
Identification of Lipid Biomarkers for Chronic Joint Pain Associated with Different Joint Diseases
 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Synovial Fluid Samples
2.1.1. Post Mortem Controls
2.1.2. Patients with Different Joint Diseases
2.2. Chemical and Lipid Standards
2.3. Lipid Extraction
2.4. Polar Lipid Purification
2.5. Electrospray Ionization-Mass Spectrometry Conditions for Lipids Analysis
2.6. Lipid Identification by MS, Calculation of Lipid Levels and Data Processing
2.7. Statistical Analysis
3. Results
3.1. Identification of Choline-Containing Lysophospholipids and Phospholipids in Human Synovial Fluids (HSF)
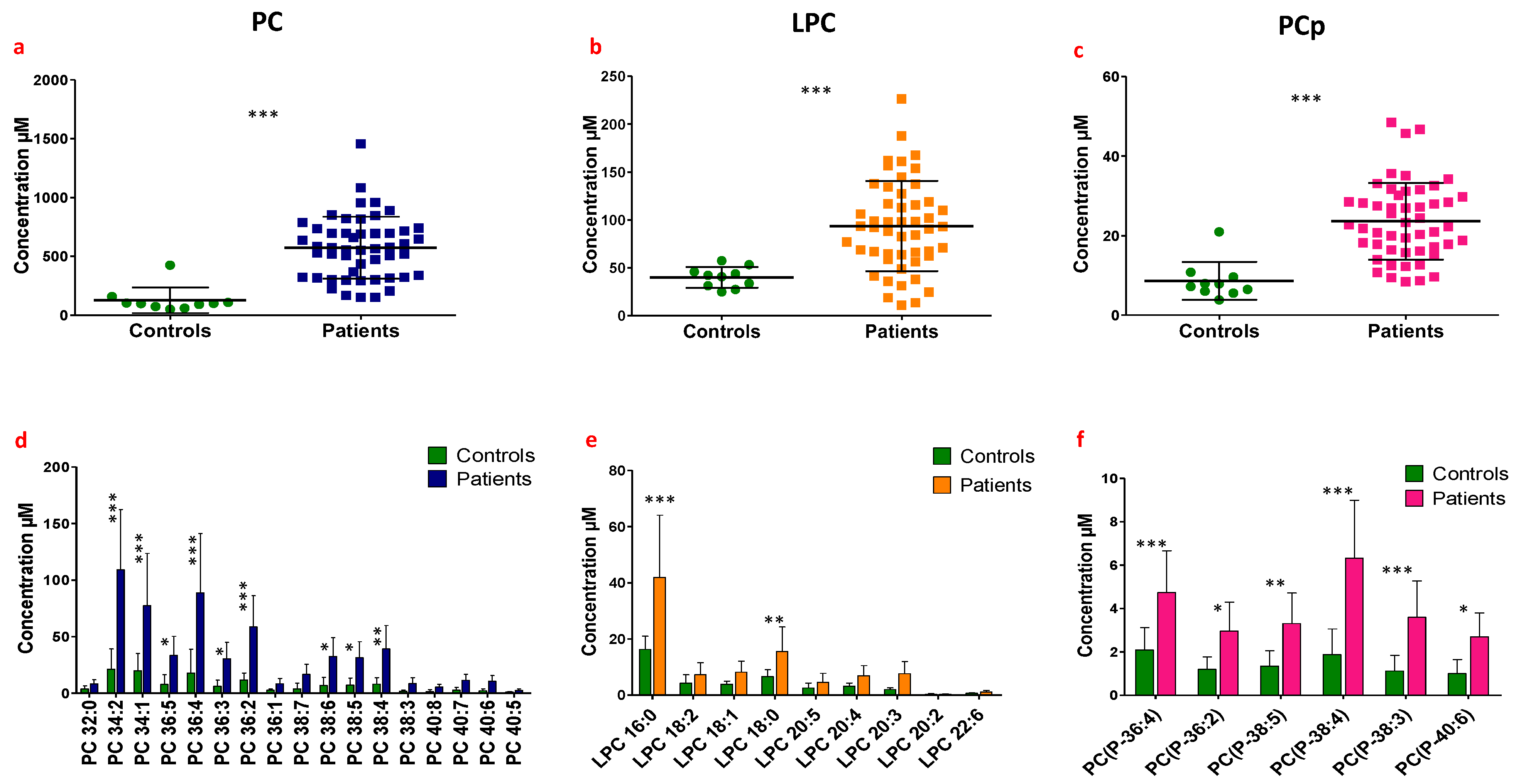
3.2. Identification of Potential Lipid Biomarkers in the Synovial Fluid of Patients Suffering from Chronic Joint Pain Compared to Control Synovial Fluids
3.3. Correlational Studies between Lipid Levels in Synovial Fluids and Patients’ Clinical Characteristics (Parameters)
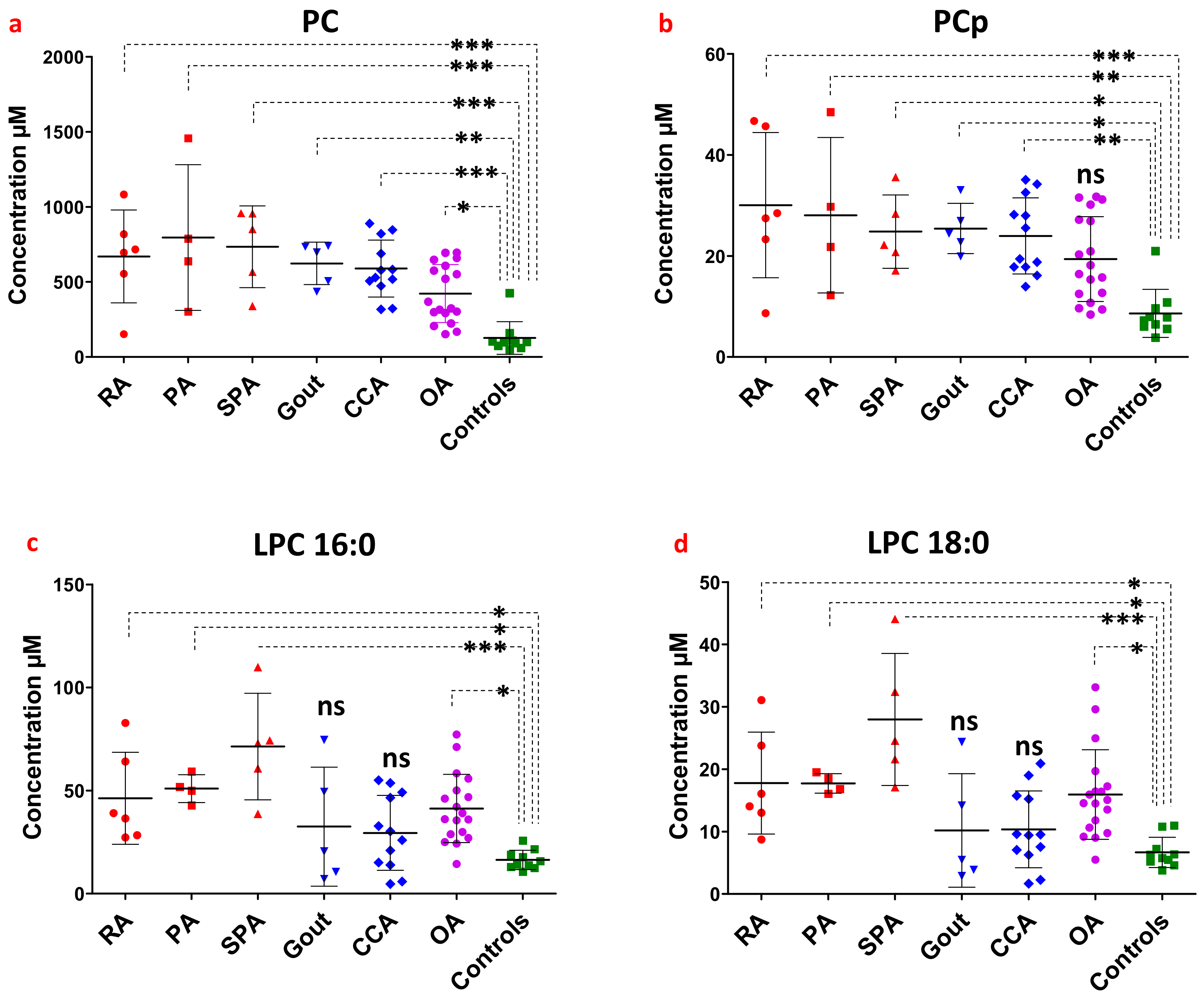
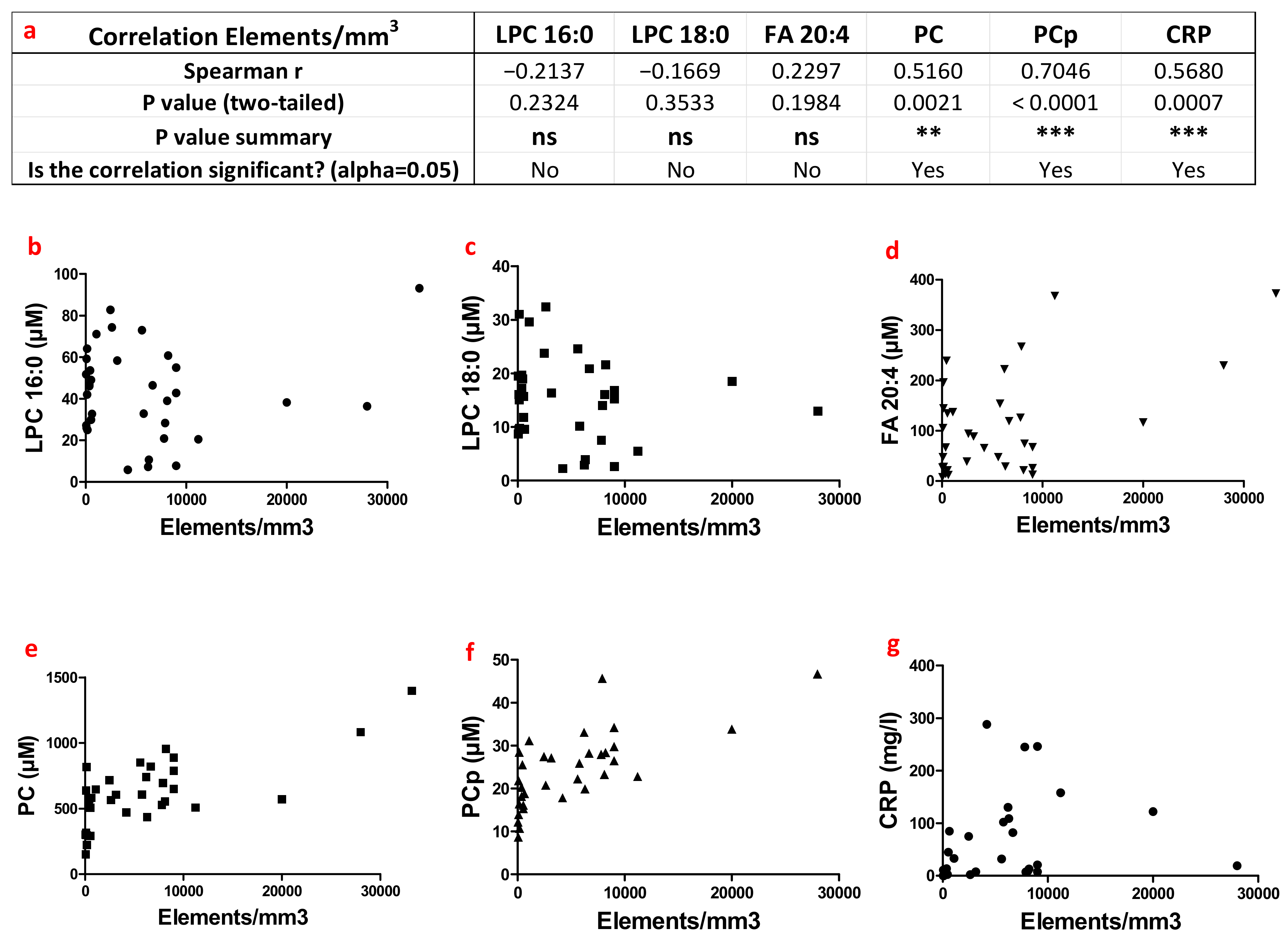
3.4. Correlation Studies between Lipid Levels in Patient Synovial Fluids, Type of Joint Pathologies and Inflammatory State
3.5. Possible Origins of High Levels of Selective Lipids in Patient Synovial Fluids
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wittenauer, R.; Smith, L.; Aden, K. Background Paper 6.12 Osteoarthritis. Backgr. Pap. 2004, 31, 78314428. [Google Scholar]
- Marra, S.; Ferru-Clément, R.; Breuil, V.; Delaunay, A.; Christin, M.; Friend, V.; Sebille, S.; Cognard, C.; Ferreira, T.; Roux, C.; et al. Non-Acidic Activation of Pain-Related Acid-Sensing Ion Channel 3 by Lipids. EMBO J. 2016, 35, 414–428. [Google Scholar] [CrossRef]
- Jacquot, F.; Khoury, S.; Labrum, B.; Delanoe, K.; Pidoux, L.; Barbier, J.; Delay, L.; Bayle, A.; Aissouni, Y.; Barriere, D.A.; et al. Lysophosphatidylcholine 16: 0 Mediates Chronic Joint Pain Associated to Rheumatic Diseases through Acid-Sensing Ion Channel 3. Pain 2022, 163, 1999–2013. [Google Scholar] [CrossRef]
- Waldmann, R.; Champigny, G.; Bassilana, F.; Heurteaux, C.; Lazdunski, M. A Proton-Gated Cation Channel Involved in Acid-Sensing. Nature 1997, 386, 173–177. [Google Scholar] [CrossRef]
- Deval, E.; Noël, J.; Lay, N.; Alloui, A.; Diochot, S.; Friend, V.; Jodar, M.; Lazdunski, M.; Lingueglia, E. ASIC3, a Sensor of Acidic and Primary Inflammatory Pain. EMBO J. 2008, 27, 3047–3055. [Google Scholar] [CrossRef]
- Law, S.-H.; Chan, M.-L.; Marathe, G.K.; Parveen, F.; Chen, C.-H.; Ke, L.-Y. An Updated Review of Lysophosphatidylcholine Metabolism in Human Diseases. Int. J. Mol. Sci. 2019, 20, 1149. [Google Scholar] [CrossRef]
- Souto, A.; Salgado, E.; Maneiro, J.R.; Mera, A.; Carmona, L.; Gómez-Reino, J.J. Lipid Profile Changes in Patients with Chronic Inflammatory Arthritis Treated With Biologic Agents and Tofacitinib in Randomized Clinical Trials: A Systematic Review and Meta-Analysis. Arthritis Rheumatol. 2015, 67, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Gang, T.B.; Hammond, D.J.; Singh, S.K.; Ferguson, D.A.; Mishra, V.; Agrawal, A. The Phosphocholine-binding Pocket on C-reactive Protein Is Necessary for Initial Protection of Mice against Pneumococcal Infection. J. Biol. Chem. 2012, 287, 43116–43125. [Google Scholar] [CrossRef]
- Agrawal, A.; Suresh, M.V.; Singh, S.K.; Ferguson, J.D.A. The Protective Function of Human C-Reactive Protein in Mouse Models of Streptococcus pneumoniae Infection. Endocr. Metab. Immune Disord. Drug Targets 2008, 8, 231–237. [Google Scholar] [CrossRef]
- Suresh, M.V.; Singh, S.K.; Ferguson, D.A.; Agrawal, A. Role of the Property of C-Reactive Protein to Activate the Classical Pathway of Complement in Protecting Mice from Pneumococcal Infection. J. Immunol. 2006, 176, 4369–4374. [Google Scholar] [CrossRef]
- Freemont, A.J. Microscopic Analysis of Synovial Fluid—The Perfect Diagnostic Test? Ann. Rheum. Dis. 1996, 55, 695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bole, G.G.; Peltier, D.F. Synovial Fluid Lipids in Normal Individuals and Patients with Rheumatoid Arthritis. Arthritis Rheum. 1962, 5, 589–601. [Google Scholar] [CrossRef] [PubMed]
- Kosinska, M.K.; Liebisch, G.; Lochnit, G.; Wilhelm, J.; Klein, H.; Kaesser, U.; Lasczkowski, G.; Rickert, M.; Schmitz, G.; Steinmeyer, J. A Lipidomic Study of Phospholipid Classes and Species in Human Synovial Fluid. Arthritis Rheum. 2013, 65, 2323–2333. [Google Scholar] [CrossRef] [PubMed]
- Kosinska, M.K.; Liebisch, G.; Lochnit, G.; Wilhelm, J.; Klein, H.; Kaesser, U.; Lasczkowski, G.; Rickert, M.; Schmitz, G.; Steinmeyer, J. Sphingolipids in Human Synovial Fluid—A Lipidomic Study. PLoS ONE 2014, 9, e91769. [Google Scholar] [CrossRef] [PubMed]
- Kosinska, M.K.; Mastbergen, S.C.; Liebisch, G.; Wilhelm, J.; Dettmeyer, R.B.; Ishaque, B.; Rickert, M.; Schmitz, G.; Lafeber, F.P.; Steinmeyer, J. Comparative Lipidomic Analysis of Synovial Fluid in Human and Canine Osteoarthritis. Osteoarthr. Cartil. 2016, 24, 1470–1478. [Google Scholar] [CrossRef] [PubMed]
- Folch, J.; Lees, M.; Sloane Stanley, G.H. A simple method for the isolation and purification of total lipides from animal tissues. J. Biol. Chem. 1957, 226, 497–509. [Google Scholar] [CrossRef]
- Yang, K.; Han, X. Accurate Quantification of Lipid Species by Electrospray Ionization Mass Spectrometry—Meets a Key Challenge in Lipidomics. Metabolites 2011, 1, 21–40. [Google Scholar] [CrossRef]
- Braverman, N.E.; Moser, A.B. Functions of Plasmalogen Lipids in Health and Disease. Biochim. Biophys. Acta Mol. Basis Dis. 2012, 1822, 1442–1452. [Google Scholar] [CrossRef]
- Snyder, F. Platelet-Activating Factor: The Biosynthetic and Catabolic Enzymes. Biochem. J. 1995, 305 Pt 3, 689–705. [Google Scholar] [CrossRef]
- Goracci, G.; Balestrieri, M.L.; Nardicchi, V. Metabolism and Functions of Platelet-Activating Factor (PAF) in the Nervous Tissue. In Handbook of Neurochemistry and Molecular Neurobiology: Neural Lipids; Lajtha, A., Tettamanti, G., Goracci, G., Eds.; Springer: Boston, MA, USA, 2009; pp. 311–352. ISBN 978-0-387-30378-9. [Google Scholar]
- Soupene, E.; Fyrst, H.; Kuypers, F.A. Mammalian Acyl-CoA:Lysophosphatidylcholine Acyltransferase Enzymes. Proc. Natl. Acad. Sci. USA 2008, 105, 88. [Google Scholar] [CrossRef]
- Scott, K.F.; Bryant, K.J.; Bidgood, M.J. Functional Coupling and Differential Regulation of the Phospholipase A2-Cyclooxygenase Pathways in Inflammation. J. Leukoc. Biol. 1999, 66, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Boilard, E.; Lai, Y.; Larabee, K.; Balestrieri, B.; Ghomashchi, F.; Fujioka, D.; Gobezie, R.; Coblyn, J.S.; Weinblatt, M.E.; Massarotti, E.M.; et al. A Novel Anti-Inflammatory Role for Secretory Phospholipase A2 in Immune Complex-Mediated Arthritis. EMBO Mol. Med. 2010, 2, 172–187. [Google Scholar] [CrossRef] [PubMed]
- Block, D.R.; Genzen, J.R. Chapter 27—Diagnostic Body Fluid Testing. In Contemporary Practice in Clinical Chemistry, 4th ed.; Clarke, W., Marzinke, M.A., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 469–486. ISBN 978-0-12-815499-1. [Google Scholar]
- Tetreault, M.; Wetters, N.G.; Moric, M.; Gross, C.E.; Della Valle, C.J. Is Synovial C-Reactive Protein a Useful Marker for Periprosthetic Joint Infection? Clin. Orthop. Relat. Res. 2014, 472, 3997–4003. [Google Scholar] [CrossRef] [PubMed]
- Rowe, I.F.; Sheldon, J.; Riches, P.G.; Keat, A.C. Comparative Studies of Serum and Synovial Fluid C Reactive Protein Concentrations. Ann. Rheum. Dis. 1987, 46, 721–726. [Google Scholar] [CrossRef]
- Shrivastava, A.; Singh, H.; Raizada, A.; Singh, S.; Pandey, A.; Singh, N.; Yadav, D.; Sharma, H. Inflammatory Markers in Patients with Rheumatoid Arthritis. Allergol. Immunopathol. 2015, 43, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Zhu, W.; Chen, C.; Yan, B.; Zhu, L.; Chen, X.; Peng, C. The Mechanisms of Lysophosphatidylcholine in the Development of Diseases. Life Sci. 2020, 247, 117443. [Google Scholar] [CrossRef]
- Kuniyasu, A.; Tokunaga, M.; Yamamoto, T.; Inoue, S.; Obama, K.; Kawahara, K.; Nakayama, H. Oxidized LDL and Lysophosphatidylcholine Stimulate Plasminogen Activator Inhibitor-1 Expression through Reactive Oxygen Species Generation and ERK1/2 Activation in 3T3-L1 Adipocytes. Biochim. Biophys. Acta Mol. Cell Biol. Lipids 2011, 1811, 153–162. [Google Scholar] [CrossRef]
- Schilling, T.; Eder, C. Sodium Dependence of Lysophosphatidylcholine-Induced Caspase-1 Activity and Reactive Oxygen Species Generation. Immunobiology 2011, 216, 118–125. [Google Scholar] [CrossRef]
- Schilling, T.; Eder, C. Importance of Lipid Rafts for Lysophosphatidylcholine-Induced Caspase-1 Activation and Reactive Oxygen Species Generation. Cell. Immunol. 2010, 265, 87–90. [Google Scholar] [CrossRef]
- Bach, G.; Perrin-Cocon, L.; Gerossier, E.; Guironnet-Paquet, A.; Lotteau, V.; Inchauspé, G.; Fournillier, A. Single Lysophosphatidylcholine Components Exhibit Adjuvant Activities in Vitro and in Vivo. Clin. Vaccine Immunol 2010, 17, 429–438. [Google Scholar] [CrossRef]
- Hung, N.D.; Sok, D.-E.; Kim, M.R. Prevention of 1-Palmitoyl Lysophosphatidylcholine-Induced Inflammation by Polyunsaturated Acyl Lysophosphatidylcholine. Inflamm. Res. 2012, 61, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Sevastou, I.; Kaffe, E.; Mouratis, M.-A.; Aidinis, V. Lysoglycerophospholipids in Chronic Inflammatory Disorders: The PLA2/LPC and ATX/LPA Axes. Biochim. Biophys. Acta Mol. Cell Biol. Lipids 2013, 1831, 42–60. [Google Scholar] [CrossRef] [PubMed]
- Drobnik, W.; Liebisch, G.; Audebert, F.-X.; Fröhlich, D.; Glück, T.; Vogel, P.; Rothe, G.; Schmitz, G. Plasma Ceramide and Lysophosphatidylcholine Inversely Correlate with Mortality in Sepsis Patients. J. Lipid Res. 2003, 44, 754–761. [Google Scholar] [CrossRef] [PubMed]
- Treede, I.; Braun, A.; Sparla, R.; Kühnel, M.; Giese, T.; Turner, J.R.; Anes, E.; Kulaksiz, H.; Füllekrug, J.; Stremmel, W.; et al. Anti-inflammatory Effects of Phosphatidylcholine. J. Biol. Chem. 2007, 282, 27155–27164. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, P.; Szabó, A.; Erős, G.; Gurabi, D.; Horváth, G.; Németh, I.; Ghyczy, M.; Boros, M. Anti-Inflammatory Effects of Phosphatidylcholine in Neutrophil Leukocyte-dependent Acute Arthritis in Rats. Eur. J. Pharmacol. 2009, 622, 58–64. [Google Scholar] [CrossRef]
- Han, M.S.; Park, S.Y.; Shinzawa, K.; Kim, S.; Chung, K.W.; Lee, J.-H.; Kwon, C.H.; Lee, K.-W.; Lee, J.-H.; Park, C.K.; et al. Lysophosphatidylcholine as a Death Effector in the Lipoapoptosis of Hepatocytes. J. Lipid Res. 2008, 49, 84–97. [Google Scholar] [CrossRef] [PubMed]
- Erős, G.; Ibrahim, S.; Siebert, N.; Boros, M.; Vollmar, B. Oral Phosphatidylcholine Pretreatment Alleviates the Signs of Experimental Rheumatoid Arthritis. Thromb. Haemost. 2009, 11, R43. [Google Scholar] [CrossRef]
- Wettstein, M.; Eich, W.; Bieber, C.; Tesarz, J. Pain Intensity, Disability, and Quality of Life in Patients with Chronic Low Back Pain: Does Age Matter? Pain Med. 2019, 20, 464–475. [Google Scholar] [CrossRef]
- Oliviero, F.; Nigro, A.L.; Bernardi, D.; Giunco, S.; Baldo, G.; Scanu, A.; Sfriso, P.; Ramonda, R.; Plebani, M.; Punzi, L. A Comparative Study of Serum and Synovial Fluid Lipoprotein Levels in Patients with Various Arthritides. Clin. Chim. Acta 2012, 413, 303–307. [Google Scholar] [CrossRef]
- Pan, F.; Tian, J.; Cicuttini, F.; Jones, G. Metabolic Syndrome and Trajectory of Knee Pain in Older Adults. Osteoarthr. Cartil. 2020, 28, 45–52. [Google Scholar] [CrossRef]
- Li, H.; George, D.M.; Jaarsma, R.L.; Mao, X. Metabolic Syndrome and Components Exacerbate Osteoarthritis Symptoms of Pain, Depression and Reduced Knee Function. Ann. Transl. Med. 2016, 4, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Synovial Fluid Lipids | |||||||
|---|---|---|---|---|---|---|---|
| LPC 16:0 | LPC 18:0 | LPC | PC | PCp | |||
| Plasma lipids | Cholesterol g/L | Spearman r | 0.7088 | 0.6588 | 0.6971 | 0.4853 | 0.02059 |
| p value | 0.0021 | 0.0055 | 0.0027 | 0.0567 | 0.9397 | ||
| p value summary | ** | ** | ** | ns | ns | ||
| HDL g/L | Spearman r | 0.6577 | 0.6220 | 0.6434 | 0.3628 | 0.1948 | |
| p value | 0.0077 | 0.0133 | 0.0097 | 0.1838 | 0.4866 | ||
| p value summary | ** | * | ** | ns | ns | ||
| LDL g/L | Spearman r | 0.5754 | 0.6196 | 0.5946 | 0.4268 | 0.09860 | |
| p value | 0.0197 | 0.0105 | 0.0151 | 0.0992 | 0.7164 | ||
| p value summary | * | * | * | ns | ns | ||
| TG | Spearman r | 0.5063 | 0.3297 | 0.4474 | 0.2693 | −0.2870 | |
| p value | 0.0454 | 0.2124 | 0.0823 | 0.3131 | 0.2812 | ||
| p value summary | * | ns | ns | ns | ns | ||
| Blood glucose plasma | Spearman r | −0.4476 | −0.5245 | −0.5035 | −0.2727 | −0.5105 | |
| p value | 0.1446 | 0.0800 | 0.0952 | 0.3911 | 0.0899 | ||
| p value summary | ns | ns | ns | ns | ns | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khoury, S.; Colas, J.; Breuil, V.; Kosek, E.; Ahmed, A.S.; Svensson, C.I.; Marchand, F.; Deval, E.; Ferreira, T. Identification of Lipid Biomarkers for Chronic Joint Pain Associated with Different Joint Diseases. Biomolecules 2023, 13, 342. https://doi.org/10.3390/biom13020342
Khoury S, Colas J, Breuil V, Kosek E, Ahmed AS, Svensson CI, Marchand F, Deval E, Ferreira T. Identification of Lipid Biomarkers for Chronic Joint Pain Associated with Different Joint Diseases. Biomolecules. 2023; 13(2):342. https://doi.org/10.3390/biom13020342
Chicago/Turabian StyleKhoury, Spiro, Jenny Colas, Véronique Breuil, Eva Kosek, Aisha S. Ahmed, Camilla I. Svensson, Fabien Marchand, Emmanuel Deval, and Thierry Ferreira. 2023. "Identification of Lipid Biomarkers for Chronic Joint Pain Associated with Different Joint Diseases" Biomolecules 13, no. 2: 342. https://doi.org/10.3390/biom13020342