
Effects of Hypolipidemic Drugs on Psoriasis

 , and
, and
Abstract
:1. Introduction
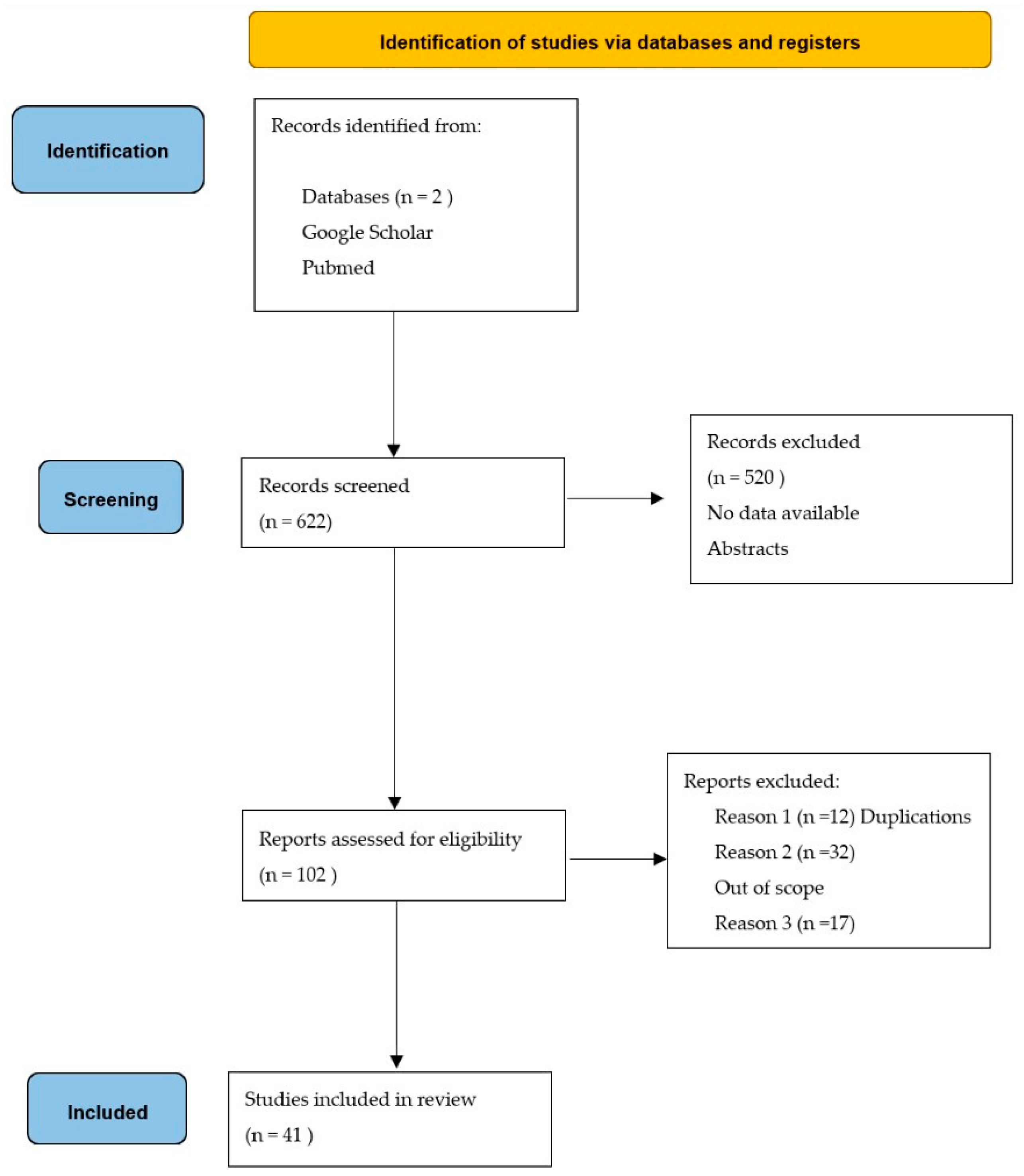
2. Materials and Methods
3. Results and Discussion
3.1. Statins’ Influence on Psoriasis
3.1.1. Statins’ Influence on Psoriasis with Therapeutic Effect
3.1.2. Lack of Statins’ Therapeutic Effect on Psoriasis
3.1.3. Statins’ Deteriorating Influence on Psoriasis
3.2. Fibrates’ Influence on Psoriasis with Therapeutic Effects
Fibrates’ Deteriorating Influence on Psoriasis
3.3. Glitazones’ Influence on Psoriasis
3.3.1. Pioglitazone’s Influence on Psoriasis with Therapeutic Effects
3.3.2. Pioglitazone’s Influence on Psoriasis along with Typical Anti-Psoriatic Treatments
3.3.3. Pioglitazone’s Influence on Psoriasis without Significant Therapeutic Effects
3.3.4. Rosiglitazone’s Influence on Psoriasis
3.4. GLP-1 Analogs’ Influence on Psoriasis
3.4.1. Liraglutide’s (a GLP-1 Analog) Influence on Psoriasis with Therapeutic Effects
3.4.2. Liraglutide’s Lack of Influence on Psoriasis
3.4.3. Exenatide’s Influence on Psoriasis
3.4.4. Liraglutide’s and Exenatide’s Influence on Psoriasis
3.4.5. Liraglutide’s Influence on Psoriasis along with Typical Anti-Psoriatic Treatments
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Trong, H.N.; Tat, T.N.; Anh, T.T.N.; Uyen, N.P.; Van, T.N.; Hau, K.T.; Gandolfi, M.; Satolli, F.; Feliciani, C.; Tirant, M.; et al. Efficacy of Adding Oral Simvastatin to Topical Therapy for Treatment of Psoriasis. Open Access Maced. J. Med. Sci. 2019, 7, 237–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imamura, T.; Takata, I.; Ogasawara, M.; Matsutani, Y.; Yamamoto, T.; Asagami, C. Clofibrate treatment of psoriasis with hypertriglycemia-clinical, histological and laboratory analysis. Nihon Hifuka Gakkai Zasshi 1991, 101, 623–628. [Google Scholar]
- Singh, S.; Bhansali, A. Randomized placebo control study of insulin sensitizers (Metformin and Pioglitazone) in psoriasis patients with metabolic syndrome (Topical Treatment Cohort). BMC Dermatol. 2016, 16, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.; Lin, L.; Chen, P.; Yu, Y.; Chen, S.; Chen, X.; Shao, Z. Treatment with liraglutide, a glucagon-like peptide-1 analogue, imporves effectively the skin lesions of psoriasis patients with type 2 diabetes: A prospective cohort study. Diabetes Res. Clin. Pract. 2019, 150, 167–173. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Garschick, M.S.; Drenkova, K.; Barrett, T.J.; Schlamp, F.; Fisher, E.A.; Katz, S.; Jelic, S.; Neimann, A.L.; Scher, J.U.; Krueger, J.; et al. A Randomized Open-Label Clinical trial of Lipid-Lowering Therapy in Psoriasis to Reduce Vascular Endothelial Inflammation. J. Investig. Dermatol. 2022, 142, 1749–1752.e4. [Google Scholar] [CrossRef]
- Naseri, M.; Hadipour, A.; Sepaskhah, M.; Namazi, M.R. The remarkable beneficial effect of adding oral simvastatin to topical betamethasone for treatment of psoriasis: A double-blind, randomized, placebo-controlled study. Niger. J. Med. 2010, 19, 58–61. [Google Scholar] [CrossRef]
- Wolkenstein, P.; Revuz, J.; Roujeau, J.C.; Bonnelye, G.; Grob, J.J.; Bastuji-Garin, S. Psoriasis in France and Associated Risk Factors: Results of a Case-Control Study Based on a Large Community Survey. Dermatology 2009, 218, 103–109. [Google Scholar] [CrossRef]
- Shirinsky, I.V.; Shirinsky, V.S. Efficacy of simvastatin in plaque psoriasis: A pilot study. J. Am. Acad. Dermatol. 2007, 57, 529–531. [Google Scholar] [CrossRef]
- Soodgupta, D.; Kaul, S.; Kanwar, A.J.; Parsad, D. Modulation of LXR-α and the effector genes by Ascorbic acid and Statins in psoriatic keratinocytes. Mol. Cell. Biochem. 2014, 397, 1–6. [Google Scholar] [CrossRef]
- Garschick, M.S.; Block, R.; Drenkova, K.; Tawil, M.; James, G.; Brenna, J.T. Statin therapy upregulates arachidonic acid status via enhanced endogenous synthesis in patients with plaque psoriasis. Prostaglandins Leukot. Essent. Fat. Acids 2022, 180, 102428. [Google Scholar] [CrossRef]
- Vasiuk, I.A.; Perlamutrov, I.N.; Shkol’nik, M.N.; Shkol’nik, E.L. Possibilities of atorvastatin in complex management of extensive psoriasis in patients with arterial hypertension. Kardiologiia 2010, 50, 37–46. [Google Scholar]
- Chua, S.H.H.; Tioleco, G.M.S.; Dayrit, C.A.F.; Mojica, W.P.; Dofitas, B.L.; Frez, L.F. Atorvastatin as adjunctive therapy for chronic type psoriasis versus betamethasone valerate alone: A randomized, double-blind, placebo-controlled trial. Indian J. Dermatol. Venerol. Leprol. 2017, 83, 441–447. [Google Scholar] [CrossRef]
- Faghihi, T.; Radfar, M.; Mehrabian, Z.; Ehsani, A.H.; Hemami, M.R. Atorvastatin for the treatment of plaque-type psoriasis. Pharmacotherapy 2011, 31, 1045–1050. [Google Scholar] [CrossRef]
- Salman, M.A.; Ghiasi, M.; Farid, A.S.; Taraz, M.; Azizpour, A.; Mahmoudi, H. Oral simvastatin combined with narrowband UVB for the treatment of psoriasis: A randomized controlled trial. Dermatol. Ther. 2021, 34, 315075. [Google Scholar] [CrossRef]
- Aslam, S.; Khurshid, K.; Asad, F.; Rani, Z.; Pal, S.S.P. Efficacy and safety of simvastatin in chronic plaque psoriasis. J. Pak. Assoc. Dermatol. 2013, 23, 310–314. [Google Scholar]
- Colsman, A.; Sticherling, M. Simvastatin in psoriasis: Ambiguous effects. Acta Derm. Venereol. 2010, 90, 411. [Google Scholar] [CrossRef]
- Cozzani, E.; Scaparro, M.; Parodi, A. A case of psoriasis worsened by atorvastatin. J. Dermatol. Case Rep. 2009, 3, 60–61. [Google Scholar] [CrossRef]
- Salna, M.P.; Singer, H.M.; Dana, A.N. Pravastatin-Induced Eczematous Eruption Mimicking Psoriasis. Case Rep. Dermatol. Med. 2017, 2017, 3418204. [Google Scholar] [CrossRef] [Green Version]
- Jacobi, T.C.; Higher, A. A clinical dilemma while treating hypercholesterolemia in psoriasis. Br. J. Dermatol. 2003, 149, 1305–1306. [Google Scholar] [CrossRef]
- Vahlquist, C.; Olsson, A.G.; Lindholm, A.; Vahlquist, A. Effects of gemfibrozil (Lopid) on hyperlipidemia in acitretin-treated patients. Results of a double-blind cross-over study. Acta Derm. Venereol. 1995, 75, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Fisher, D.A.; Elias, P.M.; LeBoit, P.L. Exacerbation of Psoriasis by the Hypolipidemic Agent, Gemfibrozil. Arch. Dermatol. 1988, 124, 854–855. [Google Scholar] [CrossRef] [PubMed]
- Bongartz, T.; Coras, B.; Vogt, T.; Scholmerlich, J.; Muller-Ladner, U. Treatment of active psoriatic arthritis with the PPARgamma ligand pioglitazone: An open-label pilot study. Rheumatology 2005, 44, 126–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafiq, N.; Malhotra, S.; Pandhi, P.; Gupta, M.; Kumar, B.; Sandhu, K. Pilot trial: Pioglitazone versus placebo in patients with plaque psoriasis (the P6). Int. J. Dermatol. 2005, 44, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Lajevardi, V.; Hallaji, Z.; Daklan, S.; Abedini, R.; Goodarzi, A.; Abdolreza, M. The efficacy of methotrexate plus pioglitazone vs. methotrexate alone in the management of patients with plaque-type psoriasis: A single-blinded randomized controlled trial. Int. J. Dermatol. 2015, 54, 95–101. [Google Scholar] [CrossRef]
- Abidi, A.; Rizvi, D.A.; Saxena, K.; Chaudhary, S.; Ahmad, A. The evaluation of efficacy and safety of methotrexate and pioglitazone psoriasis patients: A randomized, open-labeled, active-controlled clinical trial. Indian J. Pharmacol. 2020, 52, 16–22. [Google Scholar] [CrossRef]
- Mittal, R.; Malhotra, S.; Pandhi, P.; Kaur, I.; Dogra, S. Efficacy and safety of combination Acitretin and Pioglitazone therapy in patients with moderate to severe chronic plaque-type psoriasis: A randomized, double-blind, placebo-controlled clinical trial. Arch. Dermatol. 2009, 145, 387–393. [Google Scholar] [CrossRef]
- Ghiasi, M.; Ebrahimi, S.; Lajevardi, V.; Taraz, M.; Azizpour, A. Efficacy and safety of pioglitazone plus phototherapy versus phototherapy in patients with plaque type psoriasis: A Double Blinded Randomized Controlled Trial. J. Dermatol. Treat. 2019, 30, 664–667. [Google Scholar] [CrossRef]
- Hafez, V.G.; Bosseila, M.; Halim, M.R.E.A.; Shaker, O.G.; Kamal, M.; Kareem, H.S. Clinical effects of ”pioglitazone”, an insulin sensitizing drug, on psoriasis vulgaris and its co-morbidities, a double blinded randomized controlled trialx1. J. Dermatol. Treat. 2015, 26, 208–214. [Google Scholar] [CrossRef]
- Pershadsingh, H.A.; Benson, S.C.; Ellis, C.N. Improvement in psoriasis with rosiglitazone in a diabetic and a nondiabetic patient. SKINmed 2005, 4, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Ellis, C.N.; Barker, J.N.; Haig, A.E.; Parker, C.A.; Daly, S.; Jayawardene, D.A.; Avandia Psoriasis Study Group. Placebo response in two long-term randomized psoriasis studies that were negative for rosiglitazone. Am. J. Clin. Dermatol. 2007, 8, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Xu, X.; Yu, Y.; Ye, H.; He, X.; Chen, S.; Chen, X.; Shao, Z.; Chen, P. Glucagon-like peptide-1 receptor agonist liraglutide therapy for psoriasis patients with type 2 diabetes: A randomized controlled trial. J. Dermatol. Treat. 2022, 33, 1428–1434. [Google Scholar] [CrossRef] [PubMed]
- Faurschou, A.; Knop, F.K.; Thyssen, J.P.; Zachariae, C.; Skov, L.; Visboll, T. Improvement in psoriasis after treatment with the glucagon-like peptide-1 receptor agonist liraglutide. Acta Diabetol. 2014, 51, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Ahern, T.; Tobin, A.-M.; Corrigan, M.; Hogan, A.; Sweeney, C.; Kirby, B.; O’Shea, D. Glucagon-like peptide-1 analogue therapy for psoriasis patients with obesity and type 2 diabetes: A prospective cohort study. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 1440–1443. [Google Scholar] [CrossRef]
- Faurschou, A.; Gyldenlove, M.; Rohde, U.; Thyssen, J.P.; Zachariae, C.; Skov, L.; Knop, F.K.; Vilsboll, T. Lack of effect of the glucagon-like peptide-1 receptor agonist liraglutide on psoriasis in glucose-tolerant patients—A randomized placebo- controlled trial. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 555–559. [Google Scholar] [CrossRef]
- Buysschaert, M.; Tennstedt, D.; Preumont, V. Improvement of psoriasis during exenatide treatment in a patient with diabetes. Diabetes Metab. 2012, 38, 86–88. [Google Scholar] [CrossRef]
- Buysschaert, M.; Baeck, M.; Preumont, V.; Marot, L.; Hendrickx, E.; Van Belle, A.; Dumoutier, L. Improvement of psoriasis during glucagon-like peptide-1 analogue therapy in type 2 diabetes is associated with decreasing dermal γδ T-cell number: A prospective case-series study. Br. J. Dermatol. 2014, 171, 155–161. [Google Scholar] [CrossRef]
- Hogan, A.E.; Tobin, A.M.; Ahern, T.; Corrigan, M.A.; Gaoatswe, G.; Jackson, R.; O’Reilly, V.; Lynch, L.; Doherty, D.G.; Moynagh, P.N.; et al. Glucagon-like peptide-1 (GLP-1) and the regulation of human invariant natural killer T cells, lessons from obesity, diabetes and psoriasis. Diabetologia 2011, 54, 2745–2754. [Google Scholar] [CrossRef] [Green Version]
- Reid, C.T.; Tobin, A.M.; Ahern, T.; O’Shea, D.; Kirby, B. Liraglutide in combination with acitretin for severe recalcitrant psoriasis. Br. J. Dermatol. 2013, 169, 230–231. [Google Scholar] [CrossRef]
- Costanzo, G.; Curatolo, S.; Busa, B.; Belfiore, A.; Gullo, D. Two birds one stone: Semaglutide is highly effective against severe psoriasis in a type 2 diabetic patient. Endocrinol. Diabetes Metab. Case Rep. 2021, 2021, 21-0007. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author | Year | Population | Key Observations |
|---|---|---|---|
| Statins’ Influence on Psoriasis with Therapeutic Effects | |||
| Trong et al. [1] | 2019 | n1—128 patients n2—128 patients | Simvastatin might play a role in controlling hyperlipidemia, and in turn decrease the PASI scores in psoriatic patients. |
| Garshick et al. [7] | 2020 | n1—10 patients n2—15 patients | Statins can lower cardiovascular risk in psoriasis through lipid-mediated or direct effect of statins on the vascular endothelium. |
| Naseri et al. [8] | 2010 | n1—15 patients n2—patients | Oral simvastatin enhances the therapeutic effects of topical steroids against psoriasis. |
| Wolkenstein et al. [9] | 2009 | First study n1—1068 patients n2—356 patients Second study n1—501 patients n2—167 patients | Statins appeared to be associated with a decreased risk of psoriasis. |
| Shirinsky et al. [10] | 2007 | n—7 patients | Simvastatin at a dosage of 40 mg/d was associated with clinical improvements for psoriasis and was well tolerated. |
| Soodgupta et al. [11] | 2014 | n—psoriatic patients (from 18 to 40 years) | LXR may play a big role in therapeutic importance for psoriasis. |
| Garschick et al. [12] | 2022 | n1—10 patients n2—20 patients | After the treatment, LDL-C was 44% lower in the statin group compared to the no-treatment group |
| Vasiuk et al. [13] | 2010 | n1—15 patients n2—48 patients | Six months of therapy with atorvastatin resulted in a significant lowering of the PASI compared to the control group. |
| Chua et al. [14] | 2017 | n1—6 patients n2—8 patients | After 6 months, mean reductions in PASI scores of the group where patients took atorvastatin were higher than those of the placebo group. |
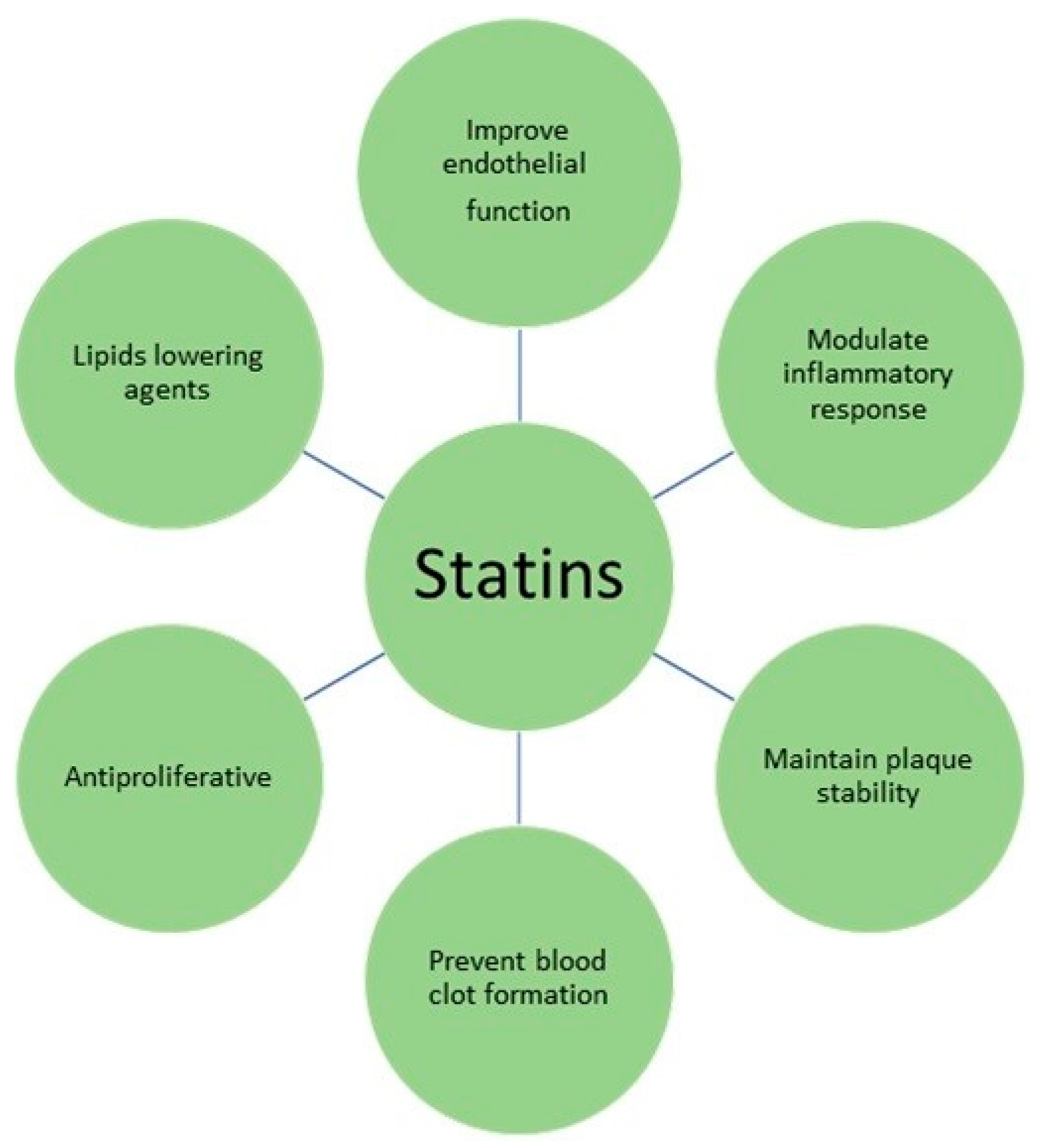
| Lipids lowering agents | Statins inhibit 2-hydroxyl-methyl-glutaryl coenzyme A (HMG-CoA) reductase, the rate-limiting step in cholesterol synthesis. This process leads to a reduced intracellular cholesterol concentration and the removal of LDL-C from the circulation. |
| Improvement of endothelial function | Statins improve flow-mediated dilatation. Statins reduce caveolin 1 levels, decreasing its inhibitory effects on nitric oxide synthesis, which has been shown to inhibit several components of the atherogenic process. |
| Modulation of inflammatory response | Statins reduce C-reactive protein (CRP) levels. Statins inhibit MHC-II expression on endothelial cells and monocyte-macrophages via inhibition of the promotor IV of the transactivator CIITA, and thereby repress MHC-II-mediated T-cell activation. In addition, statins have been shown to decrease CD40 expression and CD40-related activation of vascular cells. Moreover, statins might decrease the activity of activator protein-1 (AP-1), which regulate genes responsible for metalloproteinases (MMPs), cytokines, chemokines, adhesion molecules, and inducible nitric oxide synthase (iNOS). |
| Maintenance of plaque stability | Statins reduce the in vitro cholesterol accumulation in macrophages and the expression of matrix metalloproteinases, which subsequently leads to plaque stability. |
| Prevention of blood clot formation | Statins’ actions were associated with reduced rates of prothrombin activation, factor Va generation, fibrinogen cleavage, factor XIII activation, and increased rates of factor Va inactivation. |
| Antiproliferative function | Treatment with statins decreased PDGF-induced Rb hyperphosphorylation and cyclin-dependent kinases (cdk)-2, -4, and -6 activities. This correlated with increased levels of the Cdk inhibitor( i.e., p27Kip1) without concomitant changes in p16INK4, p21Waf1, or p53 levels. These findings indicate that statins inhibit vascular smooth muscle cell proliferation by arresting the cell cycle between G1/S phase transitions. |
| Patient’s Group | Before Treatment | p | 4th Week | p | 8th Week | p |
|---|---|---|---|---|---|---|
| Cholesterol concentration | 5.45 ± 1.21 mm/L | <0.001 | 4.20 ± 0.82 mm/L | <0.001 | 4.18 ± 0.72 mm/L | <0.001 |
| Triglyceride level | 1.86 ± 1.17 mm/L | 0.07 | 1.32 ± 0.84 mm/L | 0.07 | 1.26 ± 0.65 mm/L | <0.005 |
| LDL-c level | 3.18 ± 0.7 mm/L | <0.001 | 2.31 ± 0.80 mm/L | <0.001 | 2.26 ± 0.7 mm/L | <0.001 |
| HDL levels | 1.33 ± 0.31 mm/L | <0.001 | 1.29 ± 0.24 mm/L | 1.35 ± 0.24 mm/L | ||
| PASI | 12.8 ± 5.87 | 8.58 ± 5.62 | <0.01 | 4.17 ± 3.81 | <0.001 |
| Author | Year | Population | Key Observations |
|---|---|---|---|
| Statins’ Influence on Psoriasis without Significant Therapeutic Effects | |||
| Faghihi et al. [15] | 2011 | n1—20 patients n2—20 patients | Oral atorvastatin (40 mg/day) was not associated with therapeutic benefits when given to patients with baseline PASI scores less than 12, who were also treated with standard topical therapies. |
| Salman et al. [16] | 2021 | n1—20 patients n2—20 patients | Both groups were characterized with a significant decrease in the PASI score after 6 and 12 weeks, compared to the basic one. |
| Aslam et al. [17] | 2013 | n—60 patients | The improvement in PASI scores in patients who were given simvastatin was only noticed in 12 patients out of 60; they experienced a reduction in the PASI score of >50%. |
| Author | Year | Population | Key Observations |
|---|---|---|---|
| Statins’ Deteriorating Influence on Psoriasis | |||
| Colsman et al. [18] | 2010 | n—5 patients | In one patient the PASI deteriorated temporarily by 50% from 20 to 29, and in another patient it raised from 7 to 10. |
| Cozzani et al. [19] | 2009 | n—1 patient | After initiation with atorvastatin, the psoriatic lesions on his arms worsened and became itchy. New plaques formed on both of his legs. The PASI rose from 6.8 to 12.3. |
| Salna et al. [20] | 2017 | n—1 patient | Pravastatin can be associated with psoriasis-like eczematous lesions which may be resistant to the treatment with steroids or immunosuppressive therapies. |
| Jacobi et al. [21] | 2003 | n—1 patient | Servastatin may flare-up papular psoriasis. |
| Author | Year | Population | Key Observation |
|---|---|---|---|
| Fibrate’s Influence on Psoriasis with Therapeutic Effects | |||
| Imamura et al. [2] | 1991 | n—2 patients | Clofibrate treatment improved triglyceride levels and the histological and clinical findings in psoriatic lesions. |
| Vahlquist et al. [22] | 1995 | n—14 patients | Gemfibrozil appears useful in patients prone to retinoid-induced hyperlipidemia that is unresponsive to dietary treatments and acitretin dose reductions. |
| Author | Year | Population | Key Observations |
|---|---|---|---|
| Fibrate’s Deteriorating Influence on Psoriasis | |||
| Fisher et al. [23] | 1988 | n—1 patient | Gemfibrozil administration may cause papulosquamous skin lesions. |
| Author | Year | Population | Key Observations |
|---|---|---|---|
| Pioglitazone’s Influence on Psoriasis with Therapeutic Effects | |||
| Singh et al. [3] | 2016 | n1—23 patients n2—16 patients n3—21 patients | Pioglitazone treatment of 12 weeks showed major improvements in triglycerides, total cholesterol, LDL-C levels, and psoriatic symptoms. |
| Bongartz et al. [24] | 2004 | n—10 patients | In people who were taking pioglitazone, the average reduction in PASI was 38%. |
| Shafiq et al. [25] | 2005 | n1—25 patients n2—21 patients n3—24 patients | Two-thirds of patients with plaque psoriasis seem to improve with the use of pioglitazone. |
| Author | Year | Population | Key Observations |
|---|---|---|---|
| Pioglitazone’s Influence on Psoriasis Along with Typical Anti-Psoriatic Treatments | |||
| Lajevardi et al. [26] | 2014 | n1—22 patients n2—22 patients | The combination therapy of pioglitazone and methotrexate has a major therapeutic effect on the severity of psoriasis than the therapy with a single factor. |
| Abidi et al. [27] | 2020 | n1—30 patients n2—30 patients n3—30 patients | Combination of methotrexate and pioglitazone proved superior in efficacy. |
| Mittal et al. [28] | 2009 | n1—22 patients n2—19 patients | The percentage of reduction in the PASI score was more major in the acitretin plus pioglitazone group, than in the acitretin plus placebo group. |
| Ghiasi et al. [29] | 2018 | n1—30 patients n2—30 patients | Pioglitazone can vastly enhance the effectiveness of phototherapy in patients with plaque psoriasis. |
| Weeks | Group A (Methotrexate 7.5 mg/Week for 12 Weeks) | Group B (Pioglitazone 15 mg Tablets Once Daily for 12 Weeks) | Group C (Methotrexate 7.5 mg/Week and Pioglitazone 15 mg/Day) | |
|---|---|---|---|---|
| PASI | PASI | PASI | p | |
| 0 | 17.68 ± 1.103 | 17.73 ± 1.203 | 18.12 ± 1.419 | 0.275 |
| 4 | 11.86 ± 1.062 | 11.75 ± 1.486 | 11.87 ± 1.317 | 0.929 |
| 8 | 6.717 ± 1.026 | 6.723 ± 1.428 | 5.807 ± 1.069 | 0.004 |
| 12 | 3.797 ± 0.6185 | 4.540 ± 1.467 | 3.063 ± 0.6178 | <0.0001 |
| Author | Year | Population | Key Observations |
|---|---|---|---|
| Pioglitazone’s Influence on Psoriasis without Significant Therapeutic Effects | |||
| Hafez et al. [30] | 2015 | n1—24 patients n2—24 patients | This study revealed that pioglitazone (30 mg daily) produced no therapeutic effect on the moderate-to-severe psoriasis. |
| Author | Year | Population | Key Observations |
|---|---|---|---|
| Rosiglitazone’s Influence on Psoriasis | |||
| Pershadsingh et al. [31] | 2005 | n—2 patients | Rosiglitazone may be useful in treating psoriasis vulgaris. |
| Ellis et al. [32] | 2007 | n—2595 patients | Rosiglitazone treatment was not more effective than the placebo treatment in patients who were suffering from moderate-to-severe chronic plaque psoriasis |
| Author | Year | Population | Key Observations |
|---|---|---|---|
| Liraglutide’s Influence on Psoriasis with Therapeutic Effects | |||
| Xu et al. [4] | 2019 | n—7 patients | Liraglutide can improve psoriatic skin lesions in patients with type 2 diabetes, especially in cases of extremely severe psoriasis. |
| Lin et al. [33] | 2020 | n1—13 patients n2—12 patients | Skin lesions in psoriatic patients with type 2 diabetes were significantly improved after the treatment with liraglutide. This may be related to the inhibition of the expression of inflammatory factors, such as IL-23, IL-17, and TNF-a. |
| Faurschou et al. [34] | 2011 | n—1 patient | Liraglutide markedly improved psoriasis in a patient treated for type 2 diabetes. |
| Ahern et al. [35] | 2012 | n—7 patients | Liraglutide therapy improves psoriasis severity, increases the circulating iNKT cell number, and modulates monocyte and cytokine secretions. |
| Week | Control Group | Treatment Group | ||||
|---|---|---|---|---|---|---|
| PASI | DLQI | p | PASI | DLQI | p | |
| 0 | 13.57 ± 5.49 | 18.23 ± 5.17 | <0.05 | 14.02 ± 10.67 | 22.00 ± 5.85 | <0.05 |
| 12 | 7.42 ± 3.91 | 9.69 ± 4.59 | <0.05 | 2.40 ± 2.71 | 3.82 ± 3.60 | <0.05 |
| Author | Year | Population | Key Observations |
|---|---|---|---|
| Liraglutide’s Lack of Influence on Psoriasis | |||
| Faurschou et al. [36] | 2014 | n1—9 patients n2—11 patients | Liraglutide treatment of 8 weeks did not significantly change PASI and DLQI scores in a group of patients with plaque psoriasis, compared to the placebo group. |
| Author | Year | Population | Key Observations |
|---|---|---|---|
| Exenatide’s Influence on Psoriasis | |||
| Buysschaert et al. [37] | 2012 | n—1 patient | There was a major and rapid improvement in psoriasis in our patients with diabetes mellitus following the exenatide treatment. |
| Author | Year | Population | Key Observations |
|---|---|---|---|
| Liraglutide’s and Exenatide’s Influence on Psoriasis | |||
| Buysschaert et al. [38] | 2014 | n—7 patients | The administration of an exenatide/liraglutide improved the severity of clinical psoriasis in patients with type 2 diabetes. This favorable outcome was associated with a decrease in dermal cd T-cell numbers and the IL-17 expression. |
| Hogan et al. [39] | 2011 | n—2 patients | The PASI improved in both patients following 6 weeks of liraglutide and exenatide therapy. |
| Author | Year | Population | Key Observations |
|---|---|---|---|
| Liraglutide’s Influence on Psoriasis along with Typical Anti-Psoriatic Treatments | |||
| Reid et al. [40] | 2013 | n—1 patient | Liraglutide may be an effective adjunctive treatment option against psoriasis. |
| Costanzo et al. [41] | 2021 | n—1 patient | During semaglutide with typical anti-psoriatic treatment, a rapid improvement of severe psoriasis lesions was observed. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matwiejuk, M.; Mysliwiec, H.; Jakubowicz-Zalewska, O.; Chabowski, A.; Flisiak, I. Effects of Hypolipidemic Drugs on Psoriasis. Metabolites 2023, 13, 493. https://doi.org/10.3390/metabo13040493
Matwiejuk M, Mysliwiec H, Jakubowicz-Zalewska O, Chabowski A, Flisiak I. Effects of Hypolipidemic Drugs on Psoriasis. Metabolites. 2023; 13(4):493. https://doi.org/10.3390/metabo13040493
Chicago/Turabian StyleMatwiejuk, Mateusz, Hanna Mysliwiec, Olivia Jakubowicz-Zalewska, Adrian Chabowski, and Iwona Flisiak. 2023. "Effects of Hypolipidemic Drugs on Psoriasis" Metabolites 13, no. 4: 493. https://doi.org/10.3390/metabo13040493