
NMR-Based Metabolomics Demonstrates a Metabolic Change during Early Developmental Stages from Healthy Infants to Young Children
 ,
,
Abstract
:1. Introduction
2. Experimental Design
2.1. Research Subjects
2.2. Collection and Storage of Saliva Samples
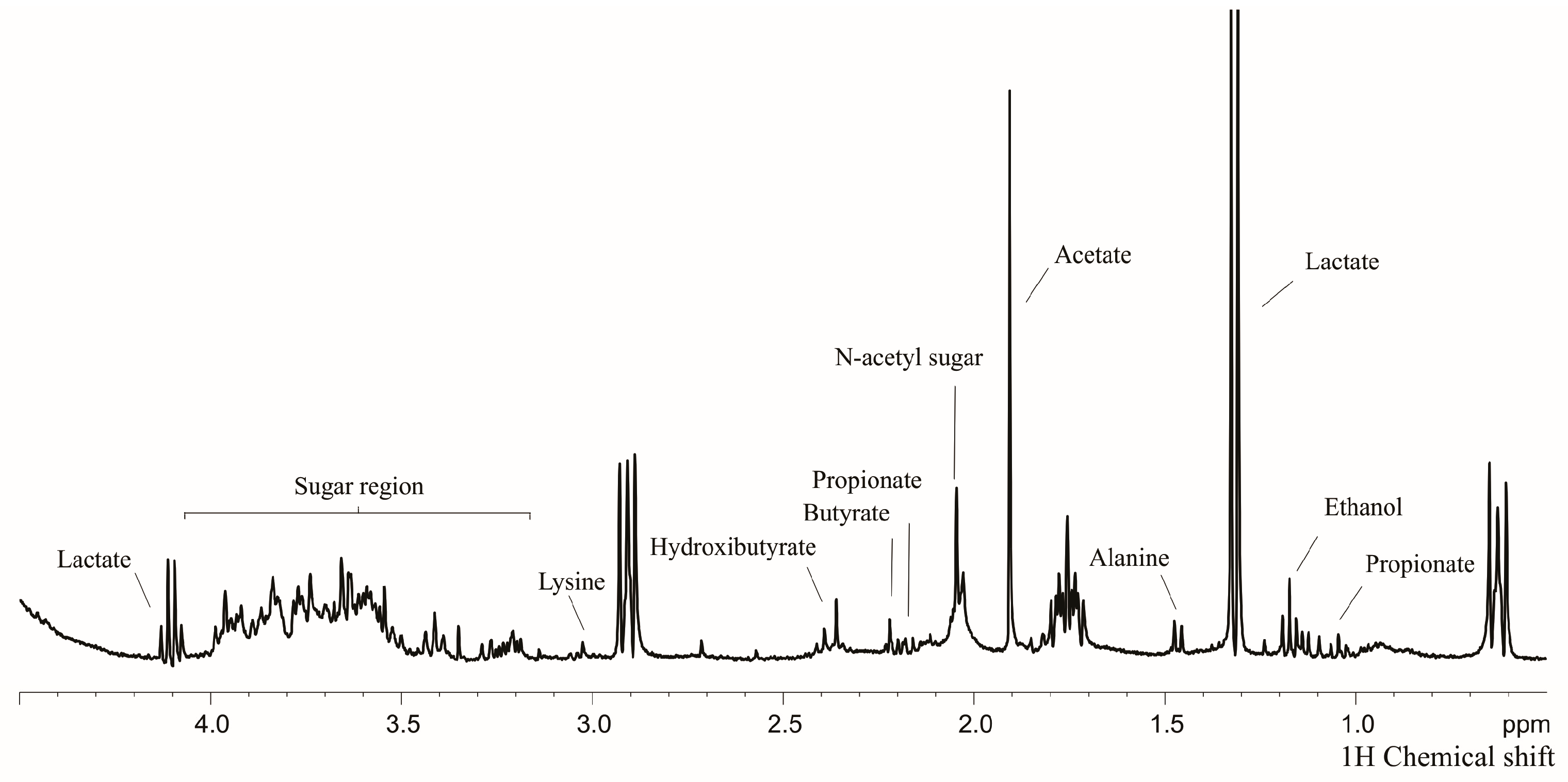
2.3. Sample Preparation for Nuclear Magnetic Resonance (NMR), Data Acquisition and Analysis
2.4. Statistical Analysis
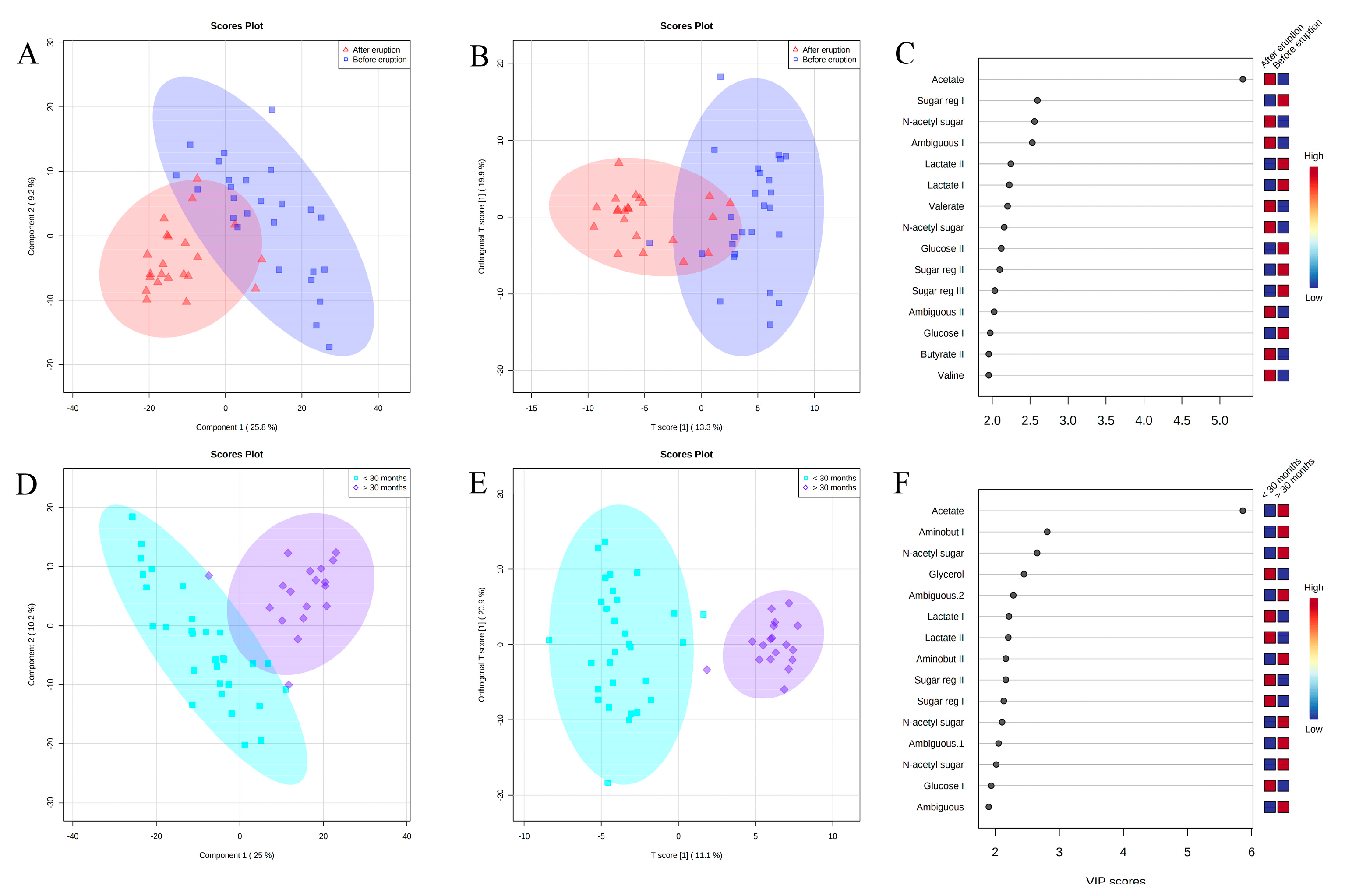
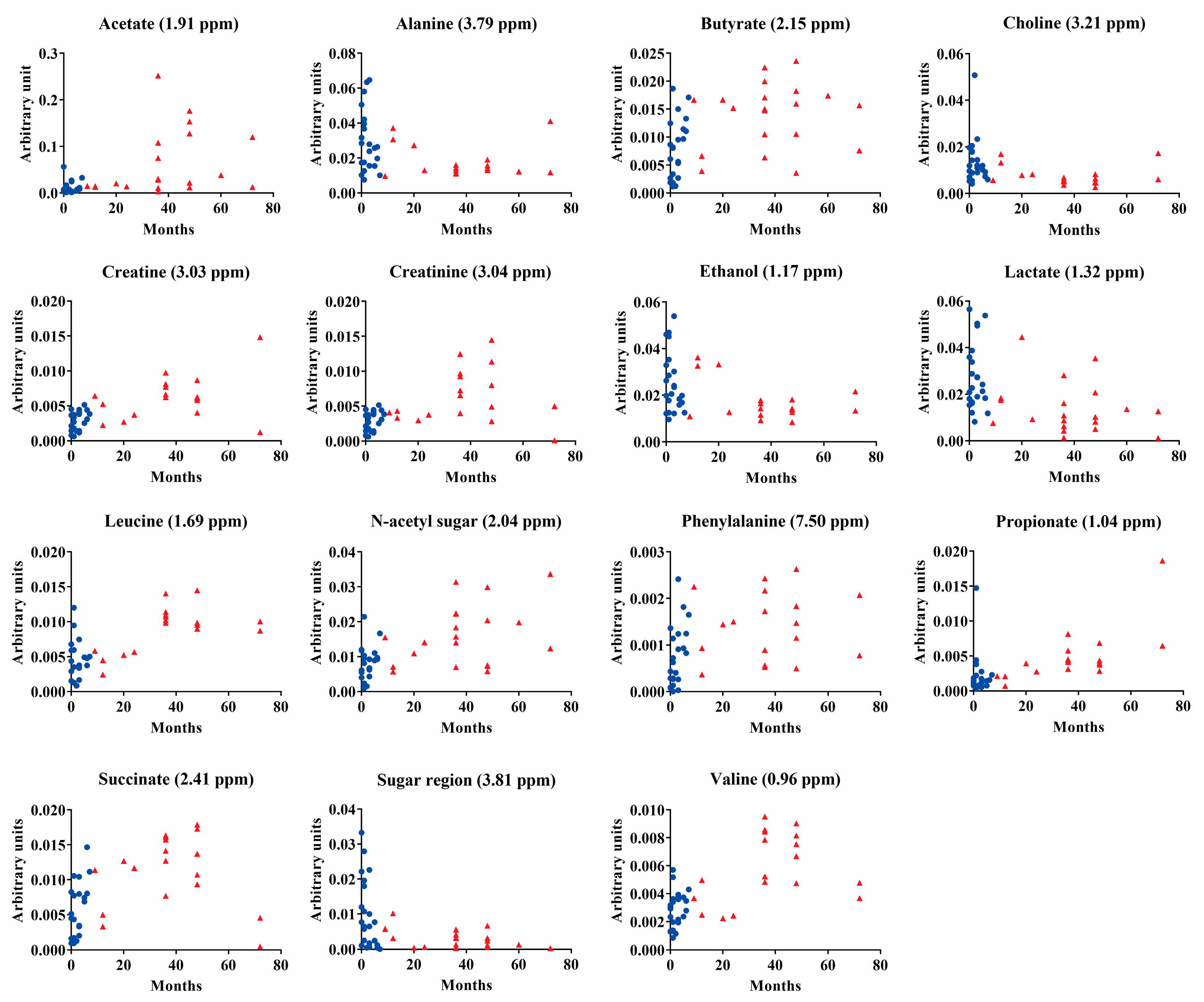
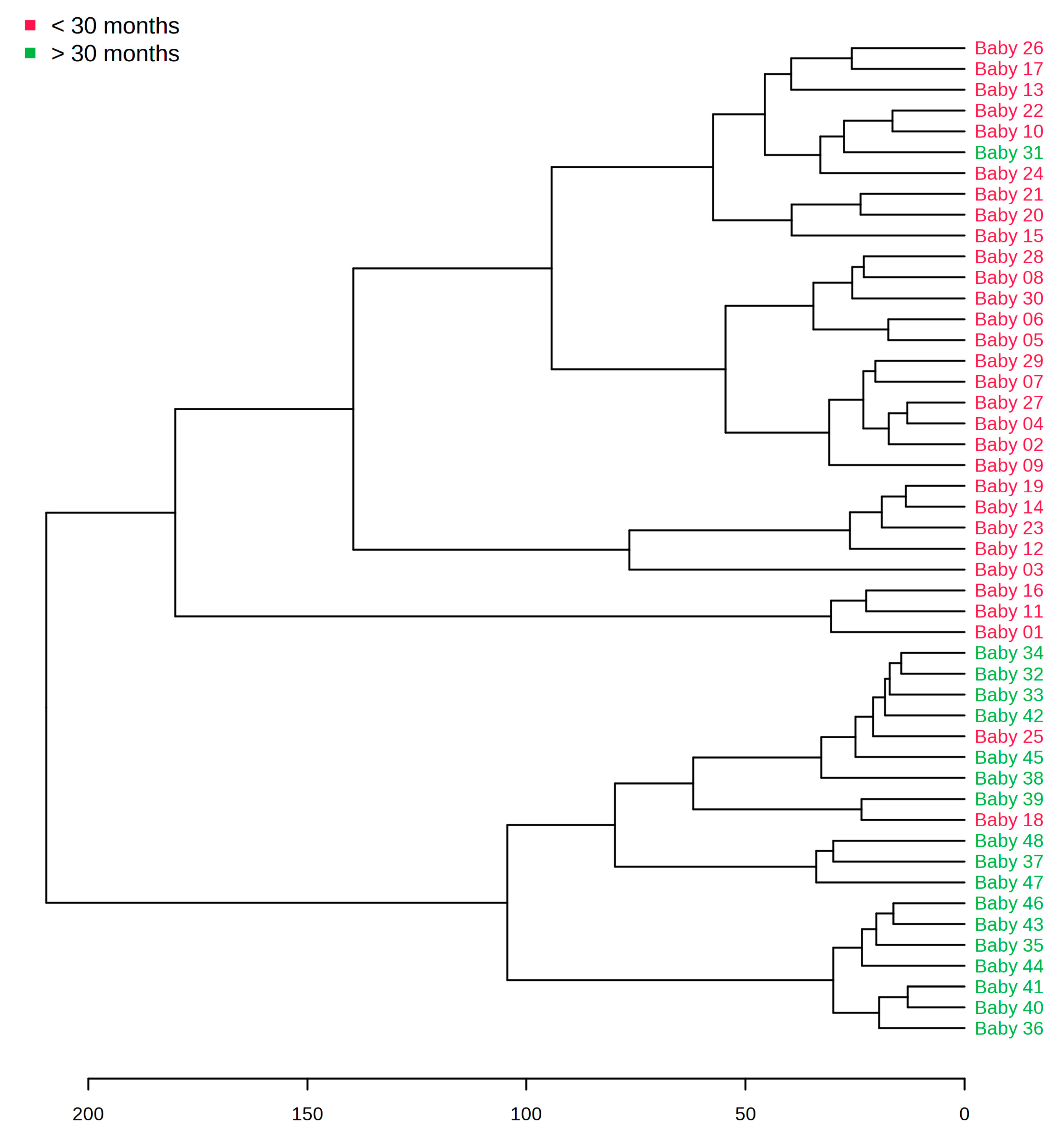
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Tarawneh, S.K.; Border, M.B.; Dibble, C.F.; Bencharit, S. Defining Salivary Biomarkers Using Mass Spectrometry-Based Proteomics: A Systematic Review. OMICS A J. Integr. Biol. 2011, 15, 353–361. [Google Scholar] [CrossRef] [Green Version]
- Dawes, C.; Wong, D. Role of Saliva and Salivary Diagnostics in the Advancement of Oral Health. J. Dent. Res. 2019, 98, 133–141. [Google Scholar] [CrossRef]
- Freitas-Fernandes, L.B.; Rundegren, J.; Arnebrant, T.; O Glantz, P. Delmopinol hydrochloride- and chlorhexidine digluconate-induced precipitation of salivary proteins of different molecular weights. Acta Odontol. Scand. 1998, 56, 2–8. [Google Scholar] [CrossRef]
- Pfaffe, T.; Cooper-White, J.; Beyerlein, P.; Kostner, K.; Punyadeera, C. Diagnostic Potential of Saliva: Current State and Future Applications. Clin. Chem. 2011, 57, 675–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeda, I.; Stretch, C.; Barnaby, P.; Bhatnager, K.; Rankin, K.; Fu, H.; Weljie, A.; Jha, N.; Slupsky, C. Understanding the human salivary metabolome. NMR Biomed. 2009, 22, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Xie, G.; Zhou, Z.; Shi, P.; Qiu, Y.; Zheng, X.; Chen, T.; Su, M.; Zhao, A.; Jia, W. Salivary metabolite signatures of oral cancer and leukoplakia. Int. J. Cancer 2010, 129, 2207–2217. [Google Scholar] [CrossRef]
- Rochfort, S. Metabolomics Reviewed: A New “Omics” Platform Technology for Systems Biology and Implications for Natural Products Research. J. Nat. Prod. 2005, 68, 1813–1820. [Google Scholar] [CrossRef] [PubMed]
- Fidalgo, T.K.S.; Freitas-Fernandes, L.B.; Almeida, F.C.L.; Valente, A.P.; Souza, I.P.R. Longitudinal evaluation of salivary profile from children with dental caries before and after treatment. Metabolomics 2015, 11, 583–593. [Google Scholar] [CrossRef]
- Letieri, A.S.; Freitas-Fernandes, L.B.; Souza, I.P.R.; Valente, A.P.; Fidalgo, T.K.S. Metabolomic Signatures of In Vitro Biofilm Maturation of Streptococcus mutans. Curr. Microbiol. 2022, 79, 1–12. [Google Scholar] [CrossRef]
- Kageyama, G.; Saegusa, J.; Irino, Y.; Tanaka, S.; Tsuda, K.; Takahashi, S.; Sendo, S.; Morinobu, A. Metabolomics analysis of saliva from patients with primary Sjogren’s syndrome. Clin. Exp. Immunol. 2015, 182, 149–153. [Google Scholar] [CrossRef] [Green Version]
- Almeida, P.A.; Fidalgo, T.K.; Freitas-Fernandes, L.B.; Almeida, F.C.; Souza, I.P.; Valente, A.P. Salivary metabolic profile after hemodialysis among children and adolescents with chronic kidney disease. Metabolomics 2017, 13, 141–150. [Google Scholar] [CrossRef]
- De Oliveira, L.R.P.; Martins, C.; Fidalgo, T.K.S.; Freitas-Fernandes, L.B.; De Oliveira Torres, R.; Soares, A.L.; Almeida, F.C.L.; Valente, A.P.; De Souza, I.P.R. Salivary Metabolite Fingerprint of Type 1 Diabetes in Young Children. J. Proteome Res. 2016, 15, 2491–2499. [Google Scholar] [CrossRef]
- Freitas-Fernandes, L.B.; Fidalgo, T.K.S.; de Almeida, P.A.; Souza, I.P.R.; Valente, A.P. Salivary metabolome of children and adolescents under peritoneal dialysis. Clin. Oral Investig. 2020, 25, 2345–2351. [Google Scholar] [CrossRef] [PubMed]
- Letieri, A.D.S.; Freitas-Fernandes, L.B.; Albarello, L.L.; Fontes, G.P.; de Souza, I.P.R.; Valente, A.P.; Fidalgo, T.K.D.S. Analysis of Salivary Metabolites by Nuclear Magnetic Resonance Before and After Oral Mucosa Cleaning of Infants in the Pre-dental Period. Front. Dent. Med. 2021, 2, 667365. [Google Scholar] [CrossRef]
- Fidalgo, T.K.S.; Freitas-Fernandes, L.B.; Angeli, R.; Muniz, A.M.S.; Gonsalves, E.; Santos, R.; Nadal, J.; Almeida, F.C.L.; Valente, A.P.; Souza, I.P.R. Salivary metabolite signatures of children with and without dental caries lesions. Metabolomics 2013, 9, 657–666. [Google Scholar] [CrossRef]
- da Silva, L.P.; De Abreu Da Silva Bastos, V.; da Silva Fidalgo, T.K.; de Oliveira, C.M.; Pomarico, L.; Valente, A.P.; Freitas-Fernandes, L.B.; De Souza, I.P.R. Oral Health of Babies and Mothers during the Breastfeeding Period. J. Clin. Diagn. Res. 2019, 13, ZC09–ZC13. [Google Scholar] [CrossRef]
- Sangeetha Priya, P.; Anitha, N.; Rajesh, E.; Masthan, K.M.K. Anitha, Embryology and development of salivary gland. Eur. J. Mol. Clin. Med. 2020, 7, 764–770. [Google Scholar]
- Verma, N.; Bansal, A.; Tyagi, P.; Jain, A.; Tiwari, U.; Gupta, R. Eruption Chronology in Children: A Cross-sectional Study. Int. J. Clin. Pediatr. Dent. 2017, 10, 278–282. [Google Scholar] [CrossRef]
- Saitou, M.; Gaylord, E.A.; Xu, E.; May, A.J.; Neznanova, L.; Nathan, S.; Grawe, A.; Chang, J.; Ryan, W.; Ruhl, S.; et al. Functional Specialization of Human Salivary Glands and Origins of Proteins Intrinsic to Human Saliva. Cell Rep. 2020, 33, 108402. [Google Scholar] [CrossRef]
- Wan, A.; Seow, W.; Purdie, D.; Bird, P.; Walsh, L.; Tudehope, D. A Longitudinal Study of Streptococcus mutans Colonization in Infants after Tooth Eruption. J. Dent. Res. 2003, 82, 504–508. [Google Scholar] [CrossRef] [Green Version]
- Caufield, P.W.; Dasanayake, A.P.; Li, Y.; Pan, Y.; Hsu, J.; Hardin, J.M. Natural History of Streptococcus sanguinis in the Oral Cavity of Infants: Evidence for a Discrete Window of Infectivity. Infect. Immun. 2000, 68, 4018–4023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holgerson, P.L.; Öhman, C.; Rönnlund, A.; Johansson, I. Maturation of Oral Microbiota in Children with or without Dental Caries. PLoS ONE 2015, 10, e0128534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neyraud, E.; Schwartz, C.; Brignot, H.; Jouanin, I.; Tremblay-Franco, M.; Canlet, C.; Tournier, C. Longitudinal analysis of the salivary metabolome of breast-fed and formula-fed infants over the first year of life. Metabolomics 2020, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ruhl, S.; Rayment, S.A.; Schmalz, G.; Hiller, K.-A.; Troxler, R.F. Proteins in Whole Saliva during the First Year of Infancy. J. Dent. Res. 2005, 84, 29–34. [Google Scholar] [CrossRef]
- Pereira, J.L.; Duarte, D.; Carneiro, T.J.; Ferreira, S.; Cunha, B.; Soares, D.; Costa, A.L.; Gil, A.M. Saliva NMR metabolomics: Analytical issues in pediatric oral health research. Oral Dis. 2019, 25, 1545–1554. [Google Scholar] [CrossRef]
- Piludu, M.; Rayment, S.A.; Liu, B.; Offner, G.D.; Oppenheim, F.G.; Troxler, R.F.; Hand, A.R. Electron Microscopic Immunogold Localization of Salivary Mucins MG1 and MG2 in Human Submandibular and Sublingual Glands. J. Histochem. Cytochem. 2003, 51, 69–79. [Google Scholar] [CrossRef] [Green Version]
- Sonesson, M. On minor salivary gland secretion in children, adolescents and adults. Swed. Dent. J. Suppl. 2011, 215, 9–64. [Google Scholar]
- Dawes, C. Circadian rhythms in human salivary flow rate and composition. J. Physiol. 1972, 220, 529–545. [Google Scholar] [CrossRef]
- Silwood, C.J.; Lynch, E.; Claxson, A.W.; Grootveld, M.C. 1H and (13)C NMR spectroscopic analysis of human saliva. J. Dent. Res. 2002, 81, 422–427. [Google Scholar] [CrossRef]
- Ramadan, Z.; Jacobs, D.; Grigorov, M.; Kochhar, S. Metabolic profiling using principal component analysis, discriminant partial least squares, and genetic algorithms. Talanta 2006, 68, 1683–1691. [Google Scholar] [CrossRef]
- van Velzen, E.J.J.; Westerhuis, J.A.; van Duynhoven, J.P.M.; van Dorsten, F.A.; Hoefsloot, H.C.J.; Jacobs, D.M.; Smit, S.; Draijer, R.; Kroner, C.I.; Smilde, A.K. Multilevel Data Analysis of a Crossover Designed Human Nutritional Intervention Study. J. Proteome Res. 2008, 7, 4483–4491. [Google Scholar] [CrossRef]
- Xia, J.; Sinelnikov, I.V.; Han, B.; Wishart, D.S. MetaboAnalyst 3.0—Making metabolomics more meaningful. Nucleic Acids Res. 2015, 43, W251–W257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massignan, C.; Cardoso, M.; Porporatti, A.L.; Aydinoz, S.; Canto, G.D.L.; Mezzomo, L.A.M.; Bolan, M. Signs and Symptoms of Primary Tooth Eruption: A Meta-analysis. Pediatrics 2016, 137, e20153501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Hulland, S.; O Lucas, J.; Wake, M.; Hesketh, K.D. Eruption of the primary dentition in human infants: A prospective descriptive study. Pediatr. Dent. 2000, 22, 415–421. [Google Scholar] [PubMed]
- Everhart, D.; Bamgboye, P.; Schwartz, M. Salivary Anti-Streptococcus mutans Changes over a Six-month Period in Children Ages Two–Five Years. J. Dent. Res. 1982, 61, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Scalabre, A.; Jobard, E.; Demède, D.; Gaillard, S.; Pontoizeau, C.; Mouriquand, P.; Elena-Herrmann, B.; Mure, P.-Y. Evolution of Newborns’ Urinary Metabolomic Profiles According to Age and Growth. J. Proteome Res. 2017, 16, 3732–3740. [Google Scholar] [CrossRef] [Green Version]
- Ilcol, Y.O.; Ozbek, R.; Hamurtekin, E.; Ulus, I.H. Choline status in newborns, infants, children, breast-feeding women, breast-fed infants and human breast milk. J. Nutr. Biochem. 2005, 16, 489–499. [Google Scholar] [CrossRef]
- Barnes, V.; Ciancio, S.; Shibly, O.; Xu, T.; DeVizio, W.; Trivedi, H.; Guo, L.; Jönsson, T. Metabolomics Reveals Elevated Macromolecular Degradation in Periodontal Disease. J. Dent. Res. 2011, 90, 1293–1297. [Google Scholar] [CrossRef]
- Morzel, M.; Palicki, O.; Chabanet, C.; Lucchi, G.; Ducoroy, P.; Chambon, C.; Nicklaus, S. Saliva electrophoretic protein profiles in infants: Changes with age and impact of teeth eruption and diet transition. Arch. Oral Biol. 2011, 56, 634–642. [Google Scholar] [CrossRef]
- Gibbons, R. Bacterial Adhesion to Oral Tissues: A Model for Infectious Diseases. J. Dent. Res. 1989, 68, 750–760. [Google Scholar] [CrossRef]
- Gardner, A.; Parkes, H.G.; So, P.-W.; Carpenter, G.H. Determining bacterial and host contributions to the human salivary metabolome. J. Oral Microbiol. 2019, 11, 1617014. [Google Scholar] [CrossRef] [Green Version]
- Meleti, M.; Quartieri, E.; Antonelli, R.; Pezzi, M.; Ghezzi, B.; Viani, M.; Setti, G.; Casali, E.; Ferrari, E.; Ciociola, T.; et al. Metabolic Profiles of Whole, Parotid and Submandibular/Sublingual Saliva. Metabolites 2020, 10, 318. [Google Scholar] [CrossRef]
- Van Houte, J.; Russo, J.; Prostak, K.S. Increased pH-lowering ability of Streptococcus mutans cell masses associated with extracellular glucan-rich matrix material and the mechanisms involved. J. Dent. Res. 1989, 68, 451–459. [Google Scholar] [CrossRef]
- Aimetti, M.; Cacciatore, S.; Graziano, A.; Tenori, L. Metabonomic analysis of saliva reveals generalized chronic periodontitis signature. Metabolomics 2011, 8, 465–474. [Google Scholar] [CrossRef]
- Marincola, F.C.; Corbu, S.; Lussu, M.; Noto, A.; Dessì, A.; Longo, S.; Civardi, E.; Garofoli, F.; Grenci, B.; Mongini, E.; et al. Impact of Early Postnatal Nutrition on the NMR Urinary Metabolic Profile of Infant. J. Proteome Res. 2016, 15, 3712–3723. [Google Scholar] [CrossRef]
- Barr, D.B.; Wilder, L.C.; Caudill, S.P.; Gonzalez, A.J.; Needham, L.L.; Pirkle, J.L. Urinary Creatinine Concentrations in the U.S. Population: Implications for Urinary Biologic Monitoring Measurements. Environ. Health Perspect. 2005, 113, 192–200. [Google Scholar] [CrossRef] [Green Version]
- Gu, H.; Pan, Z.; Xi, B.; Hainline, B.E.; Shanaiah, N.; Asiago, V.; Gowda, G.A.N.; Raftery, D. 1H NMR metabolomics study of age profiling in children. NMR Biomed. 2009, 22, 826–833. [Google Scholar] [CrossRef] [Green Version]
- Kawanishi, N.; Hoshi, N.; Masahiro, S.; Enomoto, A.; Ota, S.; Kaneko, M.; Soga, T.; Tomita, M.; Kimoto, K. Effects of inter-day and intra-day variation on salivary metabolomic profiles. Clin. Chim. Acta 2019, 489, 41–48. [Google Scholar] [CrossRef]
- Nagler, R.; Bahar, G.; Shpitzer, T.; Feinmesser, R. Concomitant Analysis of Salivary Tumor Markers—A New Diagnostic Tool for Oral Cancer. Clin. Cancer Res. 2006, 12, 3979–3984. [Google Scholar] [CrossRef] [Green Version]
- Shpitzer, T.; Bahar, G.; Feinmesser, R.; Nagler, R.M. A comprehensive salivary analysis for oral cancer diagnosis. J. Cancer Res. Clin. Oncol. 2007, 133, 613–617. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metabolites Metabocard | Chemical Shift | >30 Months Mean (95% CI) | <30 Months Mean (95% CI) | p-Value |
|---|---|---|---|---|
| Acetate 1,2 HMDB0000042 | 1.91 | 11.1 × 10−3 (0.4 × 10−3–65.0 × 10−3) | 76.5 × 10−3 (3.1 × 10−3–251.0 × 10−3) | <0.01 |
| Alanine 2 HMDB0001310 | 3.79 | 25.6 × 10−3 (4.0 × 10−3–64.0 × 10−3) | 15.5 × 10−3 (8 × 10−3–40.0 × 10−3) | 0.02 |
| Butyrate 1,2 HMDB0000039 | 2.36 | 7.9 × 10−3 (1.0 × 10−3–10.0 × 10−3) | 14.0 × 10−3 (3.2 × 10−3–14.5 × 10−3) | <0.01 |
| Choline 2 HMDB0000097 | 3.51 | 11.7 × 10−3 (3.0 × 10−3–50.0 × 10−3) | 7.0 × 10−3 (2.0 × 10−3–10 × 10−3) | 0.04 |
| Creatinine 1,2 HMDB0000562 | 3.03 | 2.7 × 10−3 (0.4 × 10−3–8.0 × 10−3) | 6.8 × 10−3 (1.0 × 10−3–14.0 × 10−3) | <0.01 |
| Ethanol 1,2 HMDB0000108 | 3.61 | 23.1 × 10−3 (0.4 × 10−3–50.0 × 10−3) | 14.9 × 10−3 (8.0 × 10−3–16.0 × 10−3) | 0.02 |
| Formate HMDB0000142 | 8.46 | 0.07 × 10−3 (1.0 × 10−3–3.0 × 10−3) | 0.5 × 10−3 (2.0 × 10−3–7.0 × 10−3) | 0.25 |
| Glycerol 1,2 HMDB0000131 | 3.63 | 38.0 × 10−3 (7.2 × 10−3–203.2 × 10−3) | 17.3 × 10−3 (6.9 × 10−3–36.8 × 10−3) | 0.03 |
| Lactate 1,2 HMDB0000190 | 1.32 | 24.3 × 10−3 (3.3 × 10−3–50.0 × 10−3) | 11.7 × 10−3 (2.0 × 10−3–20.0 × 10−3) | <0.01 |
| Leucine 2 HMDB0000687 | 1.69 | 4.1 × 10−3 (2.0 × 10−3–10.0 × 10−3) | 10.3 × 10−3 (2.2 × 10−3–20.0 × 10−3) | <0.01 |
| N−acetyl−sugar 1,2 | 2.02 | 9.1 × 10−3 (0.9 × 10−3–20.0 × 10−3) | 21.2 × 10−3 (5.0 × 10−3–30.0 × 10−3) | <0.01 |
| Phenylalanine 2 HMDB0000159 | 7.50 | 0.3 × 10−3 (1.0 × 10−3–1.7 × 10−3) | 1.4 × 10−3 (0.3 × 10−3–3.0 × 10−3) | 0.01 |
| Propionate 2 HMDB0000237 | 1.04 | 2.0 × 10−3 (0.3 × 10−3–14.0 × 10−3) | 6.2 × 10−3 (0.6 × 10−3–18.0 × 10−3) | <0.01 |
| Succinate 2 HMDB0000254 | 2.41 | 5.7 × 10−3 (0.8 × 10−3–14.0 × 10−3) | 10.0 × 10−3 (0.4 × 10−3–17.0 × 10−3) | <0.05 |
| Sugar region 1,2 | 3.81 | 26.5 × 10−3 (4.0 × 10−3–60.0 × 10−3) | 15.2 × 10−3 (9.0 × 10−3–37 × 10−3) | <0.01 |
| Trimethylamine 2 HMDB0000906 | 2.98 | 1.7 × 10−3 (0.03 × 10−3–5.0 × 10−3 | 4.4 × 10−3 (0.6 × 10−3–12.0 × 10−3 | <0.01 |
| Valerate 1,2 HMDB0000892 | 2.15 | 6.5 × 10−3 (1.2 × 10−3–13.1 × 10−3) | 10.6 × 10−3 (3.2 × 10−3–14.5 × 10−3) | <0.01 |
| Valine 2 HMDB0000883 | 0.96 | 2.7 × 10−3 (0.5 × 10−3–5.0 × 10−3) | 6.6 × 10−3 (1.4 × 10−3–9.0 × 10−3) | <0.01 |
| Caproic acid 2 HMDB0000535 | 0.91 | 4.5 × 10−3 (0.8 × 10−3–10.0 × 10−3) | 9.4 × 10−3 (4.4 × 10−3–14.0 × 10−3) | <0.01 |
| Urea HMDB0000294 | 5.7 | 1.4 × 10−3 (0.3 × 10−3–5.0 × 10−3) | 1.6 × 10−3 (0.17 × 10−3–5.0 × 10−3) | 0.72 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freitas-Fernandes, L.B.; Fontes, G.P.; Letieri, A.d.S.; Valente, A.P.; Souza, I.P.R.d.; Fidalgo, T.K.d.S. NMR-Based Metabolomics Demonstrates a Metabolic Change during Early Developmental Stages from Healthy Infants to Young Children. Metabolites 2023, 13, 445. https://doi.org/10.3390/metabo13030445
Freitas-Fernandes LB, Fontes GP, Letieri AdS, Valente AP, Souza IPRd, Fidalgo TKdS. NMR-Based Metabolomics Demonstrates a Metabolic Change during Early Developmental Stages from Healthy Infants to Young Children. Metabolites. 2023; 13(3):445. https://doi.org/10.3390/metabo13030445
Chicago/Turabian StyleFreitas-Fernandes, Liana Bastos, Gabriela Pereira Fontes, Aline dos Santos Letieri, Ana Paula Valente, Ivete Pomarico Ribeiro de Souza, and Tatiana Kelly da Silva Fidalgo. 2023. "NMR-Based Metabolomics Demonstrates a Metabolic Change during Early Developmental Stages from Healthy Infants to Young Children" Metabolites 13, no. 3: 445. https://doi.org/10.3390/metabo13030445