

Predictive Value of Collagen Biomarkers in Advanced Chronic Kidney Disease Patients
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design
2.3. Demographic, Biochemical, and Echocardiography Parameters
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Survival Analysis
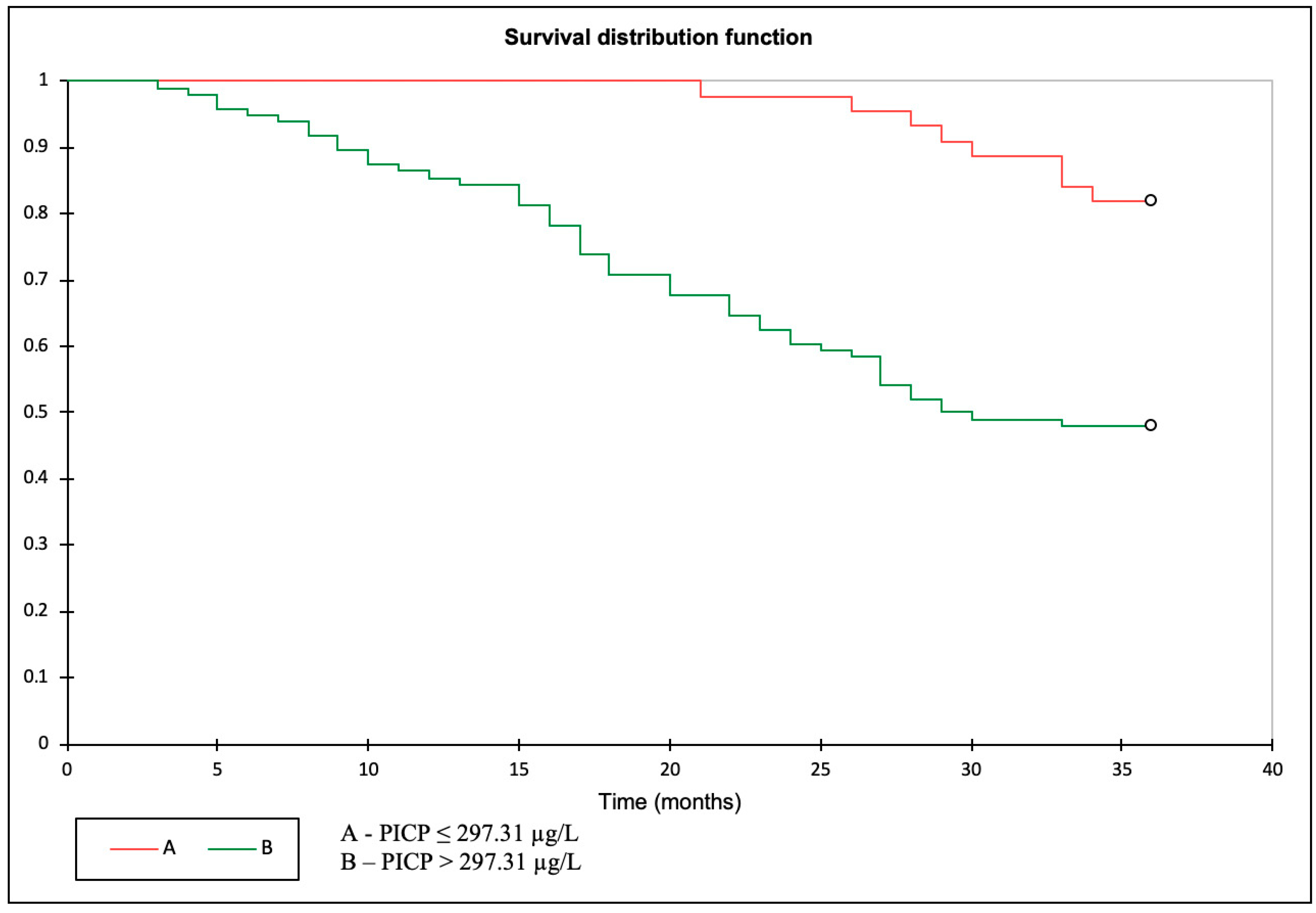
3.3. Primary Outcome: PICP as a Predictor of All-Cause Mortality
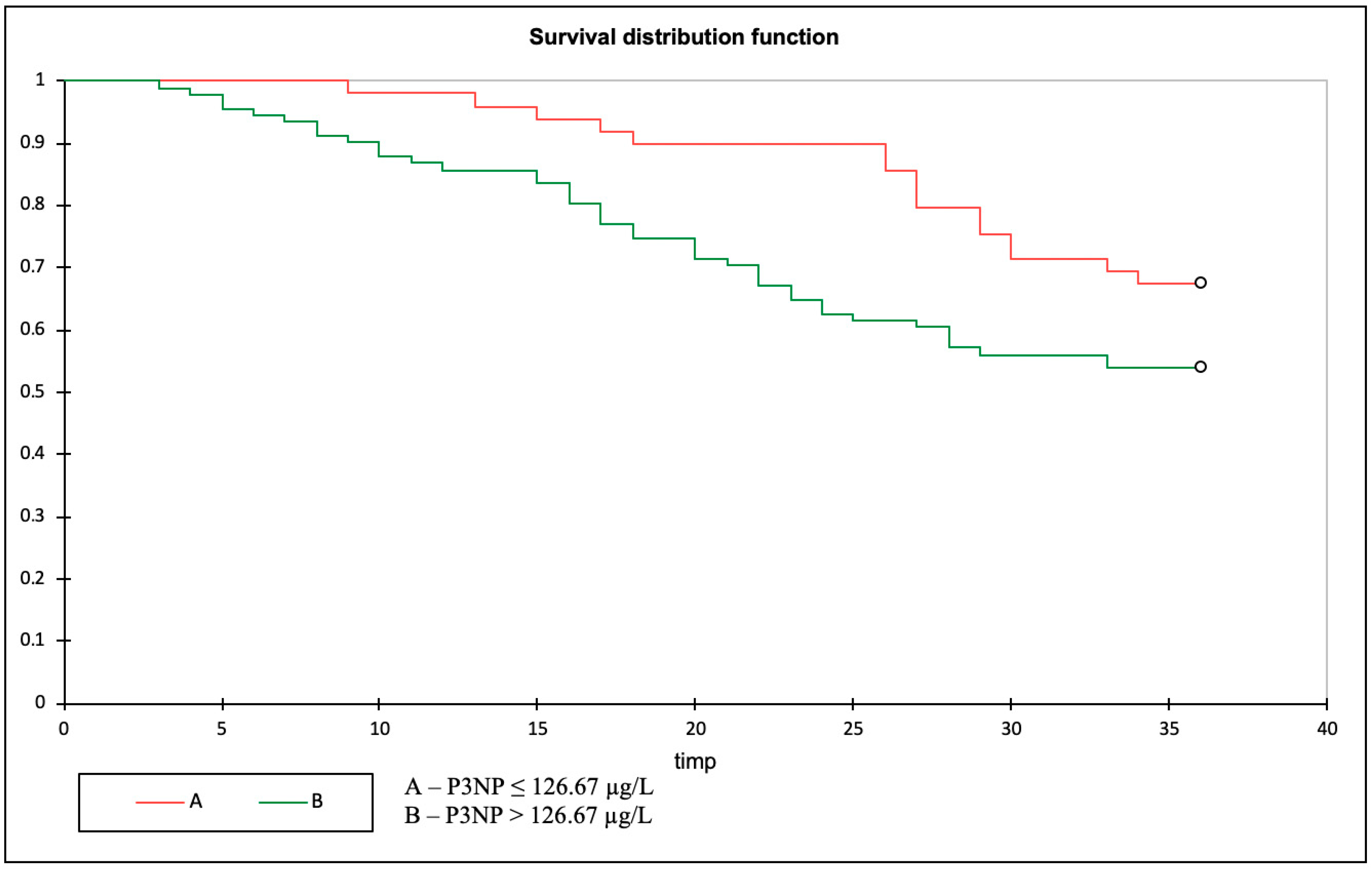
3.4. Primary Outcome: P3NP as a Predictor of All-Cause Mortality
3.5. Patient Phenotype According to PICP and P3NP Levels
3.6. Univariate Analysis and Multivariate Cox Proportional Hazards Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- United States Renal Data System. 2022 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2022. [Google Scholar]
- Racki, S.; Zaputović, L.; Mavrić, Z.; Vujicić, B.; Dvornik, S. C-reactive protein is a strong predictor of mortality in hemodialysis patients. Ren. Fail. 2006, 28, 427–433. [Google Scholar] [CrossRef]
- Michos, E.D.; Wilson, L.M.; Yeh, H.C.; Berger, Z.; Suarez-Cuervo, C.; Stacy, S.R.; Bass, E.B. Prognostic value of cardiac troponin in patients with chronic kidney disease without suspected acute coronary syndrome: A systematic review and meta-analysis. Ann. Intern. Med. 2014, 161, 491–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paniagua, R.; Ventura, M.D.; Avila-Díaz, M.; Hinojosa-Heredia, H.; Méndez-Durán, A.; Cueto-Manzano, A.; Cisneros, A.; Ramos, A.; Madonia-Juseino, C.; Belio-Caro, F.; et al. NT-proBNP, fluid volume overload and dialysis modality are independent predictors of mortality in ESRD patients. Nephrol. Dial. Transplant. 2010, 25, 551–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, Y.B.; Lee, M.J.; Park, J.T.; Han, S.H.; Kang, S.-W.; Yoo, T.-H.; Kim, H.J. Prognostic value of soluble ST2 and soluble LR11 on mortality and cardiovascular events in peritoneal dialysis patients. BMC Nephrol. 2020, 21, 228. [Google Scholar] [CrossRef]
- Plawecki, M.; Morena, M.; Kuster, N.; Chenine, L.; Leray-Moragues, H.; Jover, B.; Fesler, P.; Lotierzo, M.; Dupuy, A.M.; Klouche, K.; et al. sST2 as a New Biomarker of Chronic Kidney Disease-Induced Cardiac Remodeling: Impact on Risk Prediction. Mediat. Inflamm. 2018, 2018, 3952526. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Cao, S.; Yang, H.; Li, J. Prognostic impact of galectin-3 in chronic kidney disease patients: A systematic review and meta-analysis. Int. Urol. Nephrol. 2019, 51, 1005–1011. [Google Scholar] [CrossRef]
- Golembiewska, E.; Machowska, A.; Stenvinkel, P.; Lindholm, B. Prognostic Value of Copeptin in Chronic Kidney Disease: From General Population to End-Stage Renal Disease. Curr. Protein Pept. Sci. 2017, 18, 1232–1243. [Google Scholar] [CrossRef]
- Duprez, D.A.; Gross, M.D.; Sanchez, O.A.; Kizer, J.R.; Ix, J.H.; Lima, J.; Tracy, R.P.; Jacobs, D.R., Jr. Collagen Turnover Markers in Relation to Future Cardiovascular and Noncardiovascular Disease: The Multi-Ethnic Study of Atherosclerosis. Clin. Chem. 2017, 63, 1237–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Distler, J.H.W.; Györfi, A.H.; Ramanujam, M.; Whitfield, M.L.; Königshoff, M.; Lafyatis, R. Shared and distinct mechanisms of fibrosis. Nat. Rev. Rheumatol. 2019, 15, 705–730. [Google Scholar] [CrossRef]
- Djudjaj, S.; Boor, P. Cellular and molecular mechanisms of kidney fibrosis. Mol. Aspects Med. 2019, 65, 16–36. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Randive, R.; Stewart, J.A. Molecular mechanisms of AGE/RAGE-mediated fibrosis in the diabetic heart. World J. Diabetes 2014, 5, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Panizo, S.; Barrio-Vázquez, S.; Naves-Díaz, M.; Carrillo-López, N.; Rodríguez, I.; Fernández-Vázquez, A.; Valdivielso, J.M.; Thadhani, R.; Cannata-Andía, J.B. Vitamin D receptor activation, left ventricular hypertrophy and myocardial fibrosis. Nephrol. Dial. Transplant. 2013, 28, 2735–2744. [Google Scholar] [CrossRef] [Green Version]
- Duprez, D.A.; Heckbert, S.R.; Alonso, A.; Gross, M.D.; Ix, J.H.; Kizer, J.R.; Tracy, R.P.; Kronmal, R.; Jacobs, D.R., Jr. Collagen Biomarkers and Incidence of New Onset of Atrial Fibrillation in Subjects With No Overt Cardiovascular Disease at Baseline: The Multi-Ethnic Study of Atherosclerosis. Circ. Arrhythm. Electrophysiol. 2018, 11, e006557. [Google Scholar] [CrossRef] [PubMed]
- Duprez, D.A.; Gross, M.D.; Kizer, J.R.; Ix, J.H.; Hundley, W.G.; Jacobs, D.R., Jr. Predictive Value of Collagen Biomarkers for Heart Failure With and Without Preserved Ejection Fraction: MESA (Multi-Ethnic Study of Atherosclerosis). J. Am. Heart Assoc. 2018, 7, e007885. [Google Scholar] [CrossRef] [PubMed]
- Eiros, R.; Romero-González, G.; Gavira, J.J.; Beloqui, O.; Colina, I.; Fortún Landecho, M.; López, B.; González, A.; Díez, J.; Ravassa, S. Does Chronic Kidney Disease Facilitate Malignant Myocardial Fibrosis in Heart Failure with Preserved Ejection Fraction of Hypertensive Origin? J. Clin. Med. 2020, 9, 404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, C.T.; Liu, Y.W.; Lin, J.W.; Chen, S.I.; Yang, C.S.; Chen, J.H.; Hung, K.Y.; Tsai, W.C.; Huang, J.W. Increased procollagen type I C-terminal peptide levels indicate diastolic dysfunction in end-stage renal disease patients undergoing maintenance dialysis therapy. J. Am. Soc. Echocardiogr. 2012, 25, 895–901. [Google Scholar] [CrossRef]
- Salib, M.; Girerd, S.; Girerd, N.; März, W.; Scharnagl, H.; Massy, Z.A.; Leroy, C.; Duarte, K.; Holdaas, H.; Jardine, A.G.; et al. Serum markers of fibrosis, cardiovascular and all-cause mortality in hemodialysis patients: The AURORA trial. Clin. Res. Cardiol. 2022, 111, 614–626. [Google Scholar] [CrossRef]
- Lieb, W.; Song, R.J.; Xanthakis, V.; Vasan, R.S. Association of Circulating Tissue Inhibitor of Metalloproteinases-1 and Procollagen Type III Aminoterminal Peptide Levels With Incident Heart Failure and Chronic Kidney Disease. J. Am. Heart Assoc. 2019, 8, e011426. [Google Scholar] [CrossRef] [Green Version]
- Ghoul, B.E.; Squalli, T.; Servais, A.; Elie, C.; Meas-Yedid, V.; Trivint, C.; Vanmassenhove, J.; Grünfeld, J.P.; Olivo-Marin, J.C.; Thervet, E.; et al. Urinary procollagen III aminoterminal propeptide (PIIINP): A fibrotest for the nephrologist. Clin. J. Am. Soc. Nephrol. 2010, 5, 205–210. [Google Scholar] [CrossRef] [Green Version]
- Genovese, F.; Rasmussen, D.G.K.; Karsdal, M.A.; Jesky, M.; Ferro, C.; Fenton, A.; Cockwell, P. Imbalanced turnover of collagen type III is associated with disease progression and mortality in high-risk chronic kidney disease patients. Clin. Kidney J. 2021, 14, 593–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Contal, C.; O’Quigley, J. An application of changepoint methods in studying the effect of age on survival in breast cancer. Comput. Stat. Data Anal. 1999, 30, 253–270. [Google Scholar] [CrossRef]
- Löfsjögård, J.; Kahan, T.; Díez, J.; López, B.; González, A.; Ravassa, S.; Mejhert, M.; Edner, M.; Persson, H. Usefulness of Collagen Carboxy-Terminal Propeptide and Telopeptide to Predict Disturbances of Long-Term Mortality in Patients ≥60 Years with Heart Failure and Reduced Ejection Fraction. Am. J. Cardiol. 2017, 119, 2042–2048. [Google Scholar] [CrossRef]
- Saggese, G.; Bertelloni, S.; Baroncelli, G.I.; Di Nero, G. Serum levels of carboxyterminal propeptide of type I procollagen in healthy children from 1st year of life to adulthood and in metabolic bone diseases. Eur. J. Pediatr. 1992, 151, 764–768. [Google Scholar] [CrossRef]
- Magga, J.; Puhakka, M.; Hietakorpi, S.; Punnonen, K.; Uusimaa, P.; Risteli, J.; Vuolteenaho, O.; Ruskoaho, H.; Peuhkurinen, K. Atrial natriuretic peptide, B-type natriuretic peptide, and serum collagen markers after acute myocardial infarction. J. Appl. Physiol. 2004, 96, 1306–1311. [Google Scholar] [CrossRef] [Green Version]
- Tonelli, M.; Karumanchi, S.A.; Thadhani, R. Epidemiology and Mechanisms of Uremia-Related Cardiovascular Disease. Circulation 2016, 133, 518–536. [Google Scholar] [CrossRef]
- Khan, S.; Subedi, D.; Chowdhury, M.M. Use of amino terminal type III procollagen peptide (P3NP) assay in methotrexate therapy for psoriasis. Postgrad. Med. J. 2006, 82, 353–354. [Google Scholar] [CrossRef] [Green Version]
- Su, Y.; Gu, H.; Weng, D.; Zhou, Y.; Li, Q.; Zhang, F.; Zhang, Y.; Shen, L.; Hu, Y.; Li, H. Association of serum levels of laminin, type IV collagen, procollagen III N-terminal peptide, and hyaluronic acid with the progression of interstitial lung disease. Medicine 2017, 96, e6617. [Google Scholar] [CrossRef]
- Zheng, M.; Cai, W.M.; Weng, H.L.; Liu, R.H. ROC curves in evaluation of serum fibrosis indices for hepatic fibrosis. World J. Gastroenterol. 2002, 8, 1073–1076. [Google Scholar] [CrossRef]
- Agarwal, I.; Glazer, N.L.; Barasch, E.; Biggs, M.L.; Djoussé, L.; Fitzpatrick, A.L.; Gottdiener, J.S.; Ix, J.H.; Kizer, J.R.; Rimm, E.B.; et al. Fibrosis-related biomarkers and risk of total and cause-specific mortality: The cardiovascular health study. Am. J. Epidemiol. 2014, 179, 1331–1339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santanasto, A.J.; Cvejkus, R.K.; Wojczynski, M.K.; Marron, M.M.; Schupf, N.; Christensen, K.; Thyagarajan, B.; Zmuda, J.M. Circulating Procollagen Type III N-Terminal Peptide and Physical Function in Adults from the Long Life Family Study. J. Gerontol. A Biol. Sci. Med. Sci. 2021, 76, 1273–1279. [Google Scholar] [CrossRef] [PubMed]
- Dupuy, A.M.; Kuster, N.; Curinier, C.; Huet, F.; Plawecki, M.; Solecki, K.; Roubille, F.; Cristol, J.P. Exploring collagen remodeling and regulation as prognosis biomarkers in stable heart failure. Clin. Chim. Acta 2019, 490, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Zannad, F.; Alla, F.; Dousset, B.; Perez, A.; Pitt, B. Limitation of excessive extracellular matrix turnover may contribute to survival benefit of spironolactone therapy in patients with congestive heart failure: Insights from the randomized aldactone evaluation study (RALES). Rales Investigators. Circulation 2000, 102, 2700–2706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, J.P.; Rossignol, P.; Pizard, A.; Machu, J.L.; Collier, T.; Girerd, N.; Huby, A.C.; Gonzalez, A.; Diez, J.; López, B.; et al. Potential spironolactone effects on collagen metabolism biomarkers in patients with uncontrolled blood pressure. Heart 2019, 105, 307–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuttle, K.R.; Bakris, G.L.; Bilous, R.W.; Chiang, J.L.; de Boer, I.H.; Goldstein-Fuchs, J.; Hirsch, I.B.; Kalantar-Zadeh, K.; Narva, A.S.; Navaneethan, S.D.; et al. Diabetic kidney disease: A report from an ADA Consensus Conference. Diabetes Care 2014, 37, 2864–2883. [Google Scholar] [CrossRef] [Green Version]
- Jin, Z.Q. MicroRNA targets and biomarker validation for diabetes-associated cardiac fibrosis. Pharmacol. Res. 2021, 174, 105941. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Rhee, C.M.; Chou, J.; Ahmadi, S.F.; Park, J.; Chen, J.L.; Amin, A.N. The Obesity Paradox in Kidney Disease: How to Reconcile it with Obesity Management. Kidney Int. Rep. 2017, 2, 271–281. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Ahmadi, S.F.; Streja, E.; Molnar, M.Z.; Flegal, K.M.; Gillen, D.; Kovesdy, C.P.; Kalantar-Zadeh, K. Obesity paradox in end-stage kidney disease patients. Prog. Cardiovasc. Dis. 2014, 56, 415–425. [Google Scholar] [CrossRef] [Green Version]
- Luo, Q.; Xia, X.; Li, B.; Lin, Z.; Yu, X.; Huang, F. Serum uric acid and cardiovascular mortality in chronic kidney disease: A meta-analysis. BMC Nephrol. 2019, 20, 18. [Google Scholar] [CrossRef] [Green Version]
- Petreski, T.; Bevc, S.; Ekart, R.; Hojs, R. Hyperuricemia and long-term survival in patients with chronic kidney disease undergoing hemodialysis. Clin. Nephrol. 2017, 88, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Piani, F.; Sasai, F.; Bjornstad, P.; Borghi, C.; Yoshimura, A.; Sanchez-Lozada, L.G.; Roncal-Jimenez, C.; Garcia, G.E.; Hernando, A.A.; Fuentes, G.C.; et al. Hyperuricemia and chronic kidney disease: To treat or not to treat. J. Bras. Nefrol. 2021, 43, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.Y.; Jin, S.M.; Jee, J.H.; Bae, J.C.; Lee, M.K.; Kim, J.H. The Protective Effects of Increasing Serum Uric Acid Level on Development of Metabolic Syndrome. Diabetes Metab. J. 2019, 43, 504–520. [Google Scholar] [CrossRef] [PubMed]
- Sautin, Y.Y.; Johnson, R.J. Uric acid: The oxidant-antioxidant paradox. Nucleosides Nucleotides Nucleic Acids 2008, 27, 608–619. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Study Population (N = 140) | Survivors (N = 77) | Deceased (N = 58) | p-Value * | |
|---|---|---|---|---|
| Age (Average ± SD) | 59 ± 15 | 53.4 ± 15.9 | 67.47 ± 9.73 | <0.0001 |
| Sex (Number, %) | 62 F (44.3%), 78 M (55.7%) | 38 F, 39 M | 20 F, 38 M | 0.114 |
| eGFR (Average ± SD) (ml/min/1.73 m2) | 8.7 ± 3.3 | 8.29 ± 3.27 | 9.23 ± 3.41 | 0.099 |
| Creatinine (Average ± SD) (mg/dL, umol/L) | 6.6 ± 2.4 (583.57 ± 212.21) | 6.95 ± 2.41 | 6.19 ± 2.24 | 0.06 |
| BMI (Average ± SD) (kg/m2) | 26.04 ± 5 | 27.2 ± 6.05 | 24.83 ± 4.37 | 0.02 |
| Obesity (Number, %) | 36 (25.7%) | 22 | 14 | 0.56 |
| Smoking (Number, %) | 23 (16.4%) | 11 | 12 | 0.361 |
| HTN grade (Number, %) | 11 Grade 2 (7.8%), 129 Grade 3 (92.2%) | 10 Grade 2 (13%), 67 Grade 3 (87%) | 1 Grade 2 (1.15%), 57 Grade 3 (98.85%) | 0.01 |
| Systolic blood pressure (Mean ± SD) (mmHg) | 140 ± 15 | 137.6 ± 10.6 | 142.5 ± 13.2 | 0.06 |
| Diastolic blood pressure (Average ± SD) (mmHg) | 76 ± 5 | 74.3 ± 4 | 76.7 ± 6.5 | 0.1 |
| NYHA class (Number, %) | Class I (52.1%), Class II (47.9%) | 46 Class I (60%), 31 Class II (40%) | 24 Class I (41.3%), 34 Class II (58.7%) | 0.038 |
| Diabetes mellitus (Number, %) | 47 (33.5%) | 15 | 31 | <0.0001 |
| Ischemic heart disease (Number, %) | 16 (11.4%) | 10 | 6 | 0.79 |
| Hb (Average ± SD) (g/dL) | 9.72 ± 2 | 9.96 ± 1.98 | 9.38 ± 1.55 | 0.06 |
| Uric acid (Average ± SD) (mg/dL) | 7.51 ± 2 | 7.93 ± 1.7 | 6.92 ± 1.87 | 0.001 |
| PICP (Mean ± SD) (µg/L) | 457.2 ± 240 | 425 ± 258.8 | 502.6 ± 204.4 | 0.003 |
| P3NP (Mean ± SD) (µg/L) | 242 ± 199.9 | 240.6 ± 218.1 | 244.1 ± 172.9 | 0.0001 |
| LAVI (Mean ± SD) (ml/m2) | 45.8 ± 14.2 | 43.69 ± 12.71 | 48.79 ± 15.7 | 0.036 |
| Mean E/e’ (Mean ± SD) | 9.8 ± 4.3 | 9.64 ± 4.15 | 10.13 ± 4.61 | 0.5 |
| Ejection fraction (Mean ± SD) (%) | 53.63 ± 8 | 54.48 ± 7.91 | 52.45 ± 8.32 | 0.146 |
| GLS (Mean ± SD) (%) | −10.2 ± 5.3 | −10.8 ± 5.6 | −9 ± 4.8 | 0.005 |
| PICP < Cut-Off (N = 44) | PICP > Cut-Off (N = 96) | P3NP < Cut-Off (N = 52) | P3NP > Cut Off (N = 88) | |
|---|---|---|---|---|
| Age (Average ± SD) | 56.41 ± 3.16 | 60.54 ± 16.17 | 60.25 ± 12.29 | 58.65 ± 16.94 |
| Sex (Number, %) | 22 F (50%), 22 M (50%) | 40 F (41.66%), 56 M (58.33%) | 24 F, 28 B | 28 F, 50 B |
| BMI (Average ± SD) (kg/m2) | 27.62 ± 6.42 | 26.78 ± 4.87 | 27.54 ± 6.27 | 26.75 ± 4.83 |
| Smoking (Number, %) | 5 (11.36%) | 18 (18.75%) | 3 (5.7%) | 20 (22.72%) |
| HTN grade (Number, %) | 1 Grade 2 (2.23%), 43 Grade 3 (97.77%) | 10 Grade 2 (10.41%), 86 Grade 3 (89.58%) | 2 Grade 2 (3.84%), 50 Grade 3 (96.15%) | 9 Grade 2 (10.22%), 79 Grade 3 (89.77%) |
| Diabetes mellitus (Number, %) | 17 (38.63%) | 30 (31.25%) | 20 (38.46%) | 27 (30.68%) |
| Mean E/e’ (Mean ± SD) | 8.17 ± 2.2 | 10.61 ± 4.83 | 8.94 ± 3.12 | 8.92 ± 3.46 |
| Ejection fraction (Mean ± SD) (%) | 59.02 ± 5.37 | 51.16 ± 7.97 | 56.85 ± 5.97 | 51.74 ± 8.63 |
| GLS (Mean ± SD) (%) | −16% ± 1.9% | −7.5% ± 4% | −13% ± 3.9% | −8% ± 0.5% |
| Univariate Analysis | Multivariate Cox Analysis | |||||
|---|---|---|---|---|---|---|
| Parameters | HR | 95% CI | p | HRa | 95% CI | p |
| Age, years | 1.147 | 1.122–1.171 | 0.001 | 1.25 | 1.23–1.28 | <0.001 |
| BMI, kg/m2 | 0.9 | 0.838–0.967 | 0.004 | |||
| Diabetes | 7.291 | 3.568–11.016 | <0.0001 | 5.168 | 2.590–10.310 | <0.0001 |
| PICP > 297.31 µg/L | 5.071 | 1.935–13.29 | 0.001 | 1.22 | 1.1–1.31 | <0.0001 |
| P3NP > 126.67 µg/L | 2.089 | 1.044–4.178 | 0.03 | 1.03 | 1.021–1.04 | 0.06 |
| Uric acid, mg/dL | 0.82 | 0.7–0.97 | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ureche, C.; Dodi, G.; Șerban, A.M.; Covic, A.S.; Voroneanu, L.; Hogaș, S.; Sascău, R.A.; Stătescu, C.; Covic, A. Predictive Value of Collagen Biomarkers in Advanced Chronic Kidney Disease Patients. Biomolecules 2023, 13, 389. https://doi.org/10.3390/biom13020389
Ureche C, Dodi G, Șerban AM, Covic AS, Voroneanu L, Hogaș S, Sascău RA, Stătescu C, Covic A. Predictive Value of Collagen Biomarkers in Advanced Chronic Kidney Disease Patients. Biomolecules. 2023; 13(2):389. https://doi.org/10.3390/biom13020389
Chicago/Turabian StyleUreche, Carina, Gianina Dodi, Adela Mihaela Șerban, Andreea Simona Covic, Luminița Voroneanu, Simona Hogaș, Radu Andy Sascău, Cristian Stătescu, and Adrian Covic. 2023. "Predictive Value of Collagen Biomarkers in Advanced Chronic Kidney Disease Patients" Biomolecules 13, no. 2: 389. https://doi.org/10.3390/biom13020389