
What Is Next in Computer-Assisted Spine Surgery? Advances in Image-Guided Robotics and Extended Reality



1
Medical Center of National Defense Forces, 1134 Budapest, Hungary
2
Antal Bejczy Center for Intelligent Robotics, Óbuda University, 1034 Budapest, Hungary
3
Department of Surgical Research and Techniques, Semmelweis University, 1085 Budapest, Hungary
4
University Research and Innovation Center (EKIK), Óbuda University & Austrian Center for Medical Innovation and Technology (ACMIT), 2700 Wiener Neustadt, Austria
*
Author to whom correspondence should be addressed.
Robotics 2023, 12(1), 1; https://doi.org/10.3390/robotics12010001
Submission received: 11 October 2022
/
Revised: 18 November 2022
/
Accepted: 7 December 2022
/
Published: 20 December 2022
(This article belongs to the Special Issue Selected Papers from the 15th International Symposium on Applied Computational Intelligence and Informatics (SACI 2021))
Abstract
:Background: This article provides a scoping review on the current status of Image-Guided Navigation with various forms of digital technologies, including Extended Reality, Augmented Reality Head-Mounted Displays (AR–HMDs) and Robot-Assisted Surgery (RAS) for Pedicle Screw Placement in orthopedics and spine surgery. Methods: A scoping literature review was performed in the PubMed, Scopus, Embase, Web of Science, Google Scholar and IEEE Xplore databases to collect clinical and user satisfaction data on AR–HMDs and compare those with RAS outcomes. In vivo patient, cadaver and phantom trial accuracy data reports were identified and grouped through the analysis. Over the past two years, 14 publications were retrieved and analyzed. Pedicle screw placement accuracy was described with Linear Tip Error (LTE), Angular Trajectory Error (ATE) and Gertzbein–Robbins Scale (GRS) outcomes. Results: The Pedicle Screw Placement accuracy was seen to increase in the in vivo, cadaver and phantom model groups using AR-HMD compared to the Free-Hand insertion technique. User experience and satisfaction data were limited; however, a clear advantage for the operative results was described when it was added. RAS screwing showed similar accuracy outcomes. The need for benchmarking and quantified situation awareness for AR–HMDs is recognizable. The authors present a method for standardized scoring and visualization of surgical navigation technologies, based on measurements of the surgeon (as the end-users) user satisfaction, clinical accuracy and operation time. Conclusions: computer-technology driven support for spine surgery is well-established and efficient for certain procedures. As a more affordable option next to RAS, AR–HMD navigation has reached technological readiness for surgical use. Ergonomics and usability improvements are needed to match the potential of RAS/XR in human surgeries.
1. Introduction
In the past decades, computer technology-driven medical and surgical innovations have transformed modern healthcare. The advancements of medical diagnostic imaging, minimal invasive surgical methods and tools, bio-compatible implants, modern anesthesiology and the new aspects of digital medical technology together proved to be beneficial regarding the overall patient outcomes [1]. The advantages include faster recovery and improved rates of patients reintegration into society and the economy [2].
Spine surgery has also been largely influenced by the technological revolution [3]. Annually, 266 million patients suffer from spinal diseases worldwide, which can significantly degrade their quality of life. Pedicle Screw Placement (PSP) is the most common orthopedic procedure that is widely used for the stabilization of potential (spinal stenosis and degenerative diseases) and existing instabilities (pseudoarthrosis and post-laminectomy syndrome) of the vertebral column, spinal trauma and fractures, tumors and spinal deformities (scoliosis and kyphosis) [4,5].
The main steps of PSP in percutaneous screw fixation begin with the intra-operative posteroanterior and lateral fluoroscopy as image guidance. After planning the entry point of the vertebra, the pedicle entry site is decorticated, and, with the application of a curved or straight pedicle probe, a pathway is pre-formed for the screw through the cancellous bone. The pedicle screws are then inserted with extended tabs. Finally, the contoured fixation rod is inserted into the subfascial layer, and the screws are tightened on the rod (Figure 1A–D) [6].
Free-Hand (FH) vertebral procedures are supported by fluoroscopic image-based navigation, with the aim of precise operation next to the spinal cord. Fluoroscopy is time-consuming, presenting only 2D imaging information, and the surgical staff is exposed to radiation during the scan. Even with this utmost attention, a meta-analysis by Staartjes et al. discussed that 3.3% of FH spine fixation cases needed re-operation due to misplaced screw implantation. The prevention of this would lead to a decrease in patient morbidity and mortality, which could reduce the cost of care by $23,865–32,915 per revision surgery [7,8].
In the past decade, to achieve Minimal Invasive Surgical (MIS) PSP, different Computer-Assisted or Computer-Integrated Surgical (CAS/CIS) approaches were invented: Robot-Assisted Surgery (RAS), Computer-Assisted Navigation or Image-Guided Surgery (IGS) and Neurophysiological Monitoring [9,10,11]. More recently, the development of new spine surgery devices accelerated together with other robotic services, partially due to the complex effects of COVID-19 [12].
Robotic spine surgery systems have been used for PSP since 2004, typically for positioning the screw-guiding tubes for manual insertion [13]. The present PSP robotic systems can be divided into three different groups regarding their control strategies: the robot performs surgical sub-tasks or steps of the procedure autonomously in supervised mode, the robot is remotely controlled by the surgeon and the robot is simultaneously commanded and controlled by the robot and the surgeon [14,15]. The requirements for using RAS include high-quality preoperative imaging data, image–patient registration for navigation purpose (i.e., enabling anatomical landmarks or markers) and, if possible, real-time intra-operative tracking in order to monitor and compensate for additional patient movement [16].
The currently commercially available RAS systems use mechanical, electromagnetic or optical tracking to display patient and surgical tool movements in real-time. Though the cost of an RAS system is high, the studies report better clinical outcomes, more accurate screw insertions, less complication and fewer revision surgeries, shorter operation times and smaller radiation dosages by employing robotic technologies [3,17].
Computer-enhanced surgery provides many updates to the traditional workflow in the Operating Room (OR). Image-Guided Surgery incorporates the intra-operatively most relevant form of Extended Reality (XR): Augmented Reality (AR) for navigation in the field of spine surgery.
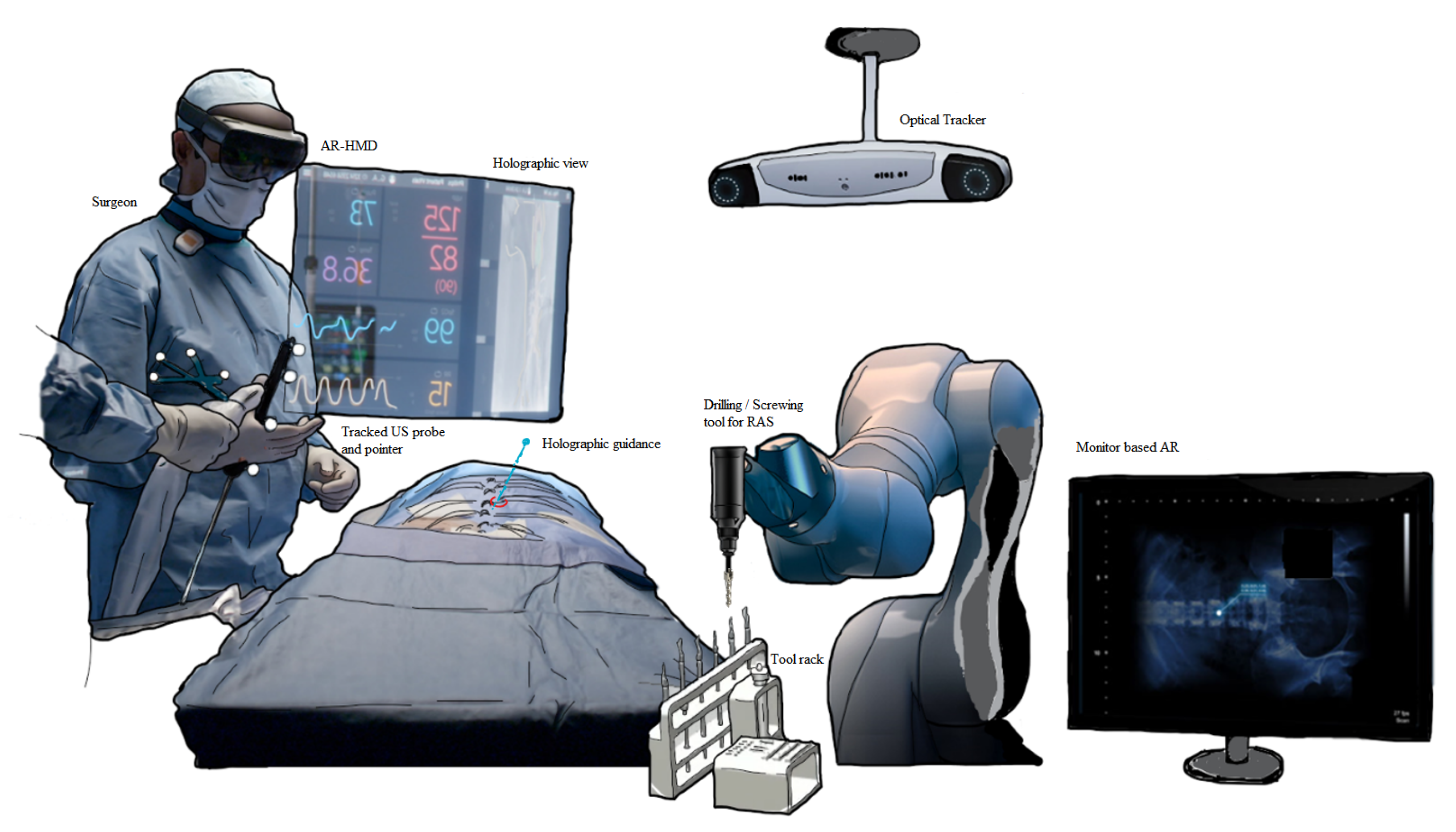
The patients’ preoperative CT/MRI diagnostic images or intra-operative cone-beam CT scans can be segmented automatically or semi-automatically into 3D models through image-computing platforms (e.g., 3D Slicer) [18]. These models can be represented as monitor-based, microscope-based or Head-Mounted Display (HMD) AR holograms. For image–patient registration, trackers are used together with anatomical or artificial landmarks (fiducials) [19]. Merging the two technologies, robotics and AR in surgery can result in additional intra-operative and post-operative benefits, including accuracy and outcomes for patients (Figure 2).
Among the many forms of XR, only a few specific modalities have found ways to test prototypes with the clinical experts.
The main advantage of using a see-through AR–HMD navigation is the ability to project the holographic image into the surgeon’s exact field of view without disrupting the workflow—as this would negatively impact the operation time risking more prolonged anesthesia. The effect of HMDs on the Operation Time (OT), overall radiation dose, PSP accuracy and cost–benefits are not yet clarified as only low number of cases and heterogeneous data were found in the literature. A previous systematic literature review by Bursröm et al., collected 28 studies focusing on AR in spine surgery in 2020 but included a limited number of clinical data sets [23]. The aim of this article was to collect and compare outcomes of robot-assisted Pedicle Screw Placement operations with the most recent experience reported by studies exclusively on AR–HMDs in spine surgery.
2. Materials and Methods
The authors systematically reviewed the recent AR-guided spine surgery scientific articles that were published in 2020–2022. PubMed, Scopus, Embase, Web of Science, Google Scholar and IEEE Xprole databases were used with the keywords of “Augmented Reality” AND “Spine Surgery”.
Inclusion criteria was defined as any article written in English, mentioning AR navigation in spine surgery with case reports and accuracy data included. Human patient, cadaver and phantom model reports were also included in the scope. Any reviews, systematic reviews, conference papers, abstracts, letters, opinions and papers describing educational, telemedicine and teleconsultation use of AR technology were excluded during the search.
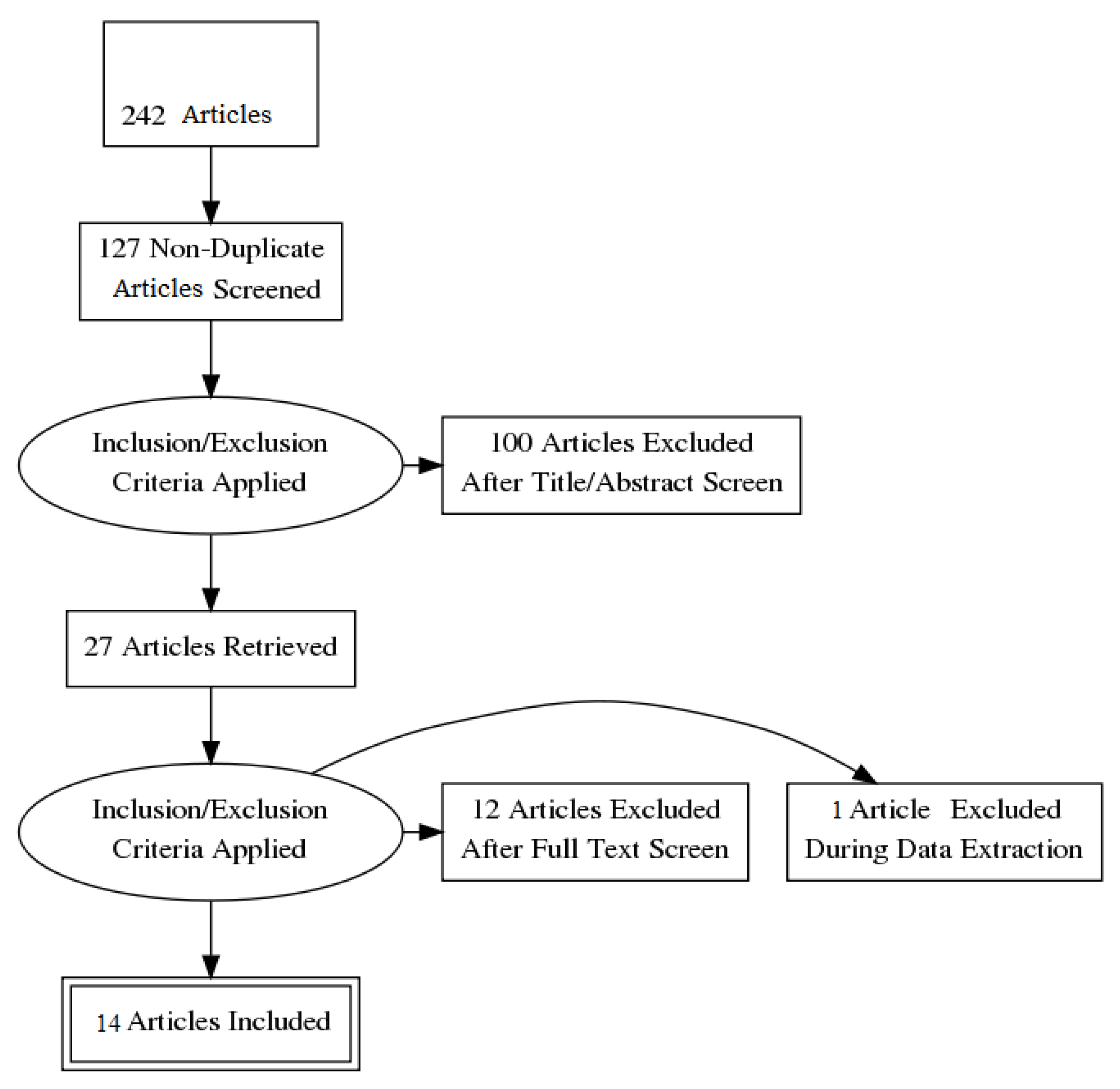
From the publications of the past two years that mentioned AR in spine surgery, 242 articles were retrieved with the keywords of “Augmented Reality” and “Spine Surgery”. With the removal of 115 duplications by Mendeley Desktop, 127 abstracts were screened, resulting in 14 eligible publications for full-text review. Figure 3 contains the PRISMA flow diagram on the search performed [24].
Clinical and procedural data were collected, analyzed and narrated from the retrieved articles as the number of surgical cases, number and accuracy of inserted pedicle screws (Linear Tip Error, Angular Trajectory Error and GRS) and surgical complications. Surgeons’ user experiences, criticisms about HDMs and AR navigation and awareness and patient-reported outcomes [25] were gathered as secondary data, where available.
Previously, the authors reviewed different manufacturers’ AR–HMDs as used in clinical–surgical environments; the derived conclusion was that information is still lacking regarding user situational awareness, and there is a lack of operating-room-specified, standardized production (benchmarking). The experience of end-users is believed to be the key to further AR device development [19].
3. Results
By means of the literature search of AR–HMD-guided spine surgery, 14 publications were reviewed and analyzed, and Table 1 contains the list of reviewed articles with authors and publication dates. Seven papers described the experience on spine surgeries of living human patients (in vivo use), while three articles narrated cadaveric ones and four presented laboratory use phantom models. We collected 154 reported cases from the 14 articles in total: 34 phantom models, 17 cadavers and 103 (103/154, 66.8%) living patients, who underwent the PSP procedure. In these reports, altogether 1189 screws were implanted, 849 (71.4%) of them in living or cadaveric thoracic, lumbar and cervical vertebrae. Overall, 557 (557/1189, 46.8%) screws were inserted into 103 patients.
3.1. Accuracy
PSP accuracy can be measured along intra- and/or post-operative X-ray, fluoroscopy or CT scans with the Linear Tip Error (LTE in mm-s), Angular Trajectory Error (ATE in degrees) and Gertzbein–Robbins Scale. The clinically used GRS classification has five different pedicle screw implantation accuracy levels based on pedicle cortex breaching of the screws [40]:
- A
- in the pedicle of vertebra screw position without breach detected;
- B
- screw exceeding the pedicle cortex is maximum 2 mm;
- C
- screw exceeding the pedicle cortex is 2–4 mm;
- D
- screw exceeding the pedicle cortex is 4–6 mm;
- E
- screw exceeding is more than 6 mm or outside of the pedicle.
Only grades A and B can be considered as satisfactory clinical results, as in the cases C to E, mild-to-severe neurological symptoms could occur during the postoperative period [41].
LTE and ATE were mentioned in only seven in vivo articles:
- LTE: 2.78 mm .
- ATE: 4.85° .
The GRS was more adequate in the living patient group using AR navigation with grades of implantation accuracy from 97.1% to 100% in the case of A and B. No intra- or post-operative surgical complications were described in the living cases, the detected misplaced screws were revised during surgery, and no secondary revision surgery was needed.
The AR–HMD navigated cadaver use case group had average accuracies of:
- LTE: 3.96 mm .
- ATE: 5.02° .
A GR-scale 96–97.5% of A and B, as in the phantom model group, had averages of
- LTE: 1.52 mm .
- ATE: 4.92° .
The 94–98.4% GR A and B scales were published.
3.2. HMDs and Registration
In most of the cases, the implantation of screws was navigated with the use of Microsoft’s HoloLens Mixed Reality glasses [42] and FDA (the U.S. Food and Drug Administration, Silver Spring, MD, USA)-approved xVision AR system from Augmedics [43]. From the reviewed articles, no significant accuracy difference could be found between the two navigation systems (97.5–100% vs. 97.1–100% GRS A–B). For patient–image registration, sterile metal marker fiducials, registration clamps, optical/infra-red reflective markers and electromagnetic sensors were used in the cases presented in the 14 articles. Registration accuracy and location errors were not reported in any cases.
3.3. User Experience of Surgeons
All the authors who added their criticism about AR–HMDs agreed on the advantages and benefits of the operative outcomes while using the technology. In the living patient group increased accuracy and precision were discussed by Molina and Dennler et al., with no attention shift to remote screens and reduction of exposure to radiation [26,29]. Yahanda et al., mentioned the similar or superior accuracy compared with the most commonly used robotic systems too [30]. According to Bhatt et al., the technology is highly effective without a significant learning curve compared to robotic guided systems where accuracy ranges from 97.9% to 100%, thereby, suggesting that AR technology is a compelling alternative [32].
Regarding cadaver experience, Farshad et al. mentioned surgeon satisfaction with AR-based screws and rod navigation was 5.38 ± 0.67 (on the scale of 1 to 6 of their questionnaire, where 6 was the best score) [35]. Using AR navigation on spine phantom models, the user experience corresponded with other groups’ findings, and the published interpolating results showed that patient safety and the outcomes could be increased with this technology [38]. Lowered procedural costs and optimized ergonomics have also been mentioned by certain authors [26,38].
Only a few comments were provided as disadvantages or difficulties with using the HMDs in living patient care. Molina et al., mentioned visual obstruction caused by the translucent data and experienced visual discomfort for one surgeon with the interpupillary distance calibration [26]. Li et al., also perceived visual discomfort and eye strain and visual difficulties in anatomical and spatial judgment [27]. Yahanda et al., mentioned that using AR in surgical procedures creates differences in the clinical workflow, and this should be more easily incorporated [30].
4. Discussion
Comparing this review’s findings of 14 articles of the past two years with the previous systematic literature review by Bursröm et al. shows that the Head-Mounted Augmented Reality navigation technology in spine surgery is slowly spreading, developing and progressing. The heterogeneity of the studies and reported data lead to difficulty in performing a meta-analysis. Not all the reviewed studies contained exact accuracy measurements, causing bias in comparison. As we can see from the tendency in Bursröm’s article, living patient-reported data is still not sufficient, as they reported only two publications using AR–HMD navigated procedures, while monitor-based and microscope AR were and still are the most popular methods [23].
4.1. Accuracy and Clinical Outcomes
From previous articles and reviews, it was clear that using AR navigation increased the Pedicle Screw Placement accuracy compared to the Free-Hand fluoroscopy group’s accuracy. Elmi-Terander et al., found higher accuracy in the AR vs. FH group (AR: 93.9% vs. FH: 89.6%, p < 0.05) and increased GRS in a cadaveric setup (AR: 85% vs. FH: 64%, p < 0.05) [44]. This review’s findings show clear advancement of the AR–HMD accuracy results in living patients, cadaver and phantom model environments with 94% to 100% GRS A and B grades and lower intra-operative screw misplacement and complications as well.
Molina et al. found that prior cadaveric data results were not significantly different from living patient clinical results, that the absence of respiratory motion had self-explanatory a positive bias, that using low-resolution CT-scans decreased the accuracy and that one pixel of difference in the images may correspond 0.5 mm in reality. They found the xVision HMD system to working better than other AR–HMDs and navigation systems, such as StealthStation (Medtronic Public Limited Company, Minneapolis, MN, USA) and ExcelsiusGPS (Globus Medical Inc., Audubon, PA, USA) [26].
In spine surgery, different robot-assisted surgical systems are already in use, for example, the SpineAssist robot, which demonstrated a GRS A or B accuracy of 97.9% for 487 screws placed in 112 patients [45]. Constant advancement and upgrades of SpineAssist increased the accuracy rate up to 99% [46].
The ExcelsiusGPS system has shown GRS A–B between 96.6% and 100% in several studies [47,48]. A recent systematic literature review on the topic of spine robotic surgery by IB Lopez et al. [49] included the findings of 74 studies, where the evaluation clearly discusses the superiority of accurate screw trajectory by robots of up to 94–98% GRS A–B compared to the FH technique. In revision surgery, PSP was shown to be more accurate than FH insertion (98.5 vs. 96.9%) with a lower number of superior facet joint violations (6.4 vs. 24.4%) [50].
A significant reduction of operation and screw insertion time was experienced using robotic systems compared to FH ones (a mean time of 90 s/screw, overall 5.58 ± 1.22 min vs. 7.25 ± 0.84 min, p < 0.001) [51]. Intra-operative blood loss and transfusion decreased according to a recent meta-analysis [52], and rarely occurring post-operative complications were published [53]. According to a recent cost-analysis report, despite the higher application costs, robotic surgery systems appear to be more cost-effective as a long-term strategy due to the shorter operation time, decreased need for revision surgery, lower infection rate and reduced length of hospital-stays [17,54].
As the cost of an AR–HMD system is significantly less than that of a robot-assisted spine surgical system [3] and their implantation accuracy and clinical outcomes are similar, the AR–HMD system appears to be a good alternative in spine surgery for countries with lower incomes or in the case of limited accessibility to robotic systems [55]. Yanni highlighted the ultimate lowering of procedural cost using AR–HMD navigation [38]. Nevertheless, no studies have been presented on any detailed cost–benefit analysis until now.
4.2. Patient–Image Registration and Surgical Workflow
In the literature, several patient–image registration techniques can be found relying on intra-operative tracker data [56,57,58]. The two main modalities are the optical and electromagnetic trackers [59,60]. Most optical tracking systems use RGB cameras to capture movements from the reflected infra red light, as they are in the field of view. Optical references can be natural anatomic landmarks or artificial reflective markers (fiducials) attached to the patient’s skin and on surgical instruments and tools. Electromagnetic navigation has the advantage that maintaining the line of sight is not required for precise tracking; however, metals and other electric instruments used in OR can distort the magnetic field and, thus, diminish the accuracy of tracked tool [61].
Surgical workflow can be positively affected by the use of Head-Mounted Augmented Reality navigation [30]. Studies reported a slight increase in the operation time, as more work was needed for patient–image registration. Urakov and Bhatt et al. mentioned more effective and shorter learning curves using AR navigation [32,39].
Lowering the radiation dose affecting patients and medical staff has been reported by several studies; however, only Bhatt et al. added exact data, where the mean total fluoroscopy time (s) was 25.7 ± 29.8, and the mean total fluoroscopy dose was 0.3 ± 0.4 mGy/cm2 for their 19 out of 27 patients. The mean total 3D imaging dose was 576.8 ± 368.8 mGy/cm to place screws using AR-navigation for 27 patients [32].
The previous systematic literature review by Burström et al., presented sporadic data about the decrease of radiation dose: one study reported a significantly lower fluoroscopy dose-area and time with the use of AR–HMD (182.6 ± 106.7 mGy/cm2 vs. FH: 367.8 ± 184.7 mGy/cm2 and 5.2 ± 2.6 s vs. FH: 10.4 ± 4.1 s). Regarding their findings, for patient registration, the effective mean dose of intra-operative CT or cone-beam CT was 0.22 ± 0.16 mSv (cervical) and 15.8 ± 1.8 mSv (thoracolumbar) [23].
In the case of RAS spine procedures, a faster learning curve was observed by IB Lopez et al., with significant elevation of accuracy and decreased operating time following 10 to 30 cases. They reported 80% less “per screw” and 78.3% “overall” radiation reduction for patients and the surgical staff during the procedure, compared to the standard FH fluoroscopy-guided technique [49]. Using Mazor Renaissance and the ROSA robotic systems, the same overall results were found [62]. In their recent systematic literature review, Luengo-Matos et al. described a lower radiation dose requirement for RAS compared with FS, based on their findings from four studies [63].
4.3. Ergonomics and Further Perspectives
From the 14 reviewed articles, some of the authors added user experience about the employed AR–HMD system, regarding ergonomics and comfort. Molina mentioned that using the device added no mechanical discomfort during short time uses, with approximately 800 g of weight, and, with the glasses, there was no need to look at the remote screen; however, he also discussed some visual discomfort and obstruction caused by translucent data [26]. Yanni et al., found that the ergonomics of using the headset was not yet optimized for the surgical suite [38].
As feedback is not yet widely provided by authors regarding the employed AR–HMD systems, further improvements and device developments cannot yet be accurately specified and standardized for OR use. More detailed experiences from the surgeons as end-users are still needed, which could be the key to achieving this specific AR–HMD development [19]. Some examples can be found as user scoring systems for AR systems, measuring how easy and accessible the use of the device is, about their complexity, or if any support was needed through their use, scoring the interface and confidentiality during use, etc. [64].
4.3.1. User Satisfaction Score
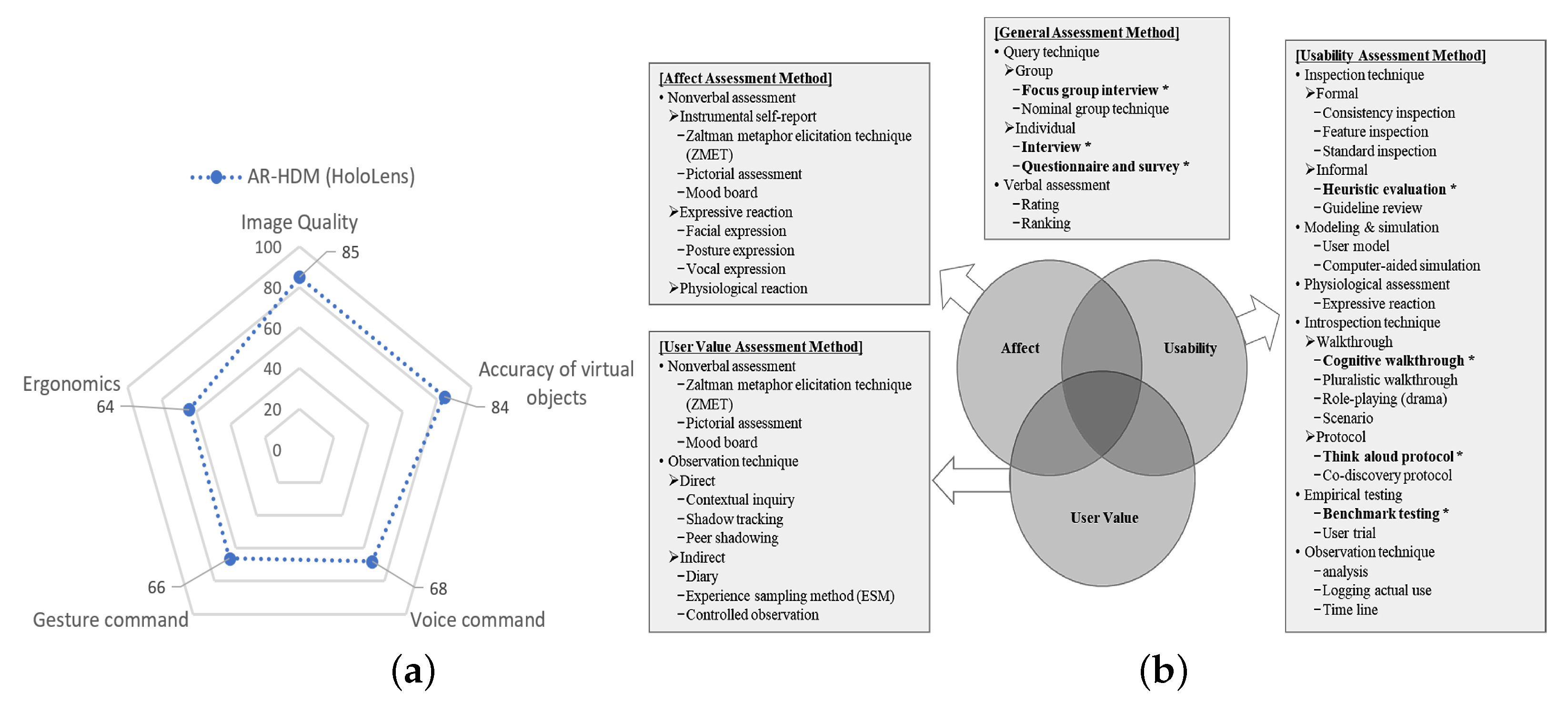
As end-users, surgeons should provide reliable and standardized feedback about the experience on AR–HMDs that they use through clinical procedures. Collecting these data would help in systematically evaluating these valuable responses for the manufacturers to improve and upgrade their devices. In this review, only one published paper [29] shared their results concerning a standardized 58-item electronic survey questionnaire using the REDCap data capture tool. Their survey based on a 100-point scale with anchor statements (1: not useful at all, to 100: very useful), asking about the usability of the AR technology and the device. The overall satisfaction with the application of AR technology in spine surgery was described (78 ± 20 points), and future access was demanded (75 ± 22 points). The main valued aspect can be seen in Figure 4 [29].
A recent overview by Bitkina et al. collected the current qualitative and quantitative evaluation possibilities of the usability and user experience of medical devices [65]. Other User Satisfaction Scoring systems can be found, such as the Questionnaire for User Interaction Satisfaction (QUIS) tool—which was designed to score human–computer interfaces (regarding the screen, system feedback, learning curve, technical capabilities and manuals, tutorials and multimedia use) [66] and the Smart Glasses User Satisfaction (SGUS) questionnaire (regarding the AR perception, interaction, location and object awareness and AR content) [67]. Specific evaluation tools for intra-operatively used AR–HMDs have not been published yet. The above-mentioned tools are only sporadically used and seem not to be well-known in the surgical practice. These should be modified for specific targets, highlighting the importance of a standardized methodology for scoring different aspects of AR–HMDs, similar to robots [68].
From the perspective of the surgeon, the modified scoring tool needs to involve the following:
- Ergonomics: Weight and comfort in wearing the device for short- (<60 min) and long-term (>60 min) use. Overheating the device, sweating or humidity could present as distracting factors.
- Field of View (FoV): Both the size and the angular position of the FoV need to be matched to the surgical procedure.
- Image Quality, Accuracy and Immersion: Clear, accurate and contrasted visibility of AR elements on the transparent display, without disturbing the surgical field.
- Control: Precision and accuracy of the gaze/motion/voice commands of the device.
- Usability and Setup: Experience in understanding and using the HMD interface through starting up, image–patient registration and navigation.
- A future-proof application and overall satisfaction levels.
4.3.2. Technical Requirements and Benchmarking
According to the recent literature, a generally deployable, universal OR-specific and proven AR headset has not yet been marketed [19]. One of the main required characteristics of an HMD would be its easy and time-efficient integration into the surgical workflow. As the surgeons would not necessarily have an IT or computing background and relevant skills, there will be no staff qualified for these tasks, and thus the system’s calibration and patient–image registration need to be adequate for the situation. On the other hand, additional health-economy investigations are needed to provide evidence of the benefits of the presumably longer operation times using AR navigation.
Precise and accurate overlay, localization in the 3D space of the projected image, the contrast and quality of holograms and immersion are indisputable key factors for a device’s success. Wearing and using AR–HMDs for longer operations are likely to happen, which highlights the importance of ergonomics and the weight distribution of the device [65]. As the surgeon’s head and FoV are usually pointing downwards to the working area (operation field), an adjustable, personally aligned and balanced device could only prevent short-term exhaustion and fatigue of the user.
In conclusion, we gathered the Benchmarking requirements of an ideal surgery-specified AR–HMD grouping in two levels [19]:
- Essential Requirements:
- –
- Wide Field of View, humidity-free see-through display with dust, water and droplet resistance (IP65).
- –
- Built-in-one computer with a high-computing capacity.
- –
- Wireless connection.
- –
- Long battery life.
- –
- Easy, understandable user interface.
- –
- Support for setup, registration and calibration.
- –
- Ergonomics and balanced weight under 400 g.
- –
- Touchless and controller-free navigation with gaze/motion/voice commands.
- Additional Requirements:
- –
- Automatic focus adjusting to pupils;
- –
- Image, video and audio capturing, streaming.
- –
- Haptic/vibration feedback.
- –
- Environmental and/or situational awareness monitoring.
4.3.3. Situation Awareness
Using an AR–HMD would help in navigation and guidance for the surgeons with projected holograms in giving additional spatial and depth knowledge on the operation region and field. As this function works passively, as with using a map with computer vision and pattern recognition, deep learning would lead to different levels of advanced environmental and situational awareness, which could reform surgery by identifying objects, calling for attention to adverse events and giving additional recommendations on the next surgical steps and approaches [69]. Understandably, while maintaining a high focus on certain surgical steps and situations, the peripheral awareness and attention of the surgeon may drop.
In the case of adverse events, such as bleeding or surgical clip misplacement, a discrete, not intrusive alarming sound/visual signal could help with the identification and localization of the problem. Virtual labels added to certain vessels, ducts or tissue structures could prevent unintentional injuries [70]. The holographic guidance of certain surgical steps, such as an incision or skin closure and suturing may help in achieving better wound-healing outcomes with less deformation and scars. Through the evolution of deep-learning and computer-vision algorithms, further environmental and situational awareness could be achieved in surgery [71].
4.3.4. Standardized Scoring and Visualization Method for Surgical Navigation and Guidance Devices
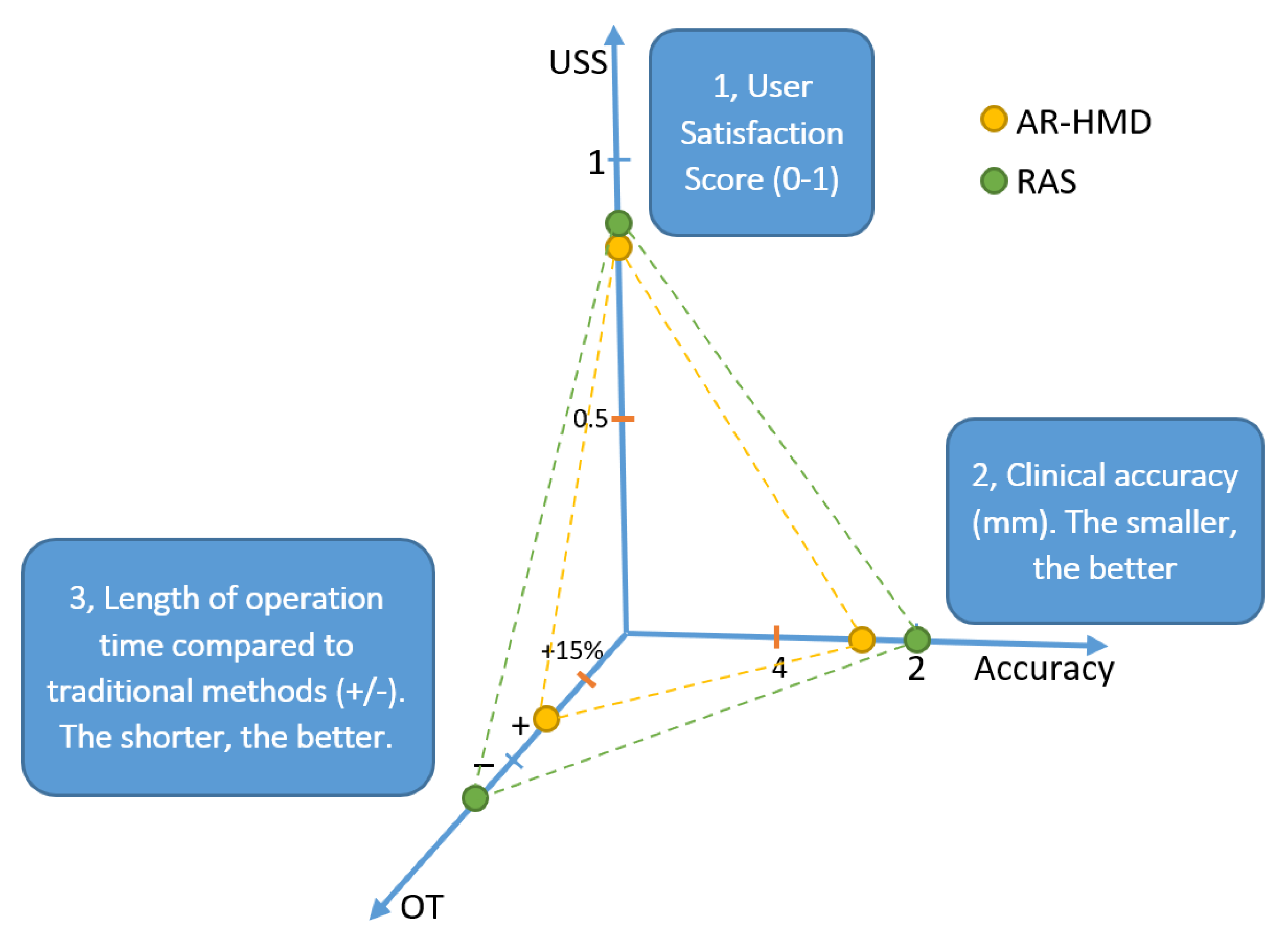
Surgical navigation and guidance technologies can be described as fulfilling technical, functional and clinical requirements. Collecting, reviewing and representing all the main attribution data through a standardized methodology could give valuable information regarding AR–HMD and RAS for the end-users. The authors implemented their visualization method using a 3D plot, where the larger triangle area indicates better overall performance in the surgical environment (Figure 5).
From a clinical perspective, navigation accuracy is one of the most important factors. The acceptable accuracy boundary and error should be lower than 4 mm but, more preferably, under 2 mm, as higher inaccuracy could cause serious organ, tissue and body structure damage, thereby, leading to complications.
Measures of feasibility and user satisfaction as standardized scores or indexes must be presented as these data contain information about the devices’ ergonomics, immersion, control and interface usability. Lastly, the effect of the devices on the procedure or OT is an important factor for end-users concerning the newly implemented technology. We decided to present this as a decrease (−) or an increase (+) in the OT compared to conventional surgical approaches. A +15 % of cut-off time-value (minutes) was applied if the procedure took longer using any of the devices, as this could also be disadvantageous to patient care (e.g., longer anesthesia involves a higher risk of complications).
5. Conclusions
The benefits of CAS/CIS systems and Augmented Reality Head-Mounted Displays in the field of spine surgery can be recognized in the cases presented in the recent literature. The collected and reviewed accuracy data of AR–HMDs from the past two years did not show significant differences compared to RAS, and the AR-navigated PSP accuracy did not differ from phantom models, cadaver experiments and in vivo patients. As the more expensive FDA-approved robotic systems have been spreading, the cheaper, yet accurate alternative AR–HMD navigation systems seem to have reached their technological readiness level for wider adoption in living patient care in spine surgery.
The relatively slow spread of AR–HMD technology in surgery has two main reasons, ergonomics and hardware, which lead to difficulties with, e.g., the registration and navigation setup. Advancement and development in both fields could lead to the increased adoption of this technology in surgeries. Using standardized scoring and value visualization methods, the end-users could better understand the overall advantages and disadvantages of a certain type of guidance technology and different devices [72]. Merging AR–HMD and RAS technologies could beneficially impact operation outcomes too.
Our future work will include the evaluation of an advanced set of use cases and the examination of large population cohort studies that publish standardized accuracy and clinical data. This could lead to a low-bias meta-analysis that highlights and fortifies the AR navigation’s advantages concerning patient’s care and safety.
Funding
This work was partially supported by the ACMIT (Austrian Center for Medical Innovation and Technology), which is funded within the scope of the COMET (Competence Centers for Excellent Technologies) program of the Austrian Government. The research was partially performed as part of project no. 2019-1.3.1-KK-2019-00007 which has been implemented with the support provided by the National Research, Development and Innovation Fund of Hungary, financed under the 2019-1.3.1-KK funding scheme. T. Haidegger is supported under the Horizon2020-2017-RISE-777911 project framework.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author (KM), upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AR | Augmented Reality |
| ATE | Angular Trajectory Error |
| CAS/CIS | Computer-Assisted/Integrated Surgery |
| FDA | U.S. Food and Drug Administration |
| FH | Free-Handed (vertebral procedure) |
| GRS | Gertzbein–Robbins Scale |
| HMD | Head-Mounted Display |
| IGS | Image-Guided Surgery |
| LTE | Linear Tip Error |
| MR | Mixed Reality |
| OT | Operating Time |
| PSP | Pedicle Screw Placement |
| RAS | Robot-Assisted Surgery |
| XR | Extended Reality |
References
- Taylor, R.H.; Simaan, N.; Menciassi, A.; Yang, G.Z. Surgical robotics and computer-integrated interventional medicine. Proc. IEEE 2022, 110, 823–834. [Google Scholar] [CrossRef]
- Georgiou, K.E.; Georgiou, E.; Satava, R.M. 5G Use in Healthcare: The Future is Present. JSLS J. Soc. Laparosc. Robot. Surg. 2021, 25, e2021.00064. [Google Scholar] [CrossRef] [PubMed]
- Fichtinger, G.; Troccaz, J.; Haidegger, T. Image-guided interventional robotics: Lost in translation? Proc. IEEE 2022, 110, 932–950. [Google Scholar] [CrossRef]
- Ravindra, V.M.; Senglaub, S.S.; Rattani, A.; Dewan, M.C.; Härtl, R.; Bisson, E.; Park, K.B.; Shrime, M.G. Degenerative lumbar spine disease: Estimating global incidence and worldwide volume. Glob. Spine J. 2018, 8, 784–794. [Google Scholar] [CrossRef] [Green Version]
- Deepak Awasthi, M.; Najeeb Thomas, M. Pedicle Screw Placement. Available online: https://www.medschool.lsuhsc.edu/neurosurgery/nervecenter/tlscrew.html (accessed on 2 November 2022).
- Dahdaleh, N.S.; Smith, Z.A.; Hitchon, P.W. Percutaneous pedicle screw fixation for thoracolumbar fractures. Neurosurg. Clin. 2014, 25, 337–346. [Google Scholar] [CrossRef]
- Staartjes, V.E.; Klukowska, A.M.; Schröder, M.L. Pedicle screw revision in robot-guided, navigated, and freehand thoracolumbar instrumentation: A systematic review and meta-analysis. World Neurosurg. 2018, 116, 433–443. [Google Scholar] [CrossRef]
- Adogwa, O.; Parker, S.L.; Shau, D.; Mendelhall, S.K.; Aaronson, O.; Cheng, J.; Devin, C.J.; McGirt, M.J. Cost per quality-adjusted life year gained of revision fusion for lumbar pseudoarthrosis: Defining the value of surgery. Clin. Spine Surg. 2015, 28, 101–105. [Google Scholar] [CrossRef]
- Amato, V.; Giannachi, L.; Irace, C.; Corona, C. Accuracy of pedicle screw placement in the lumbosacral spine using conventional technique: Computed tomography postoperative assessment in 102 consecutive patients. J. Neurosurg. Spine 2010, 12, 306–313. [Google Scholar] [CrossRef]
- Du, J.P.; Fan, Y.; Wu, Q.N.; Zhang, J.; Hao, D.J. Accuracy of pedicle screw insertion among 3 image-guided navigation systems: Systematic review and meta-analysis. World Neurosurg. 2018, 109, 24–30. [Google Scholar] [CrossRef]
- Siller, S.; Raith, C.; Zausinger, S.; Tonn, J.C.; Szelenyi, A. Indication and technical implementation of the intraoperative neurophysiological monitoring during spine surgeries—A transnational survey in the German-speaking countries. Acta Neurochir. 2019, 161, 1865–1875. [Google Scholar] [CrossRef]
- Khamis, A.; Meng, J.; Wang, J.; Azar, A.T.; Prestes, E.; Takács, Á.; Rudas, I.J.; Haidegger, T. Robotics and intelligent systems against a pandemic. Acta Polytech. Hung. 2021, 18, 13–35. [Google Scholar] [CrossRef]
- Smith, A.D.; Chapin, J.; Birinyi, P.V.; Bhagvath, P.V.; Hall, A.F. Automated polyaxial screw placement using a commercial-robot-based, image-guided spine surgery system. IEEE Trans. Med. Robot. Bionics 2020, 3, 74–84. [Google Scholar] [CrossRef]
- Overley, S.C.; Cho, S.K.; Mehta, A.I.; Arnold, P.M. Navigation and robotics in spinal surgery: Where are we now? Neurosurgery 2017, 80, S86–S99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haidegger, T. Autonomy for surgical robots: Concepts and paradigms. IEEE Trans. Med. Robot. Bionics 2019, 1, 65–76. [Google Scholar] [CrossRef]
- Haidegger, T. Probabilistic Method to Improve the Accuracy of Computer-Integrated Surgical Systems. Acta Polytech. Hung. 2019, 16, 119–140. [Google Scholar] [CrossRef]
- Menger, R.P.; Savardekar, A.R.; Farokhi, F.; Sin, A. A cost-effectiveness analysis of the integration of robotic spine technology in spine surgery. Neurospine 2018, 15, 216. [Google Scholar] [CrossRef]
- 3D Slicer Image Computing Platform. Available online: https://https://www.slicer.org/ (accessed on 9 September 2022).
- Móga, K.; Boesl, D.B.; Haidegger, T. Augmented/Mixed Reality Technologies Supporting Digital Surgery. In Proceedings of the IEEE 19th International Symposium on Intelligent Systems and Informatics (SISY), Subotica, Serbia, 16–18 September 2021; IEEE: Piscataway, NJ, USA, 2021; pp. 183–189. [Google Scholar]
- Microsoft HoloLens 2. Available online: https://www.microsoft.com/en-us/hololens/industry-healthcare (accessed on 22 August 2022).
- Philips Showcases Unique Augmented Reality Concept for Image-Guided Minimally Invasive Therapies Developed with Microsoft. Available online: https://www.philips.com/a-w/about/news/archive/standard/news/press/2019/20190224-philips-showcases-unique-augmented-reality-concept-for-image-guided-minimally-invasive-therapies-developed-with-microsoft.html (accessed on 22 September 2022).
- NDI Navigate New Possibilities. Available online: https://www.ndigital.com/ (accessed on 22 September 2022).
- Burström, G.; Persson, O.; Edström, E.; Elmi-Terander, A. Augmented reality navigation in spine surgery: A systematic review. Acta Neurochir. 2021, 163, 843–852. [Google Scholar] [CrossRef]
- PRISMA. PRISMA Statement. Available online: http://www.prisma-statement.org/PRISMAStatement/ (accessed on 22 June 2022).
- Motahari-Nezhad, H.; Fgaier, M.; Péntek, M.; Gulácsi, L.; Zrubka, Z. Populations, Interventions, and Outcomes in Digital Biomarker-Based Interventions’ Systematic Reviews: A Scoping Review. Value Health 2022, 25, S534. [Google Scholar] [CrossRef]
- Molina, C.A.; Sciubba, D.M.; Greenberg, J.K.; Khan, M.; Witham, T. Clinical accuracy, technical precision, and workflow of the first in human use of an augmented-reality head-mounted display stereotactic navigation system for spine surgery. Oper. Neurosurg. 2021, 20, 300–309. [Google Scholar] [CrossRef]
- Li, J.; Zhang, H.; Li, Q.; Yu, S.; Chen, W.; Wan, S.; Chen, D.; Liu, R.; Ding, F. Treating lumbar fracture using the mixed reality technique. BioMed Res. Int. 2021, 2021, 6620746. [Google Scholar] [CrossRef]
- Liu, A.; Jin, Y.; Cottrill, E.; Khan, M.; Westbroek, E.; Ehresman, J.; Pennington, Z.; Lo, L.S.-f.; Sciubba, D.M.; Molina, C.A.; et al. Clinical accuracy and initial experience with augmented reality–assisted pedicle screw placement: The first 205 screws. J. Neurosurg. Spine 2021, 36, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Dennler, C.; Bauer, D.E.; Scheibler, A.G.; Spirig, J.; Götschi, T.; Fürnstahl, P.; Farshad, M. Augmented reality in the operating room: A clinical feasibility study. BMC Musculoskelet. Disord. 2021, 22, 451. [Google Scholar] [CrossRef] [PubMed]
- Yahanda, A.T.; Moore, E.; Ray, W.Z.; Pennicooke, B.; Jennings, J.W.; Molina, C.A. First in-human report of the clinical accuracy of thoracolumbar percutaneous pedicle screw placement using augmented reality guidance. Neurosurg. Focus 2021, 51, E10. [Google Scholar] [CrossRef] [PubMed]
- Farshad, M.; Fürnstahl, P.; Spirig, J.M. First in man in situ augmented reality pedicle screw navigation. N. Am. Spine Soc. J. (NASSJ) 2021, 6, 100065. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, F.R.; Orosz, L.D.; Tewari, A.; Boyd, D.; Roy, R.; Good, C.R.; Schuler, T.C.; Haines, C.M.; Jazini, E. Augmented Reality-Assisted Spine Surgery: An Early Experience Demonstrating Safety and Accuracy with 218 Screws. Glob. Spine J. 2022, 21925682211069321. [Google Scholar] [CrossRef]
- Felix, B.; Kalatar, S.B.; Moatz, B.; Hofstetter, C.; Karsy, M.; Parr, R.; Gibby, W. Augmented Reality Spine Surgery Navigation: Increasing Pedicle Screw Insertion Accuracy for Both Open and Minimally Invasive Spine Surgeries. Spine 2022, 47, 865–872. [Google Scholar] [CrossRef]
- Spirig, J.M.; Roner, S.; Liebmann, F.; Fürnstahl, P.; Farshad, M. Augmented reality-navigated pedicle screw placement: A cadaveric pilot study. Eur. Spine J. 2021, 30, 3731–3737. [Google Scholar] [CrossRef]
- Farshad, M.; Spirig, J.M.; Suter, D.; Hoch, A.; Burkhard, M.D.; Liebmann, F.; Farshad-Amacker, N.A.; Fürnstahl, P. Operator independent reliability of direct augmented reality navigated pedicle screw placement and rod bending. N. Am. Spine Soc. J. (NASSJ) 2021, 8, 100084. [Google Scholar] [CrossRef]
- Dennler, C.; Safa, N.A.; Bauer, D.E.; Wanivenhaus, F.; Liebmann, F.; Götschi, T.; Farshad, M. Augmented Reality Navigated Sacral-Alar-Iliac Screw Insertion. Int. J. Spine Surg. 2021, 15, 161–168. [Google Scholar] [CrossRef]
- Frisk, H.; Lindqvist, E.; Persson, O.; Weinzierl, J.; Bruetzel, L.K.; Cewe, P.; Burström, G.; Edström, E.; Elmi-Terander, A. Feasibility and accuracy of thoracolumbar pedicle screw placement using an augmented reality head mounted device. Sensors 2022, 22, 522. [Google Scholar] [CrossRef]
- Yanni, D.S.; Ozgur, B.M.; Louis, R.G.; Shekhtman, Y.; Iyer, R.R.; Boddapati, V.; Iyer, A.; Patel, P.D.; Jani, R.; Cummock, M.; et al. Real-time navigation guidance with intraoperative CT imaging for pedicle screw placement using an augmented reality head-mounted display: A proof-of-concept study. Neurosurg. Focus 2021, 51, E11. [Google Scholar] [CrossRef] [PubMed]
- Urakov, T.M. Augmented reality-assisted pedicle instrumentation: Versatility across major instrumentation sets. Spine 2020, 45, E1622–E1626. [Google Scholar] [CrossRef] [PubMed]
- Gertzbein, S.D.; Robbins, S.E. Accuracy of pedicular screw placement in vivo. Spine 1990, 15, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.N.; Fan, Y.; Hao, D.J. Risk factors for robot-assisted spinal pedicle screw malposition. Sci. Rep. 2019, 9, 3025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Microsoft. Hololens. Available online: https://www.microsoft.com/en-us/hololens (accessed on 13 July 2022).
- Augmedics. xVision. Available online: https://augmedics.com/ (accessed on 13 July 2022).
- Elmi-Terander, A.; Burström, G.; Nachabé, R.; Fagerlund, M.; Ståhl, F.; Charalampidis, A.; Edström, E.; Gerdhem, P. Augmented reality navigation with intraoperative 3D imaging vs fluoroscopy-assisted free-hand surgery for spine fixation surgery: A matched-control study comparing accuracy. Sci. Rep. 2020, 10, 707. [Google Scholar] [CrossRef] [Green Version]
- Hoeckelmann, M.; Rudas, I.J.; Fiorini, P.; Kirchner, F.; Haidegger, T. Current capabilities and development potential in surgical robotics. Int. J. Adv. Robot. Syst. 2015, 12, 61. [Google Scholar] [CrossRef] [Green Version]
- Van Dijk, J.D.; van den Ende, R.P.; Stramigioli, S.; Köchling, M.; Höss, N. Clinical pedicle screw accuracy and deviation from planning in robot-guided spine surgery: Robot-guided pedicle screw accuracy. Spine 2015, 40, E986–E991. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Meyers, J.E.; Siasios, I.; Pollina, J. Next-generation robotic spine surgery: First report on feasibility, safety, and learning curve. Oper. Neurosurg. 2019, 17, 61–69. [Google Scholar] [CrossRef]
- Jiang, B.; Pennington, Z.; Zhu, A.; Matsoukas, S.; Ahmed, A.K.; Ehresman, J.; Mahapatra, S.; Cottrill, E.; Sheppell, H.; Manbachi, A.; et al. Three-dimensional assessment of robot-assisted pedicle screw placement accuracy and instrumentation reliability based on a preplanned trajectory. J. Neurosurg. Spine 2020, 33, 519–528. [Google Scholar] [CrossRef]
- Lopez, I.; Benzakour, A.; Mavrogenis, A.; Benzakour, T.; Ahmad, A.; Lemée, J. Robotics in spine surgery: Systematic review of literature. Int. Orthop. 2022, 1–10. [Google Scholar] [CrossRef]
- Zhang, J.N.; Fan, Y.; He, X.; Liu, T.J.; Hao, D.J. Comparison of robot-assisted and freehand pedicle screw placement for lumbar revision surgery. Int. Orthop. 2021, 45, 1531–1538. [Google Scholar] [CrossRef]
- Yson, S.C.; Sembrano, J.N.; Sanders, P.C.; Santos, E.R.G.; Ledonio, C.G.T.; Polly, D.W., Jr. Comparison of cranial facet joint violation rates between open and percutaneous pedicle screw placement using intraoperative 3-D CT (O-arm) computer navigation. Spine 2013, 38, E251–E258. [Google Scholar] [CrossRef]
- Tovar, M.A.; Dowlati, E.; Zhao, D.Y.; Khan, Z.; Pasko, K.B.; Sandhu, F.A.; Voyadzis, J.M. Robot-assisted and augmented reality–assisted spinal instrumentation: A systematic review and meta-analysis of screw accuracy and outcomes over the last decade. J. Neurosurg. Spine 2022, 37, 299–314. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.J.; Zhou, L.P.; Zhang, H.Q.; Ge, P.; Jia, C.Y.; Shen, C.L. Rates and risk factors of intrapedicular accuracy and cranial facet joint violation among robot-assisted, fluoroscopy-guided percutaneous, and freehand techniques in pedicle screw fixation of thoracolumbar fractures: A comparative cohort study. BMC Surg. 2022, 22, 52. [Google Scholar] [CrossRef] [PubMed]
- Garcia, D.; Akinduro, O.O.; De Biase, G.; Sousa-Pinto, B.; Jerreld, D.J.; Dholakia, R.; Borah, B.; Nottmeier, E.; Deen, H.G.; Fox, W.C.; et al. Robotic-assisted vs. nonrobotic-assisted minimally invasive transforaminal lumbar interbody fusion: A cost-utility analysis. Neurosurgery 2022, 90, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Takács, B.; Haidegger, T. Fasttracking Technology Transfer in Medical Robotics. In Proceedings of the 2021 IEEE 21st International Symposium on Computational Intelligence and Informatics (CINTI), Budapest, Hungary, 18–20 November 2021; pp. 61–66. [Google Scholar]
- Malham, G.M.; Munday, N.R. Comparison of novel machine vision spinal image guidance system with existing 3D fluoroscopy-based navigation system: A randomized prospective study. Spine J. 2022, 22, 561–569. [Google Scholar] [CrossRef]
- Ahmad, H.S.; Yoon, J.W. Intra-operative wearable visualization in spine surgery: Past, present, and future. J. Spine Surg. 2022, 8, 132. [Google Scholar] [CrossRef] [PubMed]
- Tu, P.; Qin, C.; Guo, Y.; Li, D.; Lungu, A.J.; Wang, H.; Chen, X. Ultrasound image guided and mixed reality-based surgical system with real-time soft tissue deformation computing for robotic cervical pedicle screw placement. IEEE Trans. Biomed. Eng. 2022, 69, 2593–2603. [Google Scholar] [CrossRef]
- Xu, D.-r.; Luan, L.-r.; Ma, X.-x.; Cong, Z.-c.; Zhou, C.-l. Comparison of electromagnetic and optical navigation assisted Endo-TLIF in the treatment of lumbar spondylolisthesis. BMC Musculoskelet. Disord. 2022, 23, 522. [Google Scholar] [CrossRef]
- Franz, A.M.; Haidegger, T.; Birkfellner, W.; Cleary, K.; Peters, T.M.; Maier-Hein, L. Electromagnetic tracking in medicine—A review of technology, validation, and applications. IEEE Trans. Med Imaging 2014, 33, 1702–1725. [Google Scholar] [CrossRef]
- Sirokai, B.; Kiss, M.; Kovács, L.; Benyó, B.I.; Benyó, Z.; Haidegger, T. Best Practices in Electromagnetic Tracking System Assessment. 2012. Available online: https://repozitorium.omikk.bme.hu/bitstream/handle/10890/4783/137019.pdf?sequence=1 (accessed on 22 August 2022).
- Vasan, N.; Scherman, D.B.; Kam, A. A tale of two robots: Operating times and learning curves in robot-assisted lumbar fusion. J. Clin. Neurosci. 2022, 97, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Luengo-Matos, S.; Sánchez-Gómez, L.M.; Hijas-Gómez, A.I.; García-Carpintero, E.E.; Ballesteros-Massó, R.; Polo-deSantos, M. Efficacy and safety of robotic spine surgery: Systematic review and meta-analysis. J. Orthop. Traumatol. 2022, 23, 49. [Google Scholar] [CrossRef] [PubMed]
- Cofano, F.; Di Perna, G.; Bozzaro, M.; Longo, A.; Marengo, N.; Zenga, F.; Zullo, N.; Cavalieri, M.; Damiani, L.; Boges, D.J.; et al. Augmented reality in medical practice: From spine surgery to remote assistance. Front. Surg. 2021, 8, 657901. [Google Scholar] [CrossRef] [PubMed]
- Bitkina, O.V.; Kim, H.K.; Park, J. Usability and user experience of medical devices: An overview of the current state, analysis methodologies, and future challenges. Int. J. Ind. Ergon. 2020, 76, 102932. [Google Scholar] [CrossRef]
- Questionnaire for User Interaction Satisfaction (QUIS). Available online: https://www.umventures.org/technologies/quis%E2%84%A2-questionnaire-user-interaction-satisfaction-0 (accessed on 22 August 2022).
- Olsson, T. Concepts and subjective measures for evaluating user experience of mobile augmented reality services. In Human Factors in Augmented Reality Environments; Springer: Berlin/Heidelberg, Germany, 2013; pp. 203–232. [Google Scholar]
- Haidegger, T.; Kazanzides, P.; Rudas, I.; Benyó, B.; Benyó, Z. The importance of accuracy measurement standards for computer-integrated interventional systems. In Proceedings of the EURON GEM Sig Workshop on the Role of Experiments in Robotics Research at IEEE ICRA, Anchorage, AK, USA, 3 May 2010; pp. 1–6. [Google Scholar]
- Nagy, T.D.; Ukhrenkov, N.; Drexler, D.A.; Takács, Á.; Haidegger, T. Enabling quantitative analysis of situation awareness: System architecture for autonomous vehicle handover studies. In Proceedings of the 2019 IEEE International Conference on Systems, Man and Cybernetics (SMC), Bari, Italy, 6–9 October 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 904–908. [Google Scholar]
- Woodward, J.; Ruiz, J. Analytic review of using augmented reality for situational awareness. IEEE Trans. Vis. Comput. Graph. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Gnjatović, M.; Maček, N.; Adamović, S. Putting Humans Back in the Loop: A Study in Human–Machine Cooperative Learning. Acta Polytech. Hung. 2020, 17, 191–210. [Google Scholar] [CrossRef]
- Nagy, T.D.; Haidegger, T. Performance and Capability Assessment in Surgical Subtask Automation. Sensors 2022, 22, 2501. [Google Scholar] [CrossRef]
Figure 1.
Steps for percutaneous pedicle screw fixation in the case of thoracolumbar fracture (A) The intra-operative posteroanterior and lateral fluoroscopy as image guidance; (B) Planning the entry point of the vertebra, the pedicle entry site is decorticated, and, with the application of a curved or straight pedicle probe, a pathway is pre-formed for the screw through the cancellous bone; (C) Pedicle screws are then inserted with extended tabs; (D) Contoured fixation rod is inserted into the subfascial layer, and the screws are tightened on the rod [6].
Figure 1.
Steps for percutaneous pedicle screw fixation in the case of thoracolumbar fracture (A) The intra-operative posteroanterior and lateral fluoroscopy as image guidance; (B) Planning the entry point of the vertebra, the pedicle entry site is decorticated, and, with the application of a curved or straight pedicle probe, a pathway is pre-formed for the screw through the cancellous bone; (C) Pedicle screws are then inserted with extended tabs; (D) Contoured fixation rod is inserted into the subfascial layer, and the screws are tightened on the rod [6].

Figure 2.
Robot-Assisted Surgery integrated with Image-Guided Surgery means the direct application of intra-operative tracking data to robotic/human intervention. Key target procedures include orthopaedics and neurosurgery. (Image credit: Microsoft, Philips and Northern Digital Inc. [20,21,22]).

Figure 3.
PRISMA chart of the literature search performed for the keywords “Augmented Reality” and “Spine Surgery”.
Figure 3.
PRISMA chart of the literature search performed for the keywords “Augmented Reality” and “Spine Surgery”.

Figure 4.
How to score AR systems? Examples: Examples of scoring AR systems. (a) Based on the article by Dennler et al. [29] and (b) Other mentioned methods based on the article by Bitkina et al. [65].

Figure 5.
3D plot chart scoring the main attributes with minimum requirements of AR–HMD (yellow) and RAS (green) in spine surgery: User Satisfaction Score (USS), Clinical Accuracy and relative Operation Time (OT). The larger triangle area is better.
Figure 5.
3D plot chart scoring the main attributes with minimum requirements of AR–HMD (yellow) and RAS (green) in spine surgery: User Satisfaction Score (USS), Clinical Accuracy and relative Operation Time (OT). The larger triangle area is better.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Publication list of search results for AR–HMD navigated pedicle screw insertions.
| Author | Year | Use Case | # Cases | # Screws | Linear Tip Error (mm) | Angular Traj. Error (°) | Gertzbein–Robbins Scale | Device |
|---|---|---|---|---|---|---|---|---|
| Molina, C.A. et al. [26] | 2021/3 | in vivo | 1 | 6 | 2.07 (1.62–2.52) | 2.41 (1.57–3.25) | 100% A | xvision, Augmedics |
| Li, J. et al. [27] | 2021/3 | in vivo | 7 | 57 | N/A | N/A | 100% A | MITINS system (HoloLens) |
| Liu, A. et al. [28] | 2021/10 | in vivo | 28 | 205 | N/A | N/A | 98% A and B | xvision, Augmedics |
| Dennler, C. et al. [29] | 2021/5 | in vivo | 25 | N/A | N/A | N/A | “increased intraop. accuracy (78 ± 23 points)” | HoloLens |
| Yahanda, A.T. et al. [30] | 2021/8 | in vivo | 9 | 63 | N/A | N/A | 96.8% A, 3.2% B | xvision, Augmedics |
| Farshad, M. et al. [31] | 2021/5 | in vivo | 1 | 4 | 3.5 ± 1.9 | 7.3 ± 3.6 | N/A | HoloLens 2 |
| Bhatt, F.R. et al. [32] | 2022/1 | in vivo | 32 | 222 | N/A | N/A | 97.1% A and B | xvision, Augmedics |
| Felix, B. et al. [33] | 2022/2 | cadaver | 7 | 124 | 1.9 | 2.4 | 96% A and B | HoloLens 2 |
| Spirig, J.M. et al. [34] | 2021/12 | cadaver | 2 | 8 | 5.99 ± 3.60 | 5.88 ± 3.69 | N/A | HoloLens |
| Farshad, M. et al. [35] | 2021/1 | cadaver | 8 | 160 | 4 ± 2.7 | 6.8 ± 3.9 | 97.5% A and B | HoloLens 2 |
| Dennler, C. et al. [36] | 2021/2 | phantom | 1 | 40 | N/A | −10.8 ± 11.77 | 97.5% A | HoloLens |
| Frisk, H. et al. [37] | 2022/1 | phantom | 4 | 48 | 1.4 ± 0.8 | 3.0 ± 1.4 | 94% A and B | MagicLeap |
| Yanni, D.S. et al. [38] | 2021/8 | phantom | 24 | 192 | N/A | 5 | 98.4% A and B | SpineAR (prototype) |
| Urakov, T.M. [39] | 2020/12 | phantom | 5 | 60 | N/A | N/A | 97% | Caduceus AR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Móga, K.; Ferencz, A.; Haidegger, T. What Is Next in Computer-Assisted Spine Surgery? Advances in Image-Guided Robotics and Extended Reality. Robotics 2023, 12, 1. https://doi.org/10.3390/robotics12010001
AMA Style
Móga K, Ferencz A, Haidegger T. What Is Next in Computer-Assisted Spine Surgery? Advances in Image-Guided Robotics and Extended Reality. Robotics. 2023; 12(1):1. https://doi.org/10.3390/robotics12010001
Chicago/Turabian StyleMóga, Kristóf, Andrea Ferencz, and Tamás Haidegger. 2023. "What Is Next in Computer-Assisted Spine Surgery? Advances in Image-Guided Robotics and Extended Reality" Robotics 12, no. 1: 1. https://doi.org/10.3390/robotics12010001
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.