eng. 2016, 44, 1–32. [Google Scholar] [CrossRef]
- Gopura, R.A.R.C.; Bandara, D.S.V.; Kiguchi, K.; Mann, G.K.I. Developments in hardware systems of active upper-limb exoskeleton robots: A review. Rob. Auton. Syst. 2016, 75, 203–220. [Google Scholar] [CrossRef]
- Hussain, S.; Jamwal, P.K.; Van Vliet, P.; Ghayesh, M.H. State-of-The-Art Robotic Devices for Wrist Rehabilitation: Design and Control Aspects. IEEE Trans. Hum. Mach. Syst. 2020, 50, 361–372. [Google Scholar] [CrossRef]
- Pehlivan, A.U.; Lee, S.; O’Malley, M.K. Mechanical design of RiceWrist-S: A forearm-wrist exoskeleton for stroke and spinal cord injury rehabilitation. In Proceedings of the IEEE RAS and EMBS International Conference on Biomedical Robotics and Biomechatronics, Rome, Italy, 24–27 June 2012; pp. 1573–1578. [Google Scholar] [CrossRef]
- Martinez, J.A.; Ng, P.; Lu, S.; Campagna, M.S.; Celik, O. Design of Wrist Gimbal: A forearm and wrist exoskeleton for stroke rehabilitation. In Proceedings of the IEEE International Conference on Rehabilitation Robotics, Seattle, WA, USA, 24–26 June 2013. [Google Scholar] [CrossRef]
- French, J.A.; Rose, C.G.; O’Malley, M.K. System characterization of MAHI Exo-II: A robotic exoskeleton for upper extremity rehabilitation. In Proceedings of the ASME 2014 Dynamic Systems and Control Conference, San Antonio, TX, USA, 22–24 October 2014; Volume 3. [Google Scholar] [CrossRef]
- Pezent, E.; Rose, C.G.; Deshpande, A.D.; O’Malley, M.K. Design and characterization of the OpenWrist: A robotic wrist exoskeleton for coordinated hand-wrist rehabilitation. In Proceedings of the IEEE International Conference on Rehabilitation Robotics, London, UK, 17–20 July 2017; pp. 720–725. [Google Scholar] [CrossRef]
- Su, Y.Y.; Yu, Y.L.; Lin, C.H.; Lan, C.C. A compact wrist rehabilitation robot with accurate force/stiffness control and misalignment adaptation. Int. J. Intell. Robot. Appl. 2019, 3, 45–58. [Google Scholar] [CrossRef]
- Mayetin, U.; Kucuk, S. Design and Experimental Evaluation of a Low Cost, Portable, 3-DOF Wrist Rehabilitation Robot with High Physical Human–Robot Interaction. J. Intell. Robot. Syst. Theory Appl. 2022, 106, 65. [Google Scholar] [CrossRef]
- Gonçalves, R.S.; Brito, L.S.F.; Moraes, L.P.; Carbone, G.; Ceccarelli, M. A fairly simple mechatronic device for training human wrist motion. Int. J. Adv. Robot. Syst. 2020, 17, 1–15. [Google Scholar] [CrossRef]
- Zhang, L.; Li, J.; Cui, Y.; Dong, M.; Fang, B.; Zhang, P. Design and performance analysis of a parallel wrist rehabilitation robot (PWRR). Rob. Auton. Syst. 2020, 125, 103390. [Google Scholar] [CrossRef]
- Xu, D.; Zhang, M.; Sun, Y.; Zhang, X.; Xu, H.; Li, Y.; Li, X.; Xie, S.Q. Development of a reconfigurable wrist rehabilitation device with an adaptive forearm holder. In Proceedings of the 2018 IEEE/ASME International Conference on Advanced Intelligent Mechatronics (AIM), Auckland, New Zealand, 9–12 July 2018; pp. 454–459. [Google Scholar] [CrossRef] [Green Version]
- Shi, K.; Song, A.; Li, Y.; Chen, D.; Li, H. Cable-Driven 3-DOF Wrist Rehabilitation Robot with optimized Human-Robot Interaction Performance. In Proceedings of the 2020 8th IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics (BioRob), New York, NY, USA, 29 November–1 December 2020; pp. 112–117. [Google Scholar] [CrossRef]
- Jeong, J.; Yasir, I.B.; Han, J.; Park, C.H.; Bok, S.K.; Kyung, K.U. Design of shape memory alloy-based soft wearable robot for assistingwrist motion. Appl. Sci. 2019, 9, 4025. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, Q. Design and testing of a soft parallel robot based on pneumatic artificial muscles for wrist rehabilitation. Sci. Rep. 2021, 11, 1273. [Google Scholar] [CrossRef]
- Perry, J.C.; Rosen, J. Design of a 7 degree-of-freedom upper-limb powered exoskeleton. In Proceedings of the First IEEE/RAS-EMBS International Conference on Biomedical Robotics and Biomechatronics, Pisa, Italy, 20–22 February 2006; Volume 2006, pp. 805–810. [Google Scholar] [CrossRef]
- Lamuta, C.; Messelot, S.; Tawfick, S. Theory of the tensile actuation of fiber reinforced coiled muscles. Smart Mater. Struct. 2018, 27, 55018. [Google Scholar] [CrossRef]
- Zhou, Y.M.; Hohimer, C.; Proietti, T.; O’Neill, C.T.; Walsh, C.J. Kinematics-Based Control of an Inflatable Soft Wearable Robot for Assisting the Shoulder of Industrial Workers. IEEE Robot. Autom. Lett. 2021, 6, 2155–2162. [Google Scholar] [CrossRef]
- Weerakkody, T.H.; Liyanaarachchi, N.; Herath, H.M.C.; Gopura, R.A.R.C.; Thilina, D.L. Development of an Active Shoulder Prosthesis with Low-Level Control Validation. Model. Identif. Control 2017, 848, 194–199. [Google Scholar] [CrossRef]
- De la Cruz-Sánchez, B.A.; Arias-Montiel, M.; Lugo-González, E. EMG-controlled hand exoskeleton for assisted bilateral rehabilitation. Biocybern. Biomed. Eng. 2022, 42, 596–614. [Google Scholar] [CrossRef]
- Hovakimyan, N.; Cao, C. L1 Adaptive Control Theory: Guaranteed Robustness with Fast Adaptation (Advances in Design and Control); SIAM: Philadelphia, PA, USA, 2010; ISBN 0898717043. [Google Scholar]
- Hammond, M.; Cichella, V.; Weerakkody, T.; Lamuta, C. Robust and Adaptive Sampled-Data Control of Twisted and Coiled Artificial Muscles. IEEE Control Syst. Lett. 2022, 6, 1232–1237. [Google Scholar] [CrossRef]
- Hirt, B.; Seyhan, H.; Wagner, M.; Zumhasch, R. Hand and wrist anatomy and biomechanics: A comprehensive guide. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 1029. [Google Scholar] [CrossRef] [Green Version]
- Betts, J.G.; Young, K.A.; Wise, J.A.; Johnson, E.; Poe, B.; Kruse, D.H.; Korol, O.; Johnson, J.E.; Womble, M.; DeSaix, P. Anatomy and Physiology; OpenStax College, Rice University: Houston, TX, USA, 2013. [Google Scholar]
- Boles, C.A.; Kannam, S.; Cardwell, A.B. The forearm: Anatomy of muscle compartments and nerves. Am. J. Roentgenol. 2000, 174, 151–159. [Google Scholar] [CrossRef]
- Ken Hub. Musculoskeletal System-Anatomy|Kenhub; Ken Hub: Berlin, Germany, 2018. [Google Scholar]
- Greco, C.; Kotak, P.; Pagnotta, L.; Lamuta, C. The evolution of mechanical actuation: From conventional actuators to artificial muscles. Int. Mater. Rev. 2022, 67, 575–619. [Google Scholar] [CrossRef]
- Plagenhoef, S.; Gaynor Evans, F.; Abdelnour, T. Anatomical Data for Analyzing Human Motion. Res. Q. Exerc. Sport 1983, 54, 169–178. [Google Scholar] [CrossRef]
- Pheasant, S.; Haslegrave, C.M.A.D. Bodyspace Anthropometry, Ergonomics and the Design of Work; CRC Press: Boca Raton, FL, USA, 2018; pp. 239–279. [Google Scholar]
- Mirvakili, S.M.; Pazukha, A.; Sikkema, W.; Sinclair, C.W.; Spinks, G.M.; Baughman, R.H.; Madden, J.D.W. Niobium nanowire yarns and their application as artificial muscles. Adv. Funct. Mater. 2013, 23, 4311–4316. [Google Scholar] [CrossRef]
- Churchill, S.W.; Chu, H.H.S. Correlating equations for laminar and turbulent free convection from a vertical plate. Int. J. Heat Mass Transf. 1975, 18, 1323–1329. [Google Scholar] [CrossRef]
- Frederick, R.L.; Quiroz, F. On the transition from conduction to convection regime in a cubical enclosure with a partially heated wall. Int. J. Heat Mass Transf. 2001, 44, 1699–1709. [Google Scholar] [CrossRef]
- Bell, S.; Bangel, A.; Weerakkody, T.; Song, X.; Lamuta, C. Automated manufacturing system for carbon fiber-based twisted and coiled artificial muscles (TCAMs). Manuf. Lett. 2022, 33, 19–23. [Google Scholar] [CrossRef]
- Lamuta, C. Perspective on highly twisted artificial muscles. Appl. Phys. Lett. 2023, 122, 040502. [Google Scholar] [CrossRef]
- Giovinco, V.; Kotak, P.; Cichella, V.; Maletta, C.; Lamuta, C. Dynamic model for the tensile actuation of thermally and electro-thermally actuated twisted and coiled artificial muscles (TCAMs). Smart Mater. Struct. 2020, 29, 25004. [Google Scholar] [CrossRef]
- Slutsky, D.J.; Herman, M. Rehabilitation of distal radius fractures: A biomechanical guide. Hand Clin. 2005, 21, 455–468. [Google Scholar] [CrossRef]
- Top Hand Therapy Exercises|Summit Orthopedics. Available online: https://www.summitortho.com/2023/01/17/top-hand-therapy-exercises/ (accessed on 18 January 2023).
- Crisco, J.J.; Heard, W.M.R.; Rich, R.R.; Paller, D.J.; Wolfe, S.W. The mechanical axes of the wrist are oriented obliquely to the anatomical axes. J. Bone Jt. Surg. Am. 2011, 93, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Mann, K.A.; Wernere, F.W.; Palmer, A.K. Frequency spectrum analysis of wrist motion for activities of daily living. J. Orthop. Res. 1989, 7, 304–306. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device Name and Reference | Joints | Actuation | DOFs | Wrist ROM | Weight | Type |
|---|---|---|---|---|---|---|
| Rice Wrist-S (2012) [36] | Series of Revolute Joints | Electric Motors and Cable Systems | Wrist F/E Wrist U/R Forearm P/S | Wrist F/E 120° Wrist U/R 70° | - | Grounded |
| Wrist-Gimbal (2013) [37] | Series of Revolute Joints | Electric Motors and Cable Systems | Wrist F/E Wrist U/R Forearm P/S | Wrist F/E 180° Wrist U/R 60° | - | Grounded |
| Mahi-Exo II (2014) [38] | Revolute–Prismatic–Spherical Joints | Electric Motors and Cable Systems | Wrist F/E Wrist U/R Forearm P/S Elbow F/E Shoulder Ab/Ad | Wrist F/E 65° Wrist U/R 63° | - | Grounded |
| Mahi Open-Wrist (2017) [39] | Series of Revolute Joints | Electric Motors and Cable Systems | Wrist F/E Wrist U/R Forearm P/S | Wrist F/E 135° Wrist U/R 75° | - | Grounded |
| Parallel spherical wrist (2019) [40] | Revolute Joints Spherical Joint | SEA with two Stepper motors | Wrist F/E Wrist U/R Forearm P/S | Wrist F/E Wrist U/R Forearm P/S | 1.5 kg | Grounded |
| POWROBOT (2022) [41] | Passive Revolute Joints | Three-geared DC motors | Wrist F/E Wrist U/R Forearm P/S | Wrist F/E Wrist U/R Forearm P/S | 0.22 kg | Grounded |
| Goncalves et al. (2020) [42] | Single Revolute Joint | One Servo motor | Wrist F/E Wrist U/R Forearm P/S | Wrist F/E Wrist U/R Forearm P/S | 2.75 kg | Grounded |
| PWRR (2020) [43] | 2-Universal Joints | Two Pneumatic actuators | Wrist F/E Wrist U/R | Wrist F/E Wrist U/R | - | Grounded |
| WReD (2018) [44] | Passive 2-Revolute Joints | One DC motor | Wrist F/E Wrist U/R | Wrist F/E Wrist U/R | - | Grounded |
| SEU (2020) [45] | Series of Revolute Joints | Bowden-cables, clutches, DC motor | Wrist F/E Wrist U/R Forearm P/S | Wrist F/E Wrist U/R Forearm P/S | - | Grounded |
| Soft Wrist Assist (SWA) (2019) [46] | - | SMA Coil Spring | Wrist F/E Wrist U/R | O-Wrist F/E 64.2° Wrist U/R 36.9° | 0.151 kg | Ungrounded |
| Soft Parallel Robot (2021) [47] | Soft Universal Joint | 6 PAM and 1 Stepper motor | Wrist F/E Wrist U/R Forearm P/S | Wrist F/E Wrist U/R Forearm P/S | - | Grounded |
| Human Wrist [48] | Wrist | Biological Muscles | Wrist F/E 115° Wrist U/R 70° | - | - |
| Gender | % of Height | % of Weight | Center of Gravity as a % of Height (Along Axis from the Origin) | References | |
|---|---|---|---|---|---|
| Hand | M | 11.00 | 0.65 | 5.75 | [60,61] |
| F | 10.65 | 0.50 | 5.75 | [60,61] | |
| Width | M | 5.11 | - | - | [61] |
| F | 4.80 | - | - | [61] | |
| Circumference | M | 12.10 | - | - | [61] |
| F | 11.42 | - | - | [61] | |
| Forearm | M | 15.70 | 1.87 | 43.00 | [60,61] |
| F | 15.22 | 1.57 | 43.40 | [60,61] |
| Extension/Flexion | ||||||||
|---|---|---|---|---|---|---|---|---|
| Hand NDL Attachment Coordinates as a % of Hand Length | Forearm Muscle Attachment Coordinates as a % of Forearm Length | |||||||
| Coordinate Axis | E1h | E2h | F1h | F2h | E1f | E2f | F1f | F2f |
| x | 16 | −16 | 16 | −16 | 16 | −16 | 16 | −16 |
| y | 16 | 16 | −16 | −16 | 11 | 11 | −11 | −11 |
| z | 16 | 16 | 16 | 16 | −75 | −75 | −75 | −75 |
| Ulnar/Radial Deviation | ||||||||
| Coordinate Axis | U1h | U2h | R1h | R2h | U1f | U2f | R1f | R2f |
| x | −5 | −5 | 5 | 5 | −5 | −5 | 5 | 5 |
| y | 16 | −16 | 16 | −16 | 11 | −11 | 11 | −11 |
| z | 16 | 16 | 16 | 16 | −75 | −75 | −75 | −75 |
| Number of Bundles | Diameter (mm) | Stress (MPa) |
|---|---|---|
| 2B | 0.7 | 18 |
| 4B | 1 | 9 |
| 6B | 1.4 | 5 |
| 8B | 1.8 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Greco, C.; Weerakkody, T.H.; Cichella, V.; Pagnotta, L.; Lamuta, C. Lightweight Bioinspired Exoskeleton for Wrist Rehabilitation Powered by Twisted and Coiled Artificial Muscles. Robotics 2023, 12, 27. https://doi.org/10.3390/robotics12010027
Greco C, Weerakkody TH, Cichella V, Pagnotta L, Lamuta C. Lightweight Bioinspired Exoskeleton for Wrist Rehabilitation Powered by Twisted and Coiled Artificial Muscles. Robotics. 2023; 12(1):27. https://doi.org/10.3390/robotics12010027
Chicago/Turabian StyleGreco, Carlo, Thilina H. Weerakkody, Venanzio Cichella, Leonardo Pagnotta, and Caterina Lamuta. 2023. "Lightweight Bioinspired Exoskeleton for Wrist Rehabilitation Powered by Twisted and Coiled Artificial Muscles" Robotics 12, no. 1: 27. https://doi.org/10.3390/robotics12010027