
Enhanced Carotid Plaque Echolucency Is Associated with Reduced Cognitive Performance in Elderly Patients with Atherosclerotic Disease Independently on Metabolic Profile

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Cognitive Function Assessment
2.3. Ultrasound Method
2.4. Plaque Echogenicity
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| GSM | NASCET | MMSE | TMT A | TMT B | TMT B-A | VFT | Z-Score | ||
|---|---|---|---|---|---|---|---|---|---|
| BMI | rho | 0.0539 | −0.1657 | 0.0958 | 0.1893 | 0.0725 | −0.0349 | −0.1007 | −0.1094 |
| p | 0.5709 | 0.0795 | 0.3127 | 0.0446 | 0.4455 | 0.7137 | 0.2886 | 0.2486 | |
| TC | rho | −0.0516 | −0.0208 | 0.0902 | −0.015 | −0.0847 | −0.0875 | 0.1255 | 0.099 |
| p | 0.5873 | 0.8268 | 0.3422 | 0.8751 | 0.3724 | 0.3566 | 0.1855 | 0.2969 | |
| HDL | rho | 0.0772 | 0.0744 | 0.1279 | −0.1338 | −0.2102 | −0.1605 | 0.1372 | 0.1916 |
| p | 0.4162 | 0.4337 | 0.177 | 0.1577 | 0.0255 | 0.0894 | 0.1474 | 0.042 | |
| LDL | rho | −0.0045 | −0.0485 | 0.0871 | −0.0397 | −0.0881 | −0.0744 | 0.1391 | 0.1095 |
| p | 0.9621 | 0.6099 | 0.3588 | 0.6764 | 0.3535 | 0.4337 | 0.1418 | 0.2484 | |
| TG | rho | −0.1173 | −0.0069 | −0.0828 | 0.1217 | 0.1478 | 0.113 | −0.0987 | −0.146 |
| p | 0.2159 | 0.9419 | 0.3833 | 0.1992 | 0.1183 | 0.2335 | 0.2981 | 0.1228 | |
| SBP | rho | −0.1022 | 0.2292 | −0.1216 | 0.0092 | 0.0459 | 0.0368 | 0.0675 | −0.0022 |
| p | 0.2816 | 0.0146 | 0.1996 | 0.9226 | 0.6294 | 0.6988 | 0.4776 | 0.9813 | |
| DBP | rho | −0.013 | 0.196 | −0.1006 | 0.0304 | 0.0403 | 0.0155 | 0.0456 | −0.0055 |
| p | 0.8917 | 0.0375 | 0.2891 | 0.7493 | 0.672 | 0.8707 | 0.6318 | 0.9543 |
Appendix B
| Z-Score | Coefficient | 95% C.I. | p |
|---|---|---|---|
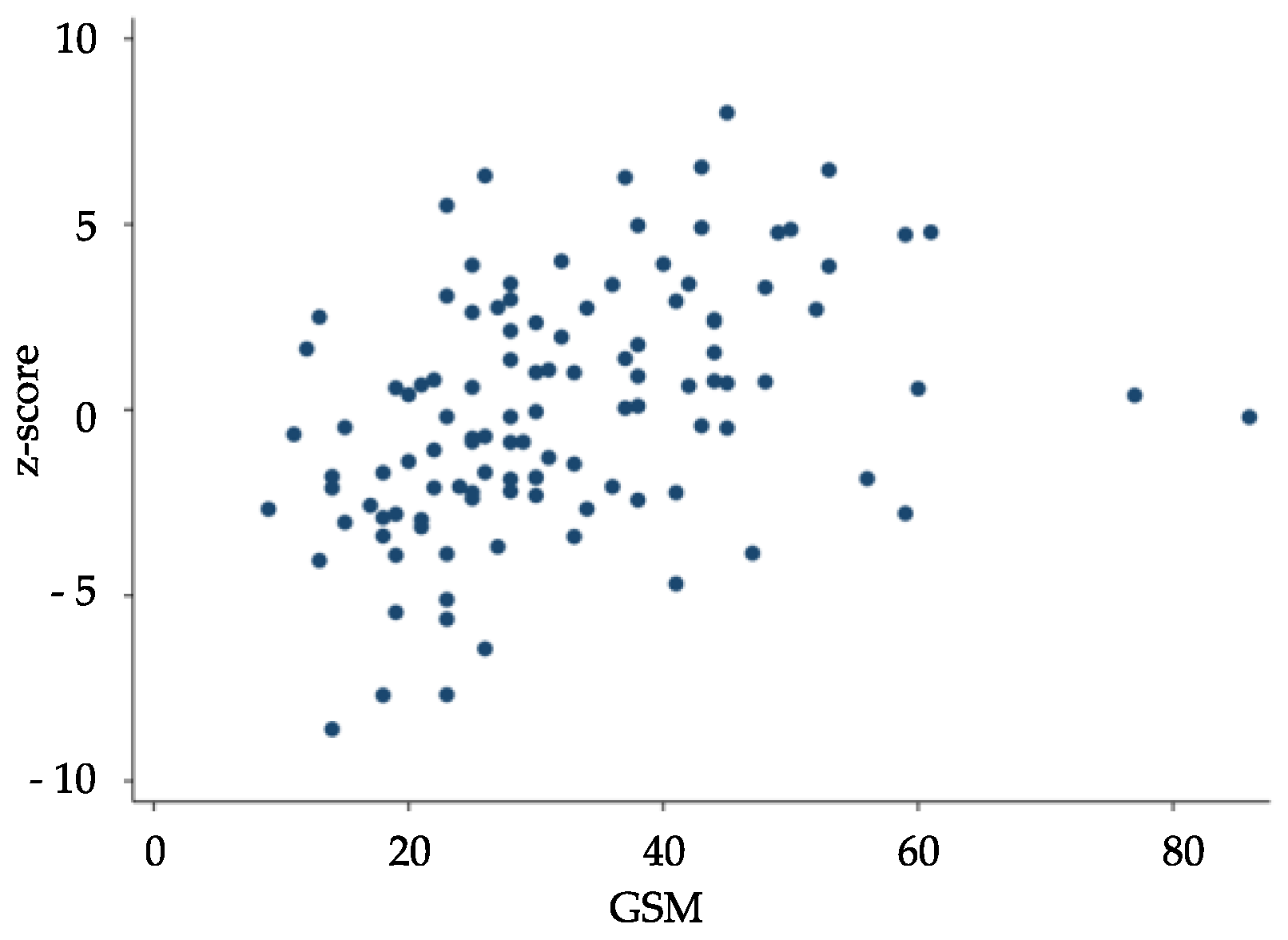
| GSM | 0.098 | 0.056; 0.14 | <0.0001 |
| BMI | −0.077 | −0.224; 0.069 | 0.298 |
| TC | 0.022 | −0.138; 0.181 | 0.786 |
| HDL | 0.011 | −0.156; 0.179 | 0.893 |
| LDL | −0.014 | −0.172; 0.144 | 0.861 |
| TG | −0.005 | −0.039; 0.028 | 0.758 |
| SBP | −0.008 | −0.051; 0.035 | 0.722 |
| DBP | 0.023 | −0.061; 0.107 | 0.588 |
References
- Brinjikji, W.; Huston, J., 3rd; Rabinstein, A.A.; Kim, G.M.; Lerman, A.; Lanzino, G. Contemporary carotid imaging: From degree of stenosis to plaque vulnerability. J. Neurosurg. 2016, 124, 27–42. [Google Scholar] [CrossRef] [PubMed]
- Naylor, R.; Rantner, B.; Ancetti, S.; de Borst, G.J.; De Carlo, M.; Halliday, A.; Kakkos, S.K.; Markus, H.S.; McCabe, D.J.H.; Sillesen, H.; et al. Editor’s choice—European Society for Vascular Surgery (ESVS) 2023 clinical practice guidelines on the management of atherosclerotic carotid and vertebral artery disease. Eur. J. Vasc. Endovasc. Surg. 2023, 65, 7–111. [Google Scholar] [CrossRef] [PubMed]
- Paraskevas, K.I.; Mikhailidis, D.P.; Antignani, P.L.; Baradaran, H.; Bokkers, R.P.H.; Cambria, R.P.; Dardik, A.; Davies, A.H.; Eckstein, H.H.; Faggioli, G.; et al. Optimal management of asymptomatic carotid stenosis in 2021: The jury is still out. An International, Multispecialty, Expert Review and Position Statement. J. Stroke. Cerebrovasc. Dis. 2022, 31, 106–182. [Google Scholar] [CrossRef] [PubMed]
- Spence, J.D.; Coates, V.; Li, H.; Tamayo, A.; Muñoz, C.; Hackam, D.G.; DiCicco, M.; DesRoches, J.; Bogiatzi, C.; Klein, J.; et al. Effects of intensive medical therapy on microemboli and cardiovascular risk in asymptomatic carotid stenosis. Arch. Neurol. 2010, 67, 180–186. [Google Scholar] [CrossRef]
- Migdalski, A.; Jawien, A. New insight into biology, molecular diagnostics and treatment options of unstable carotid ath-erosclerotic plaque: A narrative review. Ann. Transl. Med. 2021, 9, 1207. [Google Scholar] [CrossRef] [PubMed]
- Kamtchum-Tatuene, J.; Noubiap, J.J.; Wilman, A.H.; Saqqur, M.; Shuaib, A.; Jickling, G.C. Prevalence of high-risk plaques and risk of stroke in patients with asymptomatic carotid stenosis: A meta-analysis. JAMA Neurol. 2020, 77, 1524–1535. [Google Scholar] [CrossRef]
- Sprynger, M.; Rigo, F.; Moonen, M.; Aboyans, V.; Edvardsen, T.; De Alcantara, M.L.; Brodmann, M.; Naka, K.; Kownator, S.; Simova, I.; et al. Focus on echovascular imaging assessment of arterial disease: Complement to the ESC guidelines (PARTIM 1) in collaboration with the working group on aorta and peripheral vascular diseases. Eur. Heart J.-Cardiovasc. Imaging 2018, 19, 1195–1221. [Google Scholar] [CrossRef]
- Paraskevas, K.I.; Veith, F.J.; Spence, J.D. How to identify which patients with asymptomatic carotid stenosis could benefit from endarterectomy or stenting. Stroke Vasc. Neurol. 2018, 3, 92–100. [Google Scholar] [CrossRef]
- Geroulakos, G.; Ramaswami, G.; Nicolaides, A.; James, K.; Labropoulos, N.; Belcaro, G.; Holloway, M. Characterization of symptomatic and asymptomatic carotid plaques using high-resolution real-time ultrasonography. Br. J. Surg. 1993, 80, 1274–1277. [Google Scholar] [CrossRef]
- Gonçalves, I.; Lindholm, M.W.; Pedro, L.; Dias, N.; e Fernandes, J.F.; Fredrikson, G.N.; Nilsson, J.; Moses, J.; Ares, M.P. Elastin and calcium rather than collagen or lipid content are associated with echogenicity of human carotid plaques. Stroke 2004, 35, 2795–2800. [Google Scholar] [CrossRef]
- Viticchi, G.; Falsetti, L.; Potente, E.; Bartolini, M.; Silvestrini, M. Impact of carotid stenosis on cerebral hemodynamic failure and cognitive impairment progression: A narrative review. Ann. Transl. Med. 2021, 9, 1209. [Google Scholar] [CrossRef] [PubMed]
- Paraskevas, K.I.; Fag-gioli, G.; Ancetti, S.; Naylor, A.R. Editor’s choice—Asymptomatic carotid stenosis and cognitive impairment: A systematic review. Eur. J. Vasc. Endovasc. Surg. 2021, 61, 888–899. [Google Scholar] [CrossRef] [PubMed]
- Steffel, C.N.; Brown, R.; Korcarz, C.E.; Varghese, T.; Stein, J.H.; Wilbrand, S.M.; Dempsey, R.J.; Mitchell, C.C. Influence of ultrasound system and gain on grayscale median values. J. Ultrasound Med. 2018, 38, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Biasi, G.M.; Froio, A.; Diethrich, E.B.; Deleo, G.; Galimberti, S.; Mingazzini, P.; Nicolaides, A.N.; Griffin, M.; Raithel, D.; Reid, D.B.; et al. Carotid plaque echolucency increases the risk of stroke in carotid stenting: The Imaging in Carotid Angio-plasty and Risk of Stroke (ICAROS) study. Circulation 2004, 110, 756–762. [Google Scholar] [CrossRef]
- Elatrozy, T.; Nicolaides, A.; Tegos, T.; Zarka, A.Z.; Griffin, M.; Sabetai, M. The effect of B-mode ultrasonic image stand-ardisation on the echodensity of symptomatic and asymptomatic carotid bifurcation plaques. Int. Angiol. 1998, 17, 179–186. [Google Scholar]
- Biasi, G.M.; Sampaolo, A.; Mingazzini, P.; De Amicis, P.; El-Barghouty, N.; Nicolaides, A.N. Computer analysis of ultra-sonic plaque echolucency in identifying high risk carotid bifurcation lesions. Eur. J. Vasc. Endovasc. Surg. 1999, 17, 476–479. [Google Scholar] [CrossRef]
- Touboul, P.J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Hernandez Hernandez, R.; et al. Mannheim carotid intima-media thickness and plaque consensus (2004–2006-2011). An update on behalf of the advisory board of the 3rd, 4th and 5th watching the risk symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011. Cerebrovasc. Dis. 2012, 34, 290–296. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”: A practical method for grading the cognitive state of pa-tients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Reitan, R.M. Validity of the Trail Making Test as an indicator of organic brain damage. Percept. Mot. Skills 1958, 8, 271–276. [Google Scholar] [CrossRef]
- Borkowski, J.G.; Benton, A.L.; Spreen, O. Word fluency and brain damage. Neuropsychologia 1967, 5, 135–140. [Google Scholar] [CrossRef]
- Nicolaides, A.N.; Kakkos, S.K.; Kyriacou, E.; Griffin, M.; Sabetai, M.; Thomas, D.J.; Tegos, T.; Geroulakos, G.; Labropoulos, N.; Doré, C.J.; et al. Asymptomatic Carotid Stenosis and Risk of Stroke (ACSRS) study group: Asymptomatic internal ca-rotid artery stenosis and cerebrovascular risk stratification. J. Vasc. Surg. 2010, 52, 1486–1496.e1–5. [Google Scholar] [CrossRef] [PubMed]
- Griffin, M.; Nicolaides, A.; Kyriacou, E. Normalisation of ultrasonic images of atherosclerotic plaques and reproducibility of grey scale median using dedicated software. Int. Angiol. 2007, 26, 372–377. [Google Scholar] [PubMed]
- Park, D.C.; Reuter-Lorenz, P. The adaptive brain: Aging and neurocognitive scaffolding. Annu. Rev. Psychol. 2009, 60, 173–196. [Google Scholar] [CrossRef] [PubMed]
- Zlokovic, B.V.; Gottesman, R.F.; Bernstein, K.E.; Seshadri, S.; McKee, A.; Snyder, H.; Greenberg, S.M.; Yaffe, K.; Schaffer, C.B.; Yuan, C.; et al. Vascular contributions to cognitive impairment and dementia (VCID): A report from the 2018 National Heart, Lung, and Blood Institute and National Institute of Neurological Disorders and Stroke Workshop. Alzheimer’s Dement. 2020, 16, 1714–1733. [Google Scholar] [CrossRef]
- van Oijen, M.; de Jong, F.J.; Witteman, J.C.M.; Hofman, A.; Koudstaal, P.J.; Breteler, M.M.B. Atherosclerosis and risk for dementia. Ann. Neurol. 2007, 61, 403–410. [Google Scholar] [CrossRef]
- Baradaran, H.; Sarrami, A.H.; Gupta, A. Asymptomatic carotid disease and cognitive impairment: What is the evidence? Front. Neurol. 2021, 12, 741500. [Google Scholar] [CrossRef]
- Hogea, T.; Suciu, B.A.; Ivănescu, A.D.; Carașca, C.; Chinezu, L.; Arbănași, E.M.; Russu, E.; Kaller, R.; Arbănași, E.M.; Mureșan, A.V.; et al. Increased Epicardial Adipose Tissue (EAT), left coronary artery plaque morphology, and valvular atherosclerosis as risks factors for sudden cardiac death from a forensic perspective. Diagnostics 2023, 13, 142. [Google Scholar] [CrossRef]
- Gupta, A.; Baradaran, H.; Schweitzer, A.; Kamel, H.; Pandya, A.; Delgado, D.; Dunning, A.; Mushlin, A.I.; Sanelli, P.C. Carotid plaque MRI and stroke risk. Stroke 2013, 44, 3071–3077. [Google Scholar] [CrossRef]
- Auperin, A.; Berr, C.; Bonithon-Kopp, C.; Touboul, P.-J.; Ruelland, I.; Ducimetiere, P.; Alperovitch, A. Ultrasonographic assessment of carotid wall characteristics and cognitive functions in a community sample of 59- to 71-Year-Olds. Stroke 1996, 27, 1290–1295. [Google Scholar] [CrossRef]
- Chen, W.-H.; Jin, W.; Lyu, P.-Y.; Liu, Y.; Li, R.; Hu, M.; Xiao, X.-J. Carotid Atherosclerosis and Cognitive Impairment in Nonstroke Patients. Chin. Med. J. 2017, 130, 2375–2379. [Google Scholar] [CrossRef]
- Nordestgaard, L.T.; Christoffersen, M.; Frikke-Schmidt, R. Shared Risk Factors between Dementia and Atherosclerotic Cardiovascular Disease. Int. J. Mol. Sci. 2022, 23, 9777. [Google Scholar] [CrossRef]
- Chalela, J. Evaluating the Carotid Plaque: Going beyond Stenosis. Cerebrovasc. Dis. 2009, 27, 19–24. [Google Scholar] [CrossRef]
- El-Barghouty, N.; Levine, T.; Ladva, S.; Flanagan, A.; Nicolaides, A. Histological verification of computerised carotid plaque characterisation. Eur. J. Vasc. Endovasc. Surg. 1996, 11, 414–416. [Google Scholar] [CrossRef] [PubMed]
- Grønholdt, M.-L.M.; Nordestgaard, B.G.; Wiebe, B.M.; Wilhjelm, J.E.; Sillesen, H. Echo-Lucency of Computerized Ultrasound Images of Carotid Atherosclerotic Plaques Are Associated With Increased Levels of Triglyceride-Rich Lipoproteins as Well as Increased Plaque Lipid Content. Circulation 1998, 97, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Mathiesen, E.B.; Bonaa, K.H.; Joakimsen, O. Echolucent plaques are associated with high risk of ischemic cerebrovascular events in carotid stenosis: The tromso study. Circulation 2001, 103, 2171e5. [Google Scholar] [CrossRef] [PubMed]
- Takasugi, J.; Miwa, K.; Watanabe, Y.; Okazaki, S.; Todo, K.; Sasaki, T.; Sakaguchi, M.; Mochizuki, H. Cortical cerebral mi-croinfarcts on 3t magnetic resonance imaging in patients with carotid artery stenosis. Stroke 2019, 50, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Desideri, G.; Cipollone, F.; Necozione, S.; Marini, C.; Lechiara, M.C.; Taglieri, G.; Zuliani, G.; Fellin, R.; Mezzetti, A.; di Orio, F.; et al. Enhanced soluble CD40 ligand and Alzheimer’s disease: Evidence of a possible pathogenetic role. Neurobiol. Aging 2008, 29, 348–356. [Google Scholar] [CrossRef]
- Cipollone, F.; Ferri, C.; Desideri, G.; Paloscia, L.; Materazzo, G.; Mascellanti, M.; Fazia, M.; Iezzi, A.; Cuccurullo, C.; Pini, B.; et al. Preprocedural level of soluble CD40L is predictive of enhanced inflammatory response and restenosis after coronary angioplasty. Circulation 2003, 108, 2776–2782. [Google Scholar] [CrossRef]
- Niculescu, R.; Russu, E.; Arbănași, E.M.; Kaller, R.; Arbănași, E.M.; Melinte, R.M.; Coșarcă, C.M.; Cocuz, I.G.; Sabău, A.H.; Tinca, A.C.; et al. Carotid Plaque Features and Inflammatory Biomarkers as Predictors of Restenosis and Mortality Following Carotid Endarterectomy. Int. J. Environ. Res. Public Health 2022, 19, 13934. [Google Scholar] [CrossRef]
- Pugh, K.G.; Kiely, D.K.; Milberg, W.P.; Lipsitz, L.A. Selective impairment of frontal-executive cognitive function in african americans with cardiovascular risk factors. J. Am. Geriatr. Soc. 2003, 51, 1439–1444. [Google Scholar] [CrossRef]
- Kolkert, J.L.; Meerwaldt, R.; Loonstra, J.; Schenk, M.; van der Palen, J.; van den Dungen, J.J.; Zeebregts, C.J. Relation be-tween B-mode gray-scale median and clinical features of carotid stenosis vulnerability. Ann. Vasc. Surg. 2014, 28, 404–410. [Google Scholar] [CrossRef] [PubMed]


| Age | 72.4 ± 5.9 |
| Gender (males/females) | 59/54 |
| BMI (kg/m2) | 27.5 ± 4.1 |
| Total cholesterol (mg/dL) | 198.2 ± 47.0 |
| HDL-C (mg/dL) | 48.1 ± 12.4 |
| LDL-C (mg/dL) | 119.5 ± 44.2 |
| Triglyceride (mg/dL) | 154.9 ± 68.1 |
| SBP (mmHg) | 138.8 ± 15.2 |
| DBP (mmHg) | 78.3 ± 8 |
| GSM | 32.1 ± 13.7 |
| NASCET (%) | 43.6 ± 20.8 |
| Hypertension (%) | 91 (80.5%) |
| Hypercholesterolemia (%) | 83 (73.5%) |
| Diabetes mellitus (%) | 22 (19.5%) |
| Smoking (%) | 17 (15.0%) |
| MMSE score | 27.5 ± 1.8 |
| TMT-A (seconds) | 78.6 ± 35.6 |
| TMT-B (seconds) | 178.6 ± 78.3 |
| TMT B-A (seconds) | 99.9 ± 57.2 |
| VFT (n. words) | 21.4 ± 7.8 |
| z-score | 0.01 ± 3.3 |
| Coefficient | 95% C.I. | p | |
|---|---|---|---|
| Age | −0.1514065 | −0.25; −0.05 | 0.003 |
| Hypertension | −0.1155479 | −1.57; 1.34 | 0.875 |
| Hypercholesterolemia | 0.5500091 | −0.73; 1.83 | 0.397 |
| Diabetes mellitus | 0.2200304 | −1.17; 1.61 | 0.755 |
| BMI | −0.1115516 | −0.25; 0.03 | 0.113 |
| GSM | 0.0954297 | 0.05; 0.14 | <0.0001 |
| NASCET | 0.0003074 | −0.03; 0.03 | 0.983 |
| GSM ≤ 29 n = 57 | GSM > 29 n = 56 | p * | |
|---|---|---|---|
| MMSE score | 27.2 ± 1.8 | 27.8 ± 1.7 | 0.078 |
| TMT-A (seconds) | 91.2 ± 34.4 | 65.8 ± 32.2 | <0.0001 |
| TMT-B (seconds) | 205.1 ± 84.9 | 151.6 ± 60.7 | <0.0001 |
| TMT B-A (seconds) | 113.8 ± 67.9 | 85.8 ± 39.5 | 0.0178 |
| VFT (n. words) | 18.9 ± 7.4 | 24.0 ± 7.4 | 0.0002 |
| z-score | −1.3 ± 3.2 | 1.3 ± 2.9 | <0.0001 |
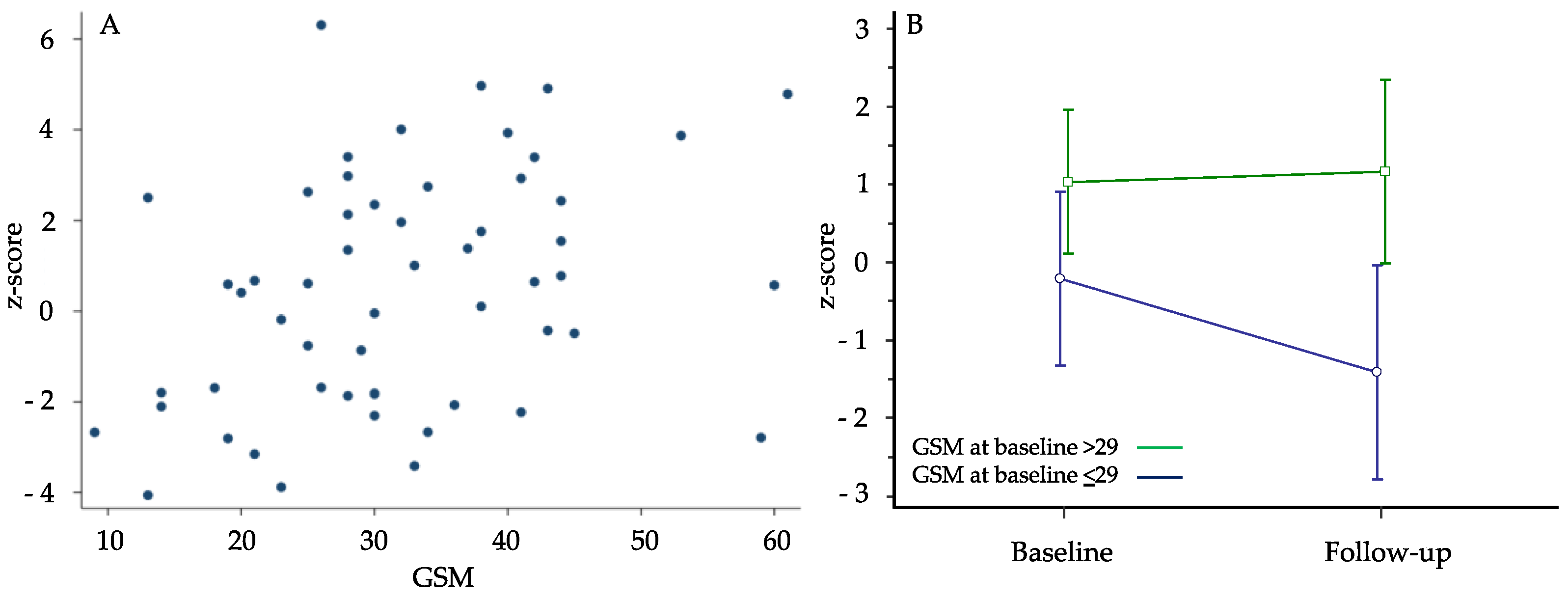
| Baseline n = 55 | Follow-Up n = 55 | p * | |
|---|---|---|---|
| MMSE score | 27.8 ± 1.7 | 27.7 ± 2.5 | 0.8710 |
| TMT-A (seconds) | 73.9 ± 30.8 | 75.0 ± 33.7 | 0.9365 |
| TMT-B (seconds) | 162.2 ± 52.8 | 193.4 ± 110.1 | 0.0103 |
| TMT B-A (seconds) | 88.3 ± 39.9 | 118.3 ± 83.8 | 0.0065 |
| VFT (n. words) | 21.7 ± 7.3 | 20.3 ± 7.2 | 0.0899 |
| z-score | 0.5 ± 2.6 | 0.1 ± 3.44 | 0.2580 |
| Coefficient | 95% C.I. | p | |
|---|---|---|---|
| Age | −0.21112 | −0.37; −0.05 | 0.013 |
| Hypertension | −2.39924 | −5.19; 0.39 | 0.09 |
| Hypercholesterolemia | 0.753556 | −1.42; 2.93 | 0.489 |
| Diabetes mellitus | 0.694924 | −1.19; 2.58 | 0.462 |
| BMI | 0.054576 | −0.16; 0.27 | 0.618 |
| GSM | 0.1117 | 0.03; 0.19 | 0.006 |
| NASCET | 0.039326 | −0.04; 0.12 | 0.316 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mastroiacovo, D.; Mengozzi, A.; Dentali, F.; Pomero, F.; Virdis, A.; Camerota, A.; Muselli, M.; Necozione, S.; Bocale, R.; Ferri, C.; et al. Enhanced Carotid Plaque Echolucency Is Associated with Reduced Cognitive Performance in Elderly Patients with Atherosclerotic Disease Independently on Metabolic Profile. Metabolites 2023, 13, 478. https://doi.org/10.3390/metabo13040478
Mastroiacovo D, Mengozzi A, Dentali F, Pomero F, Virdis A, Camerota A, Muselli M, Necozione S, Bocale R, Ferri C, et al. Enhanced Carotid Plaque Echolucency Is Associated with Reduced Cognitive Performance in Elderly Patients with Atherosclerotic Disease Independently on Metabolic Profile. Metabolites. 2023; 13(4):478. https://doi.org/10.3390/metabo13040478
Chicago/Turabian StyleMastroiacovo, Daniela, Alessandro Mengozzi, Francesco Dentali, Fulvio Pomero, Agostino Virdis, Antonio Camerota, Mario Muselli, Stefano Necozione, Raffaella Bocale, Claudio Ferri, and et al. 2023. "Enhanced Carotid Plaque Echolucency Is Associated with Reduced Cognitive Performance in Elderly Patients with Atherosclerotic Disease Independently on Metabolic Profile" Metabolites 13, no. 4: 478. https://doi.org/10.3390/metabo13040478