
Comparisons of Cytokines, Growth Factors and Clinical Efficacy between Platelet-Rich Plasma and Autologous Conditioned Serum for Knee Osteoarthritis Management
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. PRP and ACS Preparation for Cytokine Measurement
2.3. Statistical Analyses
3. Results
3.1. Comparisons of the Contents between PRP and ACS
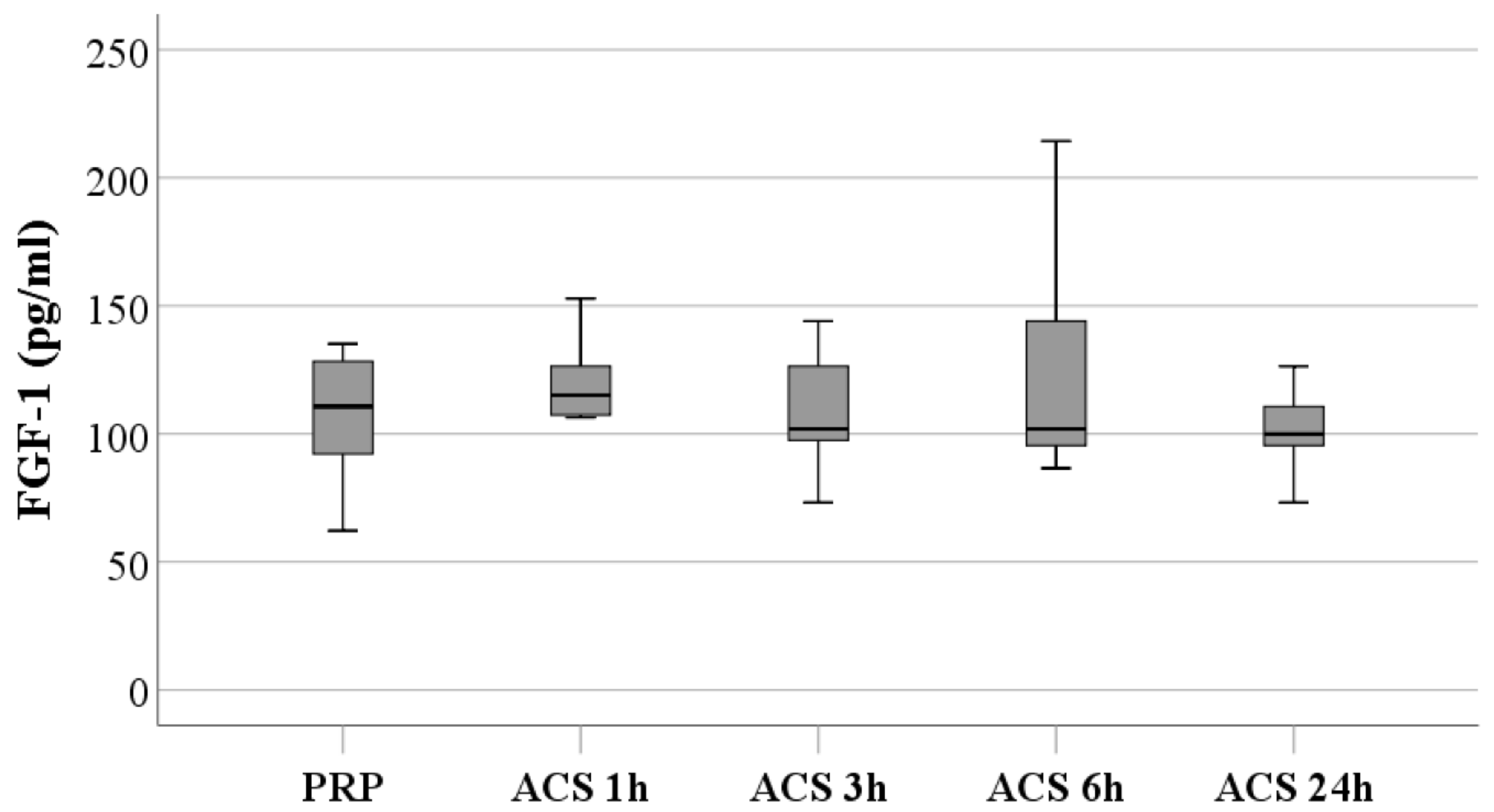
3.1.1. FGF-1 Levels
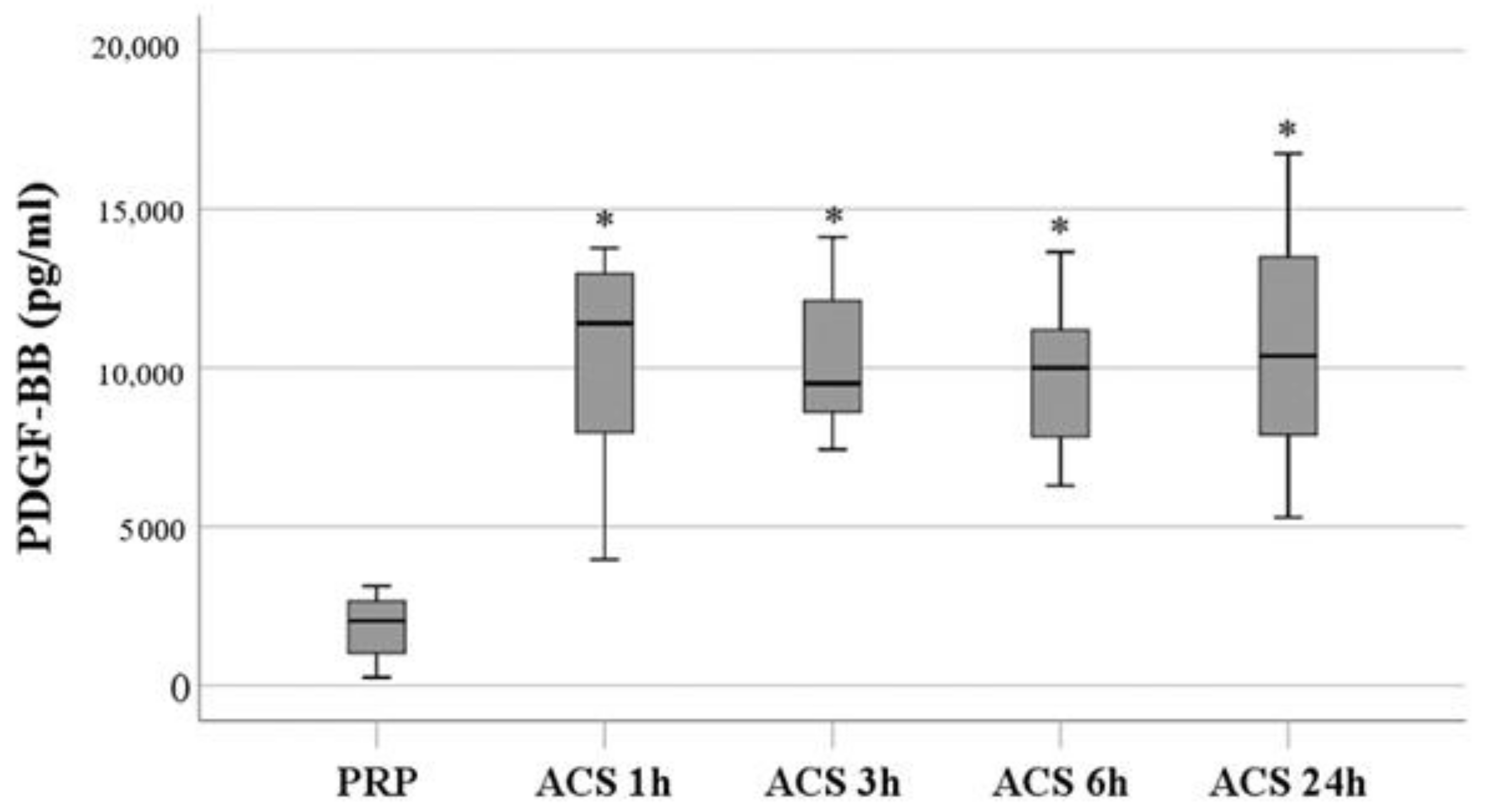
3.1.2. PDGF-BB Levels
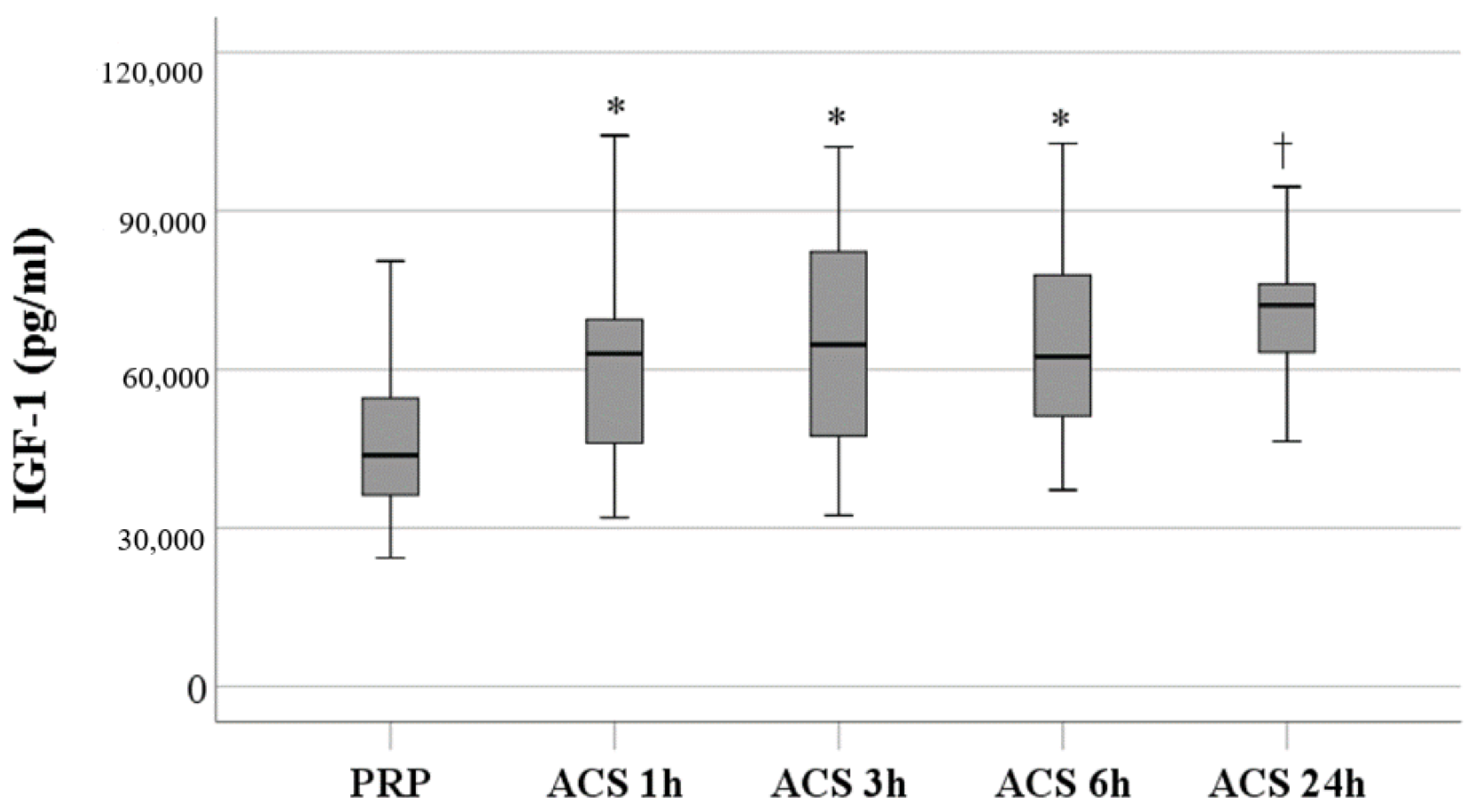
3.1.3. IGF-1 Levels
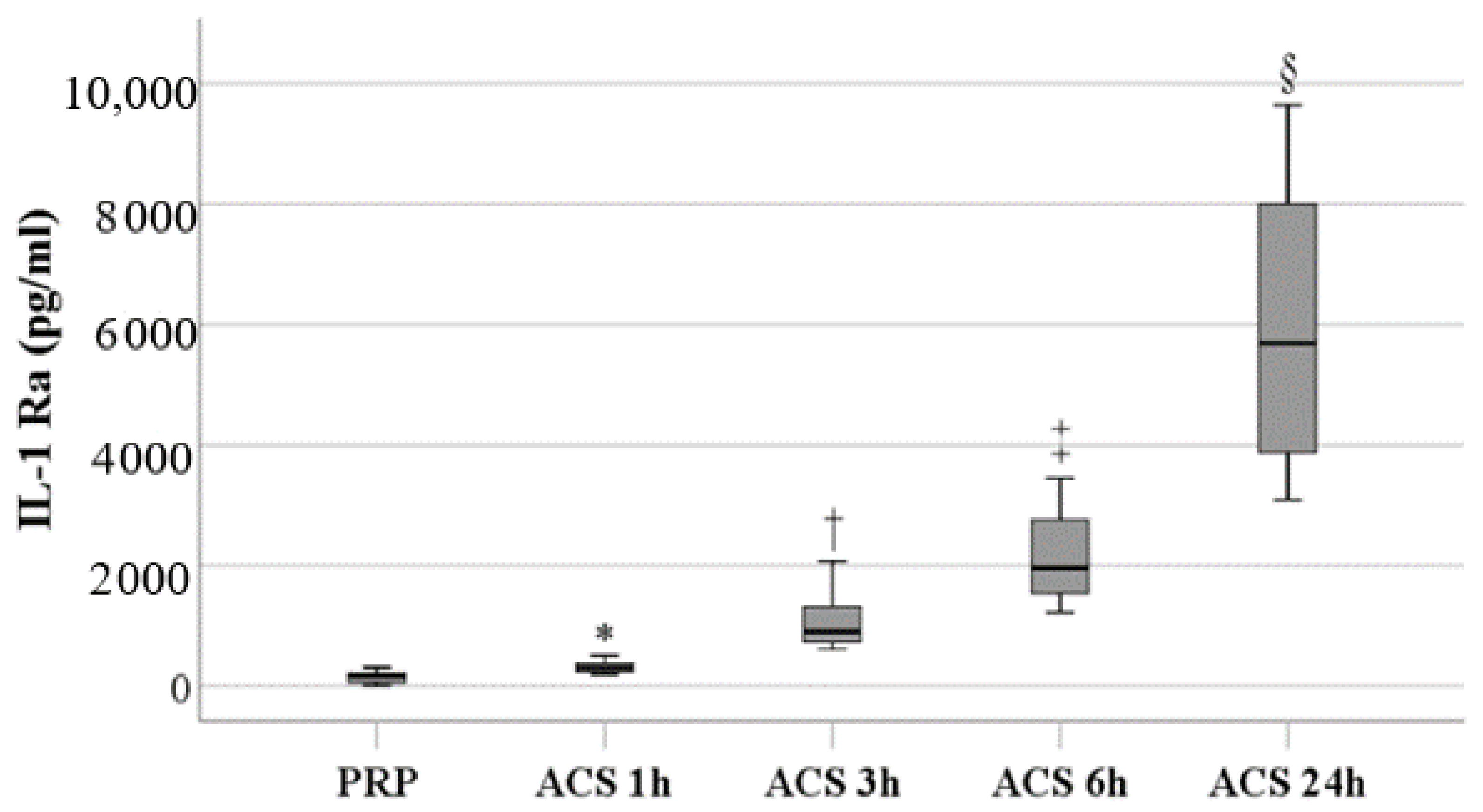
3.1.4. IL-1Ra Levels
3.1.5. TNF-α Levels
3.2. Comparisons of the Efficacy of PRP and ACS Treatment on Pain Relief in Patients with Knee OA
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Safiri, S.; Kolahi, A.-A.; Smith, E.; Hill, C.; Bettampadi, D.; Mansournia, M.A.; Hoy, D.; Ashrafi-Asgarabad, A.; Sepidarkish, M.; Almasi-Hashiani, A.; et al. Global, regional and national burden of osteoarthritis 1990-2017: A systematic analysis of the Global Burden of Disease Study 2017. Ann. Rheum. Dis. 2020, 79, 819–828. [Google Scholar] [CrossRef]
- Nüesch, E.; Dieppe, P.; Reichenbach, S.; Williams, S.; Iff, S.; Jüni, P. All cause and disease specific mortality in patients with knee or hip osteoarthritis: Population based cohort study. BMJ 2011, 342, d1165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brophy, R.H.; Fillingham, Y.A. AAOS Clinical Practice Guideline Summary: Management of Osteoarthritis of the Knee (Nonarthroplasty), Third Edition. JAAOS J. Am. Acad. Orthop. Surg. 2022, 30, e721–e729. [Google Scholar] [CrossRef] [PubMed]
- Goldring, M.B.; Berenbaum, F. Emerging targets in osteoarthritis therapy. Curr. Opin. Pharm. 2015, 22, 51–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berenbaum, F. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthr. Cartil. 2013, 21, 16–21. [Google Scholar] [CrossRef] [Green Version]
- Robinson, W.H.; Lepus, C.M.; Wang, Q.; Raghu, H.; Mao, R.; Lindstrom, T.M.; Sokolove, J. Low-grade inflammation as a key mediator of the pathogenesis of osteoarthritis. Nat. Rev. Rheumatol. 2016, 12, 580–592. [Google Scholar] [CrossRef]
- Bondeson, J.; Wainwright, S.D.; Lauder, S.; Amos, N.; Hughes, C.E. The role of synovial macrophages and macrophage-produced cytokines in driving aggrecanases, matrix metalloproteinases, and other destructive and inflammatory responses in osteoarthritis. Arthritis Res. 2006, 8, R187. [Google Scholar] [CrossRef] [Green Version]
- Hill, C.L.; Hunter, D.J.; Niu, J.; Clancy, M.; Guermazi, A.; Genant, H.; Gale, D.; Grainger, A.; Conaghan, P.; Felson, D.T. Synovitis detected on magnetic resonance imaging and its relation to pain and cartilage loss in knee osteoarthritis. Ann. Rheum. Dis. 2007, 66, 1599–1603. [Google Scholar] [CrossRef] [Green Version]
- Baker, K.; Grainger, A.; Niu, J.; Clancy, M.; Guermazi, A.; Crema, M.; Hughes, L.; Buckwalter, J.; Wooley, A.; Nevitt, M.; et al. Relation of synovitis to knee pain using contrast-enhanced MRIs. Ann. Rheum. Dis. 2010, 69, 1779–1783. [Google Scholar] [CrossRef] [Green Version]
- Sowers, M.; Karvonen-Gutierrez, C.A.; Jacobson, J.A.; Jiang, Y.; Yosef, M. Associations of anatomical measures from MRI with radiographically defined knee osteoarthritis score, pain, and physical functioning. J. Bone Jt. Surg. Am. 2011, 93, 241–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapoor, M.; Martel-Pelletier, J.; Lajeunesse, D.; Pelletier, J.P.; Fahmi, H. Role of proinflammatory cytokines in the pathophysiology of osteoarthritis. Nat. Rev. Rheumatol. 2011, 7, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Wojdasiewicz, P.; Poniatowski, Ł.A.; Szukiewicz, D. The role of inflammatory and anti-inflammatory cytokines in the pathogenesis of osteoarthritis. Mediat. Inflamm. 2014, 2014, 561459. [Google Scholar] [CrossRef] [Green Version]
- Huang, G.; Hua, S.; Yang, T.; Ma, J.; Yu, W.; Chen, X. Platelet-rich plasma shows beneficial effects for patients with knee osteoarthritis by suppressing inflammatory factors. Exp. Ther. Med. 2018, 15, 3096–3102. [Google Scholar] [CrossRef] [Green Version]
- Kubrova, E.; D’Souza, R.S.; Hunt, C.L.; Wang, Q.; van Wijnen, A.J.; Qu, W. Injectable Biologics: What Is the Evidence? Am. J. Phys. Med. Rehabil. 2020, 99, 950–960. [Google Scholar] [CrossRef] [PubMed]
- Vakharia, R.M.; Roche, M.W.; Alcerro, J.C.; Lavernia, C.J. The Current Status of Cell-Based Therapies for Primary Knee Osteoarthritis. Orthop. Clin. North Am. 2019, 50, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Zhang, C.; Tuan, R.S. Biology of platelet-rich plasma and its clinical application in cartilage repair. Arthritis Res. Ther. 2014, 16, 204. [Google Scholar] [CrossRef] [Green Version]
- Fu, C.J.; Sun, J.B.; Bi, Z.G.; Wang, X.M.; Yang, C.L. Evaluation of platelet-rich plasma and fibrin matrix to assist in healing and repair of rotator cuff injuries: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 158–172. [Google Scholar] [CrossRef]
- Laudy, A.B.; Bakker, E.W.; Rekers, M.; Moen, M.H. Efficacy of platelet-rich plasma injections in osteoarthritis of the knee: A systematic review and meta-analysis. Br. J. Sport. Med. 2015, 49, 657–672. [Google Scholar] [CrossRef] [Green Version]
- Battaglia, M.; Guaraldi, F.; Vannini, F.; Rossi, G.; Timoncini, A.; Buda, R.; Giannini, S. Efficacy of ultrasound-guided intra-articular injections of platelet-rich plasma versus hyaluronic acid for hip osteoarthritis. Orthopedics 2013, 36, e1501–e1508. [Google Scholar] [CrossRef] [Green Version]
- Riewruja, K.; Phakham, S.; Sompolpong, P.; Reantragoon, R.; Tanavalee, A.; Ngarmukos, S.; Udomsinprasert, W.; Suantawee, T.; Dechsupa, S.; Honsawek, S. Cytokine Profiling and Intra-Articular Injection of Autologous Platelet-Rich Plasma in Knee Osteoarthritis. Int. J. Mol. Sci. 2022, 23, 890. [Google Scholar] [CrossRef] [PubMed]
- Cook, C.S.; Smith, P.A. Clinical Update: Why PRP Should Be Your First Choice for Injection Therapy in Treating Osteoarthritis of the Knee. Curr. Rev. Musculoskelet. Med. 2018, 11, 583–592. [Google Scholar] [CrossRef]
- Pachito, D.V.; Latorraca, C.O.C.; Riera, R. Efficacy of platelet-rich plasma for non-transfusion use: Overview of systematic reviews. Int. J. Clin. Pr. 2019, 73, e13402. [Google Scholar] [CrossRef]
- Navani, A.; Li, G.; Chrystal, J. Platelet Rich Plasma in Musculoskeletal Pathology: A Necessary Rescue or a Lost Cause? Pain Physician 2017, 20, E345–E356. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Huang, H.; Liang, G.; Zeng, L.F.; Yang, W.; Liu, J. Effects and safety of the combination of platelet-rich plasma (PRP) and hyaluronic acid (HA) in the treatment of knee osteoarthritis: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2020, 21, 224. [Google Scholar] [CrossRef] [Green Version]
- Dai, W.L.; Zhou, A.G.; Zhang, H.; Zhang, J. Efficacy of Platelet-Rich Plasma in the Treatment of Knee Osteoarthritis: A Meta-analysis of Randomized Controlled Trials. Arthroscopy 2017, 33, 659–670. [Google Scholar] [CrossRef]
- Baltzer, A.W.; Moser, C.; Jansen, S.A.; Krauspe, R. Autologous conditioned serum (Orthokine) is an effective treatment for knee osteoarthritis. Osteoarthr. Cartil. 2009, 17, 152–160. [Google Scholar] [CrossRef] [Green Version]
- Meijer, H.; Reinecke, J.; Becker, C.; Tholen, G.; Wehling, P. The production of anti-inflammatory cytokines in whole blood by physico-chemical induction. Inflamm. Res. 2003, 52, 404–407. [Google Scholar] [CrossRef]
- Darabos, N.; Haspl, M.; Moser, C.; Darabos, A.; Bartolek, D.; Groenemeyer, D. Intraarticular application of autologous conditioned serum (ACS) reduces bone tunnel widening after ACL reconstructive surgery in a randomized controlled trial. Knee Surg. Sport. Traumatol. Arthrosc. 2011, 19 (Suppl. S1), S36–S46. [Google Scholar] [CrossRef]
- Vitali, M.; Ometti, M.; Drossinos, A.; Pironti, P.; Santoleri, L.; Salini, V. Autologous conditioned serum: Clinical and functional results using a novel disease modifying agent for the management of knee osteoarthritis. J. Drug Assess. 2020, 25, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Goldring, M.B. Anticytokine therapy for osteoarthritis. Expert. Opin. Biol. 2001, 1, 817–829. [Google Scholar] [CrossRef] [PubMed]
- Frizziero, A.; Giannotti, E.; Oliva, F.; Masiero, S.; Maffulli, N. Autologous conditioned serum for the treatment of osteoarthritis and other possible applications in musculoskeletal disorders. Br. Med. Bull. 2013, 105, 169–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barreto, A.; Braun, T.R. A new treatment for knee osteoarthritis: Clinical evidence for the efficacy of Arthrokinex™ autologous conditioned serum. J. Orthop. 2016, 14, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Baselga García-Escudero, J.; Miguel Hernández Trillos, P. Treatment of Osteoarthritis of the Knee with a Combination of Autologous Conditioned Serum and Physiotherapy: A Two-Year Observational Study. PLoS ONE 2015, 10, e0145551. [Google Scholar] [CrossRef] [PubMed]
- Shirokova, L.; Noskov, S.; Gorokhova, V.; Reinecke, J.; Shirokova, K. Intra-Articular Injections of a Whole Blood Clot Secretome, Autologous Conditioned Serum, Have Superior Clinical and Biochemical Efficacy Over Platelet-Rich Plasma and Induce Rejuvenation-Associated Changes of Joint Metabolism: A Prospective, Controlled Open-Label Clinical Study in Chronic Knee Osteoarthritis. Rejuvenation Res. 2020, 23, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Akan, O.; Sarikaya, N.O.; Kocyigit, H. Efficacy of platelet-rich plasma administration in patients with severe knee osteoarthritis: Can platelet-rich plasma administration delay arthroplasty in this patient population? Int. J. Clin. Exp. Med. 2018, 11, 9473–9483. [Google Scholar]
- Görmeli, G.; Görmeli, C.A.; Ataoglu, B.; Çolak, C.; Aslantürk, O.; Ertem, K. Multiple PRP injections are more effective than single injections and hyaluronic acid in knees with early osteoarthritis: A randomized, double-blind, placebo-controlled trial. Knee Surg. Sport. Traumatol. Arthrosc. 2017, 25, 958–965. [Google Scholar] [CrossRef]
- Rayegani, S.M.; Raeissadat, S.A.; Taheri, M.S.; Babaee, M.; Bahrami, M.H.; Eliaspour, D.; Ghorbani, E. Does intra articular platelet rich plasma injection improve function, pain and quality of life in patients with osteoarthritis of the knee? A randomized clinical trial. Orthop. Rev. 2014, 6, 5405. [Google Scholar] [CrossRef] [Green Version]
- Subramanyam, K.; Alguvelly, R.; Mundargi, A.; Khanchandani, P. Single versus multi-dose intra-articular injection of platelet rich plasma in early stages of osteoarthritis of the knee: A single-blind, randomized, superiority trial. Arch. Rheumatol. 2021, 36, 326–334. [Google Scholar] [CrossRef]
- Ngarmukos, S.; Tanavalee, C.; Amarase, C.; Phakham, S.; Mingsiritham, W.; Reantragoon, R.; Leearamwat, N.; Kongkaew, T.; Tharakhet, K.; Honsawek, S.; et al. Two or four injections of platelet-rich plasma for osteoarthritic knee did not change synovial biomarkers but similarly improved clinical outcomes. Sci. Rep. 2021, 11, 23603. [Google Scholar] [CrossRef]
- Li, Y.; Mai, Y.; Cao, P.; Wen, X.; Fan, T.; Wang, X.; Ruan, G.; Tang, S.; Ding, C.; Zhu, Z. Relative Efficacy and Safety of Anti-Inflammatory Biologic Agents for Osteoarthritis: A Conventional and Network Meta-Analysis. J. Clin. Med. 2022, 11, 3958. [Google Scholar] [CrossRef]
- Wehling, P.; Moser, C.; Frisbie, D.; McIlwraith, C.W.; Kawcak, C.E.; Krauspe, R.; Reinecke, J.A. Autologous conditioned serum in the treatment of orthopedic diseases: The orthokine therapy. BioDrugs 2007, 21, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Camargo Garbin, L.; Morris, M.J. A Comparative Review of Autologous Conditioned Serum and Autologous Protein Solution for Treatment of Osteoarthritis in Horses. Front. Vet. Sci. 2021, 8, 602978. [Google Scholar] [CrossRef]
- Rutgers, M.; Saris, D.B.; Dhert, W.J.; Creemers, L.B. Cytokine profile of autologous conditioned serum for treatment of osteoarthritis, in vitro effects on cartilage metabolism and intra-articular levels after injection. Arthritis Res. 2010, 12, R114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeda, Y.; Hiraishi, K.; Takeda, H.; Shiobara, N.; Shibusawa, H.; Saniabadi, A.R.; Adachi, M.; Kawata, S. Cellulose acetate beads induce release of interleukin-1 receptor antagonist, but not tumour necrosis factor-alpha or interleukin-1beta in human peripheral blood. Inflamm. Res. 2003, 52, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Magalon, J.; Bausset, O.; Veran, J.; Giraudo, L.; Serratrice, N.; Magalon, G.; Dignat-George, F.; Sabatier, F. Physico-chemical factors influencing autologous conditioned serum purification. Biores. Open Access 2014, 3, 35–38. [Google Scholar] [CrossRef]
- Leone, R.; de Rosa, A.; Iudicone, P.; Fioravanti, D.; Capua, G.; Rossetti, F.; Isgro, M.A.; Pierelli, L. Pain control and functional improvement in patients treated by autologous conditioned serum after failure of platelet rich plasma treatments in knee osteoarthritis. Transfus. Med. 2021, 31, 357–364. [Google Scholar] [CrossRef]
- Khurana, A.; Goyal, A.; Kirubakaran, P.; Akhand, G.; Gupta, R.; Goel, N. Efficacy of Autologous Conditioned Serum (ACS), Platelet-Rich Plasma (PRP), Hyaluronic Acid (HA) and Steroid for Early Osteoarthritis Knee: A Comparative Analysis. Indian J. Orthop. 2021, 55, 217–227. [Google Scholar] [CrossRef]
- Pishgahi, A.; Abolhasan, R.; Shakouri, S.K.; Soltani-Zangbar, M.S.; Dareshiri, S.; Ranjbar Kiyakalayeh, S.; Khoeilar, A.; Zamani, M.; Motavalli Khiavi, F.; Pourabbas Kheiraddin, B.; et al. Effect of Dextrose Prolotherapy, Platelet Rich Plasma and Autologous Conditioned Serum on Knee Osteoarthritis: A Randomized Clinical Trial. Iran. J. Allergy Asthma Immunol. 2020, 19, 243–252. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PRP (n = 30) | ACS (n = 30) | p-Value | |
|---|---|---|---|
| Sex, male | 6 (20.0%) | 9 (30.0%) | 0.552 |
| Age (year) | 65.0 (60.0, 70.0) | 67.5 (59.0, 71.0) | 0.554 |
| BMI (kg/m2) | 23.8 (21.7, 27.8) | 26.9 (24.0, 28.5) | 0.064 |
| Treatment side | 0.052 | ||
| Bilateral | 30 (100.0%) | 25 (83.3%) | |
| Left | 0 (0.0%) | 4 (13.3%) | |
| Right | 0 (0.0%) | 1 (3.3%) | |
| Pain duration (month) | 24.0 (12.0, 36.0) | 18.0 (12.0, 30.0) | 0.099 |
| Previous treatment * | |||
| Tropical medicine | 0 (0.0%) | 2 (6.7%) | 0.492 |
| Oral medicine | 5 (16.7%) | 8 (26.7%) | 0.532 |
| Rehibition | 2 (6.7%) | 2 (6.7%) | >0.999 |
| Physical therapy | 0 (0.0%) | 1 (3.3%) | >0.999 |
| Manual Therapy | 1 (3.3%) | 0 (0.0%) | >0.999 |
| Acupuncture | 4 (13.3%) | 1 (3.3%) | 0.353 |
| Acupotomy | 1 (3.3%) | 0 (0.0%) | >0.999 |
| Hyaluronic acid | 2 (6.7%) | 10 (33.3%) | 0.021 † |
| Glucose | 0 (0.0%) | 1 (3.3%) | >0.999 |
| PRP | 1 (3.3%) | 1 (3.3%) | >0.999 |
| Nutritional supplements | 4 (13.3%) | 1 (3.3%) | 0.353 |
| None | 13 (43.3%) | 8 (26.7%) | 0.279 |
| Treatment at baseline | |||
| Oral medicine | 11 (36.7%) | 11 (36.7%) | >0.999 |
| Rehabilitation | 4 (13.3%) | 10 (33.3%) | 0.125 |
| PRP (n = 30) | ACS (n = 30) | p-Value | |
|---|---|---|---|
| Pain VAS at baseline | 6.0 (4.0, 8.0) | 7.0 (6.0, 8.0) | 0.098 |
| Pain VAS at the end of the study | 1.0 (1.0, 2.0) | 1.0 (0.0, 2.0) | 0.822 |
| Change of pain VAS from baseline | −4.0 (−6.0, −2.0) | −5.0 (−7.0, −4.0) | 0.028 † |
| After which injection the patients reported improvement | <0.001 † | ||
| 1st | 14 (46.7%) | 2 (6.7%) | |
| 2nd | 10 (33.3%) | 1 (3.3%) | |
| 3rd | 5 (16.7%) | 13 (43.3%) | |
| 4th | 0 (0.0%) | 4 (13.3%) | |
| 5th | 1 (3.3%) | 10 (33.3%) | |
| Still feel pain at the end of the study | 6 (20.0%) | 18 (60.0%) | 0.003 † |
| Still need oral medicine at the end of the study | 3 (10.0%) | 13 (43.3%) | 0.007 † |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, P.-G.; Yang, K.D.; Huang, L.-G.; Wang, C.-H.; Ko, W.-S. Comparisons of Cytokines, Growth Factors and Clinical Efficacy between Platelet-Rich Plasma and Autologous Conditioned Serum for Knee Osteoarthritis Management. Biomolecules 2023, 13, 555. https://doi.org/10.3390/biom13030555
Cheng P-G, Yang KD, Huang L-G, Wang C-H, Ko W-S. Comparisons of Cytokines, Growth Factors and Clinical Efficacy between Platelet-Rich Plasma and Autologous Conditioned Serum for Knee Osteoarthritis Management. Biomolecules. 2023; 13(3):555. https://doi.org/10.3390/biom13030555
Chicago/Turabian StyleCheng, Pen-Gang, Kuender D. Yang, Liang-Gie Huang, Chi-Hui Wang, and Wang-Sheng Ko. 2023. "Comparisons of Cytokines, Growth Factors and Clinical Efficacy between Platelet-Rich Plasma and Autologous Conditioned Serum for Knee Osteoarthritis Management" Biomolecules 13, no. 3: 555. https://doi.org/10.3390/biom13030555