4. Discussion
Nephrolithiasis is a high-prevalence disease that results in significant medical expenditures. An increase in the prevalence and incidence of kidney stones has been demonstrated mainly in industrialized countries, whose causes remain unclear [
1,
2]. Environmental factors such as dietary changes have been historically pointed out as possible causes of these trends. Moreover, high fructose consumption, animal protein intake, and oxalate or sodium consumption have been identified as risk factors for kidney stone formation [
20,
21].
Nephrolithiasis affects 5–9% of the population in Europe and 13% of North Americans. The overall probability of becoming a stone former varies across the different parts of the world. Stones are slightly more frequent in males than in females and in white Caucasians than in blacks. Kidney stones in the upper urinary tract appear to be related to lifestyle factors, being more frequent in people living in developed countries in which high animal protein consumption or high-fructose diets are more frequent. However, bladder stones are mainly seen in third-world countries and are associated with infections and poor living conditions [
22].
In Spain, no official data have been published regarding the epidemiology of urolithiasis, although a recent review of previous Spanish reports has estimated an incidence of 737 cases per 100,000 inhabitants/year and a prevalence of 5066 cases per 100,000 inhabitants [
23]. A study on persons aged 40 to 65 using personal telephone surveys shows how, in Spain, renal lithiasis is associated with older age, belonging to higher socioeconomic classes, the existence of family history of urolithiasis, and hypertension, obesity, or overweight [
17].
The most important data regarding the hospitality burden of urolithiasis have been developed in the USA in which the rate of hospitalization for upper urinary stones in the year 2000 was 62 cases per 100,000 inhabitants. This rate has decreased by 15% since 1994, although hospital outpatient visits increased by 40% for this cause in the same period of time [
24]. In Spain, no data about the rates of hospitalization have been reported until now. Our study has estimated 56.7 patients hospitalized per 100,000 inhabitants. Although the periods of study are different, the rates seem to be comparable.
In France, another study with similar methods has been published, reporting data from 2006 to 2009, although no results were extrapolated to the general population [
25]. Nevertheless, the data of the paper can be extrapolated using France’s 2009 general population (64,658,856 inhabitants) from the World Bank (datatopics.worldbank.org, accesed on 17 April 2023). The hospitality burden of lithiasic patients coded with a primary diagnosis would be about 22.3 patients per 100,000 inhabitants, moderately lower than ours, although the periods of time are different.
The admissions rate was the highest in the oldest males both in the USA and Spain (no data was reported in France about gender and age). In Spain, the highest rates of hospitalization correspond to the age range between 50 and 80 years old. In the same way, in patients older than 65 years old, admission rates have been consistently higher than in younger people in the USA. The ratio of male to female has been lower in Spain than in the USA, where it has decreased from 1.86 in 1994 to 1.45 in 2000. However, it would be interesting to know if that decreasing trend was consistent over time in order to know if both ratios were comparable [
24].
The mean length of stay is significantly lower in the USA (2.4 days) than in Spain (5.23 days). However, the same trend is consistently observed in both countries in which the length of stay lowers over the years. In the same way, both studies showed an increase in the length of stay as age increases, except for the pediatric population in which it was higher. In Germany, a hospital length of 3.6 days on average has been reported for urolithiasis patients through the German Federal Statistical Office (2020) [
26]. Shulz et al., in an analysis based on health insurance claims data, estimated a 6.8 day average length of stay for inpatients with urolithiasis cases [
27]. Nevertheless, these data can be inaccurate because, in every center, some therapies can be administered under different circumstances. For example, SWL or ureteroscopy, which are therapies frequently used for kidney or ureteral stones, can be provided in an outpatient or an inpatient hospital setting, depending on hospital resources or physician preferences.
In the USA, an estimated effect on per capita costs of patients with urolithiasis of USD 4472 per year has been reported, being the highest in 45- to 54-year-old patients [
24]. An average cost of USD 26,103 for inpatient cases from 2006 to 2009 has also been estimated [
28]. In this study, an average cost of EUR 3026 was found. In Spain, most of the patients are treated in the public Spanish health system where costs are reduced.
According to demographic statistics, the proportion of people aged over 65 years or older will rise in the coming years [
29]. Because of this, a rise in lithiasic pathology in geriatric patients is expected. In our study, it has been shown how older patients present with more complicated causes of hospitalizations associated with urolithiasis, being more sensitive to present infectious complications. Mortality in geriatric patients is also higher than in younger patients, reaching up to 13% in patients over 89 years old. Arampatzis et al. analyzed current diagnostic and treatment patterns of geriatric urolithiasis patients in emergency departments. It has also been shown how elderly patients have a higher risk of complications and a twofold increased likelihood of being hospitalized [
29].
Moreover, it has been reported how mortality increases with age in lithiasic patients [
30] and how therapies widely used for the treatment of lithiasis, such as ureteroscopy, almost double mortality in elderly people [
31]. In our study, urinary tract infections have been shown to be the most frequent diagnosis coded in elderly patients. It has been widely remarked that urinary tract infections are a strong predictor of mortality and complications for stone surgery [
31]. Other factors related to a poor clinical outcome in critical illness, such as vitamin D deficiency, are frequently found in lithiasic patients [
32]. Therefore, our findings suggest a higher mortality in elderly patients influenced by a higher prevalence of urinary tract infections.
Furthermore, other comorbidity diseases have been pointed out as predictors of mortality in treated lithiasis patients, such as gender, body mass index, diabetes, cardiovascular diseases, and vitamin deficiency [
29,
31,
32]. In this paper, age, diabetes mellitus, and hypertension have been shown to be mortality predictors both in univariate and multivariate analyses.
Metabolic syndrome is a constellation of disorders, which includes obesity, hypertension, diabetes, and hyperlipidemia [
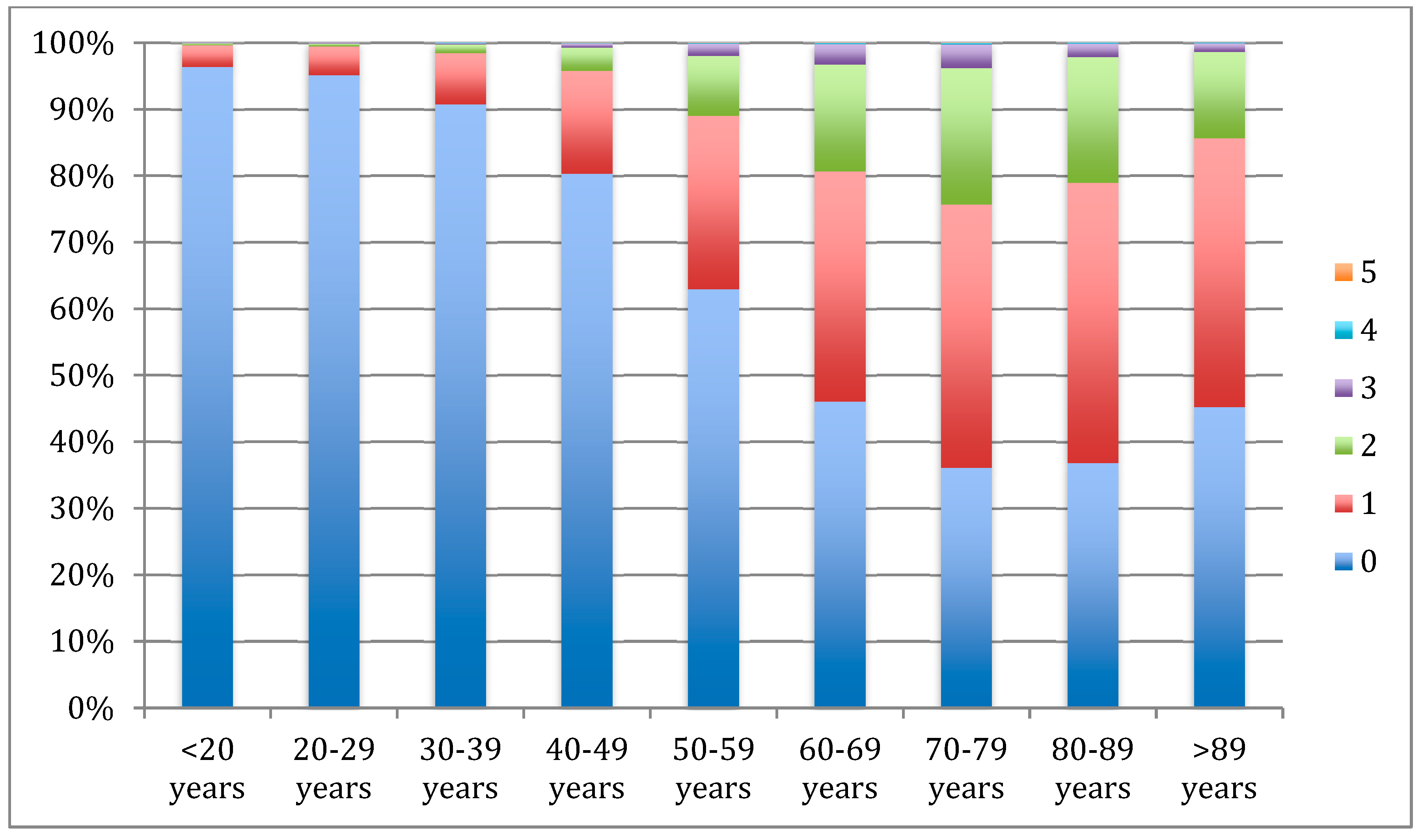
6,
9]. In our study, we have shown how metabolic syndrome components become more prevalent as age increases, with hypertension (29.3%) and diabetes (16.4%) being the most frequently coded in lithiasic patients. Epidemiological studies have reported a higher incidence of urolithiasis in diabetic patients with a RR between 1.31 and 1.67 [
33]. Furthermore, kidney stone formers exhibit a higher diabetes mellitus incidence than non-stone formers [
34].
Hyperglycemia has been related to alterations in renal handling of urinary ions [
35] and to increased oxidative stress inducing cellular changes, apoptosis and necrosis, and cellular death, which will develop a stone nidus and a precursor of a kidney stone [
36,
37].
Concerning cardiovascular morbidities, lithiasic patients develop hypertension with an OR between 1.24 and 1.96, and, conversely, hypertensive patients show a higher risk of developing kidney stones [
38,
39]. Enhanced generation of endothelial reactive oxygen species in kidney vessels has a key role in the development of endothelial dysfunction associated with low-grade inflammation morbidities such as urolithiasis [
40].
The present study has strengths and limitations. The main strengths are the use of the MBDS records which offer practically all hospital admission records from both public and private hospitals, thus increasing the power analysis even of low-prevalence diseases. However, the quality of the MBDS depends on the quality of the discharge report and on the codification process variables. The results obtained in this study provide an accurate assessment of the changes in the national incidence of hospitalizations due to urolithiasis over four years and allow us to estimate the real burden of hospitalization for urolithiasis. The mortality rate by age group provided in this study is useful to know which groups are more likely to develop complications and which risk factors are associated with them. Nevertheless, mortality rate estimations should be interpreted with caution as deaths could occur outside of the hospital environment.
The direct costs to the national health system or private insurance companies, calculated by the MDBS, were calculated using diagnosis-related groups (DRGs) for this disease. Although DRGs have been widely used as a patient classification system for hospital cost analysis, they present the limitation of including an internal variability in comorbid conditions and a lack of sensitivity to different medical practices used in similar diseases.

 ,
, 


{kind=link}
{kind=link}