
Expression of Major Lipid Raft Protein Raftlin in Chronic Rhinosinusitis with Nasal Polyps in Smoking and Non-Smoking Patients Correlated with Interleukin-17 and Tumor Necrosis Factor-α Levels
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Measurement of IL-17 and TNF-α
2.3. Measurement of Human Raftlin
2.4. Tissue Microarray
2.5. Statistical Analysis
3. Results
3.1. Patient Demographics
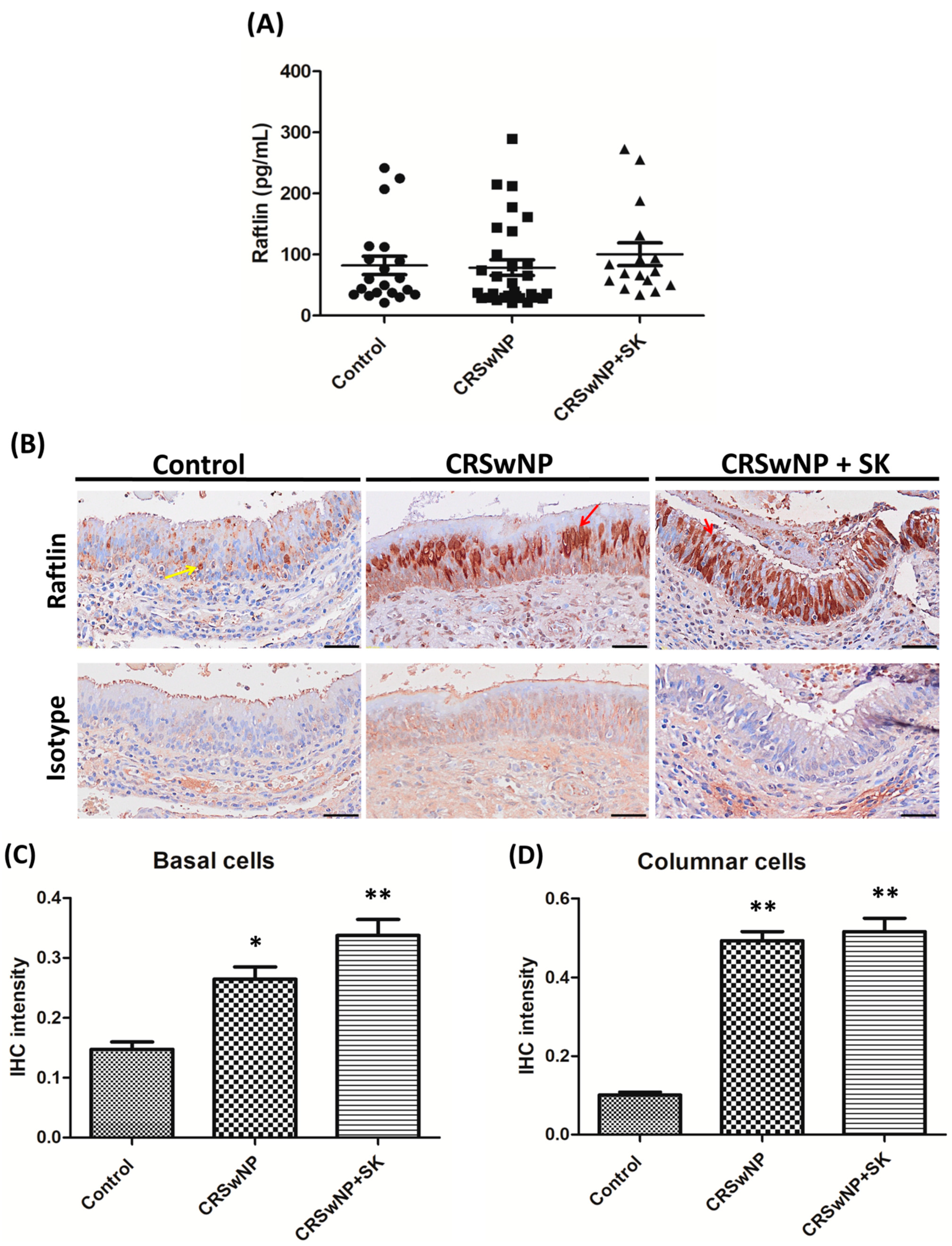
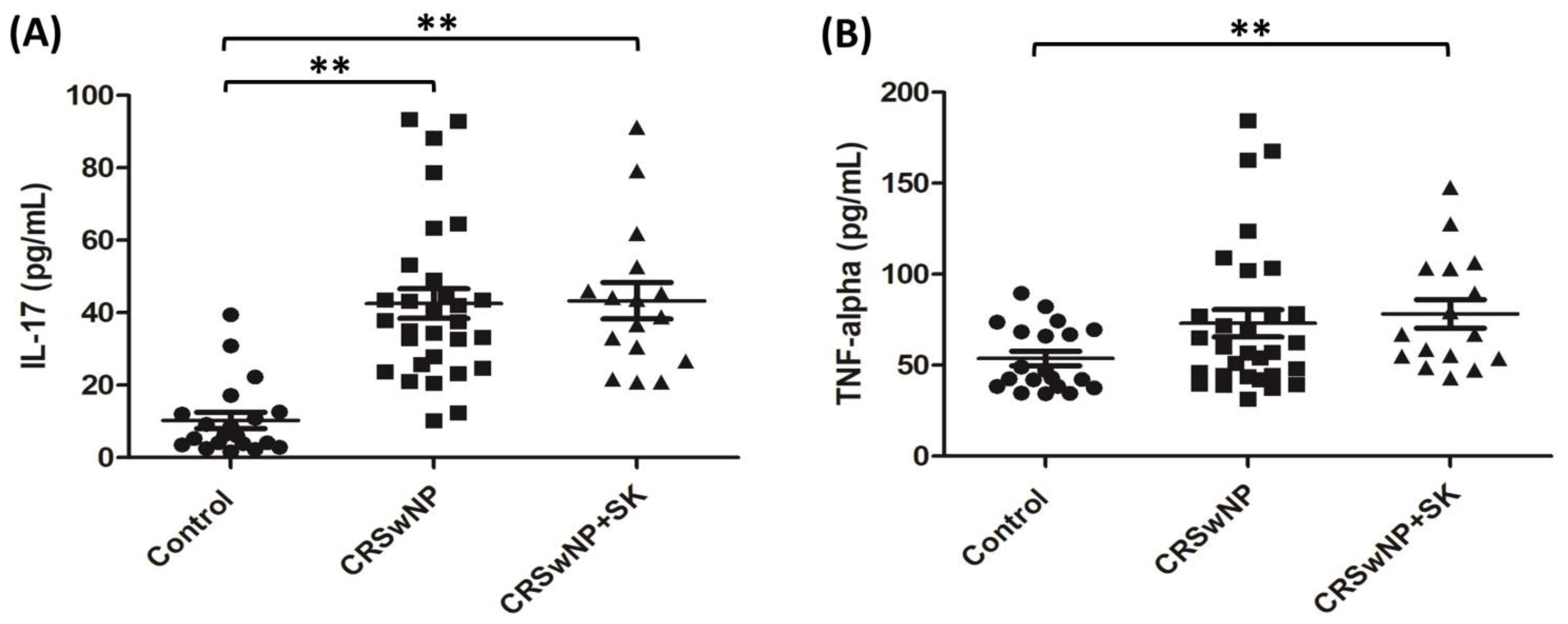
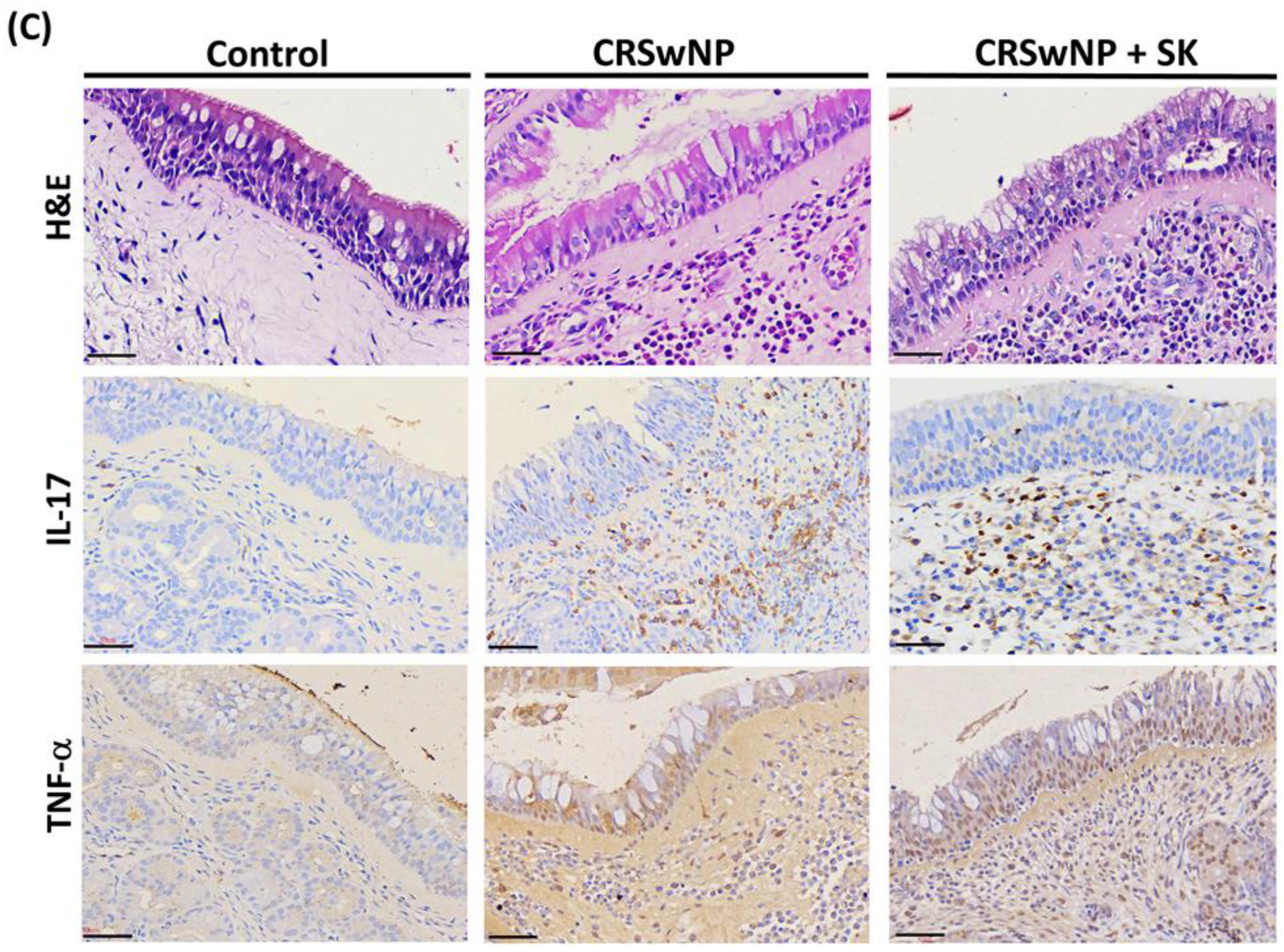
3.2. Expression of Raftlin in CRSwNP and Smoking
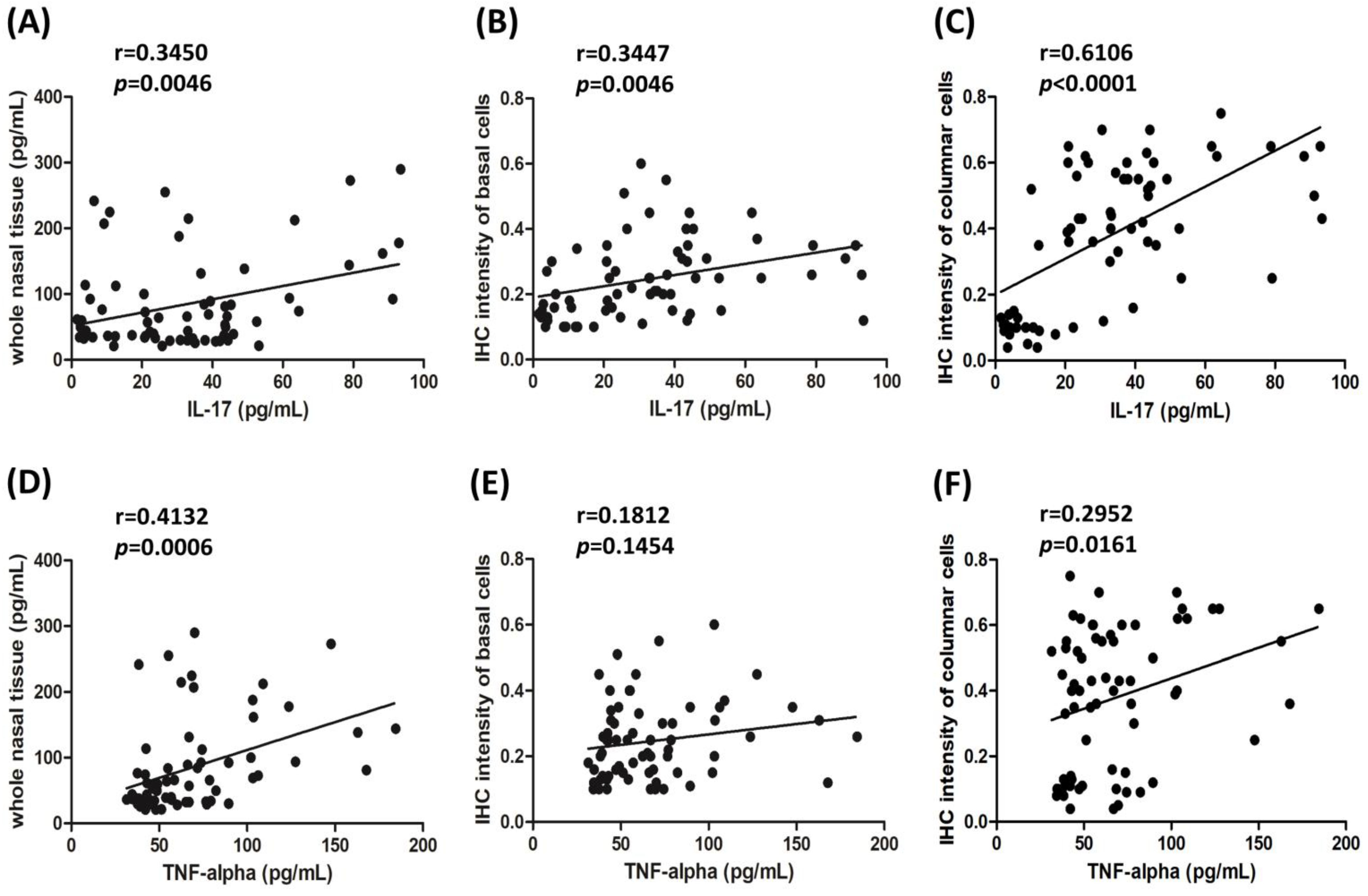
3.3. The Levels of IL-17 and TNF-α Correlated with Raftlin
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. EPOS 2020: European position paper on rhinosinusitis and nasal polyps 2020. Rhinology 2020, 58 (Suppl. S29), 1–464. [Google Scholar] [CrossRef] [PubMed]
- Tomassen, P.; Vandeplas, G.; Van Zele, T.; Cardell, L.O.; Arebro, J.; Olze, H.; Förster-Ruhrmann, U.; Kowalski, M.L.; Olszewska-Ziąber, A.; Holtappels, G.; et al. Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers. J. Allergy Clin. Immun. 2016, 137, 1449–1456. [Google Scholar] [CrossRef] [PubMed]
- Radajewski, K.; Wierzchowska, M.; Grzanka, D.; Antosik, P.; Zdrenka, M.; Burduk, P. Tissue remodelling in chronic rhinosinusitis–Review of literature. Otolaryngol. Pol. 2019, 73, 1–4. [Google Scholar]
- Samitas, K.; Carter, A.; Kariyawasam, H.H.; Xanthou, G. Upper and lower airway remodelling mechanisms in asthma, allergic rhinitis and chronic rhinosinusitis: The one airway concept revisited. Allergy 2018, 73, 993–1002. [Google Scholar] [CrossRef]
- Van Bruaene, N.; Bachert, C. Tissue remodeling in chronic rhinosinusitis. Curr. Opin. Allergy Clin. Immunol. 2011, 11, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.A.; Pulsipher, A.; Gabrielsen, D.A.; Alt, J.A. Biologics in chronic rhinosinusitis: An update and thoughts for future directions. Am. J. Rhinol. Allergy 2018, 32, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Lai, X.P.; Li, X.; Chang, L.H.; Chen, X.H.; Huang, Z.Z.; Bao, H.W.; Huang, J.C.; Yang, L.Y.; Wu, X.F.; Wang, Z.Y.; et al. IL-19 Up-Regulates Mucin 5AC Production in Patients With Chronic Rhinosinusitis via STAT3 Pathway. Front. Immunol. 2019, 10, 1682. [Google Scholar] [CrossRef]
- Workman, A.D.; Kohanski, M.A.; Cohen, N.A. Biomarkers in Chronic Rhinosinusitis with Nasal Polyps. Immunol. Allergy Clin. 2018, 38, 679–692. [Google Scholar] [CrossRef]
- Yang, Y.; Zhang, N.; Crombruggen, K.V.; Lan, F.; Hu, G.; Hong, S.; Bachert, C. Differential Expression and Release of Activin A and Follistatin in Chronic Rhinosinusitis with and without Nasal Polyps. PLoS ONE 2015, 10, e0128564. [Google Scholar] [CrossRef]
- Ishida, A.; Ohta, N.; Suzuki, Y.; Kakehata, S.; Okubo, K.; Ikeda, H.; Shiraishi, H.; Izuhara, K. Expression of pendrin and periostin in allergic rhinitis and chronic rhinosinusitis. Allergol. Int. 2012, 61, 589–595. [Google Scholar] [CrossRef]
- Saeki, K.; Miura, Y.; Aki, D.; Kurosaki, T.; Yoshimura, A. The B cell-specific major raft protein, Raftlin, is necessary for the integrity of lipid raft and BCR signal transduction. EMBO J. 2003, 22, 3015–3026. [Google Scholar] [CrossRef]
- Lee, W.; Yoo, H.; Ku, S.K.; Kim, S.W.; Bae, J.S. Raftlin: A new biomarker in human sepsis. Inflammation 2014, 37, 706–711. [Google Scholar] [CrossRef]
- Bilal, N.; Kurutas, E.B.; Orhan, I.; Bilal, B.; Doganer, A. Evaluation of preoperative and postoperative serum interleukin-6, interleukin-8, tumor necrosis factor α and Raftlin levels in patients with obstructive sleep apnea. Sleep Breath. 2021, 25, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Belce, A.; Ozkan, B.N.; Dumlu, F.S.; Sisman, B.H.; Guler, E.M. Evaluation of Oxidative Stress and Inflammatory Biomarkers Pre and Post-Treatment in New Diagnosed Atherosclerotic Patients. Clin. Exp. Hypertens. 2022, 17, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Saeki, K.; Fukuyama, S.; Ayada, T.; Nakaya, M.; Aki, D.; Takaesu, G.; Hanada, T.; Matsumura, Y.; Kobayashi, T.; Nakagawa, R.; et al. A major lipid raft protein Raftlin modulates T cell receptor signaling and enhances th17-mediated autoimmune responses. J. Immunol. 2009, 182, 5929–5937. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Gumlaw, N.; Karman, J.; Zhao, H.; Zhang, J.; Jiang, J.L.; Maniatis, P.; Edling, A.; Chuang, W.L.; Siegel, C.; et al. Lowering glycosphingolipid levels in CD4+ T cells attenuates T cell receptor signaling, cytokine production, and differentiation to the Th17 lineage. J. Biol. Chem. 2011, 286, 14787–14794. [Google Scholar] [CrossRef]
- Bilgen, F.; Ural, A.; Kurutas, E.B.; Bekerecioglu, M. The effect of oxidative stress and Raftlin levels on wound healing. Int. Wounds J. 2019, 16, 1178–1184. [Google Scholar] [CrossRef]
- Huang, C.C.; Wang, C.H.; Fu, C.H.; Huang, C.C.; Chang, P.H.; Chen, Y.W.; Wu, C.C.; Wu, P.W.; Lee, T.J. Association between cigarette smoking and interleukin-17A expression in nasal tissues of patients with chronic rhinosinusitis and asthma. Medicine 2016, 95, e5432. [Google Scholar] [CrossRef]
- Lund, V.J.; Mackay, I.S. Staging in rhinosinusitus. Rhinology 1993, 31, 183–184. [Google Scholar]
- Davies, D.E. The Role of the Epithelium in Airway Remodeling in Asthma. Proc. Am. Thorac. Soc. 2009, 6, 678–682. [Google Scholar] [CrossRef]
- Lee, K.; Tai, J.; Lee, S.H.; Kim, T.H. Advances in the Knowledge of the Underlying Airway Remodeling Mechanisms in Chronic Rhinosinusitis Based on the Endotypes: A Review. Int. J. Mol. Sci. 2021, 22, 910. [Google Scholar] [CrossRef] [PubMed]
- Uhliarova, B.; Adamkov, M.; Svec, M.; Calkovska, A. The effect of smoking on CT score, bacterial colonization and distribution of inflammatory cells in the upper airways of patients with chronic rhinosinusitis. Inhal. Toxicol. 2014, 26, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishnan, V.R.; Frank, D.N. Impact of cigarette smoking on the middle meatus microbiome in health and chronic rhinosinusitis. Int. Forum. Allergy Rhinol. 2015, 5, 981–989. [Google Scholar] [CrossRef]
- Yee, K.K.; Pribitkin, E.A.; Cowart, B.J.; Vainius, A.A.; Klock, C.T.; Rosen, D.; Hahn, C.G.; Rawson, N.E. Smoking-associated squamous metaplasia in olfactory mucosa of patients with chronic rhinosinusitis. Toxicol. Pathol. 2009, 37, 594–598. [Google Scholar] [CrossRef] [PubMed]
- Yamin, M.; Holbrook, E.H.; Gray, S.T.; Busaba, N.Y.; Lovett, B.; Hamilos, D.L. Profibrotic transforming growth factor beta 1 and activin A are increased in nasal polyp tissue and induced in nasal polyp epithelium by cigarette smoke and Toll-like receptor 3 ligation. Int. Forum. Allergy Rhinol. 2015, 5, 573–582. [Google Scholar] [CrossRef]
- Xie, L.; Liu, A.G.; Peng, L.Y.; Wang, S.J.; Zhang, Y.P.; Wang, X.S. Expression of E-prostanoid receptors in nasal polyp tissues of smoking and nonsmoking patients with chronic rhinosinusitis. PLoS ONE 2018, 13, e0200989. [Google Scholar] [CrossRef]
- Boonpiyathad, T.; Sözener, Z.C.; Satitsuksanoa, P.; Akdis, C.A. Immunologic mechanisms in asthma. Semin. Immunol. 2019, 46, 101333. [Google Scholar] [CrossRef]
- Churg, A.; Dai, J.; Tai, H.; Xie, C.; Wright, J.L. Tumor necrosis factor-alpha is central to acute cigarette smoke-induced inflammation and connective tissue breakdown. Am. J. Respir. Crit. Care Med. 2002, 166, 849–854. [Google Scholar] [CrossRef]
- Hodge, S.; Matthews, G.; Mukaro, V.; Ahern, J.; Shivam, A.; Hodge, G.; Holmes, M.; Jersmann, H.; Reynolds, P.N. Cigarette smoke-induced changes to alveolar macrophage phenotype and function are improved by treatment with procysteine. Am. J. Respir. Cell. Mol. Biol. 2011, 44, 673–681. [Google Scholar] [CrossRef]
- Liu, Y.; Zeng, M.; Liu, Z. Th17 response and its regulation in inflammatory upper airway diseases. Clin. Exp. Allergy 2015, 45, 602–612. [Google Scholar] [CrossRef]
- Mukhopadhyay, S.; Hoidal, J.R.; Mukherjee, T.K. Role of TNF-alpha in pulmonary pathophysiology. Respir. Res. 2006, 7, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Kumbul, Y.Ç.; Yasan, H.; Okur, E.; Tüz, M.; Sivrice, M.E.; Akın, V.; Şirin, F.B.; Doğan Kıran, E. The role of Raftlin in the pathogenesis of chronic rhinosinusitis with nasal polyps. Eur. Arch. Otorhinolaryngol. 2022, 279, 3519–3523. [Google Scholar] [CrossRef]
- Thomson, N.C.; Chaudhuri, R.; Livingston, E. Asthma and cigarette smoking. Eur. Respir. J. 2004, 24, 822–833. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.C.; Lee, T.J.; Huang, C.C.; Chang, P.H.; Fu, C.H.; Wu, P.W.; Wang, C.H. Impact of cigarette smoke and IL-17A activation on asthmatic patients with chronic rhinosinusitis. Rhinology 2019, 57, 57–66. [Google Scholar] [CrossRef]
- Zhang, Y.; Gevaert, E.; Lou, H.; Wang, X.; Zhang, L.; Bachert, C.; Zhang, N. Chronic rhinosinusitis in Asia. J. Allergy. Clin. Immunol. 2017, 140, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Mfuna-Endam, L.; Zhang, Y.; Desrosiers, M.Y. Genetics of rhinosinusitis. Curr. Allergy Asthma Rep. 2011, 11, 236–246. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | Subjects | |||
|---|---|---|---|---|
| Variables | Control (n = 20) | CRSwNP (n = 30) | CRSwNP + SK (n = 16) | p Value |
| Gender (male), n (%) | 12 (60.0) | 19 (63.3) | 12 (75.0) | 0.6185 |
| Age (years), Mean ± SE | 38.9 ± 2.8 | 48.3 ± 2.7 | 49.7 ± 3.5 | 0.6100 |
| Peripheral eosinophil (%), Mean ± SE | 3.2 ± 0.5 | 3.8 ± 0.5 | 3.3 ± 0.5 | 0.5315 |
| Serum IgE level (KU/L), Mean ± SE | 78.8 ± 12.8 | 116.9 ± 20.0 | 250.9 ± 36.4 | <0.001 * |
| LMK-CT score | - | 15.0 ± 0.9 | 15.6 ± 1.2 | 0.2686 & |
| Methodologies used | - | |||
| Tissue ELISA (n) | 20 | 30 | 16 | |
| Tissue IHC (n) | 20 | 30 | 16 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-T.; Tsai, M.-H.; Su, Y.-Y.; Chen, W.-C.; Huang, S.-C.; Chien, C.-Y. Expression of Major Lipid Raft Protein Raftlin in Chronic Rhinosinusitis with Nasal Polyps in Smoking and Non-Smoking Patients Correlated with Interleukin-17 and Tumor Necrosis Factor-α Levels. Biomolecules 2022, 12, 1316. https://doi.org/10.3390/biom12091316
Lin Y-T, Tsai M-H, Su Y-Y, Chen W-C, Huang S-C, Chien C-Y. Expression of Major Lipid Raft Protein Raftlin in Chronic Rhinosinusitis with Nasal Polyps in Smoking and Non-Smoking Patients Correlated with Interleukin-17 and Tumor Necrosis Factor-α Levels. Biomolecules. 2022; 12(9):1316. https://doi.org/10.3390/biom12091316
Chicago/Turabian StyleLin, Yu-Tsai, Ming-Hsien Tsai, Yan-Ye Su, Wei-Chih Chen, Shun-Chen Huang, and Chih-Yen Chien. 2022. "Expression of Major Lipid Raft Protein Raftlin in Chronic Rhinosinusitis with Nasal Polyps in Smoking and Non-Smoking Patients Correlated with Interleukin-17 and Tumor Necrosis Factor-α Levels" Biomolecules 12, no. 9: 1316. https://doi.org/10.3390/biom12091316