
Clozapine: Why Is It So Uniquely Effective in the Treatment of a Range of Neuropsychiatric Disorders?


Abstract
:1. Introduction
1.1. Clozapine
1.2. Electroconvulsive Therapy (ECT)
1.3. Clozapine, Seizures, and Neurogenesis
1.4. Search Strategy
2. Effects of Clozapine and ECT on Neuropsychiatric Disorders
2.1. Clozapine and Schizophrenia Spectrum Disorders
2.2. ECT Augmentation in Schizophrenia Spectrum Disorders
2.3. Clozapine and Bipolar Disorder
2.4. ECT and Bipolar Disorder
2.5. Clozapine and Major Depressive Disorder (MDD)
2.6. ECT and Major Depressive Disorder (MDD)
2.7. Clozapine and Parkinson’s Disease (PD)
2.8. ECT and PD
3. Other Factors Relevant to the Effects of Clozapine and ECT on Neuropsychiatric Disorders
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Hippius, H. A historical perspective of clozapine. J. Clin. Psychiatry 1999, 60 (Suppl. 12), 22–23. [Google Scholar] [PubMed]
- Seeman, P. Clozapine, a fast-off-D2 antipsychotic. ACS Chem. Neurosci. 2014, 5, 24–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grover, S.; Dutt, A.; Avasthi, A. Indian research: Focus on clozapine. Indian J. Psychiatry 2010, 52, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Kane, J.; Honigfeld, G.; Singer, J.; Meltzer, H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch. Gen. Psychiatry 1988, 45, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Claghorn, J.; Honigfeld, G.; Abuzzahab, F.S.; Wang, R.; Steinbook, R.; Tuason, V.; Klerman, G. The risks and benefits of clozapine versus chlorpromazine. J. Clin. Psychopharmacol. 1987, 7, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Khokhar, J.Y.; Henricks, A.M.; Kirk, E.; Green, A.I. Unique effects of clozapine: A pharmacological perspective. Adv. Pharmacol. 2018, 82, 137–162. [Google Scholar] [PubMed]
- Kim, D.D.; Barr, A.M.; Lu, C.; Stewart, S.E.; White, R.F.; Honer, W.G.; Procyshyn, R.M. Clozapine-associated obsessive-compulsive symptoms and their management: A systematic review and analysis of 107 reported cases. Psychother. Psychosomat. 2020, 89, 151–160. [Google Scholar] [CrossRef] [PubMed]
- De Leon, J.; Ruan, C.-J.; Schoretsanitis, G.; De Las Cuevas, C. A rational use of clozapine based on adverse drug reactions, pharmacokinetics, and clinical pharmacopsychology. Psychother. Pscychosom. 2020, 89, 200–214. [Google Scholar] [CrossRef] [PubMed]
- Yuen, J.W.Y.; Kim, D.D.; Procyshyn, R.M.; Panenka, W.J.; Honer, W.G.; Barr, A.M. A focused review of the metabolic side-efects of clozapine. Front. Endocrinol. 2021, 12, 609240. [Google Scholar] [CrossRef]
- Wenthur, C.J.; Lindsley, C.W. Classics in chemical neuroscience: Clozapine. ACS Chem. Neurosci. 2013, 4, 1018–1025. [Google Scholar] [CrossRef] [Green Version]
- Stepnicki, P.; Kondej, M.; Kaczor, A.A. Current concepts and treatments of schizophrenia. Molecules 2018, 23, 2087. [Google Scholar] [CrossRef] [Green Version]
- Nasrallah, H.A. Atypical antipsychotic-induced metabolic side effects: Insights from receptor-binding profiles. Mol. Psychiatry 2008, 13, 27–35. [Google Scholar] [CrossRef]
- Kapur, S.; Seeman, P. Does fast dissociation from the dopamine D2 receptor explain the action of atypical antipsychotics? A new hypothesis. Am. J. Pychiatry 2001, 158, 360–369. [Google Scholar] [CrossRef]
- Meltzer, H.Y.; Li, Z.; Kaneda, Y.; Ichikawa, J. Serotonin receptors: Their key role in drugs to treat schizophrenia. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2003, 27, 1159–1171. [Google Scholar] [CrossRef]
- Willcocks, I.R.; Legge, S.E.; Nalmpanti, M.; Mazzeo, L.; King, A.; Jansen, J.; Helthuis, M.; Owen, M.J.; O’Donovan, M.C.; Walters, J.T.R.; et al. Clozapine metabolism is associated with absolute neurotrophil count in individuals with treatment-resistant schizophrenia. Front. Pharmacol. 2021, 12, 658734. [Google Scholar] [CrossRef]
- Jiang, L.; Wu, X.; Wang, S.; Chen, S.-H.; Zhou, H.; Wilson, B.; Jin, C.-Y.; Lu, R.-B.; Xie, K.; Wang, Q.; et al. Clozapine metabolites protect dopaminergic neurons through inhibition of microglial NADPH oxidase. J. Neuroinflamm. 2016, 13, 110. [Google Scholar] [CrossRef] [Green Version]
- Food and Drug Administration. Clozaril: Novartis Pharmaceuticals Corporation. 2010. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/019758s062lbl.pdf (accessed on 1 May 2021).
- Young, C.R.; Longhurst, J.G.; Bowers, M.B.; Mazure, C.M. The expanding indications for clozapine. Exp. Clin. Psychopharmacol. 1997, 5, 216–234. [Google Scholar] [CrossRef]
- Tiihonen, J.; Tanskanen, A.; Hoti, F.; Vattulainen, P.; Taipale, H.; Mehtälä, J.; Lähteenvuo, M. Pharmacological treatments and risk of readmission to hospital for unipolar depression in Finland: A nationwide cohort study. Lancet Psychiatry 2017, 4, 547–553. [Google Scholar] [CrossRef]
- Baghai, T.C.; Möller, H.-J. Electroconvulsive therapy and its different indications. Dialogues Clin. Neurosci. 2008, 10, 105–117. [Google Scholar]
- NIMH. U.S. Department of Health and Human Services, National Institutes of Health, Brain Stimulation Therapies. Available online: https://www.nimh.nih.gov/health/topics/brain-stimulation-therapies/brain-stimulation-therapies.shtml (accessed on 5 May 2021).
- Li, M.; Yao, X.; Sun, L.; Zhao, L.; Xu, W.; Zhao, H.; Zhao, F.; Zou, X.; Cheng, Z.; Li, B.; et al. Effects of electroconvulsive therapy on depression and its potential mechanism. Front. Psychol. 2020, 11, 80. [Google Scholar] [CrossRef] [Green Version]
- Haskett, R.F. Electroconvulsive therapy’s mechanism of action: Neuroendocrine hypotheses. J. ECT 2014, 30, 107–110. [Google Scholar] [CrossRef]
- Schloesser, R.J.; Orvoen, S.; Jimenez, D.V.; Hardy, N.F.; Maynard, K.R.; Sukumar, M.; Manji, H.K.; Gardier, A.M.; David, D.J.; Martinowich, K. Antidepressant-like effects of electroconvulsive seizures require adult neurogenesis in a neuroendocrine model of depression. Brain Stimul. 2015, 8, 862–867. [Google Scholar] [CrossRef] [Green Version]
- Stevens, J.R.; Denney, D.; Szot, P. Kindling with clozapine: Behavioral and molecular consequences. Epilepsy Res. 1996, 26, 295–304. [Google Scholar] [CrossRef]
- Varma, S.; Bishara, D.; Besag, F.M.C.; Taylor, D. Clozapine-related EEG changes and seizures: Dose and plasma-level relationships. Ther. Adv. Psychopharmacol. 2011, 1, 47–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, D.M.; Van Cott, A.C. Clozapine (Clozaril), seizures, and EEG abnormalities. Am. J. Electroneurodiagn. Technol. 2007, 47, 190–197. [Google Scholar] [CrossRef]
- Jackson, A.; Seneviratne, U. EEG changes in patients on antipsychotic therapy: A systematic review. Epilepsy Behav. 2019, 95, 1–9. [Google Scholar] [CrossRef]
- Stevens, J.R.; Denney, D.; Szot, P. Sensitization with clozapine: Beyond the dopamine hypothesis. Biol. Psychiatry 1997, 42, 771–780. [Google Scholar] [CrossRef]
- Denney, D.; Stevens, J.R. Clozapine and seizures. Biol. Psychiatry 1995, 37, 427–433. [Google Scholar] [CrossRef]
- Aringhieri, S.; Kolachalam, S.; Gerace, C.; Carli, M.; Verdesca, V.; Brunacci, M.G.; Rossi, C.; Ippolito, C.; Solini, A.; Corsini, G.U.; et al. Clozapine as the most efficacious antipsychotic for activating ERK 1/2 kinases: Role of 5-HT2A receptor agonism. Eur. Neuropsychopharmacol. 2017, 27, 383–398. [Google Scholar] [CrossRef] [PubMed]
- Wilkowska, A.; Cubała, W.J. Clozapine as transformative treatment in bipolar patients. Neuropsychiatr. Dis. Treat. 2019, 15, 2901–2905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertson, O.D.; Coronado, N.G.; Sethi, R.; Berk, M.; Dodd, S. Putative neuroprotective pharmacotherapies to target the staged progression of mental illness. Early Interven. Psychiatry 2019, 13, 1032–1049. [Google Scholar] [CrossRef]
- Leung, C.C.-Y.; Gadelrab, R.; Ntephe, C.U.; McGuire, P.K.; Demjaha, A. Clinical course, neurobiology and therapeutic approaches to treatment resistant schizophrenia. Toward an integrated view. Front. Psychiatry 2019, 10, 601. [Google Scholar] [CrossRef]
- Nucifora, F.C.; Mihaljevic, M.; Lee, B.J.; Sawa, A. Clozapine as a model for antipsychotic development. Neurotherapeutics 2017, 14, 1750–1751. [Google Scholar] [CrossRef] [Green Version]
- Meltzer, H.Y. An overview of the mechanism of action of clozapine. J. Clin. Psychiatry 1994, 55 (Suppl. B), 47–52. [Google Scholar]
- Okhuijsen-Pfeifer, C.; Sterk, A.Y.; Horn, I.M.; Terstappen, J.; Kahn, R.S.; Luykx, J.J. Demographic and clinical features as predictors of clozapine response in patients with schizophrenia spectrum disorders: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2020, 111, 246–252. [Google Scholar] [CrossRef]
- Nair, P.C.; McKinnon, R.A.; Miners, J.O.; Bastiampillai, T. Binding of clozapine to the GABAB receptor: Clinical and structural insights. Mol. Psychiatry 2020, 25, 1910–1919. [Google Scholar] [CrossRef]
- Kaster, T.S.; de Jesus, D.; Radhu, N.; Farzan, F.; Blumberger, D.M.; Rajji, T.K.; Fitzgerald, P.B.; Daskalakis, Z.J. Clozapine potentiation of GABA mediated cortical inhibition in treatment resistant schizophrenia. Schizophr. Res. 2015, 165, 157–162. [Google Scholar] [CrossRef]
- Marx, C.E.; Shampine, L.J.; Duncan, G.E.; VanDoren, M.J.; Grobin, A.C.; Massing, M.W.; Madison, R.D.; Bradford, D.W.; Butterfield, M.I.; Lieberman, J.A.; et al. Clozapine markedly elevates pregnenolone in rat hippocampus, cerebral cortex, and serum: Candidate mechanism for superior efficacy? Pharmacol. Biochem. Behav. 2006, 84, 598–608. [Google Scholar] [CrossRef]
- Marx, C.E.; VanDoren, M.J.; Duncan, G.E.; Lieberman, J.A.; Morrow, A.L. Olanzapine and clozapine increase the GABAergic neuroactive steroid allopregnanolone in rodents. Neuropsychopharmacology 2003, 28, 1–13. [Google Scholar] [CrossRef]
- Fukuyama, K.; Kato, R.; Murata, M.; Shiroyama, T.; Okada, M. Clozapine normalizes a glutamatergic transmission abnormality induced by an impaired NMDA receptor in the thalamocortical pathway via the activation of a Group III metabotropic glutamate receptor. Biomolecules 2019, 9, 234. [Google Scholar] [CrossRef] [Green Version]
- Gray, L.; van den Buuse, M.; Scarr, E.; Dean, B.; Hannan, A.J. Clozapine reverses schizophrenia-related behaviours in the metabotropic glutamate receptor 5 knockout mouse: Association with N-methyl-D-aspartic acid receptor up-regulation. Int. J. Neuropsychopharmacol. 2009, 12, 45–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koshiyama, D.; Kirihara, K.; Tada, M.; Nagai, T.; Fujioka, M.; Ichikawa, E.; Ohta, K.; Tani, M.; Tsuchiya, M.; Kanehara, A.; et al. Electrophysiological evidence for abnormal glutamate-GABA association following psychosis onset. Transl. Psychiatry 2018, 8, 211. [Google Scholar] [CrossRef] [PubMed]
- Duman, R.S.; Sanacora, G.; Krystal, J.H. Altered connectivity in depression: GABA and glutamate neurotransmitter deficits and reversal by novel treatments. Neuron 2019, 102, 75. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.D.; Barr, A.M.; Honer, W.G.; Procyshyn, R.M. Reversal of dopamine supersensitivity as a mechanism of action of clozapine. Psychother. Psychosom. 2018, 87, 306–307. [Google Scholar] [CrossRef]
- Grover, S.; Sahoo, S.; Rabha, A.; Koirala, R. ECT in schizophrenia: A review of the evidence. Acta Neuropsychiatr. 2019, 31, 115–127. [Google Scholar] [CrossRef]
- Rothärmel, M.; Krir, M.W.; Moulier, V.; Védrine, M.-G.; Compere, V.; Guillin, O. Electroconvulsive therapy in ultra-resistant schizophrenia: A case series. Asian J. Psychiatry 2019, 44, 6–7. [Google Scholar] [CrossRef]
- Grover, S.; Shouan, A.; Chakrabarti, S.; Sahoo, S.; Mehra, A. Comparative study of the effectiveness of augmentation with ECT in clozapine resistant schizophrenia (CRS) and non-clozapine resistant schizophrenia (Non-CRS). Nord. J. Psychiatry 2021. [Google Scholar] [CrossRef]
- Lally, J.; Breese, E.; Osman, M.; Hua Sim, C.; Shetty, H.; Krivoy, A.; MacCabe, J.H. Augmentation of clozapine with ECT: A retrospective case analysis. Acta Neuropsychiatr. 2021, 33, 31–36. [Google Scholar] [CrossRef]
- Wang, G.; Zheng, W.; Li, X.-B.; Wang, S.-B.; Cai, D.-B.; Yang, X.-H.; Ungvari, G.S.; Xiang, Y.-T.; Correll, C.U. ECT augmentation of clozapine for clozapine-resistant schizophrenia: A meta-analysis of randomized controlled trials. J. Psychiatr. Res. 2018, 105, 23–32. [Google Scholar] [CrossRef]
- Kim, H.S.; Kim, S.H.; Lee, N.Y.; Youn, T.; Lee, J.H.; Chung, S.; Kim, Y.S.; Chung, I.W. Effectiveness of electroconvulsive therapy. Augmentation on clozapine-resistant schizophrenia. Psychiatry Investig. 2017, 14, 58–62. [Google Scholar] [CrossRef]
- Arumugham, S.S.; Thirthalli, J.; Andrade, C. Efficacy and safety of combining clozapine with electrical or magnetic brain stimulation in treatment-refractory schizophrenia. Expert Rev. Clin. Pharmacol. 2016, 9, 1245–1252. [Google Scholar] [CrossRef]
- Sinclair, D.J.; Zhao, S.; Qi, F.; Nyakyoma, K.; Kwong, J.S.; Adams, C.E. Electroconvulsive therapy for treatment-resistant schizophrenia. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef]
- Moulier, V.; Krir, M.W.; Dalmont, M.; SURECT Group; Guillin, O.; Rothärmel, M. A prospective multicenter assessor-blinded randomized controlled study to compare the efficacy of short versus long protocols of electroconvulsive therapy as an augmentation strategy to clozapine in patients with ultra-resistant schizophrenia (SURECT study). Trials 2021, 22, 284. [Google Scholar]
- Wagner, E.; Kane, J.M.; Correll, C.U.; Howes, O.; Siskind, D.; Honer, W.G.; Lee, J.; Falkai, P.; Schneider-Axmann, T.; Hasan, A.; et al. Clozapine combination and augmentation strategies in patients with schizophrenia—Recommendations from an international expert survey among the Treatment Response and Resistance in Psychosis (TRRIP) working group. Schizophr. Bull. 2020, 46, 1459–1470. [Google Scholar] [CrossRef]
- Sanghani, S.N.; Petrides, G.; Kellner, C.H. Electroconvulsive therapy (ECT) in schizophrenia: A review of recent literature. Curr. Opin. Psychiatry 2018, 31, 213–222. [Google Scholar] [CrossRef]
- Li, X.-B.; Tang, Y.-L.; Wang, C.-Y.; de Leon, J. Clozapine for treatment-resistant bipolar disorder: A systematic review. Bipolar Disord. 2015, 17, 235–247. [Google Scholar] [CrossRef] [PubMed]
- Bymaster, F.P.; Felder, C.C. Role of the cholinergic muscarinic system in bipolar disorder and related mechanism of action of antipsychotic agents. Mol. Psychiatry 2002, 7, S57–S63. [Google Scholar] [CrossRef]
- Poon, S.H.; Sim, K.; Baldessarini, R.J. Pharmacological approaches for treatment-resistant bipolar disorder. Curr. Neuropharmacol. 2015, 13, 592–604. [Google Scholar] [CrossRef] [Green Version]
- Frye, M.A.; Ketter, T.A.; Altshuler, L.L.; Denicoff, K.; Dunn, R.T.; Kimbrell, T.A.; Corá-Locatelli, G.; Post, R.M. Clozapine in bipolar disorder: Treatment implications for other atypical antipsychotics. J. Affect. Disord. 1998, 48, 91–104. [Google Scholar] [CrossRef]
- Yatham, L.N.; Kennedy, S.H.; Parikh, S.V.; Schaffer, A.; Bond, D.J.; Frey, B.N.; Sharma, V.; Goldstein, B.I.; Rej, S.; Beaulieu, S.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018, 20, 97–170. [Google Scholar] [CrossRef]
- Kapczinski, F.; Pfaffenseller, B.; Dursun, S.M.; de Azevedo Cardoso, T. Clozapine for bipolar disorder: What do we know so far and what next? Bipolar Disord. 2021, 23, 115–116. [Google Scholar] [CrossRef] [PubMed]
- Fehr, B.S.; Ozcan, M.E.; Suppes, T. Low doses of clozapine may stabilize treatment–resistant bipolar patients. Eur. Arch. Psychiatry Clin. Neurosci. 2005, 255, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Delgado, A.; Velosa, J.; Zhang, J.; Dursun, S.M.; Kapczinski, F.; de Azevedo Cardoso, T. Clozapine in bipolar disorder: A systematic review and meta-analysis. J. Psychiatr. Res. 2020, 125, 21–27. [Google Scholar] [CrossRef]
- Renzenbrink, M.; Wand, A.P.F. A systematic review of clozapine’s effectiveness for primary psychotic and bipolar disorders in older adults. Int. Psychogeriatr. 2021, 1–13. [Google Scholar] [CrossRef]
- Wilkowska, A.; Wiglusz, M.S.; Cubała, W.J. Clozapine in treatment-resistant bipolar disorder with suicidality. Three case reports. Front. Psychiatry 2019, 10, 520. [Google Scholar] [CrossRef]
- Pillay, S.S.; Stoll, A.L.; Weiss, M.K.; Tohen, M.; Zarate, C.A.; Banov, M.D.; Cole, J.O. EEG abnormalities before clozapine therapy predict a good clinical response to clozapine. Ann. Clin. Psychiatry 1996, 8, 1–5. [Google Scholar] [CrossRef]
- Maletic, V.; Raison, C. Integrated neurobiology of bipolar disorder. Front. Psychiatry 2014, 5, 98. [Google Scholar] [CrossRef]
- Parker, G.B.; Graham, R.K.; Tavella, G. Is there consensus across international evidence-based guidelines for the management of bipolar disorder? Acta Psychiatr. Scand. 2017, 135, 515–526. [Google Scholar] [CrossRef]
- Fagiolini, A.; Coluccia, A.; Maina, G.; Forgione, R.N.; Goracci, A.; Cuomo, A.; Young, A.H. Diagnosis, epidemiology and management of mixed states in bipolar disorder. CNS Drugs 2015, 29, 725–740. [Google Scholar] [CrossRef]
- Kessler, U.; Schoeyen, H.K.; Andreassen, O.A.; Eide, G.E.; Malt, U.F.; Oedegaard, K.J.; Morken, G.; Sundet, K.; Vaaler, A.E. The effect of electroconvulsive therapy on neurocognitive function in treatment-resistant bipolar disorder depression. J. Clin. Psychiatry 2014, 75, e1306–e1313. [Google Scholar] [CrossRef]
- Brancati, G.E.; Tripodi, B.; Novi, M.; Barbuti, M.; Medda, P.; Perugi, G. Association of treatment facets, severity of manic symptoms, psychomotor disturbances and psychotic features with response to electroconvulsive therapy in bipolar depression. World J. Biol. Psychiatry 2020. [Google Scholar] [CrossRef]
- Medda, P.; Barbuti, M.; Novi, M.; Boccolini, A.; Tripodi, B.; De Simone, L.; Perugi, G. Naturalistic follow-up in bipolar patients after successful electroconvulsive therapy. J. Affect. Disord. 2020, 271, 152–159. [Google Scholar] [CrossRef]
- Perugi, G.; Medda, P.; Barbuti, M.; Novi, M.; Tripodi, B. The role of electroconvulsive therapy in the treatment of severe bipolar mixed state. Psychiatr. Clin. N. Am. 2020, 43, 187–197. [Google Scholar] [CrossRef]
- Morcos, N.; Maixner, S.; Maixner, D.F. Electroconvulsive therapy for bipolar depression in older adults. J. ECT 2021, in press. [Google Scholar] [CrossRef]
- Calaway, K.; Coshal, S.; Jones, K.; Coverdale, J.; Livingston, R. A systematic review of the safety of electroconvulsive therapy use during the first trimester of pregnancy. J. ECT 2016, 32, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Elias, A.; Thomas, N.; Sackeim, H.A. Electroconvulsive therapy in mania: A review of 80 years of clinical experience. Am. J. Psychiatry 2021, 178, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Lv, Q.; Hu, Q.; Zhang, W.; Huang, X.; Zhu, M.; Geng, R.; Cheng, X.; Bao, C.; Wang, Y.; Zhang, C.; et al. Disturbance of oxidative stress parameters in treatment-resistant bipolar disorder and their association with electroconvulsive therapy response. Int. J. Neuropsychopharmacol. 2020, 23, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Minelli, A.; Congiu, C.; Ventriglia, M.; Bortolomasi, M.; Bonvicini, C.; Abate, M.; Sartori, R.; Gainelli, G.; Gennarelli, M. Influence of GRIK4 genetic variants on the electroconvulsive therapy response. Neurosci. Lett. 2016, 626, 94–98. [Google Scholar] [CrossRef]
- Wright, B.M.; Eiland, E.H.; Lorenz, R. Augmentation with atypical antipsychotics for depression: A review of evidence-based support from the medical literature. Pharmacotherapy 2013, 33, 344–359. [Google Scholar] [CrossRef]
- Nakajima, S.; Takeuchi, H.; Fervaha, G.; Plitman, E.; Chung, J.K.; Caravaggio, F.; Iwata, Y.; Mihashi, Y.; Gerretsen, P.; Remington, G.; et al. Comparative efficacy between clozapine and other atypical antipsychotics on depressive symptoms in patients with schizophrenia: Analysis of the CATIE phase 2E data. Schizophr. Res. 2015, 161, 429–433. [Google Scholar] [CrossRef] [Green Version]
- Morais, M.; Patrício, P.; Mateus-Pinheiro, A.; Alves, N.D.; Machado-Santos, A.R.; Correia, J.S.; Pereira, J.; Pinto, L.; Sousa, N.; Bessa, J.M. The modulation of adult neuroplasticity is involved in the mood-improving actions of atypical antipsychotics in an animal model of depression. Transl. Psychiatry 2017, 7, e1146. [Google Scholar] [CrossRef] [Green Version]
- Balu, D.T.; Hoshaw, B.A.; Malberg, J.E.; Rosenzweig-Lipson, S.; Schechter, L.E.; Lucki, I. Differential regulation of central BDNF protein levels by antidepressant and non-antidepressant drug treatments. Brain Res. 2008, 1211, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Yrondi, A.; Sporer, M.; Péran, P.; Schmitt, L.; Arbus, C.; Sauvaget, A. Electroconvulsive therapy, depression, the immune system and inflammation: A systematic review. Brain Stimul. 2018, 11, 29–51. [Google Scholar] [CrossRef]
- Cretaz, E.; Brunoni, A.R.; Lafer, B. Magnetic seizure therapy for unipolar and bipolar depression: A systematic review. Neural Plast. 2015, 2015, 521398. [Google Scholar] [CrossRef] [Green Version]
- Geduldig, E.; Kellner, C. Electroconvulsive therapy in the elderly: New findings in geriatric depression. Curr. Psychiatry Rep. 2016, 18, 40. [Google Scholar] [CrossRef]
- Dominiak, M.; Antosik-Wójcińska, A.Z.; Goetz, Z.; Sikorska, O.; Stefanowski, B.; Gorostiza, D.; Święcicki, Ł. Efficacy, safety and tolerability of formula-based unilateral vs bilateral electroconvulsive therapy in the treatment of major depression: A randomized open label controlled trial. J. Psychiatr. Res. 2021, 133, 52–59. [Google Scholar] [CrossRef]
- Farzan, F.; Boutros, N.N.; Blumberger, D.M.; Daskalakis, Z.J. What does the electroencephalogram tell us about the mechanisms of action of ECT in major depressive disorders? J. ECT 2014, 30, 98–106. [Google Scholar] [CrossRef]
- Takamiya, A.; Kishimoto, T.; Hirano, J.; Nishikata, S.; Sawada, K.; Kurokawa, S.; Yamagata, B.; Kikuchi, T.; Mimura, M. Neuronal network mechanisms associated with depressive symptom improvement following electroconvulsive therapy. Psychol. Med. 2020, 1–8. [Google Scholar] [CrossRef]
- Jonckheere, J.; Deloulme, J.-C.; Dall’Igna, G.; Chauliac, N.; Pelluet, A.; Nguon, A.-S.; Lentini, C.; Brocard, J.; Denarier, E.; Brugière, S.; et al. Short- and long-term efficacy of electroconvulsive stimulation in animal models of depression: The essential role of neuronal survival. Brain Stimul. 2018, 11, 1336–1347. [Google Scholar] [CrossRef] [Green Version]
- Chen, F.; Danladi, J.; Wegener, G.; Madsen, T.M.; Nyengaard, J.R. Sustained ultrastructural changes in rat hippocampal formation after repeated electroconvulsive seizures. Int. J. Neuropsychopharmacol. 2020, 23, 446–458. [Google Scholar] [CrossRef] [Green Version]
- Chen, F.; Ardalan, M.; Elfving, B.; Wegener, G.; Madsen, T.M.; Nyengaard, J.R. Mitochondria are critical for BDNF-mediated synaptic and vascular plasticity of hippocampus following repeated electroconvulsive seizures. Int. J. Neuropsychopharmacol. 2018, 21, 291–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camilleri, J.A.; Hoffstaedter, F.; Zavorotny, M.; Zöllner, R.; Wolf, R.C.; Thomann, P.; Redlich, R.; Opel, N.; Dannlowski, U.; Grözinger, M.; et al. Electroconvulsive therapy modulates grey matter increase in a hub of an affect processing network. Neuroimage Clin. 2020, 25, 102114. [Google Scholar] [CrossRef] [PubMed]
- Masuoka, T.; Tateno, A.; Sakayori, T.; Tiger, M.; Kim, W.; Moriya, H.; Ueda, S.; Arakawa, R.; Okubo, Y. Electroconvulsive therapy decreases striatal dopamine transporter binding in patients with depression: A positron emission tomography study with [18F] FE-PE2I. Psychiatry Res. Neuroimaging 2020, 301, 111086. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Kar, S.K. How electroconvulsive therapy works: Understanding the neurobiological mechanisms. Clin. Psychopharmacol. Neurosci. 2017, 15, 210–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilby, K.J.; Johnson, E.G.; Johnson, H.E.; Ensom, M.H.H. Evidence-based review of pharmacotherapy used for Parkinson’s disease psychosis. Ann. Pharmacother. 2017, 51, 682–695. [Google Scholar] [CrossRef] [PubMed]
- Combs, B.L.; Cox, A.G. Update on the treatment of Parkinson’s disease psychosis: Role of pimavanserin. Neuropsychiatr. Dis. Treat. 2017, 13, 737–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyle, K.; Bronstein, J.M. Treatment of psychosis in Parkinson’s disease and dementia with Lewy Bodies: A review. Parkinsonism Relat. Disord. 2020, 75, 55–62. [Google Scholar] [CrossRef]
- Parkinson Study Group. Low-dose clozapine for the treatment of drug-induced psychosis in Parkinson’s disease. N. Engl. J. Med. 1999, 340, 757–763. [Google Scholar] [CrossRef]
- Pollak, P.; Tison, F.; Rascol, O.; Destée, A.; Péré, J.J.; Senard, J.M.; Durif, F.; Bourdeix, I. Clozapine in drug induced psychosis in Parkinson’s disease: A randomised, placebo controlled study with open follow up. J. Neurol. Neurosurg. Psychiatry 2004, 75, 689–695. [Google Scholar] [CrossRef] [Green Version]
- Fox, S.H. Non-dopaminergic treatments for motor control in Parkinson’s disease. Drugs 2013, 73, 1405–1415. [Google Scholar] [CrossRef]
- Thomas, A.A.; Friedman, J.H. Current use of clozapine in Parkinson disease and related disorders. Clin. Neuropharmacol. 2010, 33, 14–16. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, L.; Fan, Y.; Yang, L.; Wen, X.; Liu, Y.; Liu, Z. Atypical antipsychotics for Parkinson’s disease psychosis: A systematic review and meta-analysis. Neuropsychiatr. Dis. Treat. 2019, 15, 2137–2149. [Google Scholar] [CrossRef]
- Schaeffer, E.; Pilotto, A.; Berg, D. Pharmacological strategies for the management of levodopa-induced dyskinesia in patients with Parkinson’s disease. CNS Drugs 2014, 28, 1155–1184. [Google Scholar] [CrossRef]
- Narang, P.; Glowacki, A.; Lippmann, S. Electroconvulsive therapy intervention for Parkinson’s disease. Innov. Clin. Neurosci. 2015, 12, 25–28. [Google Scholar]
- Rosenquist, P.B.; Youssef, N.A.; Surya, S.; McCall, W.V. When all else fails: The use of electroconvulsive therapy for conditions other than major depressive episode. Psychiatr. Clin. N. Am. 2018, 41, 355–371. [Google Scholar] [CrossRef]
- Connolly, B.S.; Lang, A.E. Pharmacological treatment of Parkinson disease: A review. JAMA 2014, 311, 1670–1683. [Google Scholar] [CrossRef]
- Takamiya, A.; Seki, M.; Kudo, S.; Yoshizaki, T.; Nakahara, J.; Mimura, M.; Kishimoto, T. Electroconvulsive therapy for Parkinson’s disease; A systematic review and meta-analysis. Mov. Disord. 2021, 36, 51–58. [Google Scholar] [CrossRef]
- Calderón-Fajardo, H.; Cervantes-Arriaga, A.; Llorens-Arenas, R.; Ramírez-Bermudez, J.; Ruiz-Chow, Á.; Rodríguez-Violante, M. Electroconvulsive therapy in Parkinson’s disease. Arq. Neuro-Psiquiatr. 2015, 73, 856–860. [Google Scholar] [CrossRef] [Green Version]
- Murayama, T.; Kobayashi, S.; Matsuoka, T.; Kigawa, Y.; Ishida, T.; Hyakumachi, K.; Utsumi, K.; Kawanishi, C. Effectiveness of electroconvulsive therapy in patients with advanced Parkinson disease. J. ECT 2021, 37, 88–93. [Google Scholar] [CrossRef]
- Ramesh, V.; Sharma, A.; Sharma, V.; Somani, A. Treatment of catatonia in Parkinson’s disease with electroconvulsive therapy. Ann. Indian Acad. Neurol. 2019, 22, 501–503. [Google Scholar]
- Volkaerts, L.; Roels, R.; Bouckaert, F. Motor function improvement after electroconvulsive therapy in a Parkinson’s disease patient with deep brain stimulator. J. ECT 2020, 36, 66–68. [Google Scholar] [CrossRef]
- Borisovskaya, A.; Bryson, W.C.; Buchholz, J.; Samii, A.; Borson, S. Electroconvulsive therapy for depression in Parkinson’s disease: Systematic review of evidence and recommendations. Neurodegener. Dis. Manag. 2016, 6, 161–176. [Google Scholar] [CrossRef]
- Cumper, S.K.; Ahle, G.M.; Liebman, L.S.; Kellner, C.H. Electroconvulsive therapy (ECT) in Parkinson’s disease: ECS and dopamine enhancement. J. ECT 2014, 30, 122–124. [Google Scholar] [CrossRef]
- Strome, E.M.; Zis, A.P.; Doudet, D.J. Electroconvulsive shock enhances striatal dopamine D1 and D3 receptor binding and improves motor performance in 6-OHDA-lesioned rats. J. Psychiatry Neurosci. 2007, 32, 193–202. [Google Scholar] [PubMed]
- Enomoto, S.; Shimizu, K.; Nibuya, M.; Toda, H.; Yoshino, A.; Suzuki, E.; Kondo, T.; Fukuda, H. Expression of endocytosis-related proteins in rat hippocampus following 10-day electroconvulsive seizure treatment. Neurosci. Lett. 2016, 624, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Al-Amin, M.M.; Udin, M.M.N.; Reza, H.M. Effects of antipsychotics on the inflammatory response system of patients with schizophrenia in peripheral blood mononuclear cell cultures. Clin. Psychopharmacol. Neurosci. 2013, 11, 144–151. [Google Scholar] [CrossRef]
- Hirsch, E.C.; Hunot, S.; Damier, P.; Faucheux, B. Glial cells and inflammation in parkinson’s disease: A role in neurodegeneration? Ann. Neurol. 1998, 44 (Suppl. 1), S115–S120. [Google Scholar] [CrossRef] [PubMed]
- Trépanier, M.O.; Hopperton, K.E.; Mizrahi, R.; Mechawar, N.; Bazinet, R.P. Postmortem evidence of cerebral inflammation in schizophrenia: A systematic review. Mol. Psychiatry 2016, 21, 1009–1026. [Google Scholar] [CrossRef]
- Haroon, E.; Miller, A.H.; Sanacora, G. Inflammation, glutamate, and glia: A trio of trouble in mood disorders. Neuropsychopharmacology 2017, 42, 193–215. [Google Scholar] [CrossRef] [PubMed]
- Lecours, C.; Bordeleau, M.; Cantin, L.; Parent, M.; Paolo, T.D.; Tremblay, M.-È. Microglial implication in Parkinson’s disease: Loss of beneficial physiological roles or gain of inflammatory functions? Front. Cell. Neurosci. 2018, 12, 282. [Google Scholar] [CrossRef]
- Lesh, T.A.; Careaga, M.; Rose, D.R.; McAllister, A.K.; Van de Water, J.; Carter, C.S.; Ashwood, P. Cytokine alterations in first-episode schizophrenia and bipolar disorder: Relationships to brain structure and symptoms. J. Inflamm. 2018, 15, 165. [Google Scholar] [CrossRef] [Green Version]
- Almeida, P.G.C.; Nani, J.V.; Oses, J.P.; Brietzke, E.; Hayashi, M.A.F. Neuroinflammation and glial cell activation in mental disorders. Brain Behav. Immun. Health. 2020, 2, 100034. [Google Scholar] [CrossRef]
- Kam, T.-I.; Hinkle, J.T.; Dawson, T.M.; Dawson, V.L. Microglia and astrocyte dysfunction in parkinson’s disease. Neurobiol. Dis. 2020, 144, 105028. [Google Scholar] [CrossRef]
- Bernstein, H.-G.; Steiner, J.; Bogerts, B. Glial cells in schizophrenia: Pathophysiological significance and possible consequences for therapy. Expert Rev. Neurother. 2009, 9, 1059–1071. [Google Scholar] [CrossRef]
- Monji, A.; Kato, T.; Kanba, S. Cytokines and schizophrenia: Microglia hypothesis of schizophrenia. Psychiatry Clin. Neurosci. 2009, 63, 257–265. [Google Scholar] [CrossRef]
- Zakharyan, R.; Boyajyan, A. Inflammatory cytokine network in schizophrenia. World J. Biol. Psychiatry 2013, 15, 174–187. [Google Scholar] [CrossRef]
- Watkins, C.C.; Sawa, A.; Pomper, M.G. Glia anda immune cell signaling in bipolar disorder: Insights from neuropharmacology and molecular imaging to clinical application. Transl. Psychiatry 2014, 4, e350. [Google Scholar] [CrossRef] [Green Version]
- Himmerich, H.; Patsalos, O.; Lichtblau, N.; Ibrahim, M.A.A.; Dalton, B. Cytokine research in depression: Principles, challenges, and open questions. Front. Psychiatry 2019, 10, 30. [Google Scholar] [CrossRef] [Green Version]
- Momtazmanesh, S.; Zare-Shahabadi, A.; Rezaei, N. Cytokine alterations in schizophrenia: An updated review. Front. Psychiatry 2019, 10, 892. [Google Scholar] [CrossRef] [Green Version]
- Stone, T.W.; Forrest, C.M.; Darlington, L.G. Kynurenine pathway inhibition as a therapeutic strategy for neuroprotection. FEBS J. 2012, 279, 1386–1397. [Google Scholar] [CrossRef]
- Limoa, E.; Hashioka, S.; Miyaoka, T.; Tsuchie, K.; Arauchi, R.; Azis, I.A.; Wake, R.; Hayashida, M.; Araki, T.; Furuya, M.; et al. Electroconvulsive shock attenuated microgliosis and astrogliosis in the hippocampus and ameliorated schizophrenia-like behavior of Gunn rat. J. Neuroinflamm. 2016, 13, 230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarasov, V.V.; Svistunov, A.A.; Chubarev, V.N.; Sologova, S.S.; Mukhortova, P.; Levushkin, D.; Somasundaram, S.G.; Kirkland, C.E.; Bachurin, S.O.; Aliev, G. Alterations of astrocytes in the context of schizophrenic dementia. Front. Pharmacol. 2020, 10, 1612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roge, R.; Moller, B.K.; Andersen, C.R.; Correll, C.U.; Nielsen, J. Immunomodulatory effects of clozapine and their clinical implications: What have we learned so far? Schizophr. Res. 2012, 140, 204–213. [Google Scholar] [CrossRef]
- Giridharan, V.V.; Scaini, G.; Colpo, G.D.; Doifode, T.; Pinjari, O.F.; Teixeira, A.L.; Petronilho, F.; Macêdo, D.; Quevedo, J.; Barichello, T. Clozapine prevents poly (I:C) induced inflammation by modulating NLRP3 pathway in microglial cells. Cells 2020, 9, 577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robichon, K.; Patel, V.; Connor, B.; La Flamme, A.C. Clozapine reduces infiltration into the CNS by targeting migration in experimental autoimmune encephalomyelitis. J. Neuroinflamm. 2020, 17, 53. [Google Scholar] [CrossRef] [PubMed]
- Ceylan, U.; Haupeltshofer, S.; Kämper, L.; Dann, J.; Ambrosius, B.; Gold, R.; Faissner, S. Clozapine regulates microglia and is effective in chronic experimental autoimmune encephalomyelitis. Front. Immunol. 2021, 12, 656941. [Google Scholar] [CrossRef]
- Drzyzga, L.; Obuchowicz, E.; Marcinowska, A.; Herman, Z.S. Cytokines in schizophrenia and the effects of antipsychotic drugs. Brain Behav. Immun. 2006, 20, 532–545. [Google Scholar] [CrossRef] [PubMed]
- Rotter, A.; Biermann, T.; Stark, C.; Decker, A.; Demling, J.; Zimmermann, R.; Sperling, W.; Kornhuber, J.; Henkel, A. Changes of cytokine profiles during electroconvulsive therapy in patients with major depression. J. ECT 2013, 29, 162–169. [Google Scholar] [CrossRef]
- Friere, T.F.V.; da Rocha, N.S.; de Almeida Fleck, M. The association of electroconvulsive therapy to pharmacological treatment and its influence on cytokines. J. Psychiatr. Res. 2017, 92, 205–211. [Google Scholar] [CrossRef]
- Goldfarb, S.; Fainstein, N.; Ben-Hur, T. Electroconvulsive stimulation attenuates chronic neuroinflammation. JCI Insight 2020, 5, e137028. [Google Scholar] [CrossRef]
- Kranaster, L.; Hoyer, C.; Aksay, S.S.; Bumb, J.M.; Müller, N.; Zill, P.; Schwarz, M.J.; Sartorius, A. Antidepressant efficacy of electroconvulsive therapy is associated with a reduction of the innate cellular immune activity in the cerebrospinal fluid in patiens with depression. World J. Biol. Psychiatry 2018, 19, 379–389. [Google Scholar] [CrossRef]
- Guloksuz, S.; Rutten, B.P.F.; Arts, B.; van Os, J.; Kenis, G. The immune system and electroconvulsive therapy for depression. J. ECT 2014, 30, 132–137. [Google Scholar] [CrossRef]
- Van Buel, E.M.; Patas, K.; Peters, M.; Bosker, F.J.; Eisel, U.L.M.; Klein, H.C. Immune and neurotrophin stimulation by electroconvulsive therapy: Is some inflammation needed after all? Transl. Psychiatry 2015, 5, e609. [Google Scholar] [CrossRef]
- Lander, M.; Bastiampillai, T.; Sareen, J. Review of withdrawal catatonia: What does this reveal about clozapine? Transl. Psychiatry 2018, 8, 139. [Google Scholar] [CrossRef] [Green Version]
- Luchini, F.; Medda, P.; Mariani, M.G.; Mauri, M.; Toni, C.; Perugi, G. Electroconvulsive therapy in catatonic patients: Efficacy and predictors of response. World J. Psychiatry 2015, 5, 182–192. [Google Scholar] [CrossRef]
- Dursun, S.M.; Hallak, J.E.C.; Haddad, P.; Leahy, A.; Byrne, A.; Strickland, P.L.; Anderson, I.M.; Zuardi, A.W.; Deakin, J.F.W. Clozapine monotherapy for catatonic schizophrenia: Should clozapine be the treatment of choice, with catatonia rather than psychosis as the main therapeutic index? J. Psychopharmacol. 2005, 19, 432–433. [Google Scholar] [CrossRef]
- Ene-Stroescu, V.; Nguyen, T.; Waiblinger, B. Successful treatment of catatonia in a young man with schizophrenia and progressive diffuse cerebral atrophy. J. Neuropsychiatry Clin. Neurosci. 2014, 26, E21–E22. [Google Scholar] [CrossRef]
- Rommel, O.; Tegenthoff, M.; Widdig, W.; Bräunig, P.; Malin, J.P. Organic catatonia following frontal lobe injury: Response to clozapine. J. Neuropsychiatry Clin. Neurosci. 1998, 10, 237–238. [Google Scholar] [CrossRef]
- Oldham, M.A.; Desan, P.H. Alcohol and sedative-hypnotic withdrawal catatonia: Two case reports, systematic literature review, and suggestion of a potential relationship with alcohol withdrawal delirium. Psychosomatics 2016, 57, 246–255. [Google Scholar] [CrossRef]
- Bastiampillai, T.; Forooziya, F.; Dhillon, R. Clozapine-withdrawal catatonia. Aust. N. Z. J. Psychiatry 2009, 43, 283–284. [Google Scholar]
- Bilbily, J.; McCollum, B.; de Leon, J. Catatonia secondary to sudden clozapine: A case with three repeated episodes and a literature review. Case Rep. Psychiatry 2017, 2017, 2402731. [Google Scholar] [CrossRef] [Green Version]
- Ellul, P.; Choucha, W. Neurobiological approach of catatonia and treatment perspectives. Front. Psychiatry 2015, 6, 182. [Google Scholar] [CrossRef] [Green Version]
- Guidotti, A.; Dong, E.; Grayson, D.R. Epigenetic basis of clozapine action. J. Drug Des. Res. 2017, 4, 1055. [Google Scholar]
- De Jong, J.O.Z.; Arts, B.; Boks, M.P.; Sienaert, P.; van den Hove, D.L.A.; Kenis, G.; van Os, J.; Rutten, B.P.F. Epigenetic effects of electroconvulsive seizures. J. ECT 2014, 30, 152–159. [Google Scholar] [CrossRef] [PubMed]
- MacKay, M.-A.B.; Paylor, J.W.; Wong, J.T.F.; Winship, I.R.; Baker, G.B.; Dursun, S.M. Multidimensional connectomics and treatment-resistant schizophrenia: Linking phenotypic circuits to targeted therapeutics. Front. Psychiatry 2018, 9, 637. [Google Scholar] [CrossRef]
- Zeng, J.; Luo, Q.; Du, L.; Liao, W.; Li, Y.; Liu, H.; Liu, D.; Fu, Y.; Qiu, H.; Li, X.; et al. Reorganization of anatomical connectome following electroconvulsive therapy in major depressive disorder. Neural Plasticity 2015, 2015, 271674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrican, R.; Söderlund, H.; Kumar, N.; Daskalakis, Z.J.; Flint, A.; Levine, B. Electroconvulsive therapy “corrects” the neural architecture of visuospatial memory: Implications for typical cognitive-affective functioning. NeuroImage Clin. 2019, 23, 101816. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Area of Interest | Comments |
|---|---|
| Schizophrenia | Clozapine is the gold standard for therapy of treatment-resistant schizophrenia despite causing a plethora of side effects. ECT is being used increasingly in schizophrenia as a promising augmentation strategy with clozapine in clozapine-resistant schizophrenia. |
| Bipolar Disorder | Although data are limited, current evidence suggests that clozapine is effective and relatively safe to use in treatment-resistant bipolar disorder. ECT is considered a second-line option in refractory mania and a first-line option in severe I disorder, psychotic depression, and suicide risk. |
| Major Depressive Disorder (MDD) | Clozapine is not normally used as a primary treatment for MDD, but a large study [19] found a reduced risk of hospital readmission in patients with MDD taking clozapine; clozapine was reported to be more effective than quetiapine in treating depressive symptoms in those patients. ECT is a very effective treatment for MDD and is considered safe and well tolerated. |
| Parkinson’s Disease (PD) | Clozapine is effective in treating psychosis in PD but has also been reported to improve symptoms of tremor and dyskinesias.ECT has been found to reduce motor symptoms and to be effective in treating comorbid depression. |
| Catatonia | Catatonia can be associated with a wide variety of neuropsychiatric disorders and some drug-induced conditions. Benzodiazepines are the first-line treatment, but ECT is also an established effective treatment. Clozapine is not used extensively but appears to be unique among antipsychotics in that it improves the symptoms of catatonia rather than causing or worsening them. |
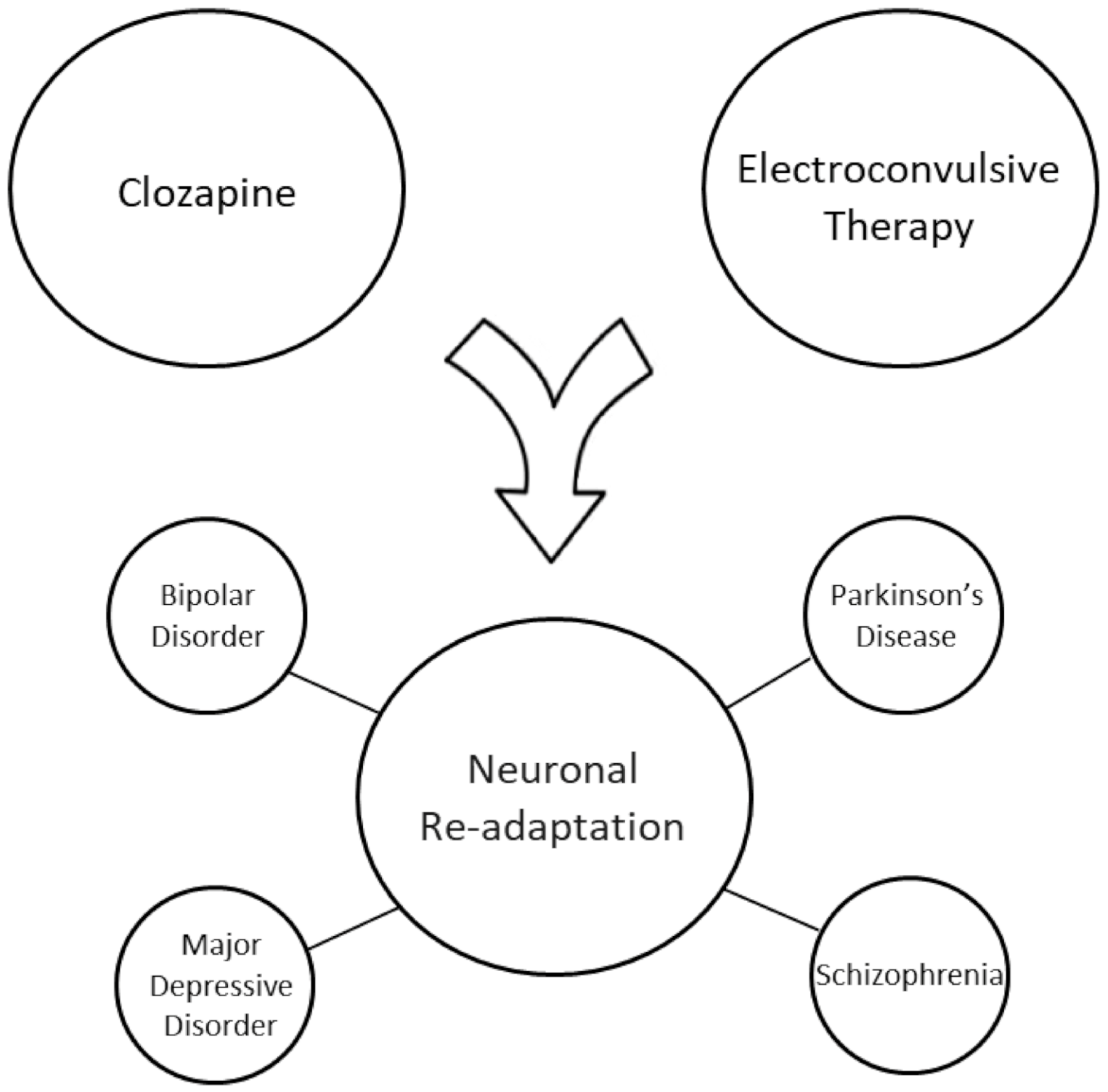
| Mechanisms of action | Although the mechanisms of action of clozapine and ECT are complex and still not clearly understood, a review of the literature on these two treatments suggests that the following may be common underlying mechanisms and may explain why both treatments are effective in a wide range of neuropsychiatric disorders: elicit epileptiform activity and alter EEG activity, increase neuroplasticity and cause an elevation of levels of neurotrophic factors, alter imbalances between GABAergic and glutamatergic systems, and reduce inflammation by acting on glia and cytokines. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gammon, D.; Cheng, C.; Volkovinskaia, A.; Baker, G.B.; Dursun, S.M. Clozapine: Why Is It So Uniquely Effective in the Treatment of a Range of Neuropsychiatric Disorders? Biomolecules 2021, 11, 1030. https://doi.org/10.3390/biom11071030
Gammon D, Cheng C, Volkovinskaia A, Baker GB, Dursun SM. Clozapine: Why Is It So Uniquely Effective in the Treatment of a Range of Neuropsychiatric Disorders? Biomolecules. 2021; 11(7):1030. https://doi.org/10.3390/biom11071030
Chicago/Turabian StyleGammon, Dara, Catherine Cheng, Anna Volkovinskaia, Glen B. Baker, and Serdar M. Dursun. 2021. "Clozapine: Why Is It So Uniquely Effective in the Treatment of a Range of Neuropsychiatric Disorders?" Biomolecules 11, no. 7: 1030. https://doi.org/10.3390/biom11071030