
The Association between Infant Colic and the Multi-Omic Composition of Human Milk

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Enrollment
2.3. Data Collection
2.4. Milk Collection
2.5. Cytokine Processing
2.6. Microbial and microRNA Processing
2.7. Statistical Analysis
3. Results
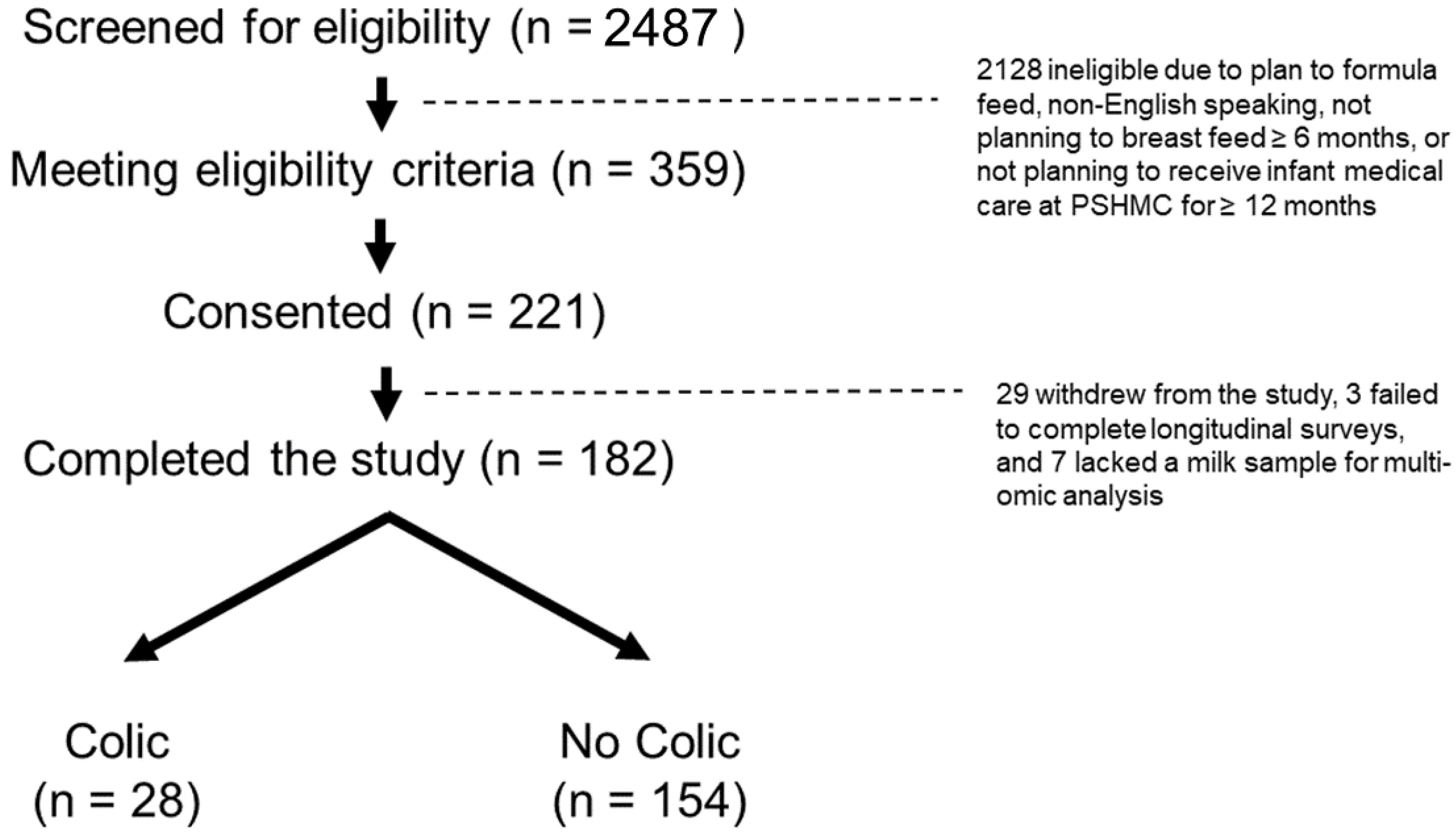
3.1. Participants
3.2. Multi-Omic Characteristics of Human Milk from Mothers of Infants with Colic
3.2.1. Milk Collection Variables
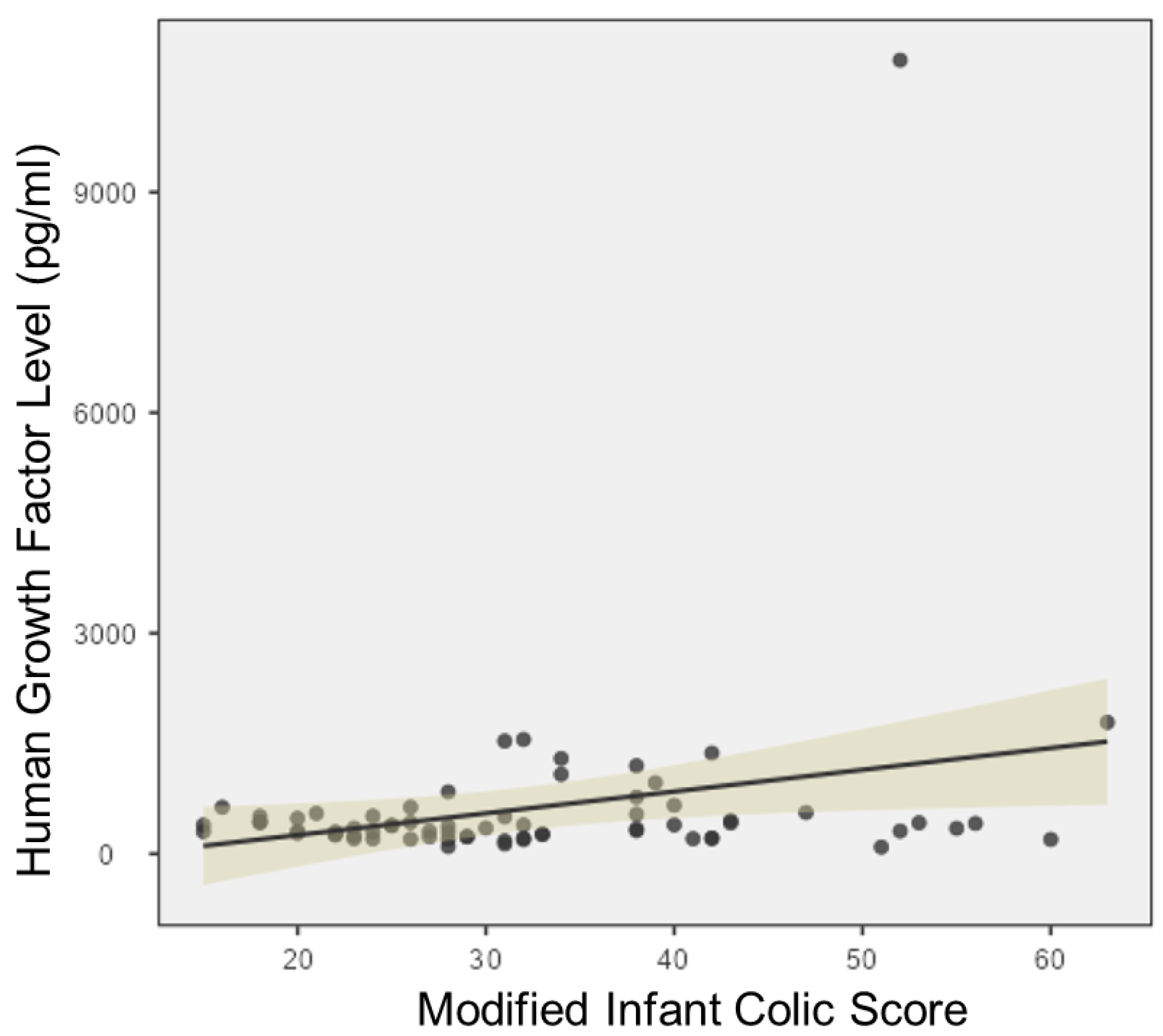
3.2.2. Proteomics
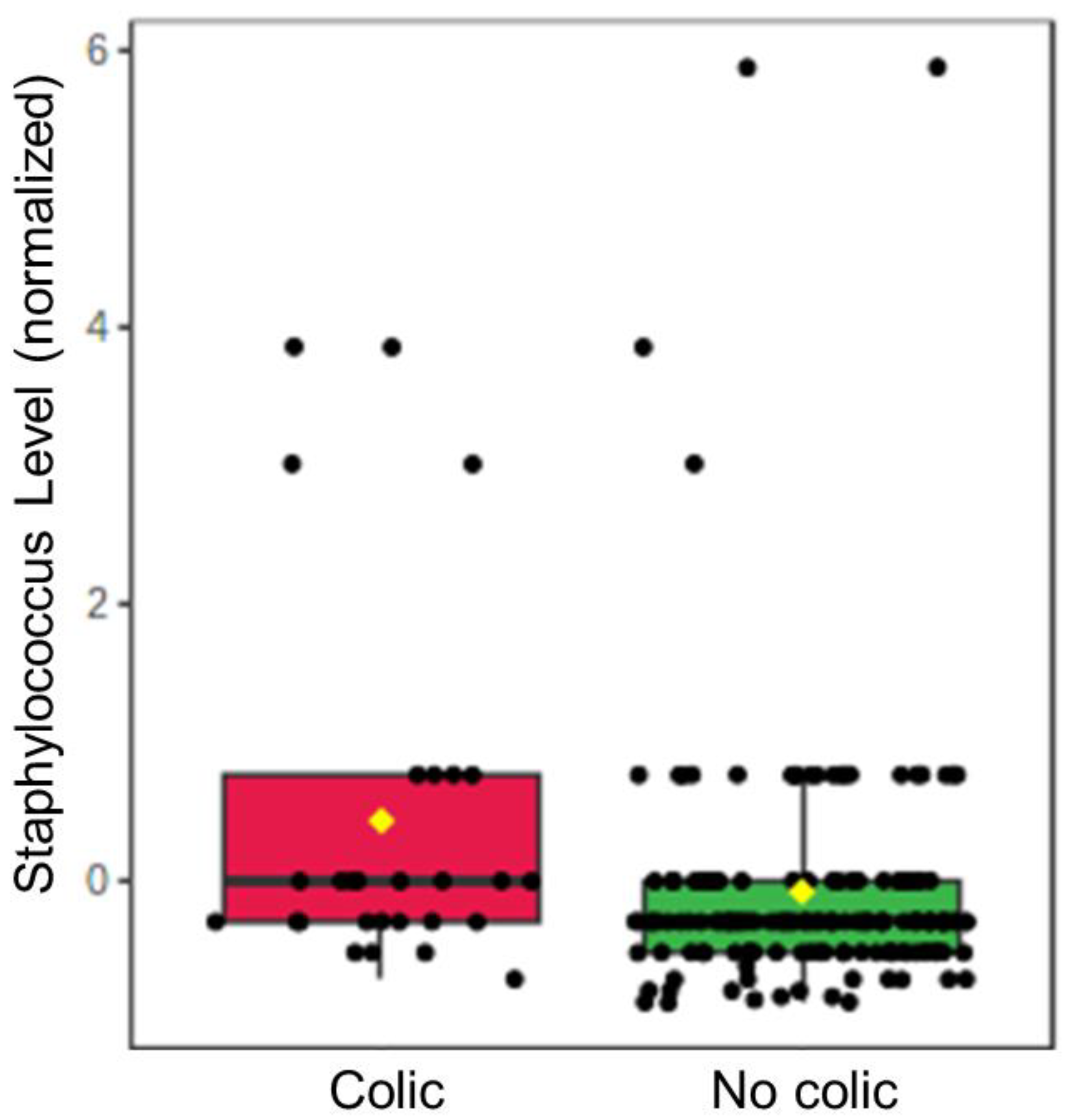
3.2.3. Microbiome
3.2.4. Human Milk miRNAs
3.3. Multi-Omic Modeling of Colic Risk
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hyman, P.E.; Milla, P.J.; Benninga, M.A.; Davidson, G.P.; Fleisher, D.F.; Taminiau, J. Childhood functional gastrointestinal disorders: Neonate/toddler. Gastroenterology 2006, 130, 1519–1526. [Google Scholar] [CrossRef] [Green Version]
- Campeotto, F.; Barbaza, M.O.; Hospital, V. Functional Gastrointestinal Disorders in Outpatients Aged up to 12 Months: A French Non-Interventional Study. Int. J. Environ. Res. Public Health 2020, 17, 4031. [Google Scholar] [CrossRef]
- van Tilburg, M.A.; Hyman, P.E.; Walker, L.; Rouster, A.; Palsson, O.S.; Kim, S.M.; Whitehead, W.E. Prevalence of functional gastrointestinal disorders in infants and toddlers. J. Pediatr. 2015, 166, 684–689. [Google Scholar] [CrossRef] [PubMed]
- Roberts, D.M.; Ostapchuk, M.; O’Brien, J.G. Infantile colic. Am. Fam. Physician 2004, 70, 735–740. [Google Scholar] [PubMed]
- Gelfand, A.A. Infant colic. Semin. Pediatr. Neurol. 2016, 23, 79–82. [Google Scholar] [CrossRef] [Green Version]
- Johnson, J.D.; Cocker, K.; Chang, E. Infantile Colic: Recognition and Treatment. Am. Fam. Physician 2015, 92, 577–582. [Google Scholar] [PubMed]
- Sarasu, J.M.; Narang, M.; Shah, D. Infantile Colic: An Update. Indian Pediatr. 2018, 55, 979–987. [Google Scholar] [CrossRef]
- Cohen-Silver, J.; Ratnapalan, S. Management of infantile colic: A review. Clin. Pediatr. 2009, 48, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Hall, B.; Chesters, J.; Robinson, A. Infantile colic: A systematic review of medical and conventional therapies. J. Paediatr. Child Health 2012, 48, 128–137. [Google Scholar] [CrossRef]
- Lucassen, P. Colic in infants. BMJ Clin. Evid. 2015, 2015, 03–09. [Google Scholar]
- Zeevenhooven, J.; Browne, P.D.; L’Hoir, M.P.; de Weerth, C.; Benninga, M.A. Infant colic: Mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 479–496. [Google Scholar] [CrossRef]
- Ouald Chaib, A.; Levy, I.E.; Ouald Chaib, M.; Vandenplas, Y. The Influence of the Gastrointestinal Microbiome on Infant Colic. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 919–932. [Google Scholar] [CrossRef]
- Savino, F. Focus on infantile colic. Acta Paediatr. 2007, 96, 1259–1264. [Google Scholar] [CrossRef]
- Critch, J.N.; Canadian Paediatric Society; Nutrition and Gastroenterology Committee. Infantile colic: Is there a role for dietary interventions? Paediatr. Child Health 2011, 16, 47–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hahn-Holbrook, J.; Fish, A.; Glynn, L.M. Human Milk Omega-3 Fatty Acid Composition Is Associated with Infant Temperament. Nutrients 2019, 11, 2964. [Google Scholar] [CrossRef] [Green Version]
- Perrella, S.; Gridneva, Z.; Lai, C.T.; Stinson, L.; George, A.; Bilston-John, S.; Geddes, D. Human milk composition promotes optimal infant growth, development and health. Semin. Perinatol. 2021, 45, 151380. [Google Scholar] [CrossRef] [PubMed]
- Iacovou, M.; Mulcahy, E.C.; Truby, H.; Barrett, J.S.; Gibson, P.R.; Muir, J.G. Reducing the maternal dietary intake of indigestible and slowly absorbed short-chain carbohydrates is associated with improved infantile colic: A proof-of-concept study. J. Hum. Nutr. Diet. 2018, 31, 256–265. [Google Scholar] [CrossRef] [Green Version]
- Duar, R.M.; Henrick, B.M.; Casaburi, G.; Frese, S.A. Integrating the Ecosystem Services Framework to Define Dysbiosis of the Breastfed Infant Gut: The Role of B. infantis and Human Milk Oligosaccharides. Front. Nutr. 2020, 7, 33. [Google Scholar] [CrossRef] [Green Version]
- de Weerth, C.; Fuentes, S.; de Vos, W.M. Crying in infants: On the possible role of intestinal microbiota in the development of colic. Gut Microbes 2013, 4, 416–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldassarre, M.E.; Di Mauro, A.; Mastromarino, P.; Fanelli, M.; Martinelli, D.; Urbano, F.; Capobianco, D.; Laforgia, N. Administration of a Multi-Strain Probiotic Product to Women in the Perinatal Period Differentially Affects the Breast Milk Cytokine Profile and May Have Beneficial Effects on Neonatal Gastrointestinal Functional Symptoms. A Randomized Clinical Trial. Nutrients 2016, 8, 677. [Google Scholar] [CrossRef] [Green Version]
- Garofalo, R.P.; Goldman, A.S. Expression of functional immunomodulatory and anti-inflammatory factors in human milk. Clin. Perinatol. 1999, 26, 361–378. [Google Scholar] [CrossRef]
- Newburg, D.; Walker, W. Protection of the Neonate by the Innate Immune System of Developing Gut and of Human Milk. Pediatr. Res. 2007, 61, 2–8. [Google Scholar] [CrossRef]
- Melnik, B.C.; Stremmel, W.; Weiskirchen, R.; John, S.M.; Schmitz, G. Exosome-Derived MicroRNAs of Human Milk and Their Effects on Infant Health and Development. Biomolecules 2021, 11, 851. [Google Scholar] [CrossRef]
- Lönnerdal, B. Human milk microRNAs/exosomes: Composition and biological effects. Nestle Nutr. Inst. Workshop Ser. 2019, 90, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Du, X.; Li, J.; Lönnerdal, B. Human milk exosomes and their microRNAs survive digestion in vitro and are taken up by human intestinal cells. Mol. Nutr. Food Res. 2017, 61, 1700082. [Google Scholar] [CrossRef]
- Kahn, S.; Liao, Y.; Du, X.; Xu, W.; Li, J.; Lönnerdal, B. Exosomal microRNAs in milk from mothers delivering preterm infants survive in vitro digestion and are taken up by human intestinal cells. Mol. Nutr. Food Res. 2018, 62, e1701050. [Google Scholar] [CrossRef] [PubMed]
- Casado-Bedmar, M.; Viennois, E. MicroRNA and Gut Microbiota: Tiny but Mighty-Novel Insights into Their Cross-talk in Inflammatory Bowel Disease Pathogenesis and Therapeutics. J. Crohns Colitis 2022, 16, 992–1005. [Google Scholar] [CrossRef] [PubMed]
- Hicks, S.D.; Beheshti, R.; Chandran, D.; Warren, K.; Confair, A. Infant consumption of microRNA miR-375 in human milk lipids is associated with protection from atopy. Am. J. Clin. Nutr. 2022, 116, 1654–1662. [Google Scholar] [CrossRef]
- Cirgin Ellett, M.L.; Murphy, D.; Stroud, L.; Shelton, R.A.; Sullivan, A.; Ellett, S.G.; Ellett, L.D. Development and Psychometric Testing of the Infant Colic Scale. Gastroenterol. Nurs. 2003, 26, 96–103. [Google Scholar] [CrossRef]
- Elliott, L.; Arbes, S.J., Jr.; Harvey, E.S.; Lee, R.C.; Salo, P.M.; Cohn, R.D.; London, S.J.; Zeldin, D.C. Dust weight and asthma prevalence in the National Survey of Lead and Allergens in Housing (NSLAH). Environ. Health Perspect. 2007, 115, 215–220. [Google Scholar] [CrossRef]
- Hicks, S.D.; Confair, A.; Warren, K.; Chandran, D. Levels of breast milk microRNAs and other non-coding RNAs are impacted by milk maturity and maternal diet. Front. Immunol. 2022, 12, 785217. [Google Scholar] [CrossRef]
- Baldassarre, M.E.; Mastromarino, P.; Miccheli, A.; Fanelli, M.; Dileone, A.; Drimaco, P.; Laforgia, N. PS-054 Vsl# 3 Supplementation To Mothers During Pregnancy And Breast Feeding Improves Colics And Regurgitation In Newborns, Perhaps By Tgf-b Modulation. Arch. Dis. Child. 2014, 99, A131–A132. [Google Scholar] [CrossRef] [Green Version]
- Munblit, D.; Treneva, M.; Peroni, D.G.; Colicino, S.; Chow, L.Y.; Dissanayeke, S.; Pampura, A.; Boner, A.L.; Geddes, D.T.; Boyle, R.J.; et al. Immune Components in Human Milk Are Associated with Early Infant Immunological Health Outcomes: A Prospective Three-Country Analysis. Nutrients 2017, 9, 532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewanto, N.E.; Firmansyah, A.; Sungkar, A.; Dharmasetiawani, N.; Sastroasmoro, S.; Kresno, S.B.; Suradi, R.; Bardosono, S.; Prasetyo, D. The effect of Bifidobacterium animalis lactis HNO19 supplementation among pregnant and lactating women on interleukin-8 level in breast milk and infant’s gut mucosal integrity. Med. J. Indones. 2017, 26, 204–211. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, M.A.E.; de Oliveira, G.G.; Oda, J.M.M.; Ono, M.A.; Guembarovski, R.L. Cytokines in Human Breast Milk: Immunological Significance for Newborns. Curr. Nutr. Food Sci. 2012, 8, 2–7. [Google Scholar] [CrossRef]
- Kelleher, S.L.; Gagnon, A.; Rivera, O.C.; Hicks, S.D.; Carney, M.C.; Alam, S. Milk-derived miRNA profiles elucidate molecular pathways that underlie breast dysfunction in women with common genetic variants in SLC30A2. Sci. Rep. 2019, 9, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, S.; Huang, Y.; Wu, Y.; Wu, Y.; Huang, G.; Xiong, J.; You, Y. Curcumin chitosan microsphere improve ulcerative colitis inflammatory response by regulating miR-224-3p/TLR4 axise. Food Sci. Technol. 2022, 14, 42. [Google Scholar] [CrossRef]
- Martínez, C.; Rodiño-Janeiro, B.K.; Lobo, B.; Stanifer, M.L.; Klaus, B.; Granzow, M.; González-Castro, A.M.; Salvo-Romero, E.; Alonso-Cotoner, C.; Pigrau, M.; et al. miR-16 and miR-125b are involved in barrier function dysregulation through the modulation of claudin-2 and cingulin expression in the jejunum in IBS with diarrhoea. Gut 2017, 66, 1537–1538. [Google Scholar] [CrossRef] [Green Version]
- Krishnachaitanya, S.S.; Liu, M.; Fujise, K.; Li, Q. MicroRNAs in inflammatory bowel disease and its complications. Int. J. Mol. Sci. 2022, 23, 8751. [Google Scholar] [CrossRef]
- Sabina, S.; Panico, A.; Mincarone, P.; Leo, C.G.; Garbarino, S.; Grassi, T.; Bagordo, F.; De Donno, A.; Scoditti, E.; Tumolo, M.R. Expression and Biological Functions of miRNAs in Chronic Pain: A Review on Human Studies. Int. J. Mol. Sci. 2022, 23, 6016. [Google Scholar] [CrossRef]
- Chen, Y.H.; Wang, H. The association between depression and gastroesophageal reflux based on phylogenetic analysis of miRNA biomarkers. Curr. Med. Chem. 2020, 38, 6536–6547. [Google Scholar] [CrossRef]
- Johnson, J.M.; Adams, E.D. The gastrointestinal microbiome in infant colic: A scoping review. MCN Am. J. Matern. Nurs. 2022, 47, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, H.; Rodríguez, J.M.; Salminen, S.; Szajewska, H. Probiotics in human milk and probiotic supplementation in infant nutrition: A workshop report. Br. J. Nutr. 2014, 112, 1119–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yi, D.Y.; Kim, S.Y. Human breast milk composition and function in human health: From nutritional components to microbiome and microRNAs. Nutrients 2021, 13, 3094. [Google Scholar] [CrossRef]
- Pannaraj, P.S.; Li, F.; Cerini, C.; Bender, J.M.; Yang, S.; Rollie, A.; Adisetiyo, H.; Zabih, S.; Lincez, P.J.; Bittinger, K.; et al. Association between breast milk bacterial communities and establishment and development of the infant gut microbiome. JAMA Pediatr. 2017, 171, 647–654. [Google Scholar] [CrossRef] [Green Version]
- Szajewska, H.; Gyrczuk, E.; Horvath, A. Lactobacillus reuteri DSM 17938 for the management of infantile colic in breastfed infants: A randomized, double-blind, placebo-controlled trial. J. Pediatr. 2013, 162, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Xiao, X.; Shi, Y.; Wu, Y.; Huang, Y.; Li, D.; Xiong, F.; He, G.; Chai, Y.; Tang, H. Inhibition of miRNA-29a regulates intestinal barrier function in diarrhea-predominant irritable bowel syndrome by upregulating ZO-1 and CLDN1. Exp. Ther. Med. 2020, 20, 1. [Google Scholar] [CrossRef] [PubMed]
- Michielan, A.; D’Incà, R. Intestinal permeability in inflammatory bowel disease: Pathogenesis, clinical evaluation, and therapy of leaky gut. Mediators Inflamm. 2015, 2015, 628157. [Google Scholar] [CrossRef] [Green Version]
- Hirai, C.; Ichiba, H.; Saito, M.; Shintaku, H.; Yamano, T.; Kusuda, S. Trophic effect of multiple growth factors in amniotic fluid or human milk on cultured human fetal small intestinal cells. J. Pediatr. Gastroenterol. Nutr. 2002, 34, 524–528. [Google Scholar] [CrossRef]
- Bauer, J.; Gerss, J. Longitudinal analysis of macronutrients and minerals in human milk produced by mothers of preterm infants. Clin. Nutr. 2011, 30, 215–220. [Google Scholar] [CrossRef]
- Carney, M.C.; Tarasiuk, A.; DiAngelo, S.L.; Silveyra, P.; Podany, A.; Birch, L.L.; Paul, I.M.; Kelleher, S.; Hicks, S.D. Metabolism-related microRNAs in maternal breast milk are influenced by premature delivery. Pediatr. Res. 2017, 82, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Al-Shehri, S.S.; Knox, C.L.; Liley, H.G.; Cowley, D.M.; Wright, J.R.; Henman, M.G.; Hewavitharana, A.K.; Charles, B.G.; Shaw, P.N.; Sweeney, E.L.; et al. Breastmilk-Saliva Interactions Boost Innate Immunity by Regulating the Oral Microbiome in Early Infancy. PLoS ONE 2015, 10, e0135047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhoads, J.M.; Collins, J.; Fatheree, N.Y.; Hashmi, S.S.; Taylor, C.M.; Luo, M.; Hoang, T.K.; Gleason, W.A.; Van Arsdall, M.R.; Navarro, F.; et al. Infant colic represents gut inflammation and dysbiosis. J. Pediatr. 2018, 203, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Pärtty, A.; Kalliomäki, M.; Salminen, S.; Isolauri, E. Infantile colic is associated with low-grade systemic inflammation. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 691–695. [Google Scholar] [CrossRef]
- Chen, L.; Liu, X.; Li, Z.; Wang, J.; Tian, R.; Zhang, H. Integrated Analysis of Transcriptome mRNA and miRNA Profiles Reveals Self-Protective Mechanism of Bovine MECs Induced by LPS. Front. Vet. Sci. 2022, 9, 890043. [Google Scholar] [CrossRef]
- Soeorg, H.; Metsvaht, T.; Eelmäe, I.; Merila, M.; Treumuth, S.; Huik, K.; Jürna-Ellam, M.; Ilmoja, M.L.; Lutsar, I. The role of breast milk in the colonization of neonatal gut and skin with coagulase-negative staphylococci. Pediatr. Res. 2017, 82, 759–767. [Google Scholar] [CrossRef]
- Rimoldi, S.G.; Pileri, P.; Mazzocco, M.I.; Romeri, F.; Bestetti, G.; Calvagna, N.; Tonielli, C.; Fiori, L.; Gigantiello, A.; Pagani, C.; et al. The Role of Staphylococcus aureus in Mastitis: A Multidisciplinary Working Group Experience. J. Hum. Lact. 2020, 36, 503–509. [Google Scholar] [CrossRef]
- Cheng, N.C.; Wang, J.T.; Chang, S.C.; Tai, H.C.; Tang, Y.B. Necrotizing fasciitis caused by Staphylococcus aureus: The emergence of methicillin-resistant strains. Ann. Plast. Surg. 2011, 67, 632–636. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | All (n = 182) | Infant colic (n = 28) | No colic (n = 154) |
|---|---|---|---|
| Medical and demographic characteristics | |||
| Maternal age, years, mean (SD) | 29 (4) | 31 (4) | 29 (4) |
| Female sex, n (%) | 107 (58) | 16 (57) | 91 (59) |
| Vaginal delivery, n (%) | 146 (80) | 20 (71) | 126 (81) |
| Birth weight, grams (IQR) | 3357 (569) | 3283 (454) | 3370 (593) |
| ∆WfL Z-score (0–1 months), mean (SD) | 1.12 (1.5) | 1.29 (1.0) | 1.09 (2.1) |
| Family food allergy, n (%) | 17 (9) | 3 (10) | 14 (9) |
| Social determinants of health | |||
| Infant racial/ethnic minority, n (%) | 43 (23) | 11 (39) * | 32 (20) |
| Family income < federal poverty level, n (%) | 10 (5) | 3 (11) | 7 (4) |
| Married, n (%) | 149 (81) | 21 (75) | 128 (83) |
| Persons in household, median (range) | 4 (2–9) | 4 (2–9) | 4 (2–9) |
| Maternal college diploma, n (%) | 131 (72) | 21 (75) | 110 (71) |
| Private health insurance, n (%) | 157 (86) | 24 (85) | 133 (86) |
| Nutrition factors | |||
| Formula introduced by 1 month, n (%) | 57 (31) | 13 (46) | 44 (28) |
| Maternal vegetables, cups/day mean (IQR) | 1.56 (0.4) | 1.63 (0.6) | 1.55 (0.4) |
| Maternal fruit, cups/day, mean (IQR) | 1.16 (0.6) | 1.26 (0.6) | 1.14 (0.6) |
| Maternal sugar, teaspoon/day mean (IQR) | 18.6 (6) | 21.3 (8) | 18.2 (6) |
| Maternal calcium, mg/day, mean (IQR) | 1055 (232) | 1036 (206) | 1058 (233) |
| Maternal dairy, cups/day, mean (IQR) | 1.89 (0.6) | 1.85 (0.6) | 1.90 (0.5) |
| Human milk factors | |||
| Infant age at collection, days (SD) | 39 (12) | 38 (10) | 39 (12) |
| Time of day at milk collection, hour (SD) | 12 (2) | 12 (3) | 11 (2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandran, D.; Warren, K.; McKeone, D.; Hicks, S.D. The Association between Infant Colic and the Multi-Omic Composition of Human Milk. Biomolecules 2023, 13, 559. https://doi.org/10.3390/biom13030559
Chandran D, Warren K, McKeone D, Hicks SD. The Association between Infant Colic and the Multi-Omic Composition of Human Milk. Biomolecules. 2023; 13(3):559. https://doi.org/10.3390/biom13030559
Chicago/Turabian StyleChandran, Desirae, Kaitlyn Warren, Daniel McKeone, and Steven D. Hicks. 2023. "The Association between Infant Colic and the Multi-Omic Composition of Human Milk" Biomolecules 13, no. 3: 559. https://doi.org/10.3390/biom13030559