
Monitoring Blood Immune Cells in Patients with Advanced Small Cell Lung Cancer Undergoing a Combined Immune Checkpoint Inhibitor/Chemotherapy
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Characteristics and General Outcome
2.2. Blood Samples, Flow Cytometry, and Antibody Staining
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics and General Outcome
3.2. Blood Cells and Therapy Response
3.3. Comparison of Baseline and Third-Cycle Blood Cell Markers
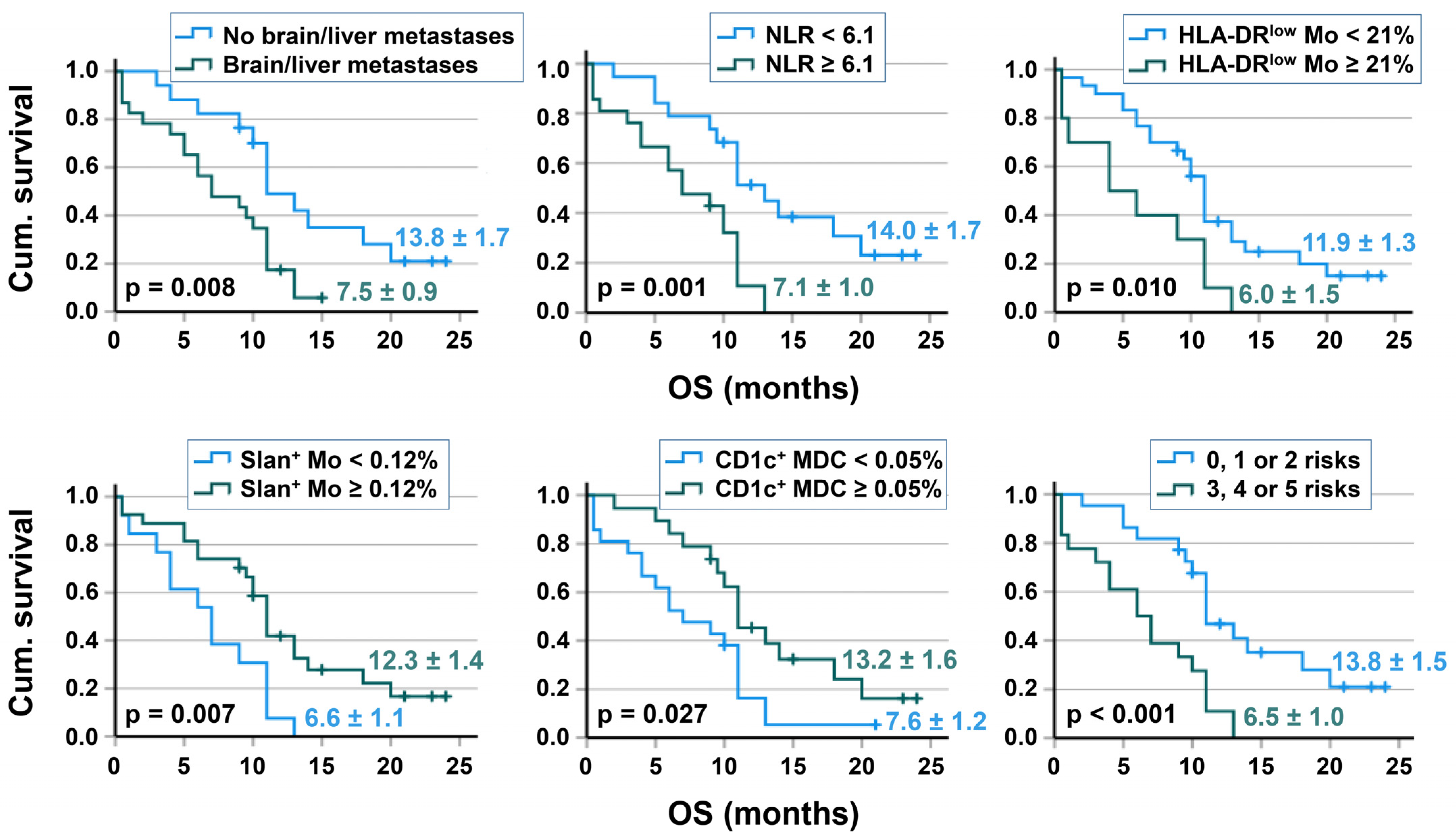
3.4. Survival Analyses
3.5. Correlation of Immune Cell Subpopulations
3.6. Comparison of Immune Cell Parameters in Patients with SCLC and NSCLC
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rudin, C.M.; Brambilla, E.; Faivre-Finn, C.; Sage, J. Small-cell lung cancer. Nat. Rev. Dis. Prim. 2021, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Dvorkin, M.; Chen, Y.; Reinmuth, N.; Hotta, K.; Trukhin, D.; Statsenko, G.; Hochmair, M.J.; Ozguroglu, M.; Ji, J.H.; et al. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (caspian): A randomised, controlled, open-label, phase 3 trial. Lancet 2019, 394, 1929–1939. [Google Scholar] [CrossRef] [PubMed]
- Giunta, E.F.; Addeo, A.; Rizzo, A.; Banna, G.L. First-line treatment for advanced sclc: What is left behind and beyond chemoimmunotherapy. Front. Med. 2022, 9, 924853. [Google Scholar] [CrossRef] [PubMed]
- Barrows, E.D.; Blackburn, M.J.; Liu, S.V. Evolving role of immunotherapy in small cell lung cancer. Semin. Cancer Biol. 2022, 86, 868–874. [Google Scholar] [CrossRef]
- Ortega-Franco, A.; Ackermann, C.; Paz-Ares, L.; Califano, R. First-line immune checkpoint inhibitors for extensive stage small-cell lung cancer: Clinical developments and future directions. ESMO Open 2021, 6, 100003. [Google Scholar] [CrossRef]
- Gandini, S.; Massi, D.; Mandala, M. Pd-l1 expression in cancer patients receiving anti pd-1/pd-l1 antibodies: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2016, 100, 88–98. [Google Scholar] [CrossRef]
- Ushio, R.; Murakami, S.; Saito, H. Predictive markers for immune checkpoint inhibitors in non-small cell lung cancer. J. Clin. Med. 2022, 11, 1855. [Google Scholar] [CrossRef]
- Acheampong, E.; Abed, A.; Morici, M.; Bowyer, S.; Amanuel, B.; Lin, W.; Millward, M.; Gray, E.S. Tumour pd-l1 expression in small-cell lung cancer: A systematic review and meta-analysis. Cells 2020, 9, 2393. [Google Scholar] [CrossRef]
- Owonikoko, T.K.; Park, K.; Govindan, R.; Ready, N.; Reck, M.; Peters, S.; Dakhil, S.R.; Navarro, A.; Rodriguez-Cid, J.; Schenker, M.; et al. Nivolumab and ipilimumab as maintenance therapy in extensive-disease small-cell lung cancer: Checkmate 451. J. Clin. Oncol. 2021, 39, 1349–1359. [Google Scholar] [CrossRef]
- Spigel, D.R.; Vicente, D.; Ciuleanu, T.E.; Gettinger, S.; Peters, S.; Horn, L.; Audigier-Valette, C.; Pardo Aranda, N.; Juan-Vidal, O.; Cheng, Y.; et al. Second-line nivolumab in relapsed small-cell lung cancer: Checkmate 331*. Ann. Oncol. 2021, 32, 631–641. [Google Scholar] [CrossRef]
- Liu, F.; Zhou, S.; Tan, L.; Jiang, H.; Huang, Y. A retrospective cohort study on pretreated neutrophil-to-lymphocyte ratio and prognosis of small cell lung cancer: Evidence of effect modification by chemotherapy regimen. Cancer Manag. Res. 2020, 12, 10341–10352. [Google Scholar] [CrossRef] [PubMed]
- Sacdalan, D.B.; Lucero, J.A.; Sacdalan, D.L. Prognostic utility of baseline neutrophil-to-lymphocyte ratio in patients receiving immune checkpoint inhibitors: A review and meta-analysis. OncoTargets Ther. 2018, 11, 955–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.A.; Ma, W.; Yuan, J.; Li, T. Translational biomarkers and rationale strategies to overcome resistance to immune checkpoint inhibitors in solid tumors. Cancer Treat. Res. 2020, 180, 251–279. [Google Scholar] [PubMed]
- Topalian, S.L.; Taube, J.M.; Anders, R.A.; Pardoll, D.M. Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy. Nat. Rev. Cancer 2016, 16, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Möller, M.; Turzer, S.; Ganchev, G.; Wienke, A.; Schütte, W.; Seliger, B.; Riemann, D. Blood immune cell biomarkers in lung cancer patients undergoing treatment with a combination of chemotherapy and immune checkpoint blockade. Cancers 2022, 14, 3690. [Google Scholar] [CrossRef] [PubMed]
- Horn, L.; Mansfield, A.S.; Szczesna, A.; Havel, L.; Krzakowski, M.; Hochmair, M.J.; Huemer, F.; Losonczy, G.; Johnson, M.L.; Nishio, M.; et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N. Engl. J. Med. 2018, 379, 2220–2229. [Google Scholar] [CrossRef]
- Dzionek, A.; Fuchs, A.; Schmidt, P.; Cremer, S.; Zysk, M.; Miltenyi, S.; Buck, D.W.; Schmitz, J. Bdca-2, bdca-3, and bdca-4: Three markers for distinct subsets of dendritic cells in human peripheral blood. J. Immunol. 2000, 165, 6037–6046. [Google Scholar] [CrossRef] [Green Version]
- Döcke, W.D.; Hoflich, C.; Davis, K.A.; Rottgers, K.; Meisel, C.; Kiefer, P.; Weber, S.U.; Hedwig-Geissing, M.; Kreuzfelder, E.; Tschentscher, P.; et al. Monitoring temporary immunodepression by flow cytometric measurement of monocytic hla-dr expression: A multicenter standardized study. Clin. Chem. 2005, 51, 2341–2347. [Google Scholar] [CrossRef] [Green Version]
- Chalmers, Z.R.; Connelly, C.F.; Fabrizio, D.; Gay, L.; Ali, S.M.; Ennis, R.; Schrock, A.; Campbell, B.; Shlien, A.; Chmielecki, J.; et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med. 2017, 9, 34. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Hodkinson, P.; McLaren, F.; Mackean, M.J.; Williams, L.; Howie, S.E.M.; Wallace, W.A.H.; Sethi, T. Histologic assessment of tumor-associated cd45(+) cell numbers is an independent predictor of prognosis in small cell lung cancer. Chest 2013, 143, 146–151. [Google Scholar] [CrossRef]
- Iams, W.T.; Shiuan, E.; Meador, C.B.; Roth, M.; Bordeaux, J.; Vaupel, C.; Boyd, K.L.; Summitt, I.B.; Wang, L.L.; Schneider, J.T.; et al. Improved prognosis and increased tumor-infiltrating lymphocytes in patients who have sclc with neurologic paraneoplastic syndromes. J. Thorac. Oncol. 2019, 14, 1970–1981. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, G.; Rath, B. Immunotherapy for small cell lung cancer: Mechanisms of resistance. Expert Opin. Biol. Ther. 2019, 19, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Hu-Lieskovan, S.; Wargo, J.A.; Ribas, A. Primary, adaptive, and acquired resistance to cancer immunotherapy. Cell 2017, 168, 707–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, S.; Zhang, T.; Zheng, L.; Liu, H.; Song, W.; Liu, D.; Li, Z.; Pan, C.X. Combination strategies to maximize the benefits of cancer immunotherapy. J. Hematol. Oncol. 2021, 14, 156. [Google Scholar] [CrossRef] [PubMed]
- Mazzaschi, G.; Minari, R.; Zecca, A.; Cavazzoni, A.; Ferri, V.; Mori, C.; Squadrilli, A.; Bordi, P.; Buti, S.; Bersanelli, M.; et al. Soluble pd-l1 and circulating cd8+pd-1+ and nk cells enclose a prognostic and predictive immune effector score in immunotherapy treated nsclc patients. Lung Cancer 2020, 148, 1–11. [Google Scholar] [CrossRef]
- Alfranca, Y.L.; Garcia, M.E.O.; Rueda, A.G.; Ballesteros, P.A.; Rodriguez, D.R.; Velasco, M.T. Blood biomarkers of response to immune checkpoint inhibitors in non-small cell lung cancer. J. Clin. Med. 2022, 11, 3245. [Google Scholar] [CrossRef]
- Gascon, M.; Isla, D.; Cruellas, M.; Galvez, E.M.; Lastra, R.; Ocariz, M.; Pano, J.R.; Ramirez, A.; Sesma, A.; Torres-Ramon, I.; et al. Intratumoral versus circulating lymphoid cells as predictive biomarkers in lung cancer patients treated with immune checkpoint inhibitors: Is the easiest path the best one? Cells 2020, 9, 1525. [Google Scholar] [CrossRef]
- Costantini, A.; Julie, C.; Dumenil, C.; Helias-Rodzewicz, Z.; Tisserand, J.; Dumoulin, J.; Giraud, V.; Labrune, S.; Chinet, T.; Emile, J.F.; et al. Predictive role of plasmatic biomarkers in advanced non-small cell lung cancer treated by nivolumab. Oncoimmunology 2018, 7, e1452581. [Google Scholar] [CrossRef] [Green Version]
- Deng, M.; Ma, X.; Liang, X.; Zhu, C.; Wang, M. Are pretreatment neutrophil-lymphocyte ratio and platelet-lymphocyte ratio useful in predicting the outcomes of patients with small-cell lung cancer? Oncotarget 2017, 8, 37200–37207. [Google Scholar] [CrossRef] [Green Version]
- Jablonska, J.; Lang, S.; Sionov, R.V.; Granot, Z. The regulation of pre-metastatic niche formation by neutrophils. Oncotarget 2017, 8, 112132–112144. [Google Scholar] [CrossRef]
- Raskov, H.; Orhan, A.; Gaggar, S.; Gogenur, I. Neutrophils and polymorphonuclear myeloid-derived suppressor cells: An emerging battleground in cancer therapy. Oncogenesis 2022, 11, 22. [Google Scholar] [CrossRef]
- Carnevale, S.; Ghasemi, S.; Rigatelli, A.; Jaillon, S. The complexity of neutrophils in health and disease: Focus on cancer. Semin. Immunol. 2020, 48, 101409. [Google Scholar] [CrossRef] [PubMed]
- Iclozan, C.; Antonia, S.; Chiappori, A.; Chen, D.T.; Gabrilovich, D. Therapeutic regulation of myeloid-derived suppressor cells and immune response to cancer vaccine in patients with extensive stage small cell lung cancer. Cancer Immunol. Immunother. 2013, 62, 909–918. [Google Scholar] [CrossRef] [Green Version]
- Faget, J.; Peters, S.; Quantin, X.; Meylan, E.; Bonnefoy, N. Neutrophils in the era of immune checkpoint blockade. J. Immunother. Cancer 2021, 9, e002242. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Spakowicz, D.; Burkart, J.; Patel, S.; Husain, M.; He, K.; Bertino, E.M.; Shields, P.G.; Carbone, D.P.; Verschraegen, C.F.; et al. Change in neutrophil to lymphocyte ratio during immunotherapy treatment is a non-linear predictor of patient outcomes in advanced cancers. J. Cancer Res. Clin. Oncol. 2019, 145, 2541–2546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winther-Larsen, A.; Aggerholm-Pedersen, N.; Sandfeld-Paulsen, B. Inflammation scores as prognostic biomarkers in small cell lung cancer: A systematic review and meta-analysis. Syst. Rev. 2021, 10, 40. [Google Scholar] [CrossRef] [PubMed]
- Rice, S.J.; Belani, C.P. Diversity and heterogeneity of immune states in non-small cell lung cancer and small cell lung cancer. PLoS ONE 2021, 16, e0260988. [Google Scholar] [CrossRef]
- Riemann, D.; Cwikowski, M.; Turzer, S.; Giese, T.; Grallert, M.; Schütte, W.; Seliger, B. Blood immune cell biomarkers in lung cancer. Clin. Exp. Immunol. 2019, 195, 179–189. [Google Scholar] [CrossRef] [Green Version]
- Mengos, A.E.; Gastineau, D.A.; Gustafson, M.P. The cd14(+)hla-dr(lo/neg) monocyte: An immunosuppressive phenotype that restrains responses to cancer immunotherapy. Front. Immunol. 2019, 10, 1147. [Google Scholar] [CrossRef] [Green Version]
- Vetsika, E.K.; Koinis, F.; Gioulbasani, M.; Aggouraki, D.; Koutoulaki, A.; Skalidaki, E.; Mavroudis, D.; Georgoulias, V.; Kotsakis, A. A circulating subpopulation of monocytic myeloid-derived suppressor cells as an independent prognostic/predictive factor in untreated non-small lung cancer patients. J. Immunol. Res. 2014, 2014, 659294. [Google Scholar] [CrossRef]
- Döcke, W.D.; Randow, F.; Syrbe, U.; Krausch, D.; Asadullah, K.; Reinke, P.; Volk, H.D.; Kox, W. Monocyte deactivation in septic patients: Restoration by ifn-gamma treatment. Nat. Med. 1997, 3, 678–681. [Google Scholar] [CrossRef] [PubMed]
- Huschak, G.; Zur Nieden, K.; Stuttmann, R.; Riemann, D. Changes in monocytic expression of aminopeptidase n/cd13 after major trauma. Clin. Exp. Immunol. 2003, 134, 491–496. [Google Scholar] [CrossRef]
- Noman, M.Z.; Desantis, G.; Janji, B.; Hasmim, M.; Karray, S.; Dessen, P.; Bronte, V.; Chouaib, S. Pd-l1 is a novel direct target of hif-1alpha, and its blockade under hypoxia enhanced mdsc-mediated t cell activation. J. Exp. Med. 2014, 211, 781–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hart, K.M.; Byrne, K.T.; Molloy, M.J.; Usherwood, E.M.; Berwin, B. Il-10 immunomodulation of myeloid cells regulates a murine model of ovarian cancer. Front. Immunol. 2011, 2, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trikha, P.; Carson, W.E., 3rd. Signaling pathways involved in mdsc regulation. Biochim. Biophys. Acta 2014, 1846, 55–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laborde, R.R.; Lin, Y.; Gustafson, M.P.; Bulur, P.A.; Dietz, A.B. Cancer vaccines in the world of immune suppressive monocytes (cd14(+)hla-dr(lo/neg) cells): The gateway to improved responses. Front. Immunol. 2014, 5, 147. [Google Scholar] [CrossRef]
- Bronte, G.; Calabro, L.; Olivieri, F.; Procopio, A.D.; Crino, L. The prognostic effects of circulating myeloid-derived suppressor cells in non-small cell lung cancer: Systematic review and meta-analysis. Clin. Exp. Med. 2022. [Google Scholar] [CrossRef]
- de Biasi, A.R.; Villena-Vargas, J.; Adusumilli, P.S. Cisplatin-induced antitumor immunomodulation: A review of preclinical and clinical evidence. Clin. Cancer Res. 2014, 20, 5384–5391. [Google Scholar] [CrossRef] [Green Version]
- Galluzzi, L.; Buque, A.; Kepp, O.; Zitvogel, L.; Kroemer, G. Immunological effects of conventional chemotherapy and targeted anticancer agents. Cancer Cell 2015, 28, 690–714. [Google Scholar] [CrossRef] [Green Version]
- Patysheva, M.; Frolova, A.; Larionova, I.; Afanas’ev, S.; Tarasova, A.; Cherdyntseva, N.; Kzhyshkowska, J. Monocyte programming by cancer therapy. Front. Immunol. 2022, 13, 994319. [Google Scholar] [CrossRef]
- Hofer, T.P.; Zawada, A.M.; Frankenberger, M.; Skokann, K.; Satzl, A.A.; Gesierich, W.; Schuberth, M.; Levin, J.; Danek, A.; Rotter, B.; et al. Slan-defined subsets of cd16-positive monocytes: Impact of granulomatous inflammation and m-csf receptor mutation. Blood 2015, 126, 2601–2610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofer, T.P.; van de Loosdrecht, A.A.; Stahl-Hennig, C.; Cassatella, M.A.; Ziegler-Heitbrock, L. 6-sulfo lacnac (slan) as a marker for non-classical monocytes. Front. Immunol. 2019, 10, 2052. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, F.; Dobel, T.; Schmitz, M.; Schakel, K. Current concepts on 6-sulfo lacnac expressing monocytes (slanmo). Front. Immunol. 2019, 10, 948. [Google Scholar] [CrossRef] [PubMed]
- Wehner, R.; Lobel, B.; Bornhauser, M.; Schakel, K.; Cartellieri, M.; Bachmann, M.; Rieber, E.P.; Schmitz, M. Reciprocal activating interaction between 6-sulfo lacnac+ dendritic cells and nk cells. Int. J. Cancer 2009, 124, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Oras, A.; Quirant-Sanchez, B.; Popadic, D.; Thunberg, S.; Winqvist, O.; Heck, S.; Cwikowski, M.; Riemann, D.; Seliger, B.; Martinez Caceres, E.; et al. Comprehensive flow cytometric reference intervals of leukocyte subsets from six study centers across europe. Clin. Exp. Immunol. 2020, 202, 363–378. [Google Scholar] [CrossRef]
- Afifi, S.S.; Helal, A.M. Cd11c+ and cd123+ dendritic cell subsets in peripheral blood of lung cancer patients. Egypt J. Immunol. 2009, 16, 9–15. [Google Scholar]
- Patente, T.A.; Pinho, M.P.; Oliveira, A.A.; Evangelista, G.C.M.; Bergami-Santos, P.C.; Barbuto, J.A.M. Human dendritic cells: Their heterogeneity and clinical application potential in cancer immunotherapy. Front. Immunol. 2018, 9, 3176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.B.; Huang, X.; Li, F.R. Impaired dendritic cell functions in lung cancer: A review of recent advances and future perspectives. Cancer Commun. 2019, 39, 43. [Google Scholar] [CrossRef] [Green Version]
- Schneider, T.; Hoffmann, H.; Dienemann, H.; Schnabel, P.A.; Enk, A.H.; Ring, S.; Mahnke, K. Non-small cell lung cancer induces an immunosuppressive phenotype of dendritic cells in tumor microenvironment by upregulating b7-h3. J. Thorac. Oncol. 2011, 6, 1162–1168. [Google Scholar] [CrossRef] [Green Version]
- Mayoux, M.; Roller, A.; Pulko, V.; Sammicheli, S.; Chen, S.; Sum, E.; Jost, C.; Fransen, M.F.; Buser, R.B.; Kowanetz, M.; et al. Dendritic cells dictate responses to pd-l1 blockade cancer immunotherapy. Sci. Transl. Med. 2020, 12, eaav7431. [Google Scholar] [CrossRef]
- Belluomini, L.; Calvetti, L.; Inno, A.; Pasello, G.; Roca, E.; Vattemi, E.; Veccia, A.; Menis, J.; Pilotto, S. Sclc treatment in the immuno-oncology era: Current evidence and unmet needs. Front. Oncol. 2022, 12, 840783. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| SCLC | NSCLC (AC) | NSCLC (SqC) | |
|---|---|---|---|
| Number | 40 | 57 | 27 |
| Age, median (IQR) | 65 (9) | 64 (15) | 67 (8) |
| Sex | |||
| Male, n (%) | 23 (57.5) | 36 (63.2) | 25 (92.6) |
| Female, n (%) | 17 (42.5) | 21 (36.8) | 2 (7.4) |
| ECOG, n (%) | |||
| 0 | 10 (25) | 35 (61.4) | 14 (51.85) |
| 1 | 26 (65) | 22 (38.6) | 13 (48.15) |
| 2 | 4 (10) | 0 | 0 |
| Smoker status | |||
| -Never-smoker | 1 (2.5) | 11 (19.3) | 1 (3.7) |
| -Smoker | 39 (97.5) | 46 (80.7) | 26 (96.3) |
| Metastases, n (%) | |||
| <3 | 17 (42.5) | 26 (45.6) | 17 (63) |
| ≥3 | 23 (57.5) | 31 (54.4) | 10 (37) |
| Brain and/or liver metastases n (%) | 22 (55) | 16 (28.6) | 6 (22.2) |
| Therapy setting: Chemotherapy | Carboplatin + Etoposid | Carboplatin + pemetrexed (TTF-1+) or + nab-Paclitaxel (TTF-1neg.) | Carboplatin + nab-Paclitaxel |
| Therapy setting: ICI + others | Atezolizumab | Pembrolizumab or (if liver metastasis) Atezolizumab + Bevacizumab | Pembrolizumab |
| Radiation before ICI, n (%) | 4 (10) | 6 (10.5) | 3 (11.1) |
| Radiation after ICI, n (%) | 15 (37.5) | 9 (15.8) | 7 (25.9) |
| Clinical response, n (%) | |||
| -Progression/Discontinuation | 6 (15) | 14 (25) | 8 (29.6) |
| -Disease stabilization | 3 (7.5) | 10 (18) | 2 (7.4) |
| -Partial/complete response | 31 (77.5) | 32 (59) | 17 (63) |
| Parameters | Progressive Disease/ Therapy Discontinuation | Clinical Response | p Value |
|---|---|---|---|
| n | 6 | 34 | |
| Neutrophil counts (cells/μL) | 12,950 (9530) | 7540 (3560) | |
| Lymphocyte counts (cells/μL) | 983 (1168) | 1625 (1073) | |
| NLR | 9.3 (6.5) | 5.0 (6.5) | 0.024 |
| CD3+ T cells | 672 (854) | 1075 (1108) | |
| CD19+ B cells | 194 (176) | 178 (181) | |
| NK cells | 67.5 (95) | 237.5 (237) | 0.010 |
| Monocytes (cells/μL) | 748 (478) | 840 (340) | |
| HLA-DRlow MDSC (% of monocytes) | 30.5 (16.1) | 7.9 (22.1) | 0.008 |
| Slan+ non-classical monocytes (% of leukocytes) | 0.17 (0.30) | 0.16 (0.32) | |
| CD1c+ MDC (% of leukocytes) | 0.013 (0.033) | 0.062 (0.074) | 0.019 |
| CD141+ MDC (% of leukocytes) | 0.001 (0.001) | 0.004 (0.005) | 0.001 |
| CD303+ PDC (% of leukocytes) | 0.0095 (0.019) | 0.067 (0.068) | 0.021 |
| Prediction Variable at Baseline | Cutoff Point | AUC | 95% CI | p Value |
|---|---|---|---|---|
| NLR | 6.1 | 0.789 | 0.645–0.934 | 0.025 |
| NK cells (cells/µL) | 150 | 0.824 | 0.671–0.976 | 0.012 |
| HLA-DRlow MDSC (% of monocytes) | 21 | 0.831 | 0.649–1.000 | 0.011 |
| Slan+ non-classical monocytes (% of leukocytes) | 0.12 | 0.576 | ||
| CD1c+ MDC (% of leukocytes) | 0.05 | 0.799 | 0.644–0.954 | 0.021 |
| CD141+ MDC (% of leukocytes) | 0.0015 | 0.887 | 0.782–0.992 | 0.003 |
| CD303+ PDC (% of leukocytes) | 0.014 | 0.792 | 0.628–0.956 | 0.024 |
| A | Cut-Off | n | Kaplan–Meier PFS | Cox Regression, PFS | ||||
|---|---|---|---|---|---|---|---|---|
| % Censored | PFS (Months) | p Value | HR | 95% CI | p Value | |||
| Neutrophil counts (cells/μL) | ≤10,000 | 30 | 23.3 | 10.2 ± 1.4 | 0.002 | 1.44–6.88 | 0.004 | |
| >10,000 | 10 | 0 | 4.0 ± 1.1 | 3.14 | ||||
| NLR | <6.1 | 19 | 31.6 | 12.3 ± 1.8 | 0.001 | 1.46–6.54 | 0.003 | |
| ≥6.1 | 21 | 4.8 | 5.1 ± 0.77 | 3.04 | ||||
| HLA-DRlow MDSC (% of monocytes) | <21 | 30 | 23.3 | 10.0 ±1.4 | 0.012 | 1.14–5.19 | 0.021 | |
| ≥21 | 10 | 0 | 4.4 ± 1.3 | 2.44 | ||||
| Slan+ monocytes (% of leukocytes) | <0.12 | 13 | 0 | 5.6 ± 0.93 | 0.038 | 2.03 | 0.99–4.16 | 0.053 |
| ≥0.12 | 27 | 25.9 | 10.2 ± 1.6 | |||||
| CD1c+ MDC (% of leukocytes) | <0.05 | 19 | 9.5 | 5.4 ± 0.8 | 0.017 | 2.24 | 1.09–4.57 | 0.028 |
| ≥0.05 | 21 | 26.3 | 11.4 ± 1.7 | |||||
| Baseline risk score | 0–2 risk factors | 22 | 31.8 | 12.1 ± 1.7 | <0.001 | 1.67–7.06 | <0.001 | |
| 3–5 risk factors | 18 | 0 | 4.6 ± 0.8 | 3.43 | ||||
| B | Cut-off | n | Kaplan–Meier OS | Cox Regression, OS | ||||
| % Censored | OS (Months) | pValue | HR | 95% CI | pValue | |||
| Neutrophil counts (cells/μL) | ≤10,000 | 30 | 23.3 | 12.2 ± 1.2 | <0.001 | 1.75–8.89 | <0.001 | |
| >10,000 | 10 | 0 | 5.2 ± 1.3 | 3.95 | ||||
| NLR | <6.1 | 19 | 31.6 | 14.0 ± 1.7 | 0.001 | 1.45–6.99 | 0.004 | |
| ≥6.1 | 21 | 4.8 | 7.1 ± 1.0 | 3.18 | ||||
| HLA-DRlow MDSC (% of monocytes) | <21 | 30 | 23.3 | 11.9 ± 1.3 | 0.010 | 1.15–5.33 | 0.020 | |
| ≥21 | 10 | 0.0 | 6.0 ± 1.5 | 2.48 | ||||
| Slan+ monocytes (% of leukocytes) | <0.12 | 13 | 0 | 6.7 ± 1.1 | 0.007 | 2.51 | 1.20–5.24 | 0.014 |
| ≥0.12 | 27 | 25.9 | 12.3 ± 1.4 | |||||
| CD1c+ MDC (% of leukocytes) | <0.05 | 19 | 9.5 | 7.6 ± 1.2 | 0.027 | 2.08 | 1.03–4.20 | 0.041 |
| ≥0.05 | 21 | 26.3 | 13.2 ± 1.6 | |||||
| Baseline risk score | 0–2 risk factors | 22 | 31.8 | 13.8 ± 1.5 | <0.001 | 1.54–6.76 | 0.002 | |
| 3–5 risk factors | 18 | 0 | 6.5 ± 1.04 | 3.23 | ||||
| Baseline Blood Immune Cells | Correlation Coefficient | p Value |
|---|---|---|
| Neutrophil number with monocyte count | 0.560 | <0.001 |
| Neutrophil number with percentage of HLA-DRlow MDSC | 0.571 | <0.001 |
| Neutrophil number with frequency of slan+ non-classical monocytes | −0.629 | <0.001 |
| Neutrophil number with frequency of CD1c+ MDC | −0.610 | <0.001 |
| Neutrophil number with frequency of CD303+ PDC | −0.463 | 0.003 |
| HLA-DRlow MDSC with frequency of slan+ non-classical monocytes | −0.527 | <0.001 |
| HLA-DRlow MDSC with frequency of CD1c+ MDC | −0.655 | <0.001 |
| HLA-DRlow MDSC with frequency of CD303+ PDC | −0.629 | <0.001 |
| slan+ non-classical monocytes with frequency of CD1c+ MDC | 0.506 | <0.001 |
| Blood immune cells at third cycle of therapy | ||
| Neutrophil number with percentage of HLA-DRlow MDSC | 0.553 | <0.001 |
| Neutrophil number with frequency of slan+ non-classical monocytes | −0.691 | <0.001 |
| Neutrophil number with frequency of CD1c+ MDC | −0.727 | <0.001 |
| HLA-DRlow MDSC with frequency of slan+ non-classical monocytes | −0.767 | <0.001 |
| HLA-DRlow MDSC with frequency of CD1c+ MDC | −0.663 | <0.001 |
| slan+ non-classical monocytes with frequency of CD1c+ MDC | 0.721 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riemann, D.; Turzer, S.; Ganchev, G.; Schütte, W.; Seliger, B.; Möller, M. Monitoring Blood Immune Cells in Patients with Advanced Small Cell Lung Cancer Undergoing a Combined Immune Checkpoint Inhibitor/Chemotherapy. Biomolecules 2023, 13, 190. https://doi.org/10.3390/biom13020190
Riemann D, Turzer S, Ganchev G, Schütte W, Seliger B, Möller M. Monitoring Blood Immune Cells in Patients with Advanced Small Cell Lung Cancer Undergoing a Combined Immune Checkpoint Inhibitor/Chemotherapy. Biomolecules. 2023; 13(2):190. https://doi.org/10.3390/biom13020190
Chicago/Turabian StyleRiemann, Dagmar, Steffi Turzer, Georgi Ganchev, Wolfgang Schütte, Barbara Seliger, and Miriam Möller. 2023. "Monitoring Blood Immune Cells in Patients with Advanced Small Cell Lung Cancer Undergoing a Combined Immune Checkpoint Inhibitor/Chemotherapy" Biomolecules 13, no. 2: 190. https://doi.org/10.3390/biom13020190