
Circulating Hsp70 Levels and the Immunophenotype of Peripheral Blood Lymphocytes as Potential Biomarkers for Advanced Lung Cancer and Therapy Failure after Surgery
 ,
,
Abstract
:1. Introduction
2. Material and Methods
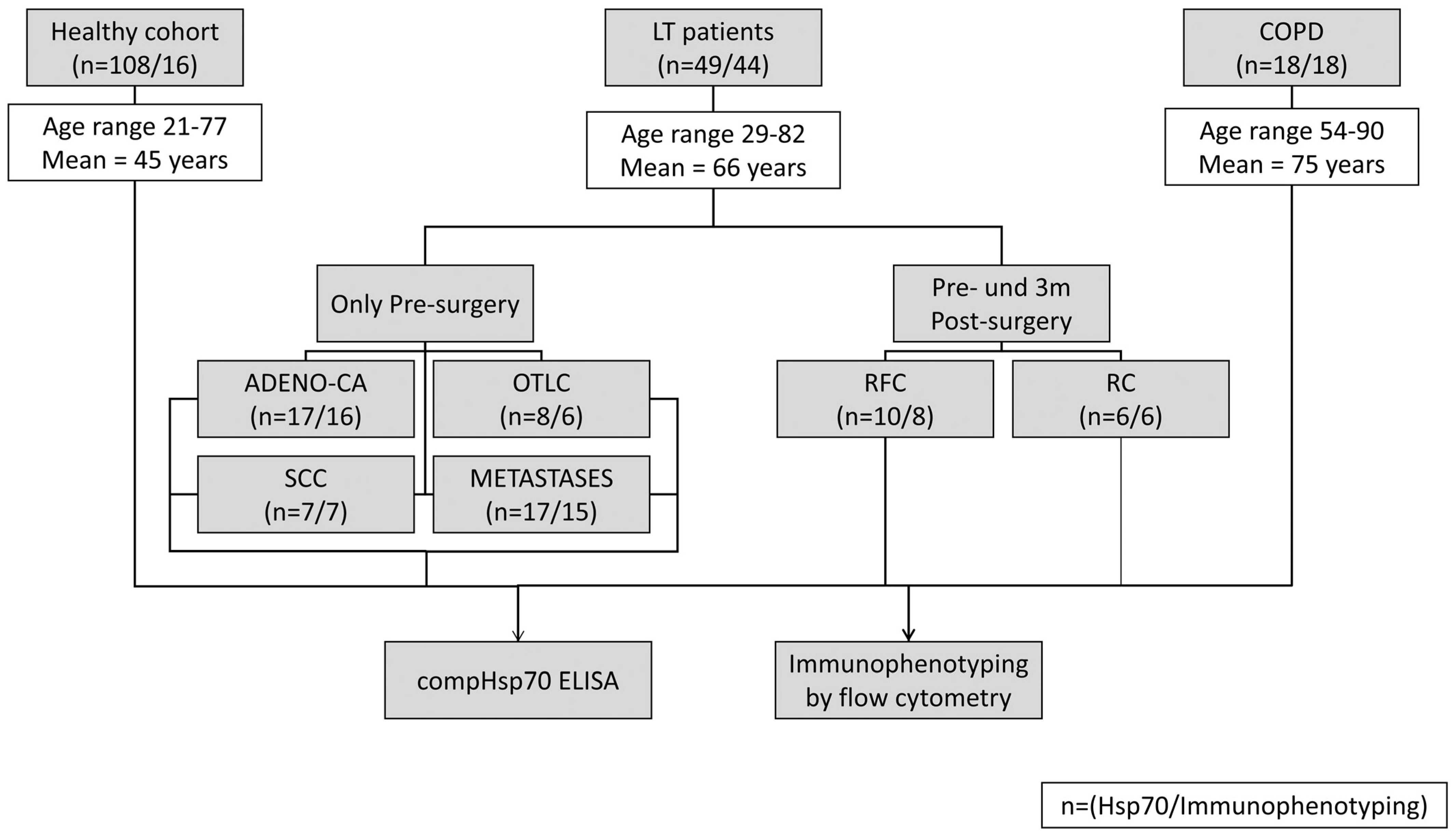
2.1. Patients and Sample Collection
2.2. Therapies
2.3. Measurement of Free and Exosomal Hsp70 in the Blood by Using the compHsp70 ELISA
2.4. Immunophenotyping of Lymphocyte Subpopulations Using Multiparameter Flow Cytometry
3. Results
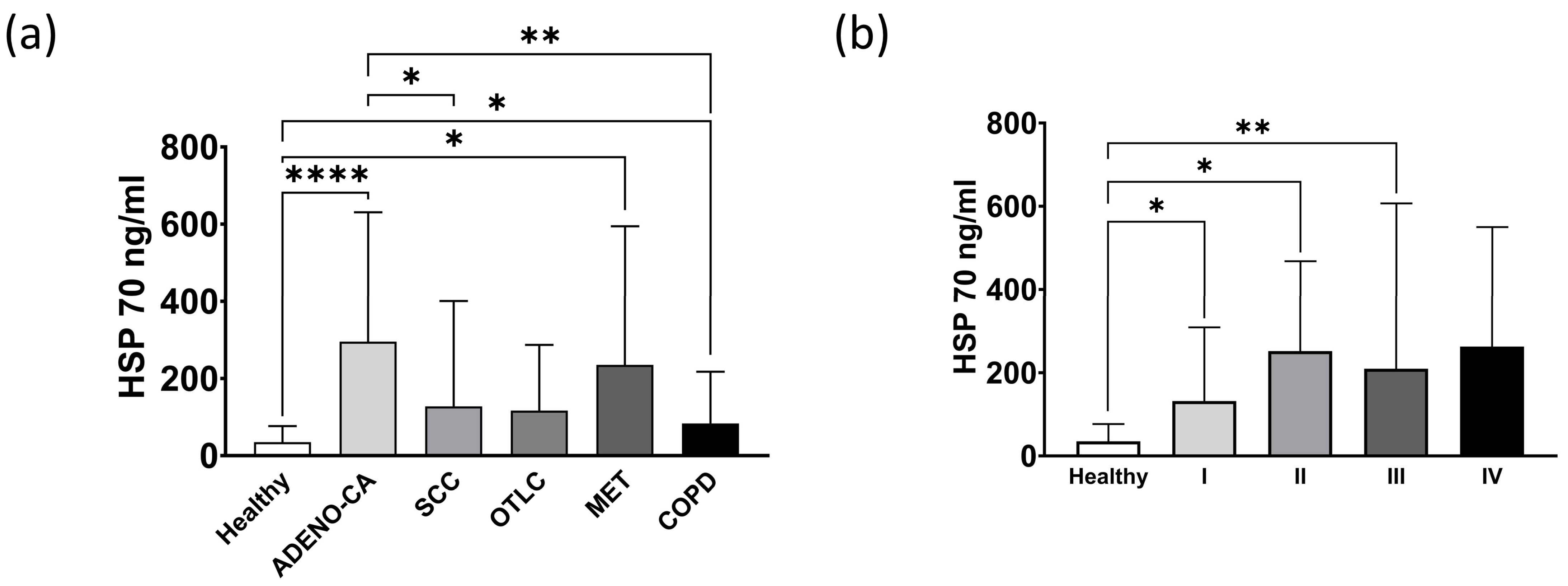
3.1. Exosomal and Free Hsp70 Levels in Circulation in the Healthy Controls, Different Types of Lung Tumors and Patients with COPD
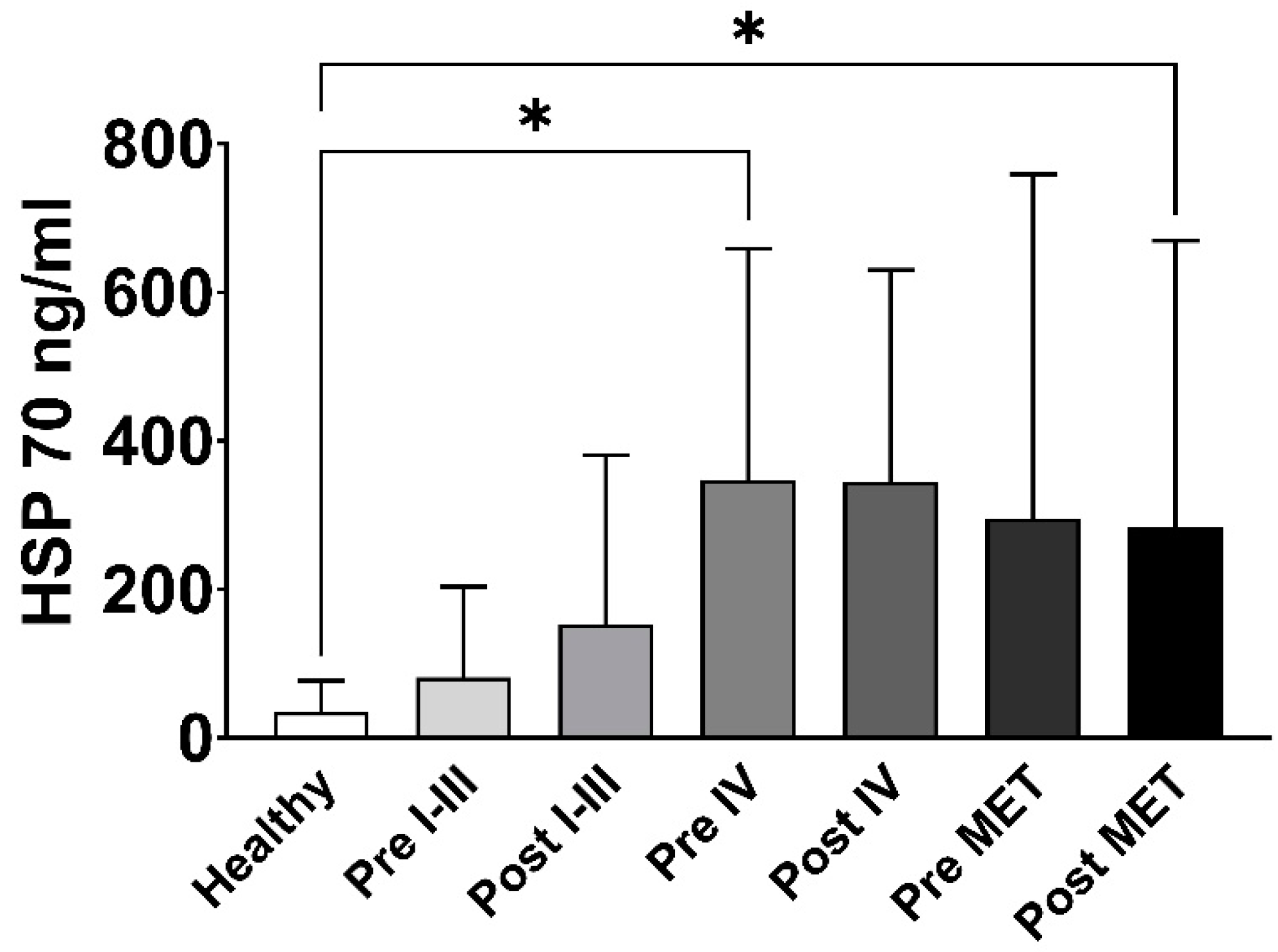
3.2. Exosomal and Free Hsp70 Levels before and after Surgery in Lung Cancer Patients in Different Tumor Stages
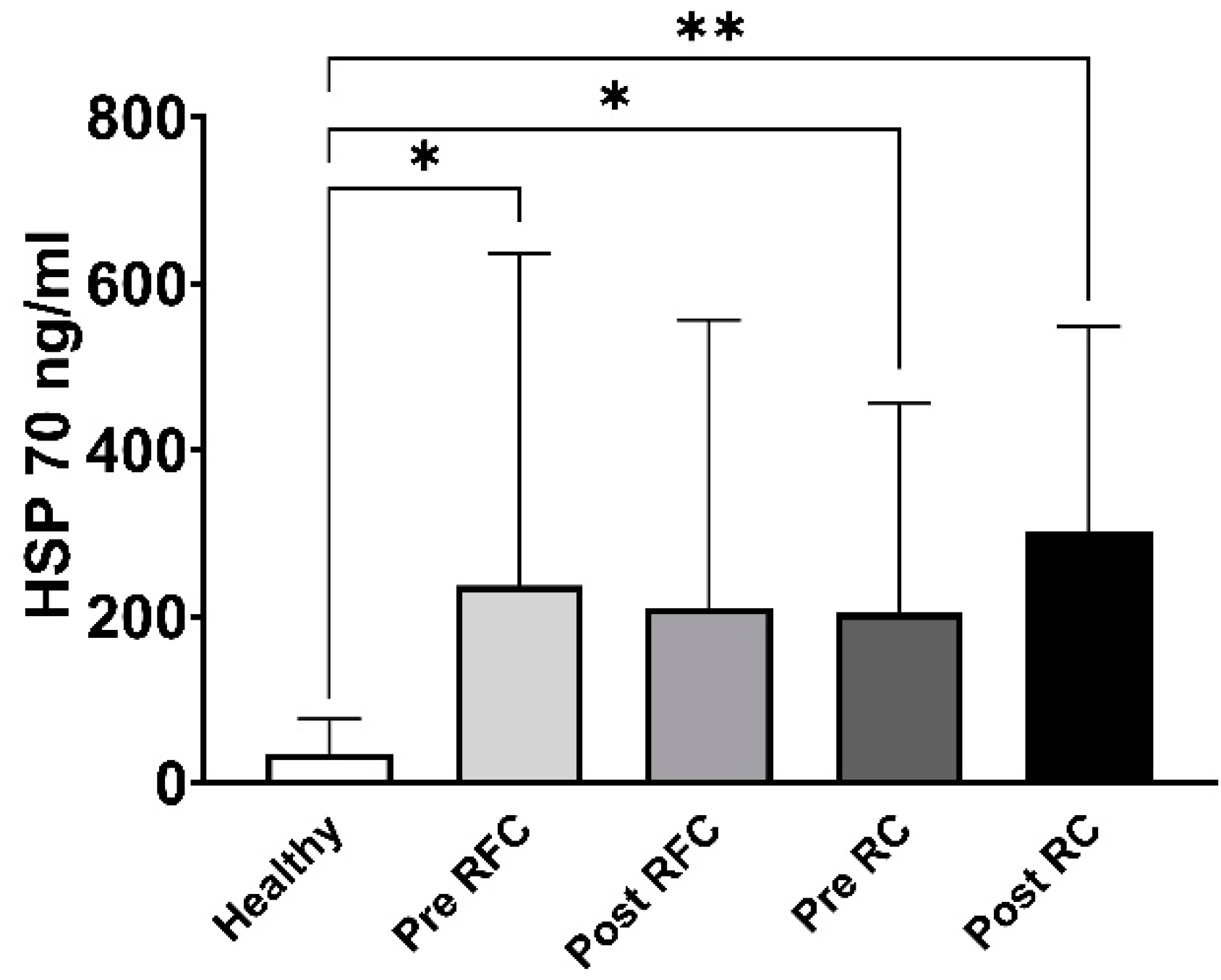
3.3. Exosomal and Free Hsp70 Levels in a Cohort of Recurrence-Free and Early Recurrence Lung Cancer Patients
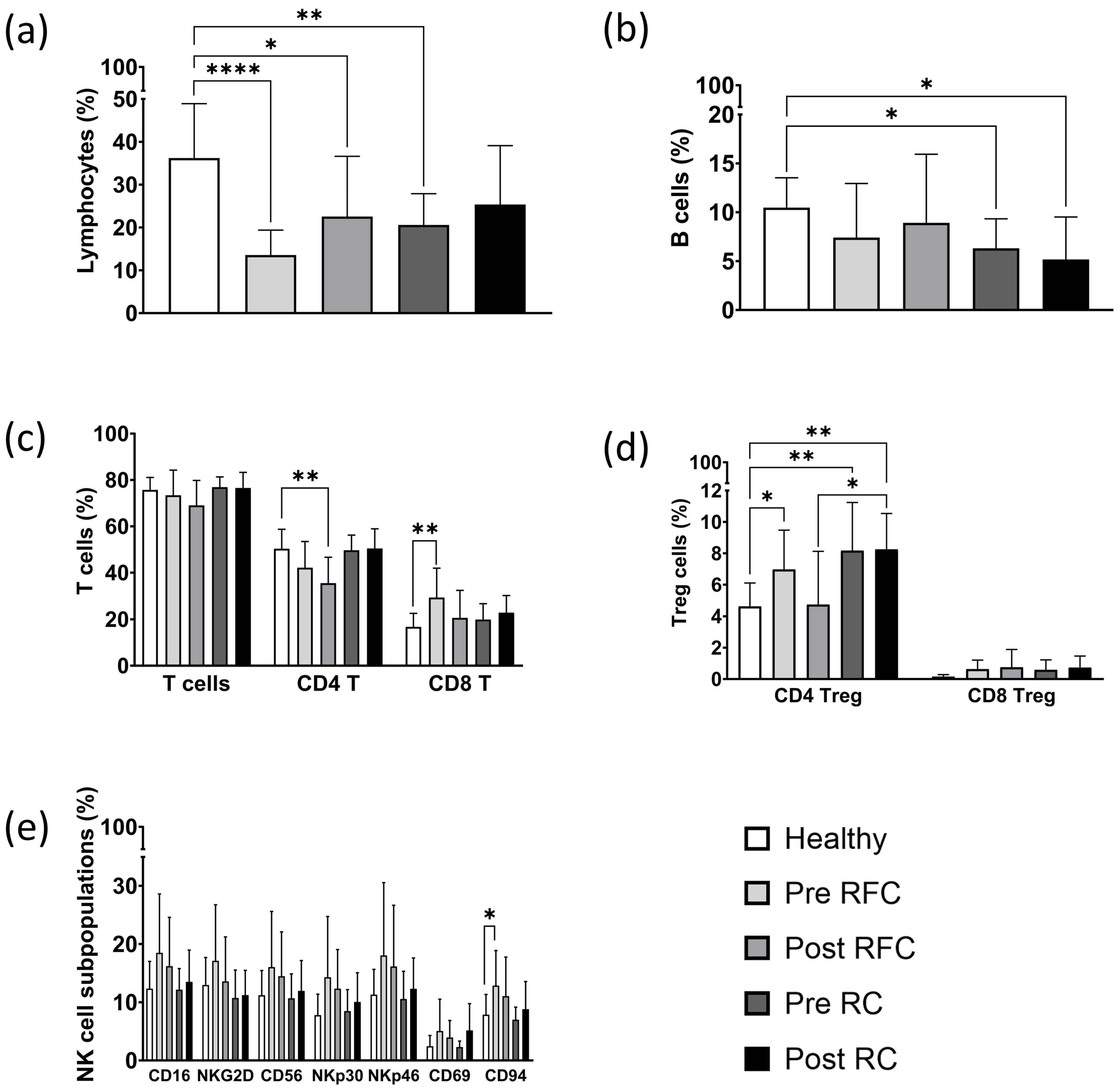
3.4. Immunophenotyping of Lymphocyte Subpopulations in a Cohort of Recurrence-Free and Early Recurrence Lung Cancer Patients
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- De Koning, H.; Van Der Aalst, C.; Ten Haaf, K.; Oudkerk, M. Effekts of volume ct lung cancer screening: Mortality results of the nelson randomised-controlled population based trial. J. Thorac. Oncol. 2018, 13, S185. [Google Scholar] [CrossRef]
- Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [CrossRef] [PubMed]
- Schabath, M.B.; Cote, M.L. Cancer progress and priorities: Lung cancer. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1563–1579. [Google Scholar] [CrossRef]
- Barnes, B.; Kraywinkel, K.; Nowossadeck, E.; Schönfeld, I.; Starker, A.; Wienecke, A.; Wolf, U. Bericht zum Krebsgeschehen in Deutschland 2016; Robert Koch Institute: Berlin, Germany, 2016; pp. 32–34. [Google Scholar] [CrossRef]
- De Torres, J.P.; Bastarrika, G.; Wisnivesky, J.P.; Alcaide, A.B.; Campo, A.; Seijo, L.M.; Pueyo, J.C.; Villanueva, A.; Lozano, M.D.; Montes, U.; et al. Assessing the relationship between lung cancer risk and emphysema detected on low-dose ct of the chest. Chest 2007, 132, 1932–1938. [Google Scholar] [CrossRef]
- Scrimini, S.; Pons, J.; Sauleda, J. Myeloid-derived suppressor cells: Possible link between chronic obstrucive pulmonary disease and lung cancer. Arch. Bronconeumol. 2016, 52, 29–35. [Google Scholar] [CrossRef]
- Yamauchi, Y.; Safi, S.; Blattner, C.; Rathinasamy, A.; Umansky, L.; Juenger, S.; Warth, A.; Eichhorn, M.; Muley, T.; Herth, F.J.F.; et al. Circulating and tumor myeloid-derived suppressor cells in resectable non-small cell lung cancer. Am. J. Respir. Crit. Care Med. 2018, 198, 777–787. [Google Scholar] [CrossRef]
- Radons, J. The human hsp70 family of chaperones: Where do we stand? Cell Stress Chaperones 2016, 21, 379–404. [Google Scholar] [CrossRef]
- Multhoff, G.; Botzler, C.; Wiesnet, M.; Muller, E.; Meier, T.; Wilmanns, W.; Issels, R.D. A stress-inducible 72-kda heat-shock protein (hsp72) is expressed on the surface of human tumor cells, but not on normal cells. Int. J. Cancer 1995, 61, 272–279. [Google Scholar] [CrossRef]
- Gehrmann, M.; Schmetzer, H.; Eissner, G.; Haferlach, T.; Hiddemann, W.; Multhoff, G. Membrane-bound heat shock protein 70 (hsp70) in acute myeloid leukemia: A tumor specific recognition structure for the cytolytic activity of autologous nk cells. Haematologica 2003, 88, 474–476. [Google Scholar]
- Gastpar, R.; Gehrmann, M.; Bausero, M.A.; Asea, A.; Gross, C.; Schroeder, J.A.; Multhoff, G. Heat shock protein 70 surface-positive tumor exosomes stimulate migratory and cytolytic activity of natural killer cells. Cancer Res. 2005, 65, 5238–5247. [Google Scholar] [CrossRef] [PubMed]
- Gunther, S.; Ostheimer, C.; Stangl, S.; Specht, H.M.; Mozes, P.; Jesinghaus, M.; Vordermark, D.; Combs, S.E.; Peltz, F.; Jung, M.P.; et al. Correlation of hsp70 serum levels with gross tumor volume and composition of lymphocyte subpopulations in patients with squamous cell and adeno non-small cell lung cancer. Front. Immunol. 2015, 6, 556. [Google Scholar] [CrossRef] [PubMed]
- Stepien, E.L.; Durak-Kozica, M.; Moskal, P. Extracellular vesicles in vascular pathophysiology: Beyond their molecular content. Pol. Arch. Intern. Med. 2023, 133, 16483. [Google Scholar] [CrossRef] [PubMed]
- Leidal, A.M.; Debnath, J. Unraveling the mechanisms that specify molecules for secretion in extracellular vesicles. Methods 2020, 177, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Yang, X.; Jiang, T.; Yan, C.; Xu, X.; Chen, Z. Tissue-derived extracellular vesicles: Isolation, purification, and multiple roles in normal and tumor tissues. Life Sci. 2023, 321, 121624. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, Y.; Li, Z.; Wei, S.; Chi, X.; Yan, X.; Lv, H.; Zhao, L.; Zhao, L. Combination of size-exclusion chromatography and ion exchange adsorption for improving the proteomic analysis of plasma-derived extracellular vesicles. Proteomics 2023, 23, e2200364. [Google Scholar] [CrossRef]
- Sojka, D.R.; Abramowicz, A.; Adamiec-Organisciok, M.; Karnas, E.; Mielanczyk, L.; Kania, D.; Blamek, S.; Telka, E.; Scieglinska, D. Heat shock protein a2 is a novel extracellular vesicle-associated protein. Sci. Rep. 2023, 13, 4734. [Google Scholar] [CrossRef]
- Fathi, M.; Martinez-Paniagua, M.; Rezvan, A.; Montalvo, M.J.; Mohanty, V.; Chen, K.; Mani, S.A.; Varadarajan, N. Identifying signatures of ev secretion in metastatic breast cancer through functional single-cell profiling. iScience 2023, 26, 106482. [Google Scholar] [CrossRef]
- Multhoff, G.; Pfister, K.; Botzler, C.; Jordan, A.; Scholz, R.; Schmetzer, H.; Burgstahler, R.; Hiddemann, W. Adoptive transfer of human natural killer cells in mice with severe combined immunodeficiency inhibits growth of hsp70-expressing tumors. Int. J. Cancer 2000, 88, 791–797. [Google Scholar] [CrossRef]
- Stangl, S.; Wortmann, A.; Guertler, U.; Multhoff, G. Control of metastasized pancreatic carcinomas in scid/beige mice with human il-2/tkd-activated nk cells. J. Immunol. 2006, 176, 6270–6276. [Google Scholar] [CrossRef]
- Gehrmann, M.; Radons, J.; Molls, M.; Multhoff, G. The therapeutic implications of clinically applied modifiers of heat shock protein 70 (hsp70) expression by tumor cells. Cell Stress Chaperones 2008, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Multhoff, G.; Mizzen, L.; Winchester, C.C.; Milner, C.M.; Wenk, S.; Eissner, G.; Kampinga, H.H.; Laumbacher, B.; Johnson, J. Heat shock protein 70 (hsp70) stimulates proliferation and cytolytic activity of natural killer cells. Exp. Hematol. 1999, 27, 1627–1636. [Google Scholar] [CrossRef] [PubMed]
- Multhoff, G.; Pfister, K.; Gehrmann, M.; Hantschel, M.; Gross, C.; Hafner, M.; Hiddemann, W. A 14-mer hsp70 peptide stimulates natural killer (nk) cell activity. Cell Stress Chaperones 2001, 6, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Gross, C.; Koelch, W.; Demaio, A.; Arispe, N.; Multhoff, G. Cell surface-bound heat shock protein 70 (hsp70) mediates perforin-independent apoptosis by specific binding and uptake of granzyme b. J. Biol. Chem. 2003, 278, 41173–41181. [Google Scholar] [CrossRef] [PubMed]
- Specht, H.M.; Ahrens, N.; Blankenstein, C.; Duell, T.; Fietkau, R.; Gaipl, U.S.; Gunther, C.; Gunther, S.; Habl, G.; Hautmann, H.; et al. Heat shock protein 70 (hsp70) peptide activated natural killer (nk) cells for the treatment of patients with non-small cell lung cancer (nsclc) after radiochemotherapy (rctx)—From preclinical studies to a clinical phase ii trial. Front. Immunol. 2015, 6, 162. [Google Scholar] [CrossRef]
- Bi, J.; Tian, Z. Nk cell exhaustion. Front. Immunol. 2017, 8, 760. [Google Scholar] [CrossRef]
- Thommen, D.S.; Schumacher, T.N. T cell dysfunction in cancer. Cancer Cell 2018, 33, 547–562. [Google Scholar] [CrossRef]
- Myers, J.A.; Miller, J.S. Exploring the nk cell platform for cancer immunotherapy. Nat. Rev. Clin. Oncol. 2021, 18, 85–100. [Google Scholar] [CrossRef]
- Seier, S.; Bashiri Dezfouli, A.; Lennartz, P.; Pockley, A.G.; Klein, H.; Multhoff, G. Elevated levels of circulating hsp70 and an increased prevalence of cd94+/cd69+ nk cells is predictive for advanced stage non-small cell lung cancer. Cancers 2022, 14, 5701. [Google Scholar] [CrossRef]
- Werner, C.; Stangl, S.; Salvermoser, L.; Schwab, M.; Shevtsov, M.; Xanthopoulos, A.; Wang, F.; Dezfouli, A.B.; Tholke, D.; Ostheimer, C.; et al. Hsp70 in liquid biopsies-a tumor-specific biomarker for detection and response monitoring in cancer. Cancers 2021, 13, 3706. [Google Scholar] [CrossRef]
- Belka, C.; Ottinger, H.; Kreuzfelder, E.; Weinmann, M.; Lindemann, M.; Lepple-Wienhues, A.; Budach, W.; Grosse-Wilde, H.; Bamberg, M. Impact of localized radiotherapy on blood immune cells counts and function in humans. Radiother. Oncol. 1999, 50, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Multhoff, G.; Seier, S.; Stangl, S.; Sievert, W.; Shevtsov, M.; Werner, C.; Pockley, A.G.; Blankenstein, C.; Hildebrandt, M.; Offner, R.; et al. Targeted natural killer cell-based adoptive immunotherapy for the treatment of patients with nsclc after radiochemotherapy: A randomized phase ii clinical trial. Clin. Cancer Res. 2020, 26, 5368–5379. [Google Scholar] [CrossRef] [PubMed]
- Lobinger, D.; Gempt, J.; Sievert, W.; Barz, M.; Schmitt, S.; Nguyen, H.T.; Stangl, S.; Werner, C.; Wang, F.; Wu, Z.; et al. Potential role of hsp70 and activated nk cells for prediction of prognosis in glioblastoma patients. Front. Mol. Biosci. 2021, 8, 669366. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Nickl, S.; Lambers, C.; Hacker, S.; Mitterbauer, A.; Hoetzenecker, K.; Rozsas, A.; Ostoros, G.; Laszlo, V.; Hofbauer, H.; et al. Discrimination of clinical stages in non-small cell lung cancer patients by serum hsp27 and hsp70: A multi-institutional case-control study. Clin. Chim. Acta. 2012, 413, 1115–1120. [Google Scholar] [CrossRef]
- Lindquist, S.; Craig, E.A. The heat-shock proteins. Annu. Rev. Genet. 1988, 22, 631–677. [Google Scholar] [CrossRef]
- Bonilla, F.A.; Oettgen, H.C. Adaptive immunity. J. Allergy Clin. Immunol. 2010, 125, S33–S40. [Google Scholar] [CrossRef]
- Shahal-Zimra, Y.; Rotem, Z.; Chezar, J.; Shochat, T.; Ross, L.; Pickholtz, I.; Rabizadeh, E. Lymphocyte subset reference ranges in healthy israeli adults. Isr. Med. Assoc. J. 2016, 18, 739–743. [Google Scholar]
- Zhao, W.; Wang, P.; Jia, H.; Chen, M.; Gu, X.; Liu, M.; Zhang, Z.; Cheng, W.; Wu, Z. Lymphocyte count or percentage: Which can better predict the prognosis of advanced cancer patients following palliative care? BMC Cancer 2017, 17, 514. [Google Scholar] [CrossRef]
- Sapski, S.; Beha, N.; Kontermann, R.; Muller, D. Tumor-targeted costimulation with antibody-fusion proteins improves bispecific antibody-mediated immune response in presence of immunosuppressive factors. Oncoimmunology 2017, 6, e1361594. [Google Scholar] [CrossRef]
- Verastegui, E.L.; Morales, R.B.; Barrera-Franco, J.L.; Poitevin, A.C.; Hadden, J. Long-term immune dysfunction after radiotherapy to the head and neck area. Int. Immunopharmacol. 2003, 3, 1093–1104. [Google Scholar] [CrossRef]
- Dovsak, T.; Ihan, A.; Didanovic, V.; Kansky, A.; Verdenik, M.; Hren, N.I. Effect of surgery and radiotherapy on complete blood count, lymphocyte subsets and inflammatory response in patients with advanced oral cancer. BMC Cancer 2018, 18, 235. [Google Scholar] [CrossRef] [PubMed]
- Largeot, A.; Pagano, G.; Gonder, S.; Moussay, E.; Paggetti, J. The b-side of cancer immunity: The underrated tune. Cells 2019, 8, 449. [Google Scholar] [CrossRef] [PubMed]
- Barth, D.A.; Stanzer, S.; Spiegelberg, J.A.; Bauernhofer, T.; Absenger, G.; Szkandera, J.; Gerger, A.; Smolle, M.A.; Hutterer, G.C.; Ahyai, S.A.; et al. Patterns of peripheral blood b-cell subtypes are associated with treatment response in patients treated with immune checkpoint inhibitors: A prospective longitudinal pan-cancer study. Front. Immunol. 2022, 13, 840207. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Liu, Y.; Till, B.; Song, Y.; Wang, Z. Pretreatment peripheral b cells are associated with tumor response to anti-pd-1-based immunotherapy. Front. Immunol. 2020, 11, 563653. [Google Scholar] [CrossRef] [PubMed]
- Qin, Z.; Richter, G.; Schuler, T.; Ibe, S.; Cao, X.; Blankenstein, T. B cells inhibit induction of t cell-dependent tumor immunity. Nat. Med. 1998, 4, 627–630. [Google Scholar] [CrossRef]
- Raskov, H.; Orhan, A.; Christensen, J.P.; Gogenur, I. Cytotoxic cd8(+) t cells in cancer and cancer immunotherapy. Br. J. Cancer 2021, 124, 359–367. [Google Scholar] [CrossRef]
- Kamphorst, A.O.; Ahmed, R. Cd4 t-cell immunotherapy for chronic viral infections and cancer. Immunotherapy 2013, 5, 975–987. [Google Scholar] [CrossRef]
- Miggelbrink, A.M.; Jackson, J.D.; Lorrey, S.J.; Srinivasan, E.S.; Waibl-Polania, J.; Wilkinson, D.S.; Fecci, P.E. Cd4 t-cell exhaustion: Does it exist and what are its roles in cancer? Clin. Cancer Res. 2021, 27, 5742–5752. [Google Scholar] [CrossRef]
- Golubovskaya, V.; Wu, L. Different subsets of t cells, memory, effector functions, and car-t immunotherapy. Cancers 2016, 8, 36. [Google Scholar] [CrossRef]
- Tanaka, A.; Sakaguchi, S. Targeting treg cells in cancer immunotherapy. Eur. J. Immunol. 2019, 49, 1140–1146. [Google Scholar] [CrossRef]
- O'callaghan, D.S.; Rexhepaj, E.; Gately, K.; Coate, L.; Delaney, D.; O'donnell, D.M.; Kay, E.; O'connell, F.; Gallagher, W.M.; O'byrne, K.J. Tumour islet foxp3+ t-cell infiltration predicts poor outcome in nonsmall cell lung cancer. Eur. Respir. J. 2015, 46, 1762–1772. [Google Scholar] [CrossRef] [PubMed]
- Lodoen, M.B.; Lanier, L.L. Natural killer cells as an initial defense against pathogens. Curr. Opin. Immunol. 2006, 18, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.; Oberle, N.; Krammer, P.H. Molecular mechanisms of treg-mediated t cell suppression. Front. Immunol. 2012, 3, 51. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Jiang, P.; Wei, S.; Xu, X.; Wang, J. Regulatory t cells in tumor microenvironment: New mechanisms, potential therapeutic strategies and future prospects. Mol. Cancer 2020, 19, 116. [Google Scholar] [CrossRef] [PubMed]
- Trzonkowski, P.; Szmit, E.; Mysliwska, J.; Dobyszuk, A.; Mysliwski, A. Cd4+cd25+ t regulatory cells inhibit cytotoxic activity of t cd8+ and nk lymphocytes in the direct cell-to-cell interaction. Clin. Immunol. 2004, 112, 258–267. [Google Scholar] [CrossRef]
- Pedroza-Pacheco, I.; Madrigal, A.; Saudemont, A. Interaction between natural killer cells and regulatory t cells: Perspectives for immunotherapy. Cell. Mol. Immunol. 2013, 10, 222–229. [Google Scholar] [CrossRef]
- Gross, C.; Schmidt-Wolf, I.G.; Nagaraj, S.; Gastpar, R.; Ellwart, J.; Kunz-Schughart, L.A.; Multhoff, G. Heat shock protein 70-reactivity is associated with increased cell surface density of cd94/cd56 on primary natural killer cells. Cell Stress Chaperones 2003, 8, 348–360. [Google Scholar] [CrossRef]
- Gross, C.; Hansch, D.; Gastpar, R.; Multhoff, G. Interaction of heat shock protein 70 peptide with nk cells involves the nk receptor cd94. Biol. Chem. 2003, 384, 267–279. [Google Scholar] [CrossRef]
- Holdenrieder, S.; Stieber, P.; Peterfi, A.; Nagel, D.; Steinle, A.; Salih, H.R. Soluble mica in malignant diseases. Int. J. Cancer 2006, 118, 684–687. [Google Scholar] [CrossRef]
- Alvarez, M.; Simonetta, F.; Baker, J.; Pierini, A.; Wenokur, A.S.; Morrison, A.R.; Murphy, W.J.; Negrin, R.S. Regulation of murine nk cell exhaustion through the activation of the DNA damage repair pathway. JCI Insight 2019, 5, e127729. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tube | Company | Cat. No. | Specificity | Antibody | Volume (µL) |
|---|---|---|---|---|---|
| 1 | BD | 345815 | Isotype Control | IgG1-FITC | 5 |
| BD | 345816 | IgG1-PE | 5 | ||
| BD | 345817 | IgG1-PerCP | 5 | ||
| Caltag/Invitrogen | MG105 | IgG1-APC | 1 | ||
| 2 | BD | 555888 | T/NK cells | CD94-FITC | 5 |
| BD | 345812 | CD56-PE | 5 | ||
| BD | 345766 | CD3-PerCP | 10 | ||
| Caltag/Invitrogen | MHCD4505 | CD45-APC | 1 | ||
| 3 | BD | 345811 | T/B/NK cells | CD56-FITC | 5 |
| BD | 555413 | CD19-PE | 20 | ||
| BD | 345766 | CD3-PerCP | 10 | ||
| Caltag/Invitrogen | MHCD4505 | CD45-APC | 1 | ||
| 4 | BD | 345811 | T/NK cells | CD56-FITC | 5 |
| BD | 555413 | CD19-PE | 10 | ||
| BD | 345766 | CD3-PerCP | 10 | ||
| Caltag/Invitrogen | MHCD4505 | CD45-APC | 1 | ||
| 5 | BD | 345811 | T/NK cells | CD56-FITC | 5 |
| R&D | FAB139P | NKG2D-PE | 10 | ||
| BD | 345766 | CD3-PerCP | 10 | ||
| BD | 340560 | CD69-APC | 5 | ||
| 6 | BD | 345811 | T/NK cells | CD56-FITC | 5 |
| BC | IM3709 | Nkp30-PE | 10 | ||
| BD | 345766 | CD3-PerCP | 10 | ||
| BD | 340560 | CD69-APC | 5 | ||
| 7 | BD | 345811 | T/NK cells | CD56-FITC | 5 |
| BC | IM3711 | Nkp46-PE | 10 | ||
| BD | 345766 | CD3-PerCP | 10 | ||
| BD | 340560 | CD69-APC | 5 | ||
| 8 | BD | 555888 | T/NK cells | CD94-FITC | 5 |
| R&D | FAB139P | NKG2D-PE | 10 | ||
| BD | 345766 | CD3-PerCP | 10 | ||
| BD | 555518 | CD56-APC | 10 | ||
| 9 | BD | 555888 | T/NK cells | CD94-FITC | 5 |
| BC | IM3709 | Nkp30-PE | 10 | ||
| BD | 345766 | CD3-PerCP | 10 | ||
| BD | 555518 | CD56-APC | 10 | ||
| 10 | BD | 555888 | T/NK cells | CD94-FITC | 5 |
| BC | IM3711 | Nkp46-PE | 10 | ||
| BD | 345766 | CD3-PerCP | 10 | ||
| BD | 555518 | CD56-APC | 10 | ||
| 11 | BD | 555346 | CD4/CD8 T cells | CD4-FITC | 20 |
| BD | 555367 | CD8-PE | 20 | ||
| BD | 345766 | CD3-PerCP | 10 | ||
| Caltag/Invitrogen | MHCD4505 | CD45-APC | 1 | ||
| 12 | BD | 345815 | Isotype Control | IgG1-FITC | 5 |
| BD | 345816 | IgG1-PE | 5 | ||
| BD | 345817 | IgG1-PerCP | 5 | ||
| Caltag/Invitrogen | MG105 | IgG1-APC | 1 | ||
| 13 | BD | 555346 | CD4 Treg cells | CD4-FITC | 20 |
| BD | 345766 | CD3-PerCP | 10 | ||
| BD | 340907 | CD25-APC | 5 | ||
| BD | 560046 | FoxP3-PE | 20 | ||
| 14 | BD | 555366 | CD8 Treg cells | CD8-FITC | 20 |
| BD | 345766 | CD3-PerCP | 10 | ||
| BD | 340907 | CD25-APC | 5 | ||
| BD | 560046 | FoxP3-PE | 20 |
| Characteristic | Clusters | n |
|---|---|---|
| Sex | Male | 33 |
| Female | 16 | |
| Age | 20–29 | 1 |
| 30–39 | 2 | |
| 40–49 | 2 | |
| 50–59 | 6 | |
| 60–69 | 15 | |
| 70–79 | 16 | |
| 80–89 | 7 | |
| Histology | ADENO-CA * | 17 |
| SCC * | 7 | |
| OTLC * | 9 | |
| MET * | 16 | |
| UICC stage | I | 7 |
| II | 5 | |
| III | 11 | |
| IV | 9 |
| Characteristic | Clusters | n |
|---|---|---|
| Sex | Male | 11 |
| Female | 7 | |
| Age | 50–59 | 2 |
| 60–69 | 3 | |
| 70–79 | 5 | |
| 80–89 | 7 | |
| 90–99 | 1 | |
| COPD GOLD | I | 0 |
| II | 4 | |
| III | 9 | |
| IV | 5 | |
| Exacerbation | Yes | 10 |
| No | 8 |
| Characteristic | Clusters | n |
|---|---|---|
| Sex | Male | 10 |
| Female | 6 | |
| Age | 20–29 | 0 |
| 30–39 | 2 | |
| 40–49 | 1 | |
| 50–59 | 3 | |
| 60–69 | 6 | |
| 70–79 | 3 | |
| 80–89 | 1 | |
| Histology | ADENO-CA * | 4 |
| SCC * | 1 | |
| OTLC * | 4 | |
| MET * | 7 | |
| UICC stage | I | 1 |
| II | 1 | |
| III | 4 | |
| IV | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Safi, S.; Messner, L.; Kliebisch, M.; Eggert, L.; Ceylangil, C.; Lennartz, P.; Jefferies, B.; Klein, H.; Schirren, M.; Dommasch, M.; et al. Circulating Hsp70 Levels and the Immunophenotype of Peripheral Blood Lymphocytes as Potential Biomarkers for Advanced Lung Cancer and Therapy Failure after Surgery. Biomolecules 2023, 13, 874. https://doi.org/10.3390/biom13050874
Safi S, Messner L, Kliebisch M, Eggert L, Ceylangil C, Lennartz P, Jefferies B, Klein H, Schirren M, Dommasch M, et al. Circulating Hsp70 Levels and the Immunophenotype of Peripheral Blood Lymphocytes as Potential Biomarkers for Advanced Lung Cancer and Therapy Failure after Surgery. Biomolecules. 2023; 13(5):874. https://doi.org/10.3390/biom13050874
Chicago/Turabian StyleSafi, Seyer, Luis Messner, Merten Kliebisch, Linn Eggert, Ceyra Ceylangil, Philipp Lennartz, Benedict Jefferies, Henriette Klein, Moritz Schirren, Michael Dommasch, and et al. 2023. "Circulating Hsp70 Levels and the Immunophenotype of Peripheral Blood Lymphocytes as Potential Biomarkers for Advanced Lung Cancer and Therapy Failure after Surgery" Biomolecules 13, no. 5: 874. https://doi.org/10.3390/biom13050874